Development and Fidelity Testing of the Test@Work Digital Toolkit for Employers on Workplace Health Checks and Opt-In HIV Testing




Abstract
1. Background
2. Methods
- Pre-define; STAGE 1: Online survey to understand the context.
- Define; STAGE 1 and STAGE 2: Stakeholder consultation to define toolkit.
- Design; STAGE 3: Draft content and technical development by project team with internal user testing.
- Develop; STAGE 3: Expert reviews leading to toolkit refinement and production.
- Deploy; STAGE 4: Real-world fidelity testing with employer users.
3. Study STAGES 1–4: Methods and Results
3.1. STAGE 1: Online Survey
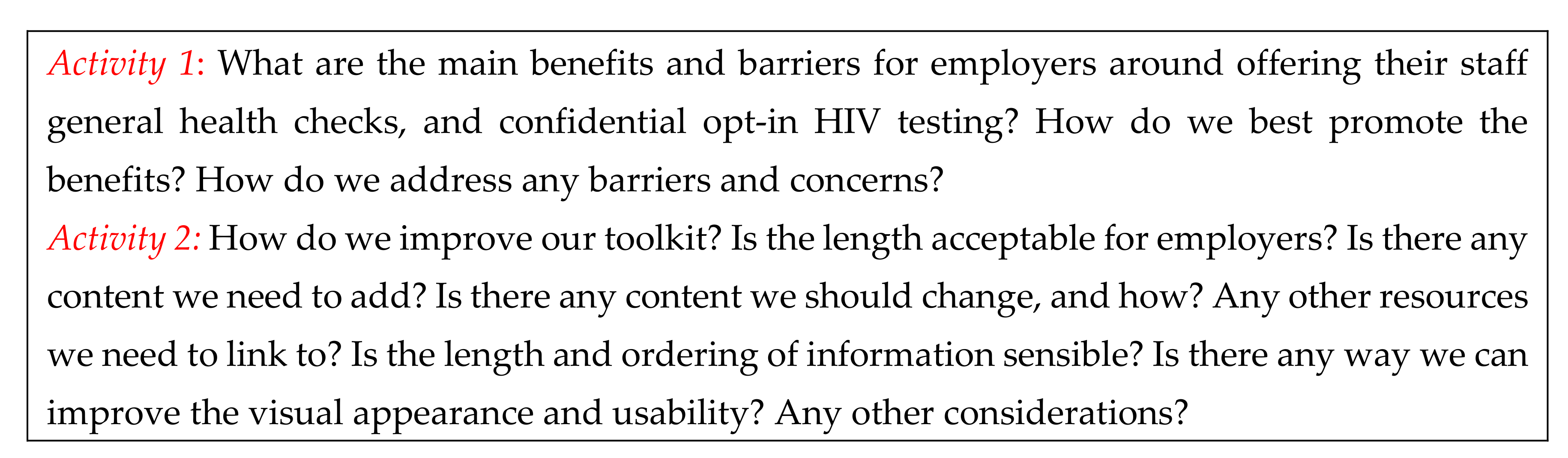
3.2. STAGE 2: Stakeholder Consultation
3.3. STAGE 3: Toolkit Development and Expert Peer Review
3.4. STAGE 4: Toolkit Fidelity Testing
- (a)
- Assessment of fidelity (delivery and engagement).
- (b)
- Assessment of implementation qualities.
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burton, J. WHO Healthy Workplace Framework and Model: Background and Supporting Literature and Practice; World Health Organisation: Geneva, Switzerland, 2010; Available online: https://www.who.int/occupational_health/healthy_workplace_framework.pdf (accessed on 12 December 2019).
- Jepson, R.G.; Harris, F.M.; Platt, S.; Tannahill, C. The effectiveness of interventions to change six health behaviours: A review of reviews. BMC Public Health 2010, 10, 538–554. [Google Scholar] [CrossRef]
- PriceWaterHouse Coopers. Building the Case for Wellness; PriceWaterHouse Coopers: London, UK, 2008. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/209547/hwwb-dwp-wellness-report-public.pdf (accessed on 12 December 2019).
- Secommbe, I.; Fenton, K. Health, Work and Health Related Worklessness: A Guide for Local Authorities; Public Health England: London, UK, 2016. Available online: https://www.local.gov.uk/health-work-and-health-related-worklessness-guide-local-authorities (accessed on 10 May 2016).
- Pieper, C.; Schröer, S.; Eilerts, A.L. Evidence of Workplace Interventions-A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2019, 16, 3553. [Google Scholar] [CrossRef]
- Jones, D.; Molitor, D.; Reif, J. What do Workplace Wellness Programs do? Evidence from the Illinois Workplace Wellness Study. Q. J. Econ. 2019, 134, 1747–1791. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Zhou, D.; Batt, M.E. Five-year workplace wellness intervention in the NHS. Perspect. Public Health 2013, 133, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Bennett, E.; EBatt, M. Evaluation of occupational health checks for hospital employees. IJWHM 2014, 7, 247–266. [Google Scholar] [CrossRef]
- Shain, M.; Kramer, D.M. Health promotion in the workplace: framing the concept; reviewing the evidence. Occup. Environ. Med. 2004, 61, 643–648. [Google Scholar] [CrossRef]
- EASHW (European Agency for Safety and Health at Work). Workplace Health Promotion for Employees. Fact Sheet. 2010, p. 94. Available online: http://osha.europa.eu (accessed on 12 December 2019).
- Shamu, S.; Farirai, T.; Kuwanda, L.; Slabbert, J.; Guloba, G.; Khupakonke, S.; Johnson, S.; Masihleho, N.; Kamera, J.; Nkhwashu, N. Comparison of community-based HIV counselling and testing (CBCT) through index client tracing and other modalities: Outcomes in 13 South African high HIV prevalence districts by gender and age. PLoS ONE 2019, 14, e0221215. [Google Scholar] [CrossRef]
- Weihs, M.; Meyer-Weitz, A. Barriers to workplace HIV testing in South Africa: A systematic review of the literature. AIDS Care 2016, 28, 495–499. [Google Scholar] [CrossRef]
- Ishimaru, T.; Wada, K.; Smith, D.R. HIV testing and attitudes among the working-age population of Japan: Annual health checkups may offer an effective way forwards. Ind. Health 2016, 54, 116–122. [Google Scholar] [CrossRef][Green Version]
- Gourlay, A.J.; Pharris, A.M.; Noori, T.; Supervie, V.; Rosinska, M.; Ard van, S.; Touloumi, G.; Porter, K. Towards standardized definitions for monitoring the continuum of HIV care in Europe. AIDS 2017, 31, 2053–2058. [Google Scholar] [CrossRef]
- Nash, S.G.; Furegato, M.; Gill, O.N.; Connor, N. HIV Testing in England: 2017 Report; Public Health England: London, UK, 2017. [Google Scholar]
- Blake, H.; Banerjee, A.; Evans, C. Employer attitudes towards general health checks and HIV testing in the workplace. Public Health 2018, 156, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Hussain, B.; Hand, J.; Juma AEvans, C. Employers’ views of the ‘Healthy Hub Roadshow’: A workplace HIV testing intervention in England. AIDS Care Psychol. Socio-Med. Asp. AIDS/HIV 2018, 20, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Hussain, B.; Hand, J.; Juma, A.; Rowlands, D.; Evans, C. Healthy Hub Roadshow: Employee perceptions of a workplace HIV testing intervention. IJWHM 2018, 11, 333–348. [Google Scholar] [CrossRef]
- Alvarez-Del Arco, D.; Fakoya, I.; Thomadakis, C.; Pantazis, N.; Touloumi, G.; Gennotte, A.F.; Zuure, F.; Barros, H.; Staehelin, C.; Göpel, S.; et al. Advancing Migrant Access to Health Services in Europe (aMASE) study team, High levels of postmigration HIV acquisition within nine European countries. AIDS 2017, 31, 1979–1988. [Google Scholar] [CrossRef]
- Kharsany, A.B.M.; Karim, Q.A. HIV infection and AIDS in Sub-Saharan Africa: Current status, challenges and opportunities. Open AIDS J. 2016, 10, 34–48. [Google Scholar] [CrossRef]
- Poder, A.; Haldre, M. HIV in Europe. Clin. Dermatol. 2014, 32, 282–285. [Google Scholar] [CrossRef]
- Carolan, S.; Harris, P.R.; Cavanagh, K. Improving Employee Well-Being and Effectiveness: Systematic Review and Meta-Analysis of Web-Based Psychological Interventions Delivered in the Workplace. J. Med. Internet Res. 2017, 19, e271. [Google Scholar] [CrossRef]
- Ryan, C.; Bergin, M.; Chalder, T.; Wells, J.S. Web-based interventions for the management of stress in the workplace: Focus, form, and efficacy. J. Occup. Health 2017, 59, 215–236. [Google Scholar] [CrossRef]
- Kerr, D.C.; Ornelas, I.J.; Lilly, M.M.; Calhoun, R.; Meischke, H. Participant Engagement in and Perspectives on a Web-Based Mindfulness Intervention for 9-1-1 Telecommunicators: Multimethod Study. J. Med. Internet Res. 2019, 21, e13449. [Google Scholar] [CrossRef]
- Deitz, D.; Cook, R.F.; Hersch, R.K.; Leaf, S. Heart healthy online: an innovative approach to risk reduction in the workplace. J. Occup. Environ. Med. 2014, 56, 547–553. [Google Scholar] [CrossRef]
- Colkesen, E.B.; Niessen, M.A.; Peek, N.; Vosbergen, S.; Kraaijenhagen, R.A.; van Kalken, C.K.; Tijssen, J.G.; Peters, R.J. Initiation of health-behaviour change among employees participating in a web-based health risk assessment with tailored feedback. J. Occup. Med. Toxicol. 2011, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- De Cocker, K.; Cardon, G.; Vergeer, I.; Radtke, T.; Vandelanotte, C. Who Uses Action Planning in a Web-Based Computer-Tailored Intervention to Reduce Workplace Sitting and What do Action Plans Look Like? Analyses of the Start to stand Intervention among Flemish Employees. Appl. Psychol. Health Well Being 2019, 11, 543–561. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Eakin, E.G.; Winkler, E.A.; Hadgraft, N.; Dunstan, D.W.; Gilson, N.D.; Goode, A.D. Assessing the Feasibility and Pre-Post Impact Evaluation of the Beta (Test) Version of the BeUpstanding Champion Toolkit in Reducing Workplace Sitting: Pilot Study. JMIR Form. Res. 2018, 2, e17. [Google Scholar] [CrossRef] [PubMed]
- Compernolle, S.; Vandelanotte, C.; Cardon, G.; De Bourdeaudhuij, I.; De Cocker, K. Effectiveness of a web-based, computer-tailored, pedometer-based physical activity intervention for adults: a cluster randomized controlled trial. J. Med. Internet Res. 2015, 17, e38. [Google Scholar] [CrossRef] [PubMed]
- De Bourdeaudhuij, I.; Stevens, V.; Vandelanotte, C.; Brug, J. Evaluation of an interactive computer-tailored nutrition intervention in a real-life setting. Ann. Behav. Med. 2007, 33, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Montagni, I.; Dehman, A.; Yu, Z.; Martinez, M.J.; Banner, S.; Rimbert, S.; Hayez, S.; Foster, C.; Fontvieille, A.M. Effectiveness of a Blended Web-Based Intervention to Raise Sleep Awareness at Workplace: The WarmUapp™ Pilot Study. J. Occup. Environ. Med. 2019, 61, e253–e259. [Google Scholar] [CrossRef]
- Martinsson, C.; Lohela-Karlsson, M.; Kwak, L.; Bergström, G.; Hellman, T. What incentives influence employers to engage in workplace health interventions? BMC Public Health 2016, 16, 854. [Google Scholar] [CrossRef]
- Panagiotakopoulos, A. Barriers to employee training and learning in small and medium‐sized enterprises (SMEs). Dev. Learn. Org. Int. J. 2011, 25, 15–18. [Google Scholar] [CrossRef]
- Rhodes, C. Business Statistics. Briefing Paper: Number 06152; House of Commons Library: London, UK, 2018; Available online: https://researchbriefings.parliament.uk/ResearchBriefing/Summary/SN06152 (accessed on 30 December 2018).
- Blake, H. How to Manage Employee Wellbeing in A Small Business. Financ. Dige. 2019. Available online: https://www.financedigest.com/how-to-manage-employee-wellbeing-in-a-small-business.html (accessed on 12 December 2019).
- UNISON. Working With HIV: A Guide for UNISON Safety Reps; UNISON: London, UK, 2013; Available online: https://www.unison.org.uk/content/uploads/2013/06/On-line-Catalogue204713.pdf (accessed on 12 December 2019).
- National Aids Trust (NAT). HIV@ Work—Advice for Employers. June 2012. Available online: https://www.nat.org.uk/sites/default/files/publications/Jul_2012_HIV%40Work_Advice_for_employers_0.pdf (accessed on 12 December 2019).
- Liu, C.; Shao, S.; Liu, C.; Bennett, G.G.; Prvu Bettger, J.; Yan, L.L. Academia-industry digital health collaborations: A cross-cultural analysis of barriers and facilitators. Digit. Health 2019, 5, 2055207619878627. [Google Scholar] [CrossRef]
- Hekler, E.; Klasnja, P.; Riley, W.; Buman, M.P.; Huberty, J.L. Agile science: Creating useful products for behavior change in the real-world. Transl. Behav. Med. 2016, 6, 317–328. [Google Scholar] [CrossRef]
- Todhunter, F. The usefulness of an Agile methodology to underpin a public engagement activity. SJNP 2017, 1, 13–108. [Google Scholar]
- Blake, H.; Gartshore, E. Workplace wellness using online learning tools in a healthcare setting. Nurse Educ. Pract. 2016, 20, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Sucala, M.; Ezeanochie, N.M.; Cole-Lewis, H.; Turgiss, J. An iterative, interdisciplinary, collaborative framework for developing and evaluating digital behavior change interventions. Transl. Behav. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Linnan, L.; Steckler, A. Process Evaluation for Public Health Interventions and Research: An Overview; Jossey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- Murray, E.; Hekler, E.B.; Andersson, G.; Collins, L.M.; Doherty, A.; Hollis, C.; Rivera, D.E.; West, R.; Wyatt, J.C. Evaluating Digital Health Interventions: Key Questions and Approaches. Am. J. Prev. Med. 2016, 51, 843–851. [Google Scholar] [CrossRef]
- Agile Alliance, Manifesto for Agile Software Development. 2001. Available online: https://www.agilealliance.org/agile101/the-agile-manifesto/ (accessed on 12 December 2019).
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]


{kind=link}
| Section | Tab Header | Content |
|---|---|---|
| 1 | About this toolkit | General introduction to the toolkit and tab signposting. |
| 2 | Importance of workplace health | Business case for promoting health at work. Benefits of workplace health promotion. |
| 3 | Health screening in the workplace | Examples of health checks or tests and how they can be offered. Height, weight and body mass index (BMI); blood pressure; cholesterol testing; blood glucose; lung function; cardio fitness. |
| 4 | What is HIV? | About HIV, early testing and treatment, statistics for undiagnosed HIV. How is HIV passed on? What is the treatment for HIV? HIV diagnosis, and rates across UK. |
| 5 | What does HIV testing involve? | Types of test. HIV testing in the workplace. |
| 6 | The role of the employer | Normalising HIV testing and breakdown of stigma. Advice for employers on: What would I do if an employee disclosed a health problem after having a health check at work? Is this different for HIV? Treating employees fairly. |
| 7 | Useful resources | For HIV and HIV testing information. For general health. |
| Research Questions | Test@Work Toolkit and Delivery |
|---|---|
| Is there a clear health need which this toolkit is intended to address? | Reduction of undiagnosed HIV—need to reduce stigma around HIV, normalise HIV testing and increase access to testing. |
| Is there a defined population who could benefit from this toolkit? | Directly: Employers, through a business case for workplace health promotion, support, guidance and resources. Indirectly: Employees, if employers subsequently choose to offer workplace health checks to their workforce. |
| Is the toolkit likely to reach this population, and if so, is the population likely to use it? | Reach and uptake of the toolkit will be assessed in a future health check intervention study with employers. |
| Acceptability and usability | Determined by expert peer reviews, and toolkit usability evaluation questions. |
| Demand | Confirmed by online surveys with employers, and consultations with public-, private- and third-sector partners. |
| Implementation | High fidelity: toolkit has been tested ‘in the wild’ (with competing demands on user’s attention). |
| Practicability | Interactive portable document format (PDF) is accessible across a range of commonly used operating systems and devices. |
| Adaptation | Toolkit can be reviewed and updated without compromising fidelity/integrity. |
| Integration | Publicly accessible, hosted on trusted site, integrated into existing repository of e-learning resources. |
| Is there a credible causal explanation for the toolkit to achieve the desired impact? | Credibility of authors. Toolkit was developed through multi-professional consultation. Content addresses knowledge gaps and needs as identified in prior research and stakeholder consultation. Dual purpose:
|
| What are the key components of the toolkit? Which ones impact on the predicted outcome, and how do they interact with each other? | Key components: Requires < 1 h per user, free access to all users. Content is not tailored, although context-specific information can be provided alongside. Section completion does not reply on completion of earlier sections. Toolkit is brief (to maximise user compliance). Format is simple interactive PDF to maximise implementation and scalability. Content and signposting to further resources (Table 1). |
| What strategies should be used to support tailoring the toolkit to participants over time? | Full package completion is intended. However, there is opportunity for tailoring, adaptive learning and user choice. Users may self-select components of interest, e.g., to individually tailor order and dosage of learning, and access to external signposted resources. Context-specific information (e.g., job-related, organisation type) can be included separately. |
| What is the likely direction and magnitude of the effect of the toolkit or its components compared to a comparator that is meaningful for the stage of the research process? | Demonstrated benefit to employers, shown to be acceptable and feasible. Toolkit will remain stable over the medium term. Reach and uptake to be determined in future health check intervention study. Direction and magnitude of effect be tested in a future definitive randomised controlled trial. |
| Has the possibility of harm been adequately considered? And the likelihood of risks or adverse outcomes assessed? | Provision of accurate information and advice relating to HIV testing produced by a health care team. Stakeholder consultation suggested low risk of content misinterpretation. Potential for toolkit to encourage more employers to offer workplace health checks—this could result in identification of health issues in their employees. However, toolkit contains guidance on roles and responsibilities of employers. No issues with data security or privacy breaches-the toolkit does not collect personal data. No adverse outcomes were reported during testing. Free toolkit means there are no opportunity costs for employers. |
| Has cost been adequately considered and measured? | Free and widely accessible delivery platform (interactive PDF). Long-term maintenance/updating costs should be calculated in a formal health economic analysis as part of a future trial. Estimated 2 h per year maintenance for toolkit authors. |
| What is the overall assessment of the utility of this intervention? And how confident are we in this overall assessment? | High overall utility of the toolkit—based on its potential to increase knowledge on workplace health and HIV testing, providing guidance identified in employer needs assessment. Potential for wide reach, with high uptake, low development costs, immediately scalable intervention with no reported adverse effects, positive evaluation with employers. True assessment of confidence requires testing in a future trial. However, the developed toolkit could easily be incorporated into routine organisational practice in its current form. |
| Question Item | Type of Organisation | p | ||
|---|---|---|---|---|
| Public n= 131 (65.17%) | Private n = 39 (19.40%) | Thirdb n = 31(15.42%) | ||
| Primary job role | <0.001 ** | |||
| Worker | 72 (54.96) | 17 (43.59) | 5 (16.13) | |
| Middle manager/team leader | 33 (25.19) | 10 (25.64) | 10 (32.26) | |
| Senior manager/director/executive a | 26 (19.85) | 12 (30.77) | 16 (51.61) | |
| Does your organisation promote health to employees? | <0.001 ** | |||
| Yes No | 116 (88.55) 15 (11.45) | 23 (58.97) 16 (41.03) | 18 (58.06) 13 (41.94) | |
| Does your organisation offer any health screening c to employees? | <0.001 ** | |||
| Yes No | 61 (46.56) 70 (53.44) | 13 (33.33) 26 (66.67) | 3 (9.68) 28 (90.32) | |
| Would you be interested in offering general health checks in the workplace that included HIV testing c? | 0.137 | |||
| Yes Maybe No | 66 (50.38) 49 (37.40) 16 (12.21) | 17 (43.59) 18 (46.15) 4 (10.26) | 8 (25.81) 19 (61.29) 4 (12.90) | |
| Assessment Type (n = 20) | Actual Success Rate | Pre-Defined Success Rate |
|---|---|---|
| Fidelity Assessment | n (%) or n (mean, SD) | % or mean |
| Fidelity of Delivery | ||
| Per-protocol delivery (functioning link) | 20 (100) | >90% * |
| Toolkit completion rate (% content accessed) | 20 (96.9) | >75% * |
| Fidelity of Engagement | ||
| Understanding of the toolkit | 20 (100) | >90% * |
| Intervention receipt (perceived knowledge) | 19 (95) | >90% * |
| Intervention enactment (knowledge use) | 8 (40) | >30% * |
| Perceived enactment (future use) | 12 (60) | >50% * |
| Implementation Qualities | n (%) or n (mean, SD) | n (%) or mean |
| Practicality | ||
| Use by any organisation | 20 (100) | >75% * |
| Level of burden | 20 (2.1, 2.19) | <6 * |
| Resource Challenges | ||
| Time challenges | 4 (20) | <25% * |
| Technical challenges (skills) | 0 (0) | <25% * |
| Financial challenges | 0 (0) | <25% * |
| Attitudes | ||
| Perceptions toward availability | 20 (9.4, 0.99) | >6 * |
| Acceptability | ||
| Appropriate for needs | 19 (95) | >75% * |
| Contains meaningful information | 20 (100) | >75% |
| Perceived usefulness of the toolkit | 20 (9.3, 0.72) | >6 * |
| Usability | ||
| Ease of navigation | 20 (9.9, 0.31) | >6 * |
| Technical difficulties (functioning) | 0 (0) | <25% * |
| Cost | ||
| Acceptable cost implications | 20 (100) | >75% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blake, H.; Somerset, S.; Evans, C. Development and Fidelity Testing of the Test@Work Digital Toolkit for Employers on Workplace Health Checks and Opt-In HIV Testing. Int. J. Environ. Res. Public Health 2020, 17, 379. https://doi.org/10.3390/ijerph17010379
Blake H, Somerset S, Evans C. Development and Fidelity Testing of the Test@Work Digital Toolkit for Employers on Workplace Health Checks and Opt-In HIV Testing. International Journal of Environmental Research and Public Health. 2020; 17(1):379. https://doi.org/10.3390/ijerph17010379
Chicago/Turabian StyleBlake, Holly, Sarah Somerset, and Catrin Evans. 2020. "Development and Fidelity Testing of the Test@Work Digital Toolkit for Employers on Workplace Health Checks and Opt-In HIV Testing" International Journal of Environmental Research and Public Health 17, no. 1: 379. https://doi.org/10.3390/ijerph17010379
APA StyleBlake, H., Somerset, S., & Evans, C. (2020). Development and Fidelity Testing of the Test@Work Digital Toolkit for Employers on Workplace Health Checks and Opt-In HIV Testing. International Journal of Environmental Research and Public Health, 17(1), 379. https://doi.org/10.3390/ijerph17010379