The Effectiveness of Digital Interventions for Psychological Well-Being in the Workplace: A Systematic Review Protocol




Abstract
1. Introduction
1.1. Review Aim
1.2. Review Objectives
- (1)
- To describe measures that have been utilised to assess the effectiveness of digital interventions designed to improve the following:
- (i)
- Psychological well-being at work;
- (ii)
- The prevention/management of poor mental well-being in the workplace.
- (2)
- To identify associations of digital interventions designed to improve the psychological well-being and/or the prevention/management of poor mental well-being in the workplace with individual and organisational outcomes.
- (3)
- To assess whether theory-informed digital interventions for the promotion of psychological well-being are more effective or not, and
- (i)
- to identify which theory or mechanism is associated with greater effectiveness.
2. Methods
2.1. Eligibility
2.1.1. Inclusion Criteria
- a)
- Type of participants:The included studies will report the result of interventions targeting “employees” defined as working-age adults, as well as adults over 65 years that are still in a contracted role within their organisations.
- b)
- Context/Setting:Included studies will report interventions delivered in the workplace setting.
- c)
- Type of Interventions:Included studies will report interventions that are delivered using digital technology via any delivery channel (e.g., these will include but are not limited to web-based interventions, email, mobile phone and apps). Interventions will focus on psychological or mental well-being (e.g., behavioural, cognitive or educational interventions) delivered via any type of digital technology via any delivery channel. Both controlled (e.g., reporting comparisons with a control group, another intervention, face-to-face intervention) and uncontrolled (e.g., single-group studies, pilot and feasibility studies) studies will be considered for inclusion. There will be no restrictions with regards to the timing, duration, or modality of the interventions.
- d)
- Type of studies:The types of the studies that will be included in this review will be experimental (e.g., randomised controlled trials, cluster-randomised Controlled Trials (RCTs), controlled before-and-after studies) or quasi-experimental studies (e.g., one-group pre-test-post-test design, time series designs). Furthermore, included studies will provide an analysis of the results of the intervention.
- e)
- Comparator(s)/control:Included studies will report digital interventions that are compared with any other type of interventions or a no intervention control group, or have no comparator group. Controlled-studies (e.g., reporting comparisons with a no intervention control group, alternative form of digital intervention or a non-digital intervention) and uncontrolled studies (e.g., single group pre-test post-test studies, uncontrolled pilot and feasibility studies) will be considered for inclusion. Separate analysis will be presented for those studies with randomisation to comparator/control groups.
- f)
- Type of publication:Included studies will report empirical research published in peer-reviewed journals or conference proceedings that are accompanied with full-length peer-reviewed papers.
- g)
- Outcome measures:Included studies will report interventions for which the primary outcome is a focus on the improvement of psychological well-being and/or prevention/management of poor mental well-being.
2.1.2. Exclusion Criteria
- a)
- Type of participants:The study will exclude children and young people (under 18 years of age), and retirees.
- b)
- Context/setting:Studies will be excluded if they report interventions delivered in settings other than the participants’ workplace.
- c)
- Type of interventions:Studies will be excluded if (i) they report digital interventions delivered in conjunction with other interventions (since it would be difficult to ascertain the unique contribution of the digital element), and/or (ii) they do not include a psychological intervention (such as reporting on digital interventions without a psychological component that primarily target physical/behavioural outcomes; i.e., weight loss, physical activity, tracking alcohol consumption).
- d)
- Type of studies:Studies will be excluded if they are not original intervention studies, if they are published in journals that are not peer-reviewed, or if they are not in the English language. They will be excluded if they do not report on a digital intervention. Previous relevant systematic reviews will be identified for the purpose of identification of primary studies, but they will not be included in the review. Studies that report case studies, cohort studies, cross-sectional research designs, conference abstracts (without a corresponding full-length peer-reviewed paper) and unpublished research (e.g., unpublished dissertations/theses) will not be included.
- e)
- Comparator(s)/control:Studies will be excluded if they do not use a randomised or quasi-experimental design (e.g., the review will include randomised and non-randomised studies with comparator/control groups as well as those using a one-group pre-test- post-test design, or time series design).
- f)
- Outcome measures:Studies will be excluded if they (i) do not include relevant outcome measures, (ii) report on interventions or outcomes that focus primarily on the clinical treatment of mental health disorders (e.g., Post-traumatic stress disorder (PTSD), major depression), and (iii) if their primary outcomes do not measure psychological well-being and/or mental well-being outcome(s).
2.2. Search Strategy
2.3. Selection Processes
2.4. Data Extraction
2.5. Quality Appraisal
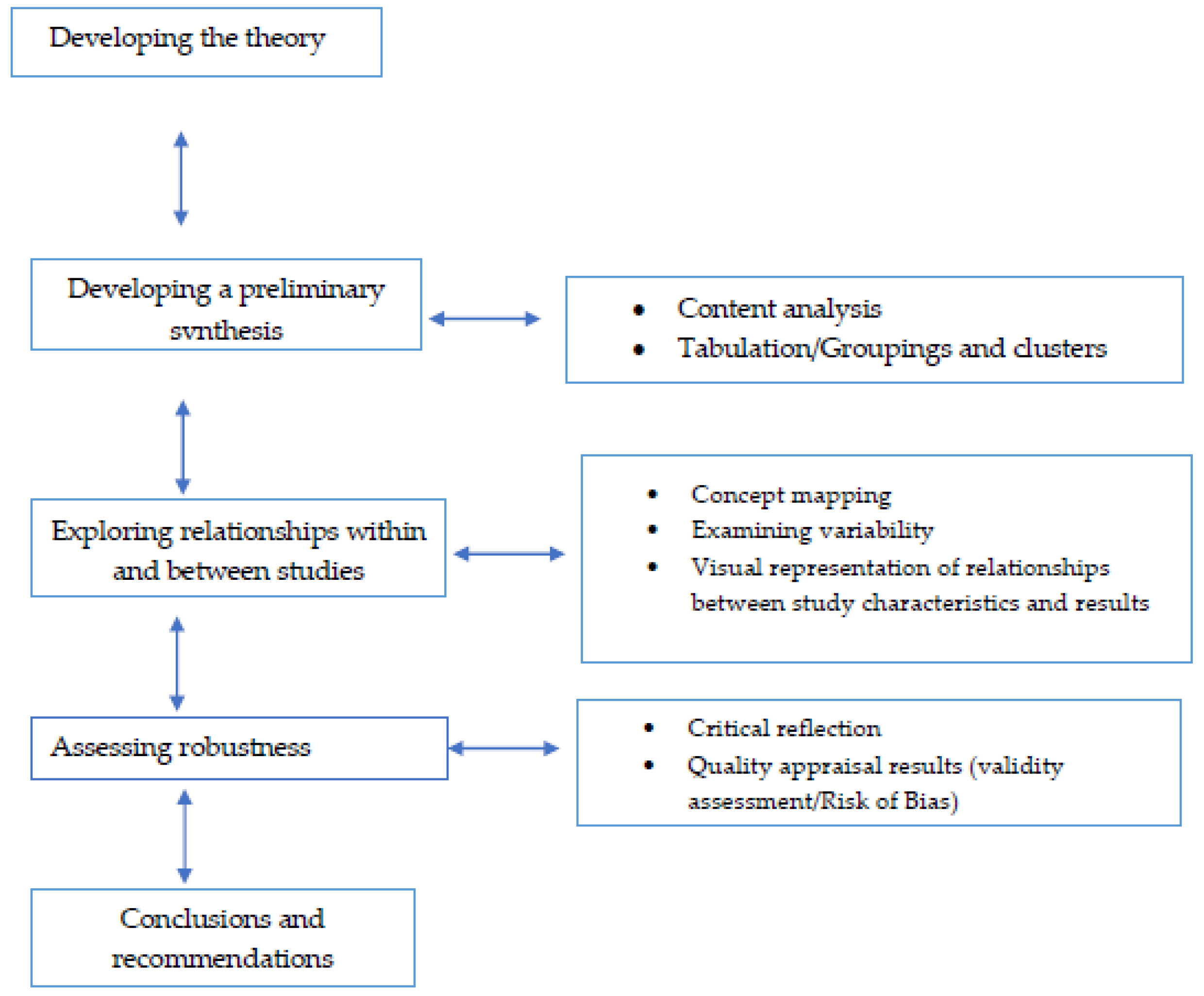
2.6. Data Synthesis
3. Practical Policy Implications
- Recommendations on the use of digital interventions, their strengths and limitations;
- Guidance in identifying specific indicators of psychological well-being in the workplace that can be targeted via an individual-level intervention;
- An understanding of the theories that guide such interventions and the role of theory in their development;
- An exploration of a range of individual-level outcomes, assessed via standardised measures, and their associations with other individual and organisational outcomes.
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Griffiths, F.; Lindenmeyer, A.; Powell, J.; Lowe, P.; Thorogood, M. Why are health care interventions delivered over the internet? A systematic review of the published literature. J. Med. Internet Res. 2006, 8, e10. [Google Scholar] [CrossRef]
- Ebert, D.D.; Lehr, D.; Smit, F.; Zarski, A.C.; Riper, H.; Heber, E.; Cuijpers, P.; Berking, M. Efficacy and cost-effectiveness of minimal guided and unguided internet-based mobile supported stress-management in employees with occupational stress: A three-armed randomised controlled trial. BMC Public Health 2014, 14, 807. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, S.; Farmer, P. Thriving at Work: A Review of Mental Health and Employers. 2017. Available online: https://www.gov.uk/government/publications/thriving-at-work-a-review-of-mental-health-and-employers (accessed on 1 October 2019).
- Buchan, J.; Seccombe, I.; Charlesworth, A. Staffing Matters; Funding Counts. The Health Foundation, 2016. Available online: https://www.health.org.uk/publications/staffing-matters-funding-counts (accessed on 1 August 2019).
- NHS Staff Survey. 2018. Available online: http://www.nhsstaffsurveys.com/Page/1064/Latest-Results/2018-Results/ (accessed on 15 September 2019).
- Corbière, M.; Shen, J.; Rouleau, M.; Dewa, C.S. A systematic review of preventive interventions regarding mental health issues in organizations. Work 2009, 33, 81–116. [Google Scholar] [CrossRef] [PubMed]
- Tetrick, L.E.; Winslow, C.J. Workplace stress management interventions and health promotion. Annu. Rev. Organ. Psychol. Organ. Behav. 2015, 2, 583–603. [Google Scholar] [CrossRef]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69–93. [Google Scholar] [CrossRef]
- Bhui, K.S.; Dinos, S.; Stansfeld, S.A.; White, P.D. A synthesis of the evidence for managing stress at work: A review of the reviews reporting on anxiety, depression, and absenteeism. J. Environ. Public Health 2012, 2012, 515874. [Google Scholar] [CrossRef]
- Vanhove, A.J.; Herian, M.N.; Perez, A.L.; Harms, P.D.; Lester, P.B. Can resilience be developed at work? A meta-analytic review of resilience-building programme effectiveness. J. Occup. Organ. Psychol. 2016, 89, 278–307. [Google Scholar] [CrossRef]
- LaMontagne, A.D.; Martin, A.; Page, K.M.; Reavley, N.J.; Noblet, A.J.; Milner, A.J.; Keegel, T.; Smith, P.M. Workplace mental health: Developing an integrated intervention approach. BMC Psychiatry 2014, 14, 131. [Google Scholar] [CrossRef]
- Warr, P. Well-being and the workplace. In Employee Engagement Well-Being: The Foundations of Hedonic Psychology; Kahneman, D., Diener, E., Schwarz, N., Eds.; Russell-Sage: New York, NY, USA, 1999; pp. 392–412. [Google Scholar]
- Ilies, R.; Aw, S.S.; Pluut, H. Intraindividual models of employee well-being: What have we learned and where do we go from here? Eur. J. Work Organ. Psychol. 2015, 24, 827–838. [Google Scholar] [CrossRef]
- Carolan, S.; Harris, P.; Cavanagh, K. Improving employee well-being and effectiveness: Systematic review and meta-analysis of web-based psychological interventions delivered in the workplace. J. Med. Internet Res. 2017, 19, e271. [Google Scholar] [CrossRef]
- Murphy, L.R.; Sauter, S.L. The USA perspective: Current issues and trends in the management of work stress. Aust. Psychol. 2003, 38, 151–157. [Google Scholar] [CrossRef]
- Holman, D.; Johnson, S.; O’Connor, E. Stress management interventions: Improving subjective psychological well-being in the workplace. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Parks, K.M.; Steelman, L.A. Organizational wellness programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Richardson, K.M. Managing employee stress and wellness in the new millennium. J. Occup. Health Psychol. 2017, 22, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Memish, K.; Martin, A.; Bartlett, L.; Dawkins, S.; Sanderson, K. Workplace mental health: An international review of guidelines. Prev. Med. 2017, 101, 213–222. [Google Scholar] [CrossRef]
- Nexø, M.A.; Kristensen, J.V.; Grønvad, M.T.; Kristiansen, J.; Poulsen, O.M. Content and quality of workplace guidelines developed to prevent mental health problems: Results from a systematic review. Scand. J. Work Environ. Health 2018, 44, 443–457. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B.H.; Love, G.D. Positive health: Connecting wellbeing with biology. Philos. Trans. R. Soc. 2004, 359, 1383–1394. [Google Scholar] [CrossRef]
- Wright, E.M. Evaluation of a Web-Based Holistic Stress Reduction Pilot Program Among Nurse-Midwives. J. Holist. Nurs. 2018, 36, 159–169. [Google Scholar] [CrossRef]
- Robertson, I.T.; Cooper, C.L. Full engagement: The integration of employee engagement and psychological well-being. Leadersh. Organ. Dev. J. 2010, 31, 324–336. [Google Scholar] [CrossRef]
- Bockerman, P.; Bryson, A.; Ilmakunnas, P. Does high involvement management improve worker wellbeing? J. Econ. Behav. Organ. 2012, 84, 660–680. [Google Scholar] [CrossRef]
- Youssef, C.M.; Luthans, F. Positive organizational behavior in the workplace: The impact of hope, optimism, and resiliency. J. Manag. 2007, 33, 774–800. [Google Scholar] [CrossRef]
- Knight, C.; Patterson, M.; Dawson, J.F. Building work engagement: A systematic review and meta-analysis investigating the effectiveness of work engagement interventions. J. Organ. Behav. 2017, 38, 792–812. [Google Scholar] [CrossRef] [PubMed]
- Di Fabio, A. Positive Healthy Organizations: Promoting well-being, meaningfulness, and sustainability in organizations. Front. Psychol. 2017, 8, 1938. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, S.; Cooper, C.L. Towards organizational health: Stress, positive organizational behavior, and employee well-being. In Bridging Occupational, Organizational and Public Health; Bauer, G.F., Hämmig, O., Eds.; Springer: Dordrecht, The Netherlands, 2014; pp. 29–42. [Google Scholar] [CrossRef]
- Huang, J.; Wang, Y.; You, X. The job demands-resources model and job burnout: The mediating role of personal resources. Curr. Psychol. 2016, 35, 562–569. [Google Scholar] [CrossRef]
- Bakker, A.; Demerouti, E. Multiple levels in job demands-resources theory: Implications for employee well-being and performance. In Handbook of Well-Being; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Day, A.; Nielsen, K. What does our organization do to help our well-being? Creating healthy workplaces and workers. In An Introduction of Work and Organizational Psychology; Chmiel, N., Fraccaroli, F., West, M., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2017; in press. [Google Scholar]
- Nielsen, K.; Nielsen, M.B.; Ogbonnaya, C.; Känsälä, M.; Saari, E.; Isaksson, K. Workplace resources to improve both employee well-being and performance: A systematic review and meta-analysis. Work Stress 2017, 31, 101–120. [Google Scholar] [CrossRef]
- Nielsen, K.; Yarker, J.; Munir, F.; Bueltmann, U. IGLOO: An integrated framework for sustainable return to work in workers with common mental disorders. Work Stress 2018, 32, 400–417. [Google Scholar] [CrossRef]
- Halbesleben, J.R.B.; Neveu, J.P.; Paustian-Underdahl, S.C.; Westman, M. Getting to the “COR”: Understanding the role of resources in conservation of resources theory. J. Manag. 2014, 40, 1334–1364. [Google Scholar] [CrossRef]
- Wan Mohd Yunus, W.M.A.; Musiat, P.; Brown, J.S.L. Systematic review of universal and targeted workplace interventions for depression. Occup. Environ. Med. 2018, 75, 66–75. [Google Scholar] [CrossRef]
- Stratton, E.; Lampit, A.; Choi, I.; Calvo, R.A.; Harvey, S.B.; Glozier, N. Effectiveness of eHealth interventions for reducing mental health conditions in employees: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189904. [Google Scholar] [CrossRef]
- Michie, S.; Yardley, L.; West, R.; Patrick, K.; Greaves, F. Developing and Evaluating Digital Interventions to Promote Behaviour Change in Health and Health Care: Recommendations Resulting From an International Workshop. J. Med. Internet Res. 2017, 19, e232. [Google Scholar] [CrossRef]
- Hekler, E.B.; Michie, S.; Pavel, M.; Rivera, D.E.; Collins, L.M.; Jimison, H.B.; Garnett, C.; Parral, S.; Spruijt-Metz, D. Advancing models and theories for digital behavior change interventions. Am. J. Prev. Med. 2016, 51, 825–832. [Google Scholar] [CrossRef]
- Katelaar, S.M.; Nieuwenhuijsen, K.; Bolier, L.; Smeets, O.; Sluiter, J.K. Improving Work Functioning and Mental Health of Health Care Employees Using an E-Mental Health Approach to Workers’ Health Surveillance: Pretest-Posttest Study. Saf. Health Work 2014, 5, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Spadara, K.; Hunker, D. Exploring the effects of an online asynchronous mindfulness meditation intervention with nursing students on stress, mood and cognition: A descriptive study. Nurse Educ. Today 2016, 39, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Hersch, R.K.; Cook, R.F.; Deitz, D.K.; Kaplan, S.; Hughes, D.; Friesen, M.A.; Vezina, M. Reducing nurses’ stress: A randomized controlled trial of a web-based stress management program for nurses. Appl. Nurse Res. 2016, 32, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Bergin, M.; Chalder, T.; Wells, J.S. Web-based interventions for the management of stress in the workplace: Focus, form and efficacy. J. Occup. Health 2017, 59, 215–236. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Bishop, D.B. The role of behavioral science theory in development and implementation of public health interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef]
- Lippke, S.; Ziegelmann, J.P. Theory-based health behavior change: Developing, testing, and applying theories for evidence-based interventions. Appl. Psychol. 2008, 57, 698–716. [Google Scholar] [CrossRef]
- Jamal, F.; Fletcher, A.; Shackleton, N.; Elbourne, D.; Viner, R.; Bonell, C. The three stages of building and testing mid-level theories in a realist RCT: A theoretical and methodological case-example. Trials 2015, 16, 1–10. [Google Scholar] [CrossRef]
- Kersemaekers, W.; Rupprecht, S.; Wittmann, M.; Tamdjidi, C.; Falke, P.; Donders, R.; Speckens, A.; Kohls, N. A workplace mindfulness intervention may be associated with improved psychological well-being and productivity. A preliminary field study in a company setting. Front. Psychol. 2018, 9, 195. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration & explanation. BMJ 2015, 349, g7647. [Google Scholar]
- Higgins, J.P.T.; Green, S.E. Preparing a Cochrane review. In Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; Higgins, J.P.T., Green, S., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2008; pp. 11–30. [Google Scholar]
- Godfrey, C.M.; Harrison, M.B. CAN-SYNTHESIZE Is a Quick Reference Resource to Guide the Use of the Joanna Briggs Institute Methodology of Synthesis, Queen’s Joanna Briggs Collaboration Version 4.0. 2015. Available online: http://joannabriggs.org/assets/docs/jbc/operations/can-synthesise/CAN_SYNTHSISE_Resource-V4.pdf (accessed on 1 June 2019).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Joana Briggs Institute. The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Reviews-Checklist for Quasi-Experimenal Studies (Non-Randomised Experimental Studies). 2017. Available online: http://joannabriggs.org/assets/docs/critical-appraisal-tools/JBI_Quasi-Experimental_Appraisal_Tool2017.pdf (accessed on 1 June 2019).
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. A Product from the ESRC Methods Programme. Version 1; Lancaster University: Lancaster, UK, 2006. [Google Scholar]
- Petticrew, M.; Roberts, H. Systematic Reviews in Social Sciences: A Practical Guide; Wiley Blackwell: Oxford, UK, 2005. [Google Scholar]
- Grimshaw, J. A Guide to Knowledge Synthesis: A Knowledge Synthesis Chapter; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2010. [Google Scholar]
- Review Manager (RevMan) [Computer Program]. Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Danmark, 2014.
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: Chichester, UK, 2009. [Google Scholar]


{kind=link}
| Psychological Well-Being | ||
|---|---|---|
| Interventions targeting common mental well-being outcomes at work (e.g., perceived anxiety, depression), | Interventions targeting work-related well-being (e.g., perceived work stress, burnout, work-engagement) | Interventions targeting psychological indicators for mental well-being at work (e.g., positive psychological capital, resilience, self-efficacy, coping strategies, optimism). |
| Concepts and constructs for psychological well-being at work | ||
| Description of characteristics of interventions | ||
| Description of measures and outcomes (primary outcomes and associations with secondary outcomes | ||
| Research designs | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armaou, M.; Konstantinidis, S.; Blake, H. The Effectiveness of Digital Interventions for Psychological Well-Being in the Workplace: A Systematic Review Protocol. Int. J. Environ. Res. Public Health 2020, 17, 255. https://doi.org/10.3390/ijerph17010255
Armaou M, Konstantinidis S, Blake H. The Effectiveness of Digital Interventions for Psychological Well-Being in the Workplace: A Systematic Review Protocol. International Journal of Environmental Research and Public Health. 2020; 17(1):255. https://doi.org/10.3390/ijerph17010255
Chicago/Turabian StyleArmaou, Maria, Stathis Konstantinidis, and Holly Blake. 2020. "The Effectiveness of Digital Interventions for Psychological Well-Being in the Workplace: A Systematic Review Protocol" International Journal of Environmental Research and Public Health 17, no. 1: 255. https://doi.org/10.3390/ijerph17010255
APA StyleArmaou, M., Konstantinidis, S., & Blake, H. (2020). The Effectiveness of Digital Interventions for Psychological Well-Being in the Workplace: A Systematic Review Protocol. International Journal of Environmental Research and Public Health, 17(1), 255. https://doi.org/10.3390/ijerph17010255