Systemic Barriers and Equitable Interventions to Improve Vegetable and Fruit Intake in Children: Interviews with National Food System Actors

 ,
, 
Abstract
:1. Introduction
- current systemic barriers to meeting the fruit and vegetable (FV) intake guidelines among New Zealand children aged 2–14 years; and
- acceptable and equitable options for systemic interventions which would improve nutrition by increasing children’s consumption of FVs.
2. Materials and Methods
2.1. Cognitive Mapping Interviews
2.2. Procedures
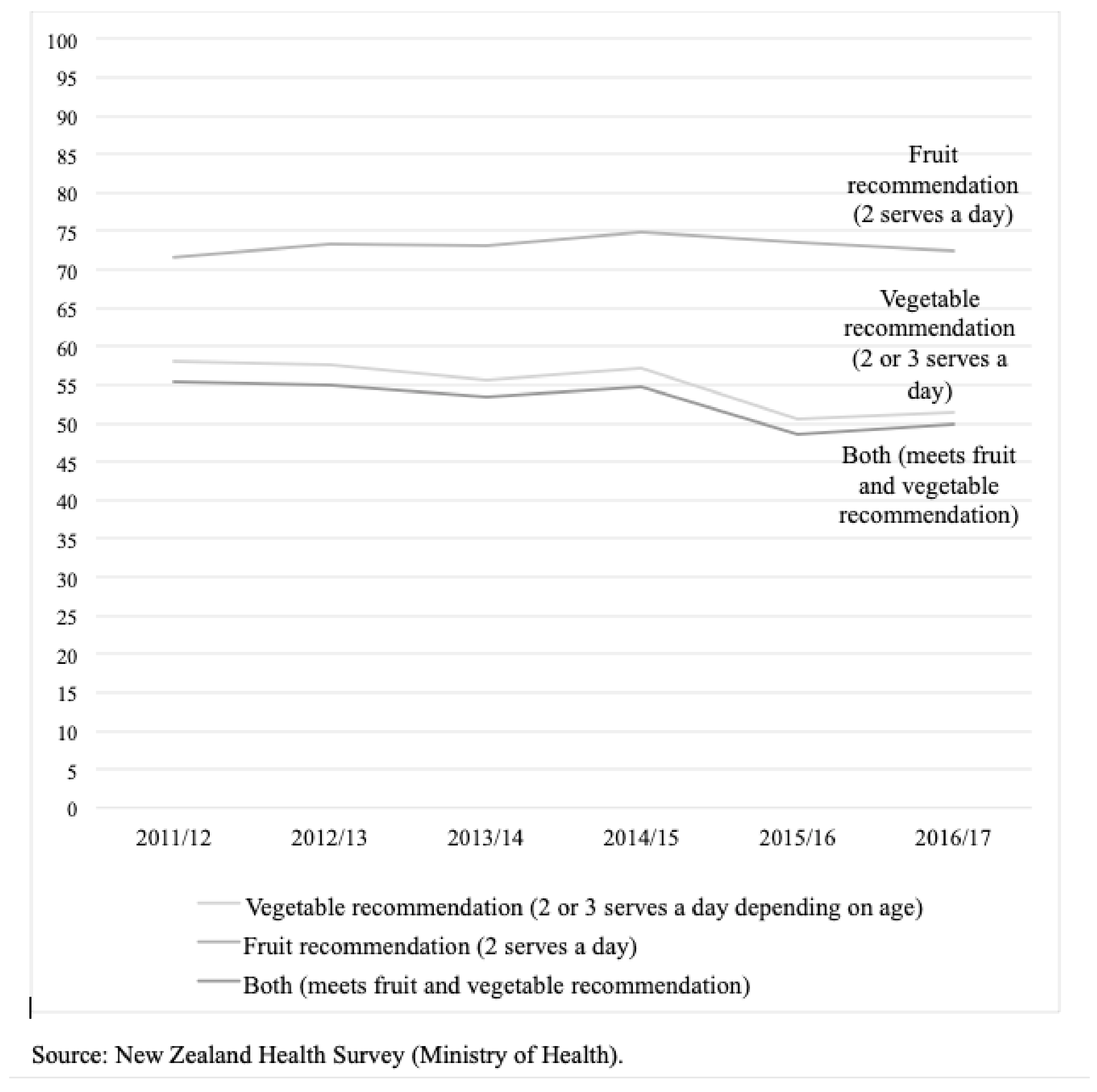
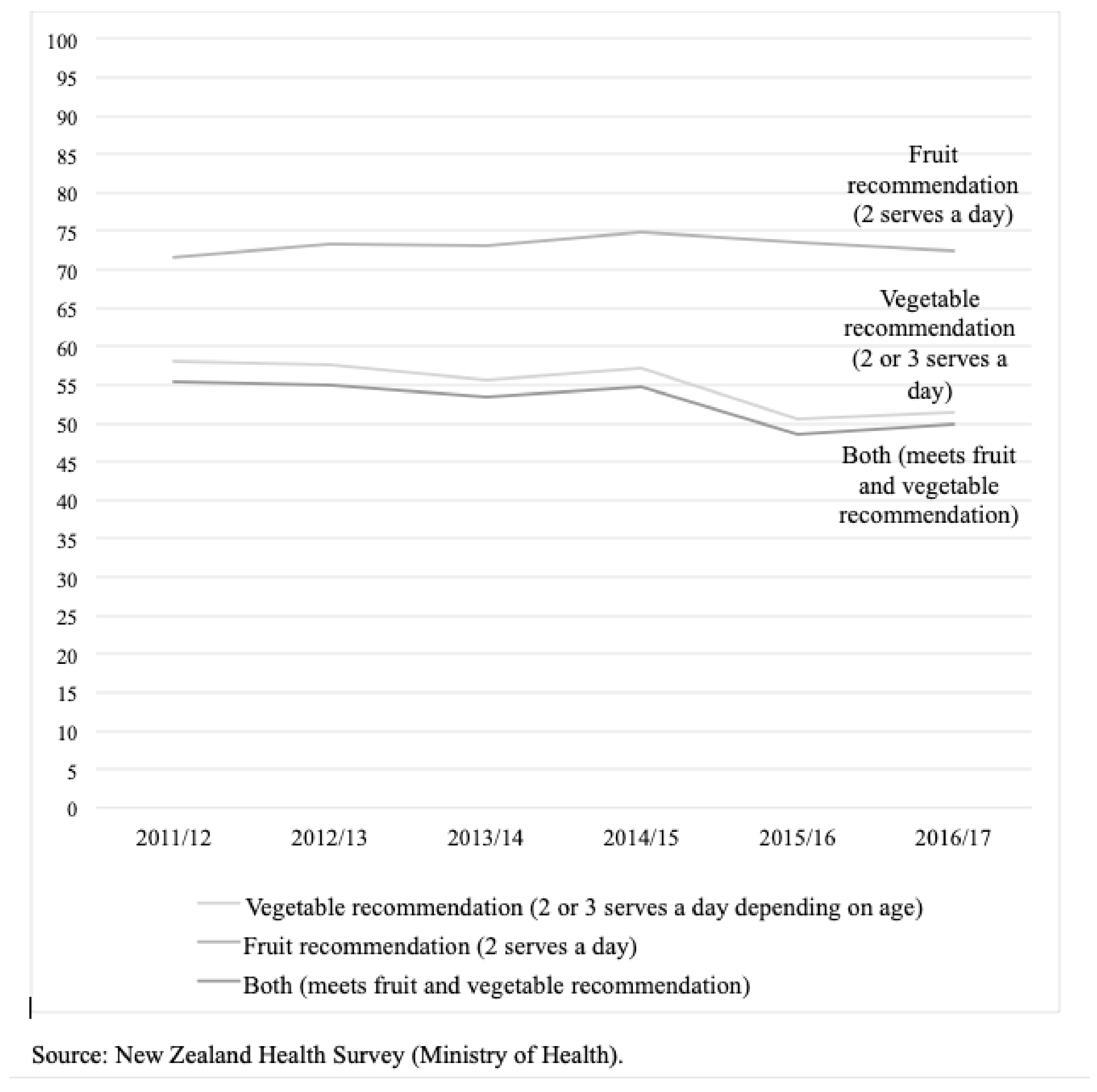
- We can see (in the graph) that in the past 5 years, fruit intake hasn’t changed and vegetable intake has declined overall, with a pronounced drop in 2015. What do you consider to be the primary causes of these patterns?
- What do you think are the consequences if these patterns continue?
- What would be the consequence if these patterns changed and increasing numbers of children consumed the recommended amount of fruit and vegetables?
- What would need to happen to bring these lines up to 100%?
- Fruit and vegetable intake is lowest among children who live in low-income communities. Why do you think this is, and would they require different interventions to see these patterns change?
- Is there anything else you would like to add on this issue before we finish?
2.3. Analysis
3. Results
3.1. Description of Interview Participants
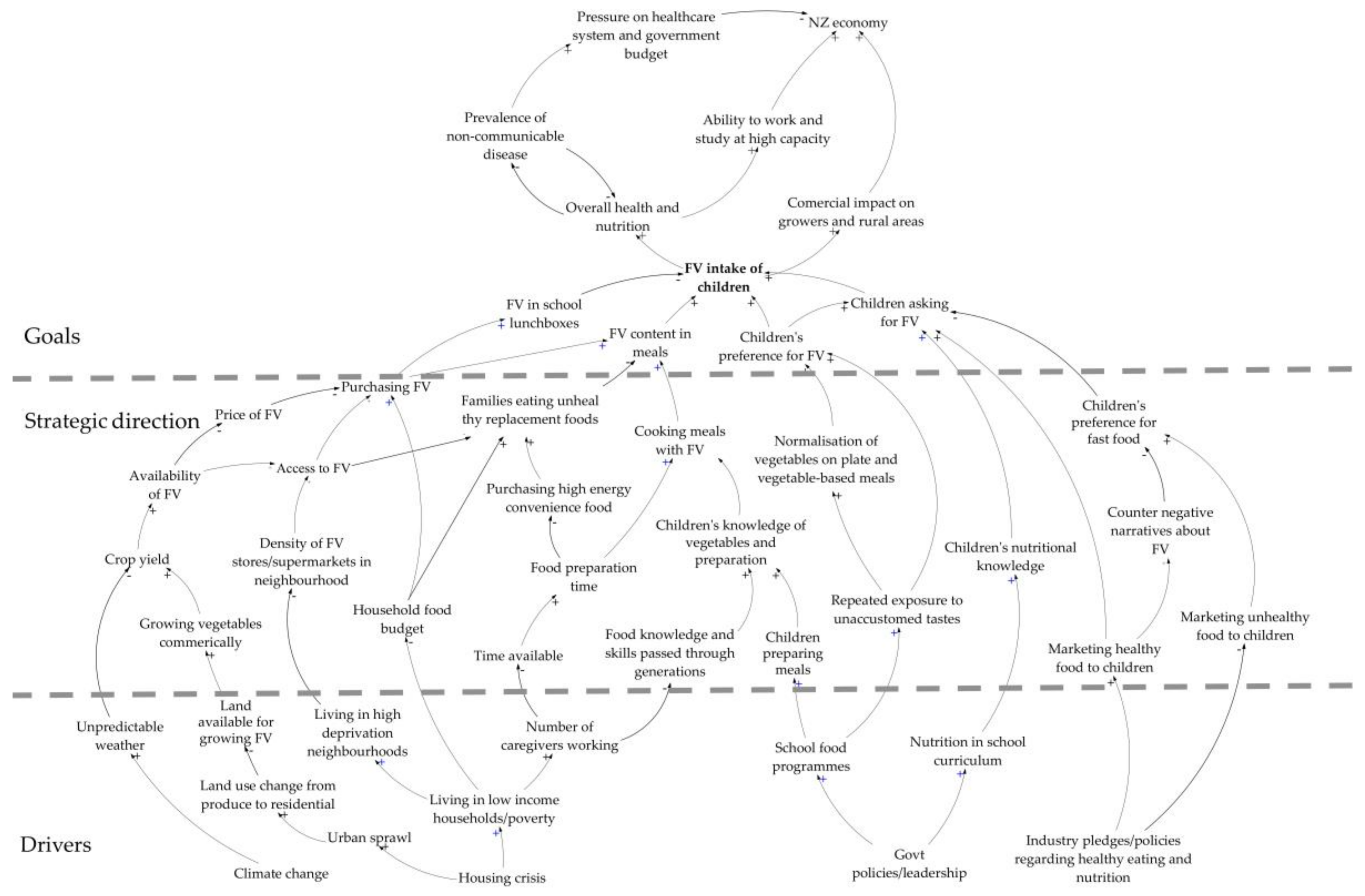
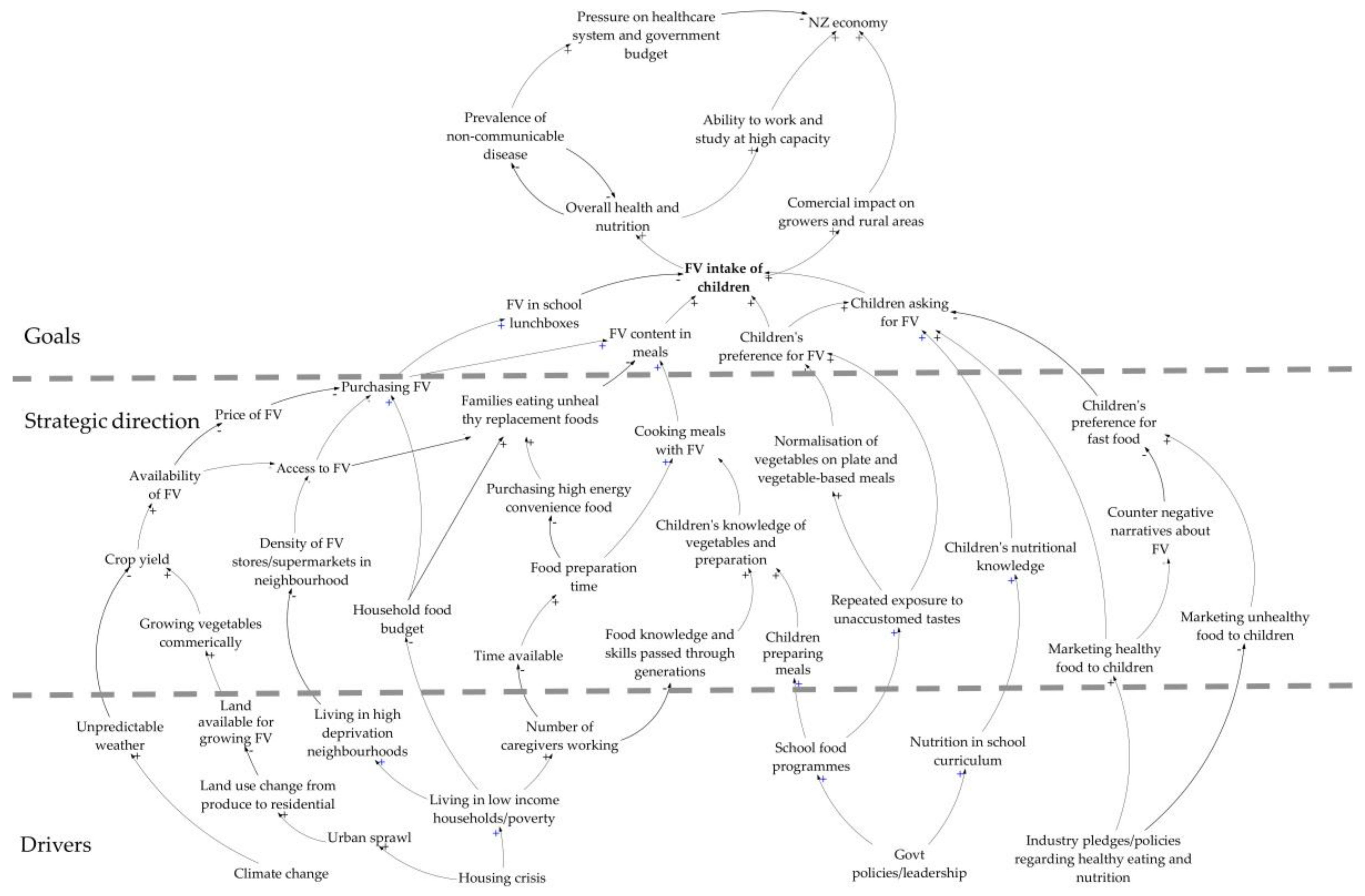
3.2. Themes from the Interview Maps and the Composite Summary Map
3.3. Consequences of Low Fruit and Vegetable Intake in Children
“Lack of vegetable intake, in particular, is probably like a proxy for diet poverty as a whole. It’s obvious the nutrients that vegetables provide, but looking wider than that, lots of processed foods (create) micronutrient deficiencies in children, and their ability to grow. There’s a knock-on effect too, oral health… chronic disease is that end-point, but that middle point in between is a less healthy group of children and adolescents that have poorer–not just health outcomes, but educational outcomes too.”—Interview 112
“We already have really high rates of non-communicable diseases like obesity, and diabetes, and malnutrition. And I think that those are just going to escalate. And those children are going to grow up to have children who will follow the same habits and are also just as likely to be in maybe low-income areas if they already were in low-income areas. I think the problem will escalate. Absolutely.”—Interview 109
“In some ways, it’s a fairly fragmented industry. What we hear from our growers, which are generally large farming operations, may not be the overall sentiment of the grower community. We’re selling plenty. They’re selling plenty. We don’t see what’s going on in the whole market... I’d imagine the smaller, less efficient growers would be most impacted by a reduction in volume…”—Interview 104
“If you have a look, there’s massive consolidation in the grower base in New Zealand. When I started 30 years ago in the industry, there were 60, 70 cauliflower growers in Pukekohe. Today there’s six. And there has had to be consolidation so that they can survive and become efficient. It’s all about volume. But you get to the point where you can’t be any more efficient.”—Interview 105
3.4. Barriers to Fruit and Vegetable Intake in Children
3.4.1. Fruit and Vegetable Prices
“We’ve had lots of strong rains and storms coming through, and I’ve read about rotting kumara in the ground, rather than it getting to be dug up and sold, therefore, driving up the cost. Things like cauliflower; that’s been crazy.”—Interview 107
“One of the things that really, really worries me that I think could help, is that retailers don’t make any money in grocery. It’s all about shelf space, volume, and small margins. Fresh food is where retailers make their money… in (grocery) it’s all about a price point. They pretty much do it at either cost or a small margin. Coca-Cola or Arnott’s or Greg’s or whoever will buy the shelf. The middle shelves at eye level or at the end of the aisle, the supermarkets will get thousands and thousands of dollars for it. They make their money out of selling shelf space, not the product themselves. In fresh foods that’s where they make their margins. Produce makes up about 10% of the store’s turnover but probably close to 25% to 30% of their margin. I have no issues with the margin that retailers make. I mean, they’re running big businesses… it just seems a little bit back to front that all the stuff that’ll kill you is cheap and the supermarkets don’t make their margin on it. Versus all the stuff that’s healthy and fresh is where they make their margin.”—Interview 105
“There’s been a lot of press about fruit and fresh veg prices, and there hasn’t been anybody jumping up and down about increasing prices of fast food, have they? I tend to go 2.5 kilos of potatoes at 8 bucks versus other vegetables or other things for a kilo, there might’ve been a 5% increase and it’s way out in front, but it’s still bloody good value compared to other things.”—Interview 115
“Everybody’s been saying price... And I think at that time, yeah, sure, cauliflower was $10 or whatever it was, but you could still buy lettuce for 99 cents… When people are talking about the price, they’re not talking about if it’s old-season, new-season, the quality or anything like that.”—Interview 116
3.4.2. Limited Household Food Budgets
“If you look back at the socioeconomic deprivation over the recent years and housing costs, that although our employment has been fairly good, the difficulty of bringing up a family on current incomes where there hasn’t been much of a move while costs have gone up and up, I would think that financial stress plays a huge part”—Interview 103
“The reason why [we have low FV intake in children] is because of families and children living in low-income situations and living in poverty. Knowing that food is generally the last item that people buy, so that’s when they’ve got the pay packet each week, whether it’s from benefits, or paid work, or tax credits, it pays the rent, pays the bills, pays the outstanding debt. Food is the last items that you choose. When I go to the supermarket and look at fruit, how much you pay and what you get, I can see why families would choose to get high-energy food, and easier foods to prepare.”—Interview 101
3.4.3. Advertising and Promotion of Unhealthy Food
“Marketing and advertising contributes to children asking for packaged food. The food environment is cluttered with mixed messages, and where nutrition literacy is lower, parents and caregivers are unsure of what to give their children. The perceived quick and easy option is processed food.”—Interview 110
“The other thing I was thinking of was looking at policies around advertising and sponsorship. You see those big sponsors still sponsoring huge events, like Coca-Cola Christmas in the Park. I don’t know if we can even match that, but that’s what we’re up against.”—Interview 111
3.4.4. Children’s Food Preferences
“It’s been known for a long time that children have a preference for things that are slightly sweeter so apart from the fact that the number of serves required of fruit a day is lower than that of vegetables… most kids prefer the flavour of fruit to vegetables because it’s sweeter.”—Interview 113
3.4.5. Limited Availability of Fresh Produce
“Thinking of places like (suburb), they don’t have a supermarket anymore due to it being earthquake-prone and for whatever reasons, it has financially not been viable. Whereas, there’s a laundromat, and a dairy, and a couple of hot roast shops and things like that. The dairy might have a few manky old bits of fruit, but there’s not anywhere for them to go in walking distance to get fresh fruit and vegetables.”—Interview 107
“You go to (suburb) and look in the mall there… every second shop is a fast food takeaway. And very little in the way of fresh food. But you’ve also got the advertising which promotes junk food, sugary drinks, all that sort of thing everywhere.”—Interview 103
3.4.6. Lack of Time for Food Preparation and Skills/Knowledge
“The misconception that we hear is that people living in poverty or people on low incomes have lots of time. But that’s not true, especially if you’re in the welfare system, you’ve got all these appointments to go to. If you’ve got children, you need to look after your children. That involves time. And you may have other family members that you’re looking after too.”—Interview 101
“More and more mums are working full time now. They’re not in the house to prepare meals. It’s like everybody gets home at 5, 6 o’clock. Everybody’s tired. Everybody wants to eat quickly. You just don’t have time to do it.”—Interview 112
“Although fruit and vegetables are quite convenient, there’s an idea that takeaway foods are more convenient, and you wouldn’t be getting lots of vegetables (in takeaways) unless you chose very carefully.”—Interview 106
“Who is there to teach our kids to cook? My grandma and my mum taught me how to cook. But my mum has been working; I don’t have time, because I work full time and I’m a single mum, so my kids can’t cook. And my sons at the age where he’s ready to move out, and he’s lucky if he can make himself a toasted sandwich, and that’s on me. That’s on me. With a population that can’t cook for themselves, and can’t fend for themselves, what’s their alternative? Junk food.”—Interview 112
3.4.7. Loss of Fertile Land to Urban Development
“Unfortunately, a lot of development tends to be on productive soils because it’s flat. I don’t know if you’ve looked at future urban area from Westgate out to Kumeu (North-West Auckland). That’s all designated future urban out there, and that’s where all the strawberry farms are. The strawberries only grow in class 1 soils, and that’s all going to be built over. And 98% of the class 1 soils are in South Auckland, so that means not much of it is in Rodney. The majority of that will be gone once that Westgate to Kumeu goes through.”—Interview 109
“There is also the urban sprawl going on, so that’s taking away some of the land as well. The growers might give up (and) sell for urban sprawl. There’s a grower on one corner and he’s getting hemmed in with houses. And (another grower) sold all that land which is now developed with roads, no houses, just roads, for 10 million. And of course, that’s really tempting.”—Interview 102
3.4.8. Government Regulations
“The businesses that trade food have to comply with the Food Act, 2014. The Food Act came into effect in March 2016 and it’s a three-year rollout. And, in fact, we’re only just getting to the horticulture sector. But we’ve been doing quite a bit of work with the horticulture sector to try and make it as straightforward as possible. Broadly, up until now, from a sort of food safety perspective, growing fruit and veg hasn’t fallen under food and safety legislation, but it’s about to. There’s a registration process for a business to go through. However, it’s pretty minimal. If you’re a packhouse, for example, if you’re growing things or packing them, there’s a registration, there’s a check that you’re meeting the requirements of the Act. And after that, there’s no future programme for checks. So you would only have somebody coming back if something went wrong.”—Interview 113
“There’s a lot more paperwork for growers these days and a lot more regulation, a lot more rules, a lot more laws that they have to abide by. What you’re seeing is smaller growers just giving up. And you’ve got much bigger growing operations now. And some of those operations will have multi-sites through the country, which cushions some of the weather, depending on what they’re growing.”—Interview 102
3.5. Solutions to Low Fruit and Vegetable Intake in Children
3.5.1. Health Promotion in Schools
3.5.2. Educational Interventions
“The problem is the kids are not able to action those [healthy eating] messages that they are getting because of their environment, whether it be home, or the supermarket, or the dairy, or whatever. So they know that they should be eating their fruit and veg but actually being able to do it is totally different.”—Interview 107
“One of my first thoughts was the 5+ A Day campaign is a failure, because of the data you’ve just presented. If the 5+ A Day campaign was working, you’d expect to see an improvement rather than a decline… One thing that I used to challenge 5+ A Day on was you don’t go right across the store. The Health Star Rating will go right across the store. If you think about a retailer’s desire to get behind something, I’m pretty sure a marketing team would rather market something that goes right across the store.”—Interview 104
3.5.3. Price Promotions
3.5.4. Government-Led Interventions
“Planning and consenting around land use is quite important. Consenting would be around the types of food businesses that can locate in certain areas, or the numbers of them, concentration of fast-food stores, for instance, in a certain area, or proximity to schools, for example.”—Interview 109
“Well, if removing the GST makes enough of a price difference (I’d support that)… I know that’s going to be considered. And we’re obviously supporting anything that makes fruit and vegetables more accessible.”—Interview 108
“I don’t know where I personally stand on subsidising fruit and vegetable because I have read both arguments of people not wanting to change the GST from the 15% on everything. But it has been done in some places internationally. And it has had mixed results. But I can see a case for it. How it would pan out in a New Zealand environment, I don’t know. I haven’t looked into it enough.”—Interview 107
“I don’t really know about the evidence around reducing the costs of GST on fruits and vegetables and things like that. Will that actually translate to families buying them more? Because I think it still comes down to food skills, and preferences, and time, and all those other barriers.”—Interview 112
3.5.5. Early Interventions
“But I think if you’re starting right from that early age, and embedding it within children as a priority, and that is what is normal, I think that’s probably—for me, personally, I think it’s a good investment.”—Interview 112
“You start Year 7 with cooking at school… The horse has bolted by the time they’re Year 7 and 8”—Interview 118
3.6. Differences by Sector
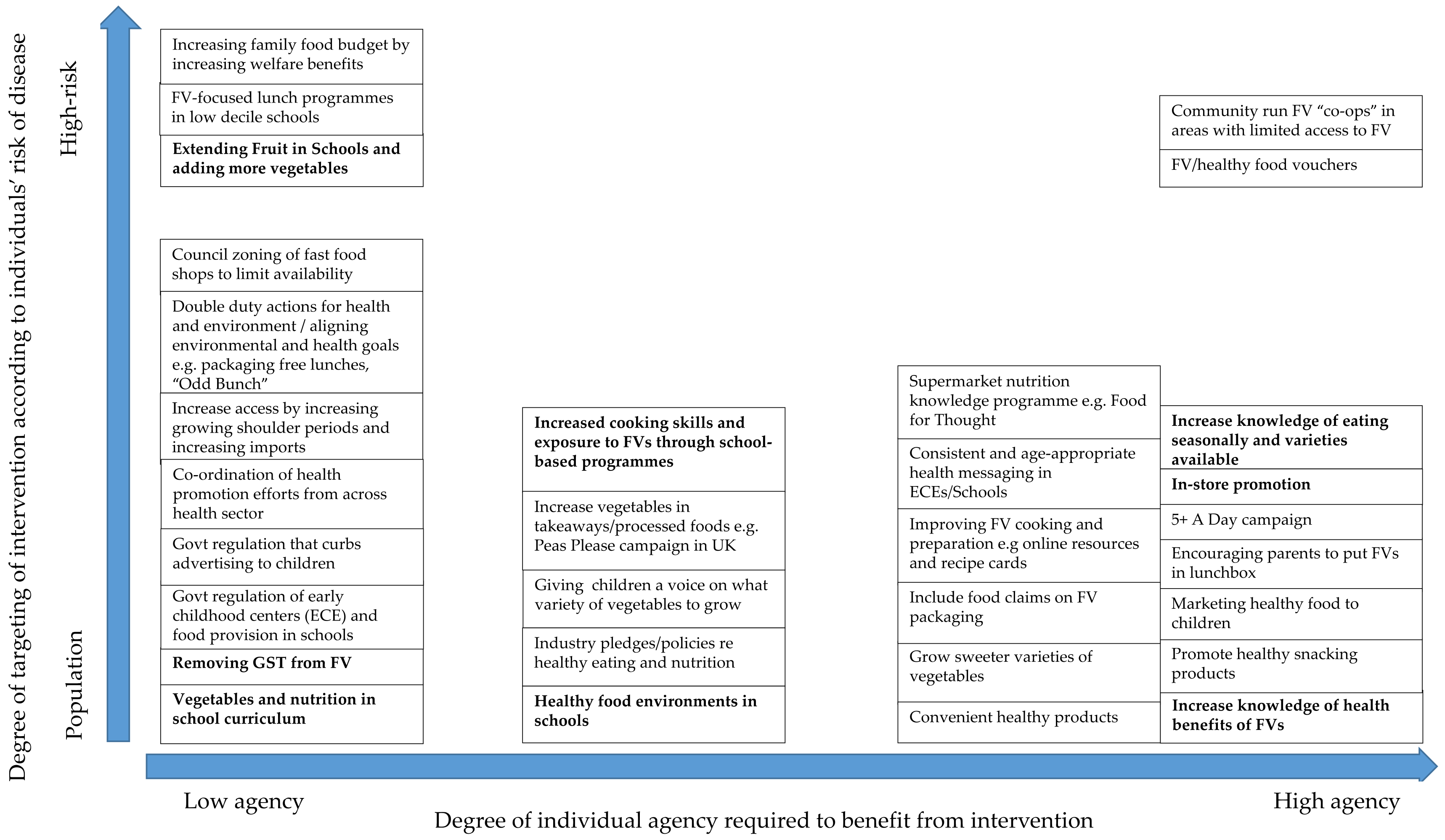
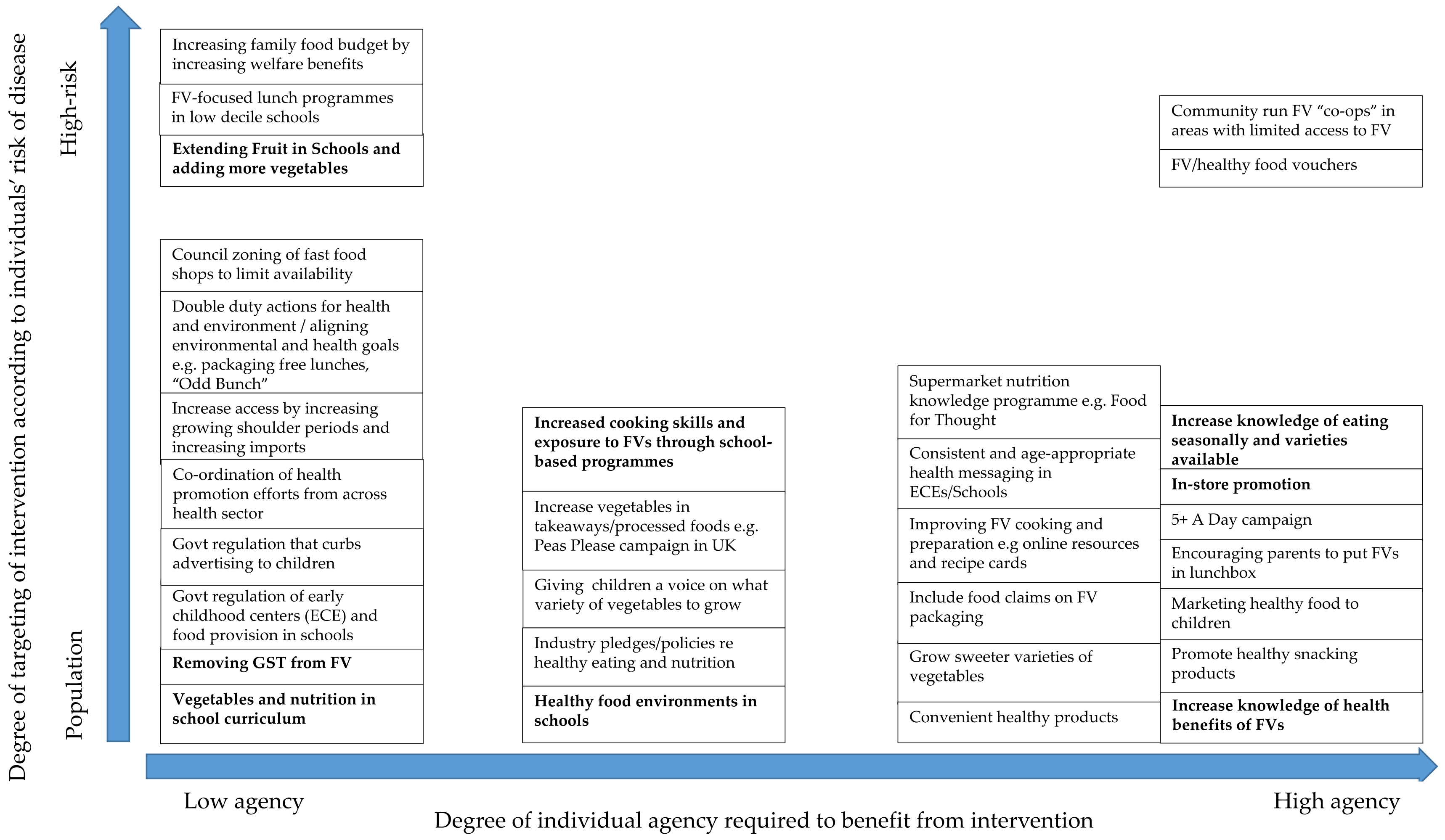
3.7. Equity and Effectiveness of the Interventions Proposed
4. Discussion
4.1. School Environment
4.2. Repeated Exposure to Fruit and Vegetables in Early Childhood
4.3. The Price of Fruit and Vegetables and Household Poverty
4.4. The Food Environment
4.5. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. WHO Global Strategy on Diet, Physical Activity and Health; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Annual Data Explorer 2016/17: New Zealand Health Survey. Available online: https://minhealthnz.shinyapps.io/nz-health-survey-2016-17-annual-update (accessed on 11 December 2018).
- Rasmussen, M.; Krølner, R.; Klepp, K.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 22. [Google Scholar] [CrossRef] [PubMed]
- Krolner, R.; Rasmussen, M.; Brug, J.; Klepp, K.I.; Wind, M.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part II: Qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Food Systems for Children and Adolescents: Working together to secure nutritious diets. In Proceedings of the UNICEF Office Research Innocenti, Florence, Italy, 5–7 November 2018. [Google Scholar]
- Curran-Cournane, F.; Vaughan, M.; Memon, A.; Fredrickson, C. Trade-offs between high class land and development: Recent and future pressures on Auckland’s valuable soil resources. Land Use Policy 2014, 39, 146–154. [Google Scholar] [CrossRef]
- Bartos, A.E. Food Sovereignty and the Possibilities for an Equitable, Just and Sustainable Food System. In Eating, Drinking: Surviving: The International Year of Global Understanding—IYGU; Jackson, P., Spiess, W.E.L., Sultana, F., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 91–98. [Google Scholar]
- Ministry of Social Development. Families and Whanau Status Report; Ministry of Social Development: Wellington, New Zealand, 2018. [Google Scholar]
- Eden, C. Cognitive Mapping. Eur. J. Oper. Res. 1988, 36, 1–13. [Google Scholar] [CrossRef]
- Friel, S.; Pescud, M.; Malbon, E.; Lee, A.; Carter, R.; Greenfield, J.; Cobcroft, M.; Potter, J.; Rychetnik, L.; Meertens, B. Using systems science to understand the determinants of inequities in healthy eating. PLoS ONE 2017, 12, e0188872. [Google Scholar] [CrossRef]
- Kelly, G.A. The Psychology of Personal Constructs; WW Norton: New York, NY, USA, 1955; Volumes 1–2. [Google Scholar]
- Ackermann, F.; Alexander, J. Researching complex projects: Using causal mapping to take a systems perspective. Int. J. Proj. Manag. 2016, 34, 891–901. [Google Scholar] [CrossRef]
- Ackermann, F.; Eden, C.; Cropper, S. Getting Started with Cognitive Mapping. Banxia Softw. 1992, 82, 1–14. [Google Scholar]
- Eden, C.; Ackermann, F. Theory into practice, practice to theory: Action research in method development. Eur. J. Oper. Res. 2018, 271, 1145–1155. [Google Scholar] [CrossRef]
- Rees, D.; Cavana, R.Y.; Cumming, J. Using cognitive and causal modelling to develop a theoretical framework for implementing innovative practices in primary healthcare management in New Zealand. Health Syst. 2018, 7, 51–65. [Google Scholar] [CrossRef]
- Allender, S.; Owen, B.; Kuhlberg, J.; Lowe, J.; Nagorcka-Smith, P.; Whelan, J.; Bell, C.; Carpenter, D.O. A Community Based Systems Diagram of Obesity Causes. PLoS ONE 2015, 10, e0129683. [Google Scholar] [CrossRef]
- Brennan, L.K.; Sabounchi, N.S.; Kemmer, A.L.; Hovmand, P. Systems Thinking in 49 Communities Related to Healthy Eating, Active Living, and Childhood Obesity. Public Health Manag. Pract. 2015, 21 (Suppl. 3), S69. [Google Scholar] [CrossRef]
- Owen, B.; Brown, A.D.; Kuhlberg, J.; Millar, L.; Nichols, M.; Economos, C.; Allender, S. Understanding a successful obesity prevention initiative in children under 5 from a systems perspective. PLoS ONE 2018, 13, e0195141. [Google Scholar] [CrossRef] [PubMed]
- Heke, I.; Rees, D.; Swinburn, B.; Waititi, T.; Stewart, A. Systems Thinking and indigenous systems: Native contributions to obesity prevention. AlterNative 2019, 1–9. [Google Scholar] [CrossRef]
- Adams, J.; Mytton, O.; White, M.; Monsivais, P. Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLoS Med. 2016, 13, 1–7. [Google Scholar]
- Backholer, K.; Beauchamp, A.; Ball, K.; Turrell, G.; Martin, J.; Woods, J.; Peeters, A. A Framework for Evaluating the Impact of Obesity Prevention Strategies on Socioeconomic Inequalities in Weight. Am. J. Public Health 2014, 104, e50. [Google Scholar] [CrossRef] [PubMed]
- Olstad, D.L.; Teychenne, M.; Minaker, L.M.; Taber, D.R.; Raine, K.D.; Nykiforuk, C.I.J.; Ball, K. Can policy ameliorate socioeconomic inequities in obesity and obesity-related behaviours? A systematic review of the impact of universal policies on adults and children. Obes. Rev. 2016, 17, 1198–1217. [Google Scholar] [CrossRef] [PubMed]
- Guthman, J. Weighing In: Obesity, Food Justice, and the Limits of Capitalism; University of California Press: Berkeley, CA, USA, 2011. [Google Scholar]
- Nuffield Council on Bioethics. Public Health: Ethical Issues; Nuffield Council on Bioethics: London, UK, 2007. [Google Scholar]
- Evans, C.E.L.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 years. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, S.; Wall, C. How We Eat—Reviews of the Evidence on Food and Eating Behaviours Related to Diet and Body Size; Ministry of Health: Wellington, New Zealand, 2017. [Google Scholar]
- Dudley, D.A.; Cotton, W.G.; Peralta, L.R. Teaching approaches and strategies that promote healthy eating in primary school children: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Activ. 2015, 12, 28. [Google Scholar] [CrossRef]
- Langellotto, G.A.; Gupta, A. Gardening increases vegetable consumption in school-aged children: A meta-analytical synthesis. HortTechnology 2012, 22, 430. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Lease, H.J.; Bowen, J.; Baird, D.L.; Cox, D.N. Strategies to increase children’s vegetable intake in home and community settings: A systematic review of literature. Matern. Child Nutr. 2017, 13, e12276. [Google Scholar] [CrossRef]
- Ward, S.; Bélanger, M.; Donovan, D.; Carrier, N. Systematic review of the relationship between childcare educators’ practices and preschoolers’ physical activity and eating behaviours. Obes. Rev. 2015, 16, 1055–1070. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Kostka, T.; von Kries, R.; Rehfuess, E.A. Impacts of in utero and early infant taste experiences on later taste acceptance: A systematic review. J. Nutr. 2015, 145, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Barends, C.; de Vries, J.H.M.; Mojet, J.; de Graaf, C. Effects of starting weaning exclusively with vegetables on vegetable intake at the age of 12 and 23 months. Appetite 2014, 81, 193–199. [Google Scholar] [CrossRef]
- Vegetable prices up 31 percent in year to May. Statistics New Zealand Press, 14 June 2017.
- Cheaper to get your 5+ a day at the end of 2018. Statistics New Zealand Press, 14 January 2019.
- Pearson, A.L.; Winter, P.R.; McBreen, B.; Stewart, G.; Roets, R.; Nutsford, D.; Bowie, C.; Donnellan, N.; Wilson, N. Obtaining Fruit and Vegetables for the Lowest Prices: Pricing survey of different outlets and geographical analysis of competition effects. PLoS ONE 2014, 9, e89775. [Google Scholar] [CrossRef] [PubMed]
- University of Otago; Ministry of Health. A Focus on Nutrition: Key findings of the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011. [Google Scholar]
- Ministry of Social Development. Benefits Fact Sheet 2018 June Quarter; Ministry of Social Development: Wellington, New Zealand, 2018.
- Johnson, A. Kei a Tātou: It Is Us; State of the Nation Report; The Salvation Army Social Policy and Parliamentary Unit: Manukau, New Zealand, 2018. [Google Scholar]
- Hutt, K. Food Bank Supplies Run Low as Auckland Hits Peak Poverty, and It’s Not Even Winter. Stuff NZ. 2018. Available online: https://www.stuff.co.nz/auckland/103514452/food-bank-supplies-run-low-as-auckland-hits-peak-poverty-and-its-not-even-winter (accessed on 8 February 2019).
- Demand for KidsCan Food In-School Programme Doubles in the Past Five Years. KidsCan Press, 29 September 2017.
- Johnstone, K. Number of New Zealand Children Hospitalised with Malnutrition Doubles as Food Costs Bite. NZ Herald. 2017. Available online: https://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=11923626 (accessed on 8 February 2019).
- Afshin, A.; Peñalvo, J.L.; Del Gobbo, L.; Silva, J.; Michaelson, M.; O’Flaherty, M.; Capewell, S.; Spiegelman, D.; Danaei, G.; Mozaffarian, D.; et al. The prospective impact of food pricing on improving dietary consumption: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0172277. [Google Scholar] [CrossRef]
- Niebylski, M.L.; Redburn, K.A.; Duhaney, T.; Campbell, N.R. Healthy food subsidies and unhealthy food taxation: A systematic review of the evidence. Nutrition 2015, 31, 787–795. [Google Scholar] [CrossRef]
- Thow, A.M.; Downs, S.; Jan, S. A systematic review of the effectiveness of food taxes and subsidies to improve diets: Understanding the recent evidence. Nutr. Rev. 2014, 72, 551–565. [Google Scholar] [CrossRef]
- Eyles, H.; Ni Mhurchu, C.; Nghiem, N.; Blakely, T. Food pricing strategies, population diets, and non-communicable disease: A systematic review of simulation studies. PLoS Med. 2012, 9, e1001353. [Google Scholar] [CrossRef]
- Andreyeva, T.; Long, M.W.; Brownell, K.D. The Impact of Food Prices on Consumption: A Systematic Review of Research on the Price Elasticity of Demand for Food. Ethics 2008, 36, 256. [Google Scholar] [CrossRef]
- Sushil, Z.; Vandevijvere, S.; Exeter, D.J.; Swinburn, B. Food swamps by area socioeconomic deprivation in New Zealand: A national study. Int. J. Public Health 2017, 62, 869–877. [Google Scholar] [CrossRef]
- Vandevijvere, S.; Mackay, S.; D’Souza, E.; Swinburn, B. How Healthy are New Zealand Food Environments? A Comprehensive Assessment 2014–2017; University of Auckland: Auckland, New Zealand, 2018. [Google Scholar]
- Curran-Cournane, F.; Cain, T.; Greenhalgh, S.; Samarsinghe, O. Attitudes of a farming community towards urban growth and rural fragmentation—An Auckland Case Study. Land Use Policy 2016, 58, 241–250. [Google Scholar] [CrossRef]
- Auckland Council. Auckland Plan 2050; Auckland Council: Auckland, New Zealand, 2018. [Google Scholar]
- Hovmand, P.S. Group Model Building and Community-Based System Dynamics Process. Community Based Syst. Dyn. 2014, 17–30. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Interview Code | Date and Location | Sector | Organisation Description | Role |
|---|---|---|---|---|
| 109 | 12.04.18 Interviewee’s Workplace | Government | Local Government | Sustainability & Resilience Advisor |
| 103 | 05.04.18 Interviewee’s Workplace | Government | Central Government | Portfolio Manager |
| 113 | 03.05.18 Video conference | Government | Central Government | Retail Sales Advisor |
| 113 | Senior Advisor Food Claims | |||
| 107 | 10.04.18 Interviewee’s Workplace | Health Promotion | Nutrition & Activity Advisor | |
| 110 | 13.04.18 Interviewee’s Workplace | Health Promotion | Marketing Manager | |
| 111 | 16.04.18 Videoconference | Health Promotion | Māori Nutrition Kaiārahi | |
| 112 | 04.05.18 Interviewee’s Workplace | Health Promotion | Education Setting Manager | |
| 112 | Programme Manager | |||
| 112 | Pacific Education | |||
| 112 | Food & Nutrition Manager | |||
| 112 | National Nutrition Advisor | |||
| 101 | 29.03.18 University of Auckland | Social policy | Chief executive | |
| 106 | 10.04.18 Interviewee’s Workplace | Private | Research | Director |
| 105 | 06.04.18 Interviewee’s Workplace | Produce Industry | Grower & Wholesaler | Executive GM of NZ Produce |
| 115 | 26.04.18 Interviewee’s Workplace | Produce Industry | Grower | Marketing Manager |
| 115 | Owner | |||
| 116 | 12.04.18 Interviewee’s Workplace | Produce Industry | Grower | Owner and Marketing Manager |
| 118 | 14.05.18 Interviewee’s Workplace | Produce Industry | Grower | Owner |
| 108 | 10.04.18 Interviewee’s Workplace | Produce Industry | Industry Body | Chief Executive |
| 102 | 04.04.18 University of Auckland | Produce Industry | Health promotion | Education & Marketing Manager |
| 104 | 06.04.18 Interviewee’s Workplace | Retail Sector | Supermarket | Head of Produce |
| Theme | Subtheme |
|---|---|
| Price | Actual price |
| Perceived price | |
| Social context | Socioeconomic conditions |
| Food environment | Community Home School Retail Marketing/advertising Workplace |
| Time | Convenience Preparation |
| Skills and knowledge | Skills Knowledge |
| Food preferences and taste | Preference Taste |
| Built and natural environment | Weather Climate change Urbanisation Land use Growing practices |
| Government & business | Social welfare benefits Council Imports/exports Funding Industry Policy & Regulations |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerritsen, S.; Harré, S.; Swinburn, B.; Rees, D.; Renker-Darby, A.; Bartos, A.E.; Waterlander, W.E. Systemic Barriers and Equitable Interventions to Improve Vegetable and Fruit Intake in Children: Interviews with National Food System Actors. Int. J. Environ. Res. Public Health 2019, 16, 1387. https://doi.org/10.3390/ijerph16081387
Gerritsen S, Harré S, Swinburn B, Rees D, Renker-Darby A, Bartos AE, Waterlander WE. Systemic Barriers and Equitable Interventions to Improve Vegetable and Fruit Intake in Children: Interviews with National Food System Actors. International Journal of Environmental Research and Public Health. 2019; 16(8):1387. https://doi.org/10.3390/ijerph16081387
Chicago/Turabian StyleGerritsen, Sarah, Sophia Harré, Boyd Swinburn, David Rees, Ana Renker-Darby, Ann E. Bartos, and Wilma E. Waterlander. 2019. "Systemic Barriers and Equitable Interventions to Improve Vegetable and Fruit Intake in Children: Interviews with National Food System Actors" International Journal of Environmental Research and Public Health 16, no. 8: 1387. https://doi.org/10.3390/ijerph16081387
APA StyleGerritsen, S., Harré, S., Swinburn, B., Rees, D., Renker-Darby, A., Bartos, A. E., & Waterlander, W. E. (2019). Systemic Barriers and Equitable Interventions to Improve Vegetable and Fruit Intake in Children: Interviews with National Food System Actors. International Journal of Environmental Research and Public Health, 16(8), 1387. https://doi.org/10.3390/ijerph16081387