Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
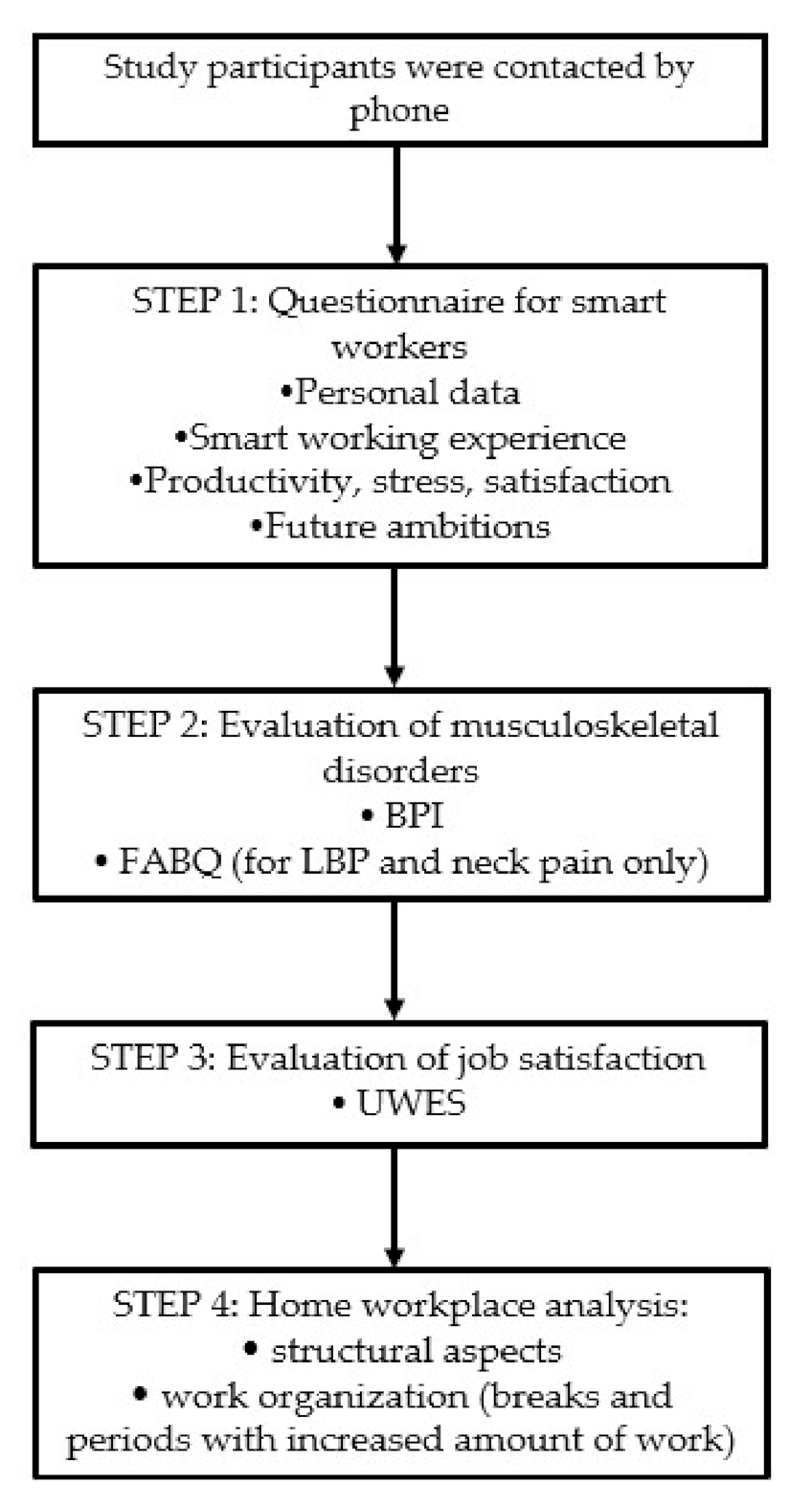
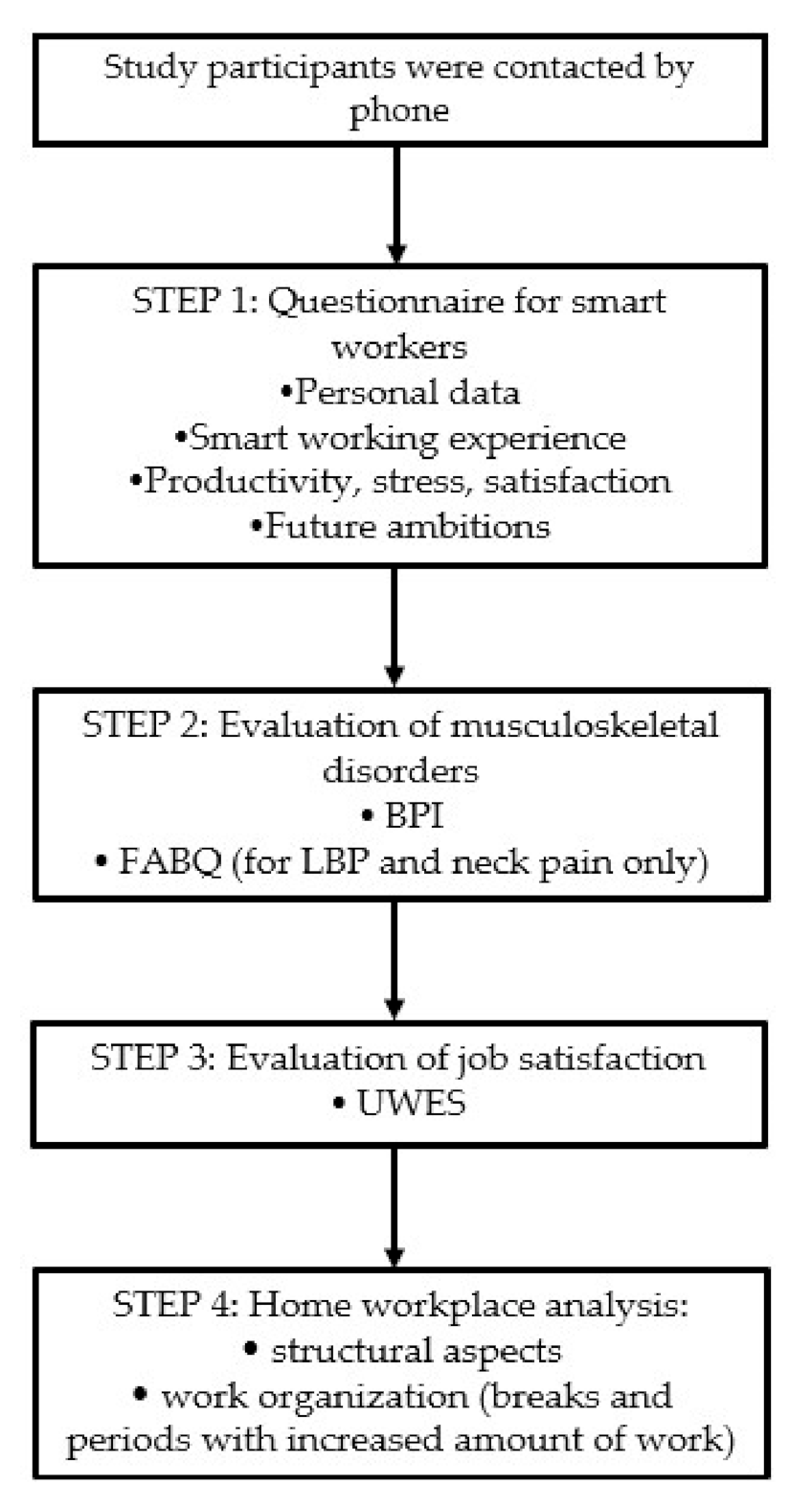
2.1. Study Participants and Procedures
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Productivity
4.2. Job Satisfaction
4.3. Mental Health
4.4. Physical Health
4.5. Limitations
5. Implications for Practice
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Eurofound and the International Labour Office. Working Anytime, Anywhere: The Effects on the World of Work; European Union: Luxembourg; the International Labour Office: Geneva, Switzerland, 2017. [Google Scholar]
- Savic, D. COVID-19 and Work from Home: Digital Transformation of the Workforce. Grey J. (TGJ) 2020, 16, 101–104. [Google Scholar]
- The Balance Careers. The Pros and Cons of a Flexible Work Schedule. Available online: https://www.thebalancecareers.com/advantages-and-disadvantages-of-flexible-work-schedules-1917964 (accessed on 26 June 2020).
- Nibusinessinfo. Employees Working from Home. Available online: https://www.nibusinessinfo.co.uk/content/advantages-and-disadvantages-employees-working-home (accessed on 26 June 2020).
- Pillastrini, P.; Mugnai, R.; Bertozzi, L.; Costi, S.; Curti, S.; Guccione, A.; Mattioli, S.; Violante, F.S. Effectiveness of an ergonomic intervention on work-related posture and low back pain in video display terminal operators: A 3 year cross-over trial. Appl. Ergon. 2010, 41, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Will, J.S.; Bury, D.C.; Miller, J.A. Mechanical Low Back Pain. Am. Fam. Physician 2018, 98, 421–428. [Google Scholar] [PubMed]
- Côté, P.; van der Velde, G.; David Cassidy, J.; Carroll, L.J.; Hogg-Johnson, S.; Holm, L.W.; Carragee, E.J.; Haldeman, S.; Nordin, M.; Hurwitz, E.L. The Burden and Determinants of Neck Pain in Workers. Eur. Spine J. 2008, 17, 60–74. [Google Scholar] [CrossRef]
- Baker, R.; Coenen, P.; Howie, E.; Williamson, A.; Straker, L. The Short Term Musculoskeletal and Cognitive Effects of Prolonged Sitting During Office Computer Work. Int. J. Environ. Res. Public Health 2018, 15, 1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association Foundation. Working Remotely During COVID-19. Available online: http://workplacementalhealth.org/getmedia/fd8a9b98-b491-4666-8f27-2bf59b00e475/Working-Remotely-During-COVID-19-CWMH-Guide (accessed on 11 June 2020).
- Grant, C.A.; Wallace, L.M.; Spurgeon, P. An exploration of the psychological factors affecting remote e-worker’s job effectiveness, well-being and work-life balance, Empl. Relat. 2013, 35, 527–546. [Google Scholar] [CrossRef]
- Kotera, Y.; Vione, K. Psychological Impacts of the New Ways of Working (NWW): A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5080. [Google Scholar] [CrossRef]
- Vittersø, J.; Akselsen, S.; Evjemo, B.; Julsrud, T.; Yttri, B.; Bergvik, S. Impacts of Home-Based Telework on Quality of Life for Employees and Their Partners. Quantitative and Qualitative Results from a European Survey. J. Happiness Stud. 2003, 4, 201–233. [Google Scholar] [CrossRef]
- Hilbrecht, M.; Shaw, S.M.; Johnson, L.C.; Andrey, J. I’m home for the kids: Contradictory implications for work-life balance of teleworking mothers. Gend. Work Organ. 2008, 5, 455–471. [Google Scholar] [CrossRef]
- Nakrošienė, A.; Bučiūnienė, I.; Goštautaitė, B. Working from home: Characteristics and outcomes of telework. Int. J. Manpow. 2019, 40, 87–101. [Google Scholar] [CrossRef]
- Hartig, T.; Kylin, C.; Johansson, G. The Telework Tradeoff: Stress Mitigation vs Constrained Restoration. Appl. Psychol. 2007, 56, 231–253. [Google Scholar] [CrossRef]
- Mann, S.; Holdsworth, L. The psychological impact of teleworking: Stress, emotions and health. New Technol. Work Employ. 2003, 18, 196–211. [Google Scholar] [CrossRef]
- Caraceni, A.; Mendoza, T.R.; Mencaglia, E.; Baratella, C.; Edwards, K.; Forjaz, M.J.; Martini, C.; Serlin, R.C.; de Conno, F.; Cleeland, C.S. A validation study of an Italian version of the brief pain inventory (Breve questionario per la valutazione del dolore). Pain 1996, 65, 87–92. [Google Scholar] [CrossRef]
- Monticone, M.; Baiardi, P.; Bonetti, F.; Ferrari, S.; Foti, C.; Pillastrini, P.; Rocca, B.; Vanti, C.; Zanoli, G. The Italian version of the Fear-Avoidance Beliefs Questionnaire (FABQ-I): Cross-cultural adaptation, factor analysis, reliability, validity, and sensitivity to change. Spine 2012, 37, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The Measurement of Work Engagement with a Short Questionnaire. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Flexjobs. Annual survey Finds Workers are More Productive at Home. Available online: https://www.flexjobs.com/blog/post/2018-annual-survey-finds-workers-more-productive-at-home/ (accessed on 11 June 2020).
- Golden, T.D.; Veiga, J.F. The impact of extent of telecommuting on job satisfaction. Resolving inconsistent findings. J. Manag. 2005, 31, 301–318. [Google Scholar] [CrossRef] [Green Version]
- Golden, T.D. The role of relationships in understanding telecommuter satisfaction. J. Organ. Behav. 2006, 27, 319–340. [Google Scholar] [CrossRef]
- Fana, M.; Torrejón Pérez, S.; Fernández-Macías, E. Employment impact of Covid-19 crisis: From short term effects to long terms prospects. J. Ind. Bus. Econ. 2020, 15, 1–20. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Tripi, S.; Mattei, G. COVID-19 and Public Administration: Implications of Smart Working for Management and Workers’ Mental Health. Available online: https://www.researchgate.net/publication/342163063_COVID-19_and_Public_Administration_implications_of_smart_working_for_management_and_workers’_mental_health (accessed on 22 July 2020).
- Fatoye, F.; Gebrye, T.; Odeyemi, I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol. Int. 2019, 39, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Safiri, S.; Kolahi, A.A.; Hoy, D.; Buchbinder, R.; Mansournia, M.A.; Bettampadi, D.; Ashrafi-Asgarabad, A.; Almasi-Hashiani, A.; Smith, E.; Sepidarkish, M.; et al. Global, regional, and national burden of neck pain in the general population, 1990–2017: Systematic analysis of the Global Burden of Disease Study 2017. BMJ 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef]
- Allegri, M.; Lucioni, C.; Mazzi, S.; Serra, G. Social cost of chronic pain in Italy. Glob. Reg. Health Technol. Assess. 2015, 2, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Bontrup, C.; Taylor, W.R.; Brenner-Fliesser, M.; Visscher, R.; Green, T.; Wippert, P.-M.; Zemp, R. Low back pain and its relationship with sitting behaviour among sedentary office workers. Appl. Ergon. 2019, 81, 102894. [Google Scholar] [CrossRef] [PubMed]
- Cholewicki, J.; Pathak, P.; Reeves, N.; Popovich, J. Simulation of Multifactorial Causes of Low Back Pain. Spine J. 2016, 16, S277. [Google Scholar] [CrossRef]
- Spyropoulos, P.; Papathanasiou, G.; Georgoudis, G.; Chronopoulos, E.; Koutis, H.; Koumoutsou, F. Prevalence of low back pain in Greek public office workers. Pain Physician 2007, 10, 651–659. [Google Scholar] [PubMed]
- Burdorf, A.; Naaktgeboren, B.; de Groot, H.C. Occupational risk factors for low back pain among sedentary workers. J. Occup. Med. 1993, 35, 1213–1220. [Google Scholar] [PubMed]
- Mörl, F.; Bradl, I. Lumbar posture and muscular activity while sitting during office work. J. Electromyogr. Kinesiol. 2013, 23, 362–1368. [Google Scholar] [CrossRef]
- Wahlstrom, J.; Hagberg, M.; Toomingas, A.; Tornqvist, E.W. Perceived muscular tension, job strain, physical exposure, and associations with neck pain among VDU users; a prospective cohort study. Occup. Environ. Med. 2004, 61, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Johnston, V.; Jull, G.; Souvlis, T.; Jimmieson, N.L. Neck movement and muscle activity characteristics in female office workers with neck pain. Spine 2008, 33, 555–563. [Google Scholar] [CrossRef]
- Office Ergonomics: Your How-to Guide. Mayo Foundation for Medical Education and Research. Available online: https://www.mayoclinic.org/healthy-lifestyle/adult-health/in-depth/office-ergonomics/art-20046169 (accessed on 24 June 2020).
- Mal di Quarantena: Il mal di Schiena è Stato il Disturbo più Diffuso Durante il Lockdown, ne ha Sofferto 1 Italiano su 2 Federchimica Assosalute–Associazione Nazionale Farmaci di Automedicazione. Available online: https://www.federchimica.it/webmagazine/dettaglio-news/2020/05/29/mal-di-schiena-assosalute (accessed on 24 June 2020).

{kind=link}
| Study Participants | Total (N = 51) |
|---|---|
| Age (years) | 46.67 ± 11.26 |
| Weight (kg) | 72.69 ± 13.57 |
| Height (cm) | 168.82 ± 8.43 |
| BMI (kg/m2) | 25.41 ± 4.29 |
| Gender | |
| Male | 22 (43.1%) |
| Female | 29 (56.9 %) |
| Cohabitants | |
| ≥3 | 29 (56.9%) |
| <3 | 22 (43.1%) |
| Minor children | |
| No | 36 (70.6%) |
| Yes | 15 (29.4%) |
| Education | |
| Primary School | 0 (0%) |
| Secondary School | 0 (0%) |
| High School | 17 (33.3%) |
| First Level Degree | 4 (7.8%) |
| Second Level Degree | 28 (55%) |
| University Master | 1 (1.9%) |
| PhD | 1 (1.9%) |
| Home Working Feature | Total (N = 51) |
|---|---|
| Type of remote work | |
| Same as office work | 27 (53%) |
| Different tasks | 8 (15.7%) |
| Different schedule | 15 (29.4%) |
| Different salary | 1 (1.9%) |
| Working hours per week | |
| <36 | 26 (51%) |
| ≥36 | 25 (49%) |
| Productivity | |
| Lower | 20 (39.2%) |
| Equal | 16 (31.4%) |
| Higher | 15 (29.4%) |
| Stress | |
| Lower | 20 (39.2%) |
| Equal | 14 (27.5%) |
| Higher | 17 (33.3%) |
| Satisfaction | |
| Lower | 18 (35.3%) |
| Equal | 26 (51%) |
| Higher | 7 (13.7%) |
| Advantages * | |
| Saved travel time | 42 (82.4%) |
| Time flexibility | 12 (23.5%) |
| Greater autonomy | 5 (9.8%) |
| Time spent with family | 13 (25.4%) |
| Enhanced attention | 6 (11.8%) |
| Disadvantages * | |
| Distractions in the domestic environment | 20 (40.6%) |
| Planning difficulties | 5 (9.8%) |
| Impaired interaction with colleagues | 21 (41.2%) |
| Technical failures | 12 (23.5%) |
| Desire to continue home working | |
| Yes, as much as possible | 12 (23.5%) |
| Yes, occasionally | 20 (39.2%) |
| No, for difficult job management | 0 (0%) |
| No, for increased costs | 0 (0%) |
| No, for the lack of interaction with colleagues | 16 (31.4%) |
| No, for the increase in distraction factors | 3 (5.9%) |
| No, for increased work amount | 0 (0%) |
| Site | Total (N = 51) |
|---|---|
| Low back | 21 (41.2%) |
| Neck | 12 (23.5%) |
| Shoulder | 4 (7.8%) |
| Hip | 4 (7.8%) |
| Knee | 4 (7.8%) |
| Thigh | 3 (5.9%) |
| Elbow | 2 (3.9%) |
| Site | BPI Severity Index | BPI Interference Index |
|---|---|---|
| Low back pain | 1.52 ± 1.63 | 2.28 ± 1.33 |
| Neck pain | 1.97 ± 1.70 | 2.75 ± 1.78 |
| Shoulder pain | 1.40 ± 1.06 | 1.97 ± 1.26 |
| Hip pain | 0.80 ± 1.04 | 1.95 ± 1.44 |
| Knee pain | 1.43 ± 0.98 | 2.06 ± 1.38 |
| Thigh pain | 1.20 ± 0.50 | 0.95 ± 0.08 |
| Elbow pain | 3.05 ± 0.63 | 2.95 ± 1.20 |
| FABQ-PA | FABQ-W | FABQ-TOT | |
|---|---|---|---|
| Low back pain | 10.10 ± 5.96 | 11.52 ± 11.04 | 21.62 ± 13.67 |
| Neck pain | 10.67 ± 6.37 | 14.08 ± 10.46 | 24.75 ± 14.56 |
| Low Back PainN = 21 | Neck PainN = 12 | Shoulder PainN = 4 | Hip PainN = 4 | Knee Pain N = 4 | Thigh Pain N = 3 | Elbow Pain N = 2 | |
|---|---|---|---|---|---|---|---|
| Improved | 3 (14.3%) | 1 (8.3%) | 0(0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Worsened | 8 (38.1%) | 6 (50%) | 2 (50%) | 1 (25%) | 0 (0%) | 0 (0%) | 2 (100%) |
| Equal | 10 (47.6%) | 5 (41.7%) | 2 (50%) | 3 (75%) | 4 (100%) | 3 (100%) | 0 (0%) |
| UWES-17 | p-Value | |
|---|---|---|
| Home workers with pain (N = 36) | 74.86 ± 14.42 | 0.009 * |
| Home workers without pain (N = 15) | 87.70 ± 9.10 | |
| Total home workers (N = 51) | 78.17 ± 16.29 |
| Equipment | Total (N = 51) |
|---|---|
| Chair | |
| Adjustable seat height | |
| Yes | 23 (45.1%) |
| No | 28 (54.9%) |
| Support | |
| 4 legs | 29 (56.9%) |
| 5 wheels | 22 (43.1%) |
| Back | |
| Flat | 23 (45.1%) |
| Concave | 28 (54.9%) |
| Adjustable back height | |
| Yes | 15 (29.4%) |
| No | 36 (70.6%) |
| Adjustable back inclinationYes | 16 (31.4%) |
| No | 35 (68.6%) |
| Table | |
| Type of table | |
| Single top not adjustable in height | 44 (86.3%) |
| Single or double top adjustable in height | 6 (11.8%) |
| Two-height top with lowered keyboard holder | 1 (1.9%) |
| Table height | |
| Over 73.5 cm | 20 (39.2%) |
| 72 ± 1.5 cm | 24 (47%) |
| Under 70.5 cm | 7 (13.8%) |
| Equipment | Total(N = 51) |
|---|---|
| Desktop/Laptop | |
| Desktop | 30 (58.8%) |
| Laptop | 21(41.2%) |
| Monitor | |
| Not adjustable | 6(11.8%) |
| Adjustable in inclination | 30 (58.8%) |
| Adjustable in inclination, height, rotation | 15 (29.4%) |
| Eye distance from the monitor | |
| <50 cm | 9 (17.7%) |
| 50–70 cm | 34 (66.6%) |
| >70 cm | 8 (15.7%) |
| Keyboard distance from the edge | |
| <15 cm | 4 (7.8%) |
| >15 cm | 47 (92.2%) |
| External keyboard | |
| No | 19 (37.3%) |
| Yes | 32 (62.7%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. https://doi.org/10.3390/ijerph17176284
Moretti A, Menna F, Aulicino M, Paoletta M, Liguori S, Iolascon G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. International Journal of Environmental Research and Public Health. 2020; 17(17):6284. https://doi.org/10.3390/ijerph17176284
Chicago/Turabian StyleMoretti, Antimo, Fabrizio Menna, Milena Aulicino, Marco Paoletta, Sara Liguori, and Giovanni Iolascon. 2020. "Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis" International Journal of Environmental Research and Public Health 17, no. 17: 6284. https://doi.org/10.3390/ijerph17176284
APA StyleMoretti, A., Menna, F., Aulicino, M., Paoletta, M., Liguori, S., & Iolascon, G. (2020). Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. International Journal of Environmental Research and Public Health, 17(17), 6284. https://doi.org/10.3390/ijerph17176284