Factors Associated with Knowledge, Attitude and Practices of Common Eye Diseases in General Population: A Multicenter Cross-Sectional Study from Pakistan

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Study Population and Recruitment
2.3. Statement of Ethical Approval
2.4. KAP Questionnaire
2.5. Statistical Analysis
3. Results
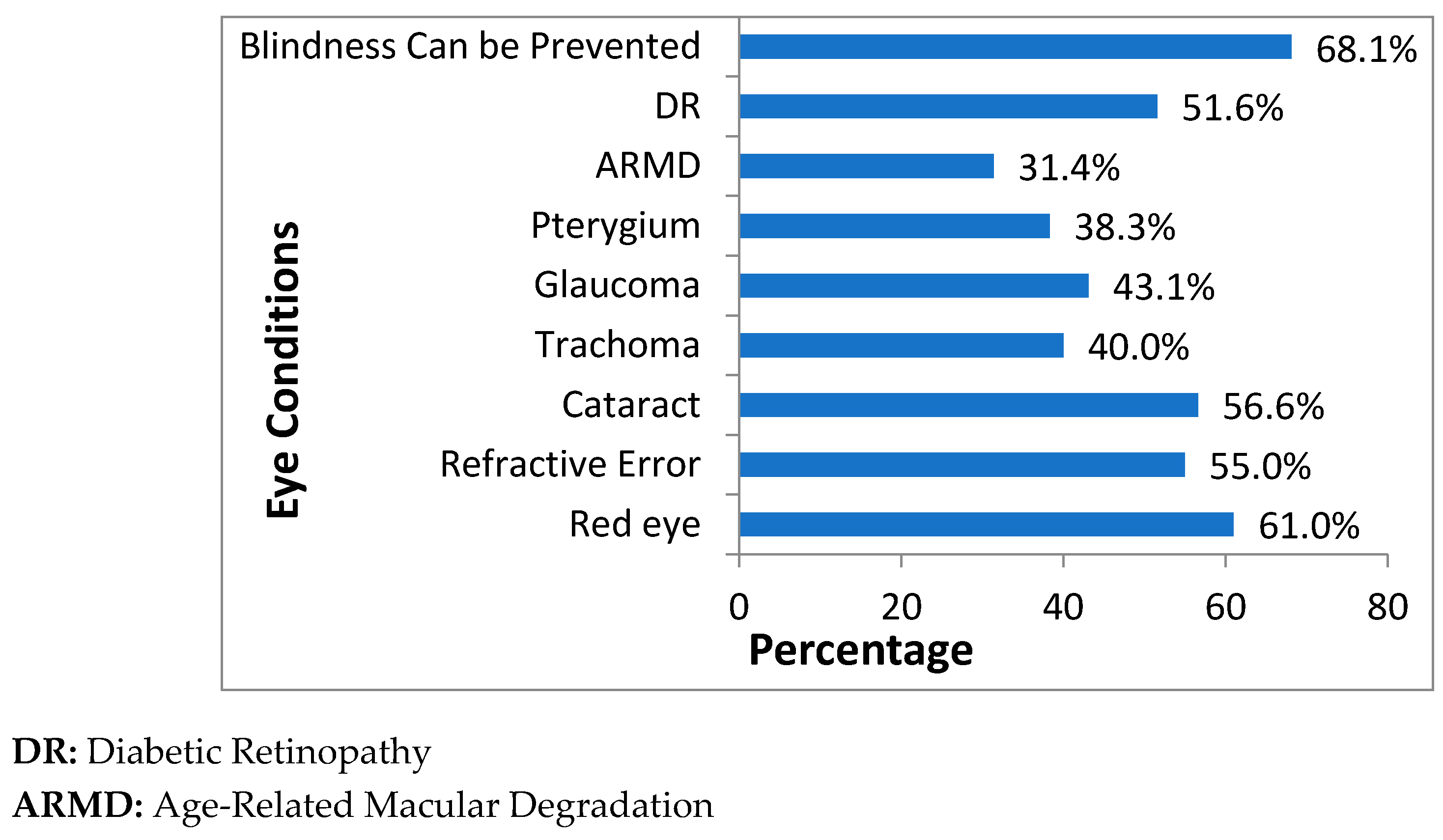
3.1. Knowledge Assessment
3.2. Demographic Association with Knowledge Score Using Rasch Analysis.
3.3. Attitudes
3.4. Practice
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stevens, G.A.; White, R.A.; Flaxman, S.R.; Price, H.; Jonas, J.B.; Keeffe, J.; Leasher, J.; Naidoo, K.; Pesudovs, K.; Resnikoff, S.; et al. Global prevalence of vision impairment and blindness: Magnitude and temporal trends, 1990–2010. Ophthalmology 2013, 120, 2377–2384. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Loon, S.C.; Saw, S.M. The epidemiology of age related eye diseases in Asia. Br. J. Ophthalmol. 2006, 90, 506–511. [Google Scholar] [CrossRef]
- Rajavi, Z.; Katibeh, M.; Ziaei, H.; Fardesmaeilpour, N.; Sehat, M.; Ahmadieh, H.; Javadi, M.A. Rapid assessment of avoidable blindness in Iran. Ophthalmology 2011, 118, 1812–1818. [Google Scholar] [CrossRef] [PubMed]
- Javadi, M.A.; Katibeh, M.; Rafati, N.; Dehghan, M.H.; Zayeri, F.; Yaseri, M.; Sehat, M.; Ahmadieh, H. Prevalence of diabetic retinopathy in Tehran province: A population-based study. BMC Ophthalmol. 2009, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Fotouhi, A.; Hashemi, H.; Mohammad, K. Eye care utilization patterns in Tehran population: A population based cross-sectional study. BMC Ophthalmol. 2006, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Jadoon, M.Z.; Dineen, B.; Bourne, R.R.; Shah, S.P.; Khan, M.A.; Johnson, G.J.; Gilbert, C.E.; Khan, M.D. Prevalence of blindness and visual impairment in Pakistan: The Pakistan National Blindness and Visual Impairment Survey. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4749–4755. [Google Scholar] [CrossRef] [PubMed]
- Dineen, B.; Bourne, R.R.A.; Jadoon, Z.; Shah, S.P.; Khan, M.A.; Foster, A.; Khan, M.D. Causes of blindness and visual impairment in Pakistan. The Pakistan national blindness and visual impairment survey. Br. J. Ophthalmol. 2007, 91, 1005–1010. [Google Scholar] [PubMed]
- Lau, J.T.F.; Lee, V.; Fan, D.; Lau, M.; Michon, J. Knowledge about cataract, glaucoma, and age related macular degeneration in the Hong Kong Chinese population. Br. J. Ophthalmol. 2002, 86, 1080–1084. [Google Scholar] [CrossRef]
- Marzieh, K.; Hossein, Z.; Elnaz, P.; Hamid-Reza, M.; Sara, H.M.K.; Armen, E.; Yaseri, M. Knowledge and Awareness of Age Related Eye Diseases: A Population-Based Survey. J. Ophthalmic Vis. Res. 2014, 9, 223–231. [Google Scholar]
- Altangerel, U.; Nallamshetty, H.S.; Uhler, T.; Fontanarosa, J.; Steinmann, W.C.; Almodin, J.M.; Chen, B.H.; Henderer, J.D. Knowledge about glaucoma and barriers to follow-up care in a community glaucoma screening program. Can. J. Ophthalmol. 2009, 44, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Livingston, P.M.; McCarty, C.A.; Taylor, H.R. Knowledge, attitudes, and self care practices associated with age related eye disease in Australia. Br. J. Ophthalmol. 1998, 82, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Hubley, J.; Gilbert, C. Eye health promotion and the prevention of blindness in developing countries: Critical issues. Br. J. Ophthalmol. 2006, 90, 279–284. [Google Scholar] [CrossRef]
- Klein, B.E. Overview of epidemiologic studies of diabetic retinopathy. Ophthalmic Epidemiol. 2007, 14, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Zaman, M.J.; Patel, A.; Jan, S.; Hillis, G.S.; Raju, P.K.; Neal, B.; Chow, C.K. Socio-economic distribution of cardiovascular risk factors and knowledge in rural India. Int. J. Epidemiol. 2012, 4, 1302–1314. [Google Scholar] [CrossRef]
- Norris, S.L.; Engelgau, M.M.; Narayan, K.M. Effectiveness of self-management training in type 2 diabetes: A systematic review of randomized controlled trials. Diabetes Care 2001, 24, 561–587. [Google Scholar] [CrossRef]
- Attebo, K.; Mitchell, P.; Cumming, R.; Smith, W. Knowledge and beliefs about common eye diseases. Aust. N. Z. J. Ophthalmol. 1997, 25, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Varma, R.; Lee, P.P.; Goldberg, I.; Kotak, S. An assessment of the health and economic burdens of glaucoma. Am. J. Ophthalmol. 2011, 152, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Huang, O.S.; Tay, W.T.; Tai, E.S.; Wang, J.J.; Saw, S.M.; Jeganathan, V.S.; Sandar, M.; Wong, T.Y. Lack of awareness amongst community patients with diabetes and diabetic retinopathy: The Singapore Malay eye study. Ann. Acad. Med. Singap. 2009, 38, 1048–1055. [Google Scholar] [PubMed]
- Muller, A.; Vu, H.T.; Ferraro, J.G.; Keeffe, J.E.; Taylor, H.R. Utilization of eye care services in Victoria. Clin. Exp. Ophthalmol. 2006, 34, 445–448. [Google Scholar] [CrossRef]
- Bylsma, G.W.; Le, A.; Mukesh, B.N.; Taylor, H.R.; McCarty, C.A. Utilization of eye care services by Victorians likely to benefit from eye care. Clin. Exp. Ophthalmol. 2004, 32, 573–577. [Google Scholar] [CrossRef]
- Memon, M.; Shaikh, S.A.; Shaikh, A.R.; Fahim, M.F.; Mumtaz, S.N.; Ahmed, N. An assessment of knowledge, attitude and practices (KAP) towards diabetes and diabetic retinopathy in a suburban town of Karachi. Pak. J. Med. Sci. 2015, 31, 183. [Google Scholar] [CrossRef] [PubMed]
- List of Tehsils Punjab, Pakistan. Available online: https://en.wikipedia.org/wiki/List_of_tehsils_of_Punjab,_Pakistan (accessed on 20 May 2017).
- Punjab, Pakistan. Available online: https://en.wikipedia.org/wiki/Punjab,_Pakistan (accessed on 20 May 2017).
- Gillani, A.H.; Amirul Islam, F.M.; Hayat, K.; Atif, N.; Yang, C.; Chang, J.; Qu, Z.; Fang, Y. Knowledge, Attitudes and Practices Regarding Diabetes in the General Population: A Cross-Sectional Study from Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 1906. [Google Scholar] [CrossRef] [PubMed]
- Ormsby, G.M.; Arnold, A.-L.; Busija, L.; Mörchen, M.; Bonn, T.S.; Keeffe, J.E. The Impact of Knowledge and Attitudes on Access to Eye-Care Services in Cambodia Asia-Pacific. J. Ophthalmol. 2012, 1, 331–335. [Google Scholar]
- Islam, F.M.A.; Chakrabarti, R.; Islam, S.Z.; Finger, R.P.; Critchley, C. Factors Associated with Awareness, Attitudes and Practices Regarding Common Eye Diseases in the General Population in a Rural District in Bangladesh: The Bangladesh Population-based Diabetes and Eye Study (BPDES). PLoS ONE 2015, 10, e0133043. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.H.; Chi, I.; Boey, K.W.; Ko, L.S.; Chou, K.L. Self-rated economic condition and the health of elderly persons in Hong Kong. Soc. Sci. Med. 2002, 55, 1415–1424. [Google Scholar] [CrossRef]
- Rasch, G. An item analysis which takes individual differences into account. Br. J. Math. Stat. Psychol. 1966, 19, 49–57. [Google Scholar] [CrossRef]
- Uddin, M.N.; Islam, F.M.A.; Al Mahmud, A. Psychometric evaluation of an interviewadministered version of the Kessler 10-item questionnaire (K10) for measuring psychological distress in rural Bangladesh. BMJ Open 2018, 8, e022967. [Google Scholar] [CrossRef]
- Dandona, R.; Dandona, L.; John, R.K.; McCarty, C.A.; Rao, G.N. Awareness of eye diseases in an urban population in southern India. Bull. World Health Organ. 2001, 79, 96–102. [Google Scholar]
- Islam, F.M.; Chakrabarti, R.; Dirani, M.; Islam, M.T.; Ormsby, G.; Wahab, M.; Critchley, C.; Finger, R.P. Knowledge, Attitudes and Practice of Diabetes in Rural Bangladesh: The Bangladesh Population Based Diabetes and Eye Study (BPDES). PLoS ONE 2014, 9, e110368. [Google Scholar] [CrossRef]
- Shrestha, M.K.; Guo, C.W.; Maharjan, N.; Gurung, R.; Ruit, S. Health literacy of common ocular diseases in Nepal. BMC Ophthalmol. 2014, 14, 2. [Google Scholar] [CrossRef]
- Zafar, S.; Badsha, H.; Mofti, A.; Delosantos, A.; Altares, J.; Matudio, G.; Kong, K.O. Efforts to increase public awareness may result in more timely diagnosis of rheumatoid arthritis. JCR: J. Clin. Rheumatol. 2012, 18, 279–282. [Google Scholar] [CrossRef]
- Alemayehu, A.M.; Belete, G.T.; Adimassu, N.F. Knowledge, attitude and associated factors among primary school teachers regarding refractive error in school children in Gondar city, Northwest Ethiopia. PLoS ONE 2018, 13, e0191199. [Google Scholar] [CrossRef] [PubMed]
- Aitaoto, N.; Braun, K.L.; Estrella, J.; Epeluk, A.; Tsark, J. Design and results of a culturally tailored cancer outreach project by and for Micronesian women. Prev. Chronic Dis. 2012, 9, E82. [Google Scholar] [CrossRef] [PubMed]
- Paudel, P.; Naduvilath, T.; Kovai, V.; Phuong, H.T.; Ho, S.M.; Wilson, D. Health literacy of adult Vietnamese population in relation to common eye conditions and factors for not seeking an eye examination. Eye Sci. 2016, 31, 130–139. [Google Scholar] [CrossRef]
- Rani, P.K.; Raman, R.; Subramani, S.; Perumal, G.; Kumaramanickavel, G.; Sharma, T. Knowledge of diabetes and diabetic retinopathy among rural populations in India, and the influence of knowledge of diabetic retinopathy on attitude and practice. Rural Remote Health 2008, 8, 838. [Google Scholar] [PubMed]


{kind=link}
| Variables | Number (N) | Percentage (%) | |
|---|---|---|---|
| Age (32.92 ± 11.4), years | |||
| 18–30 | 1134 | 56.2 | |
| 31–45 | 596 | 29.5 | |
| 46–60 | 242 | 12.0 | |
| More than 60 | 47 | 2.3 | |
| Gender | |||
| Male | 1309 | 64.8 | |
| Female | 710 | 35.2 | |
| Residence | |||
| Urban | 980 | 48.5 | |
| Rural | 1039 | 51.5 | |
| Education | |||
| Nil | 62 | 3.1 | |
| 1–5 | 420 | 20.8 | |
| 6–10 | 464 | 23.0 | |
| 10–12 | 333 | 16.5 | |
| More than Intermediate | 740 | 36.6 | |
| Occupation | |||
| Student | 828 | 41.0 | |
| Farmer (kisan) | 276 | 13.7 | |
| Laborer | 184 | 9.1 | |
| Housewife | 218 | 10.8 | |
| Teacher | 194 | 9.6 | |
| Business man | 222 | 10.5 | |
| Other | 53 | 2.6 | |
| None | 43 | 2.1 | |
| Socioeconomic Status (SES) | |||
| Inadequate resources for complete year | 222 | 11.0 | |
| Inadequate for a few times | 462 | 22.9 | |
| Balanced | 1122 | 55.6 | |
| Adequate resources for most of the time | 213 | 10.5 | |
| Disease Related Questions | Gender | Age Group | Education Status | ||||||||
| Male n = 1309 (%) | Female n = 710 (%) | 18–30 n = 1134 (%) | 31–45 n = 596 (%) | 46–60 n = 242 (%) | >60 n = 47 (%) | Nil n = 62 (%) | 1–5 n = 420 (%) | 6–10 n = 464 (%) | 10–12 n = 333 (%) | More Than Inter n = 740 (%) | |
| Red eye | 738 (56.4) | 493 (69.4) | 758 (66.8) | 307 (51.5) | 133 (54.9) | 33 (70.2) | 24 (38.7) | 198 (47.1) | 254 (54.7) | 222 (66.7) | 533 (72.0) |
| Refractive error/Blurred vision | 648 (49.5) | 461 (64.9) | 666 (58.8) | 295 (49.5) | 129 (53.3) | 19 (40.4) | 36 (58) | 203 (48.3) | 197 (42.4) | 197 (59.1) | 476 (64.3) |
| Cataract | 674 (51.5) | 470 (66.2) | 707 (62.3) | 298 (50.0) | 116 (47.9) | 23 (48.9) | 30 (48.4) | 190 (45.2) | 203 (43.7) | 226 (67.9) | 495 (66.9) |
| Trachoma | 438 (33.5) | 368 (51.8) | 565 (49.8) | 167 (28.0) | 64 (25.4) | 10 (21.3) | 17 (27.4) | 91 (21.6) | 128 (27.6) | 166 (49.8) | 404 (54.6) |
| Glaucoma | 502 (38.3) | 369 (52.0) | 565 (49.8) | 220 (36.9) | 70 (28.9) | 16 (34.0) | 20 (32.2) | 135 (32.1) | 160 (34.5) | 169 (36.4) | 387 (52.3) |
| Pterygium | 421 (32.2) | 352 (49.6) | 539 (47.5) | 171 (28.7) | 53 (21.9) | 10 (21.3) | 12 (19.3) | 109 (25.9) | 138 (29.7) | 153 (33.0) | 361 (48.8) |
| Age-related macular degradation. | 362 (27.6) | 273 (38.4) | 416 (36.7) | 164 (27.5) | 45 (18.6) | 10 (21.3) | 4 (6.4) | 105 (25.0) | 99 (21.3) | 121 (36.3) | 306 (41.3) |
| Diabetic retinopathy | 607 (46.4) | 436 (61.4) | 610 (53.8) | 283 (47.5) * | 129 (53.3) * | 21 (44.7) * | 20 (32.2) | 179 (42.6) | 215 (46.3) | 186 (55.8) | 443 (59.9) |
| Vision loss can be prevented | 837 (63.9) | 539 (75.9) | 821 (72.4) | 366 (61.4) | 157 (64.8) | 32 (68.1) | 42 (67.7) | 247 (58.8) | 291 (62.7) | 239 (71.8) | 557 (75.3) |
| Residence | SES | ||||||||||
| Urban n = 980 (%) | Rural n = 1039 (%) | Inadequate Resources for Complete Year n = 222 (%) | Inadequate for a Few Times n = 462 (%) | Adequate Resources for Most of the Time n = 213 (%) | |||||||
| Red eye | 534 (54.5) | 697 (67.1) | 117 (52.7) | 205 (44.4) | 137 (64.3) | ||||||
| Refractive error/Blurred vision | 517 (52.7) * | 592 (57.0) * | 122 (54.9) | 205 (44.4) | 120 (56.3) | ||||||
| Cataract | 583 (59.5) | 561 (54) | 116 (52.2) * | 274 (59.3) * | 123 (57.7) * | ||||||
| Trachoma | 410 (41.8) * | 396 (38.1) * | 100 (54.0) | 159 (34.4) | 103 (61.0) | ||||||
| Glaucoma | 422 (43.1) * | 449 (43.2) * | 112 (50.4) | 184 (39.8) | 114 (53.5) | ||||||
| Pterygium | 391 (39.9) * | 382 (36.8) * | 121 (54.5) | 161 (34.8) | 89 (41.8) | ||||||
| Age-related macular degradation | 329 (33.6) | 306 (29.4) | 96 (43.2) | 151 (32.7) | 67 (31.4) | ||||||
| Diabetic retinopathy | 485 (49.5) * | 558 (53.7) * | 106 (47.7) | 212 (45.9) | 122 (57.3) | ||||||
| Vision loss can be prevented | 642 (65.5) | 734 (70.6) | 140 (63.1) | 261 (56.5) | 154 (72.3) | ||||||
| Demographic Variable | Red Eye | Refractive Error | Cataract | Trachoma | Glaucoma | Pterygium | Age-related Macular Degradation | Diabetic Retinopathy | Vision Loss Can Be Prevented |
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| 18–30 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 31–45 | 0.48 (0.28, 0.97) | 1.31 (0.70, 2.44) | 0.92 (0.50, 1.70) | 1.71 (0.82, 3.58) | 1.20 (0.63, 2.28) | 1.75 (0.88, 3.46) | 1.06 (0.50, 2.23) | 0.72 (0.42, 1.47) | 0.82 (0.44, 1.66) |
| 45–60 | 0.34 (0.17, 0.68) | 01.24 (0.68, 2.36) | 0.84 (0.46, 1.55) | 1.09 (0.52, 2.28) | 0.96 (0.50, 1.82) | 1.09 (0.52, 2.27) | 1.00 (0.48, 2.09) | 0.88 (0.47, 1.62) | 0.67 (0.35, 1.29) |
| More than 60 | 0.45 (0.22, 0.92) | 1.51 (0.79, 2.88) | 0.90 (0.47, 1.69) | 1.21 (0.56, 2.61) | 0.72 (0.37, 1.42) | 0.88 (0.41, 1.91) | 0,71 (0.32, 1.56) | 1.34 (0.71, 2.53) | 0.81 (0.41, 1.61) |
| Gender | |||||||||
| Male | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Female | 1.55 (1.25, 1.92) | 1.69 (1.38, 2.07) | 1.54 (1.25, 1.88) | 1.68 (1.37, 2.07) | 1.51 (1.23, 1.84) | 1.83 (1.49,2.25) | 1.42 (1.15, 1.75) | 1.75 (1.43, 2.14) | 1.63 (1.30, 2.03) |
| Residence | |||||||||
| Urban | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Rural | 2.08 (1.71, 2.55) | 1.27 (1.05, 1.53) | 0.90 (0.75, 1.09) | 1.08 (0.89, 1.31) | 1.19 (0.98, 1.43) | 1.07 (0.88, 1.30) | 0.98 (0.80, 1.20) | 1.28 (1.06, 1.54) | 1.37 (1.12, 1.67) |
| Education | |||||||||
| Nil | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 0–5 | 1.69 (0.91, 2.83) | 0.70 (0.40, 1.22) | 0.88(0.51, 1.51) | 0.6 (0.36, 1.24) | 0.99 (0.55, 1.77) | 1.40 (0.71, 2.77) | 4.78 (1.68, 13.58) | 1.695 (0.95, 3.01) | 0.72 (0.40, 1.29) |
| 6–10 | 2.54 (1.45, 4.51) | 0.61 (0.35, 1.07) | 0.85 (0.49, 1.46) | 1.00 (0.54, 1.85) | 1.23 (0.69, 2.19) | 2.00 (1.01, 3.94) | 4.32 (1.51, 12.33) | 2.30 (1.28, 4.10) | 0.93 (0.52, 1.68) |
| 10–12 | 3.94 (2.16, 7.18) | 1.04 (0.58, 1.85) | 2.09 (1.18, 3.70) | 1.90 (1.02, 3.55) | 1.82 (1.00, 3.31) | 2.85 (1.42, 5.71) | 7.40 (2.58, 21.21) | 3.03 (1.67, 5.53) | 1.23 (0.66, 2.27) |
| More than Intermediate | 4.66 (2.60, 8.33) | 1.24 (0.71, 2.16) | 2.07 (1.19, 3.60) | 2.29 (1.25, 4.21) | 1.98 (1.11, 3.54) | 3.34 (1.69, 6.58) | 9.79 (3.45, 27.80) | 3.64 (2.03, 6.52) | 1.36 (0.75, 2.47) |
| SES | |||||||||
| Insufficient funds for whole year | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Insufficient for some time | 0.890 (0.59, 1.33) | 1.20 (0.81, 1.78) | 1.11 (0.74, 1.64) | 1.31 (0.87, 1.97) | 1.16 (0.78, 1.72) | 2.47 (1.64, 3.70) | 2.13 (1.52, 3.49) | 0.91 (0.61, 1.35) | 0.83 (0.54, 1.26) |
| Balanced | 0.63 (0.44, 0.90) | 0.82 (0.58, 1.16) | 1.55 (1.09, 2.20) | 0.85 (0.59, 1.21) | 0.76 (0.54, 1.08) | 1.08 (0.76, 1.54) | 1.50 (1.04, 2.17) | 0.85 (0.60, 1.20) | 0.64 (0.44, 0.92) |
| Sufficient funds for most of times | 1.53 (1.10, 2.11) | 1.32 (0.97, 1.80) | 1.18 (0.87, 1.61) | 0.86 (0.63, 1.18) | 0.69 (0.51, 0.94) | 0.94 (0.68, 1.28) | 1.03 (0.74 1.43) | 1.03 (0.75, 1.39) | 1.21 (0.86, 1.69) |
| Variable | Un Adjusted β (95% CI) | p | Adjusted β (95% CI) | p |
|---|---|---|---|---|
| Age | −0.02 (−0.03, −0.02) | <0.001 | −0.008 (−0.01, −0.002) | 0.010 |
| Gender | 0.72 (0.59, 0.86) | <0.001 | 0.53 (0.39, 0.66) | <0.001 |
| Residence | 0.03 (−0.09, 0.16) | 0.586 | 0.22 (0.09, 0.34) | 0.001 |
| Education | 0.37 (0.32, 0.42) | <0.001 | 0.31 (0.25, 0.37) | <0.001 |
| SES | 0.09 (0,01, 0.17) | 0.030 | −0.04 (−0.11, 0.03) | 0.297 |
| Variable | No | Yes | AOR (95% CI) | p | |||
|---|---|---|---|---|---|---|---|
| N | N | % | N | % | |||
| Age, years | |||||||
| 18–30 | 1134 | 179 | 15.8 | 955 | 84.2 | 1 | |
| 31–45 | 596 | 136 | 22.8 | 460 | 77.3 | 1.47 (0.72, 3.09) | 0.032 |
| 46–60 | 242 | 37 | 15.3 | 205 | 84.7 | 1.06 (0.59, 2.17) | 0.227 |
| More than 60 | 47 | 11 | 23.4 | 36 | 76.6 | 1.69 (0.78, 3.66) | 0.868 |
| Gender | |||||||
| Male | 1309 | 243 | 18.5 | 1066 | 81.5 | 1 | |
| Female | 710 | 120 | 16.9 | 590 | 83.1 | 0.98 (0.75, 1.27) | 0.879 |
| Residence | |||||||
| Urban | 980 | 185 | 18.9 | 795 | 81.1 | 1 | |
| Rural | 1039 | 178 | 17.1 | 861 | 82.9 | 1.21 (0.95, 1.54) | 0.109 |
| Education | |||||||
| Nil | 62 | 4 | 6.4 | 58 | 93.6 | 1 | |
| 1–5 | 420 | 94 | 22.4 | 326 | 77.6 | 0.25 (0.08, 0.72) | <0.001 |
| 6–10 | 464 | 106 | 22.8 | 358 | 77.2 | 0.24 (0.08, 0.70) | 0.010 |
| 10–12 | 333 | 62 | 18.6 | 271 | 81.4 | 0.32 (0.11, 0.93) | 0.009 |
| More than Intermediate | 740 | 97 | 13.1 | 643 | 86.9 | 0.46 (0.16, 1.33) | 0.152 |
| SES | |||||||
| Inadequate resources for complete year | 222 | 55 | 24.8 | 167 | 75.2 | 1 | |
| Inadequate for a few times | 462 | 88 | 19.0 | 374 | 81.0 | 1.02 (0.64, 1.61) | 0.925 |
| Balanced | 1122 | 171 | 15.2 | 951 | 84.8 | 1.58 (1.05, 2.39) | 0.027 |
| Adequate resources for most of the time | 213 | 49 | 23.0 | 164 | 77.0 | 1.82 (1.26, 2.62) | 0.001 |
| Variable | N | More Than Once in a Year | At Least Once in a Year | When You Think You Have Eye Disease | Never | p |
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |||
| Age, years | ||||||
| 18–30 | 1134 | 241 (21.2) | 270 (23.8) | 375 (33.2) | 248 (21.8) | <0.001 |
| 31–45 | 596 | 72 (12.1) | 136 (22.0) | 245 (41.1) | 143 (23.9) | |
| 46–60 | 242 | 30 (12.4) | 19 (7.8) | 111 (45.9) | 82 (33.9) | |
| More than 60 | 47 | 4 (8.5) | 10 (21.3) | 22 (46.8) | 11 (23.4) | |
| Gender | ||||||
| Male | 1309 | 207 (15.8) | 235 (18.0) | 527 (40.2) | 340 (26.0) | <0.001 |
| Female | 710 | 140 (19.7) | 200 (28.2) | 226 (31.8) | 144 (20.3) | |
| Residence | ||||||
| Urban | 980 | 191 (19.5) | 233 (23.8) | 375 (38.2) | 181 (18.5) | <0.001 |
| Rural | 1039 | 156 (15.0) | 202 (19.4) | 378 (36.4) | 303 (29.2) | |
| Education | ||||||
| Nil | 62 | 11 (17.7) | 2 (3.2) | 32 (51.7) | 17 (27.4) | <0.001 |
| 1–5 | 420 | 75 (17.9) | 67 (15.9) | 158 (37.6) | 120 (28.6) | |
| 6–10 | 464 | 38 (8.2) | 135 (29.1) | 167 (36.0) | 124 (26.7) | |
| 10–12 | 333 | 56 (16.8) | 69 (20.8) | 134 (40.2) | 74 (22.2) | |
| More than Intermediate | 740 | 167 (22.5) | 162 (21.9) | 262 (35.5) | 149 (20.1) | |
| SES | ||||||
| Inadequate resources for complete year | 222 | 73 (32.9) | 26 (11.7) | 80 (36.0) | 43 (19.4) | <0.001 |
| Inadequate for a few times | 462 | 71 (15.4) | 133 (28.8) | 183 (36.9) | 75 (16.2) | |
| Balanced | 1122 | 159 (14.2) | 212 (18.9) | 417 (37.2) | 334 (29.7) | |
| Adequate resources for most of the time | 213 | 44 (20.6) | 64 (30.0) | 73 (34.4) | 32 (15.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, M.; Gillani, A.H.; Amirul Islam, F.M.; Ji, W.; Hayat, K.; Li, Z.; Akbar, J.; Ahmed, A.B.; Azam, A.; Masood, I.; et al. Factors Associated with Knowledge, Attitude and Practices of Common Eye Diseases in General Population: A Multicenter Cross-Sectional Study from Pakistan. Int. J. Environ. Res. Public Health 2019, 16, 1568. https://doi.org/10.3390/ijerph16091568
Zhao M, Gillani AH, Amirul Islam FM, Ji W, Hayat K, Li Z, Akbar J, Ahmed AB, Azam A, Masood I, et al. Factors Associated with Knowledge, Attitude and Practices of Common Eye Diseases in General Population: A Multicenter Cross-Sectional Study from Pakistan. International Journal of Environmental Research and Public Health. 2019; 16(9):1568. https://doi.org/10.3390/ijerph16091568
Chicago/Turabian StyleZhao, Mingyue, Ali Hassan Gillani, Fakir Mohammad Amirul Islam, Wenjing Ji, Khezar Hayat, Zongjie Li, Jamshaid Akbar, Abu Bakar Ahmed, Ans Azam, Imran Masood, and et al. 2019. "Factors Associated with Knowledge, Attitude and Practices of Common Eye Diseases in General Population: A Multicenter Cross-Sectional Study from Pakistan" International Journal of Environmental Research and Public Health 16, no. 9: 1568. https://doi.org/10.3390/ijerph16091568
APA StyleZhao, M., Gillani, A. H., Amirul Islam, F. M., Ji, W., Hayat, K., Li, Z., Akbar, J., Ahmed, A. B., Azam, A., Masood, I., & Fang, Y. (2019). Factors Associated with Knowledge, Attitude and Practices of Common Eye Diseases in General Population: A Multicenter Cross-Sectional Study from Pakistan. International Journal of Environmental Research and Public Health, 16(9), 1568. https://doi.org/10.3390/ijerph16091568