Good Practices in Home Kitchens: Construction and Validation of an Instrument for Household Food-Borne Disease Assessment and Prevention

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Items Construction
- (a)
- Building and facilities;
- (b)
- Kitchen equipment, furniture, and utensils;
- (c)
- Manipulators;
- (d)
- Raw materials and ingredients;
2.2. Content Validation
2.3. Semantic Evaluation
2.4. Data Analysis
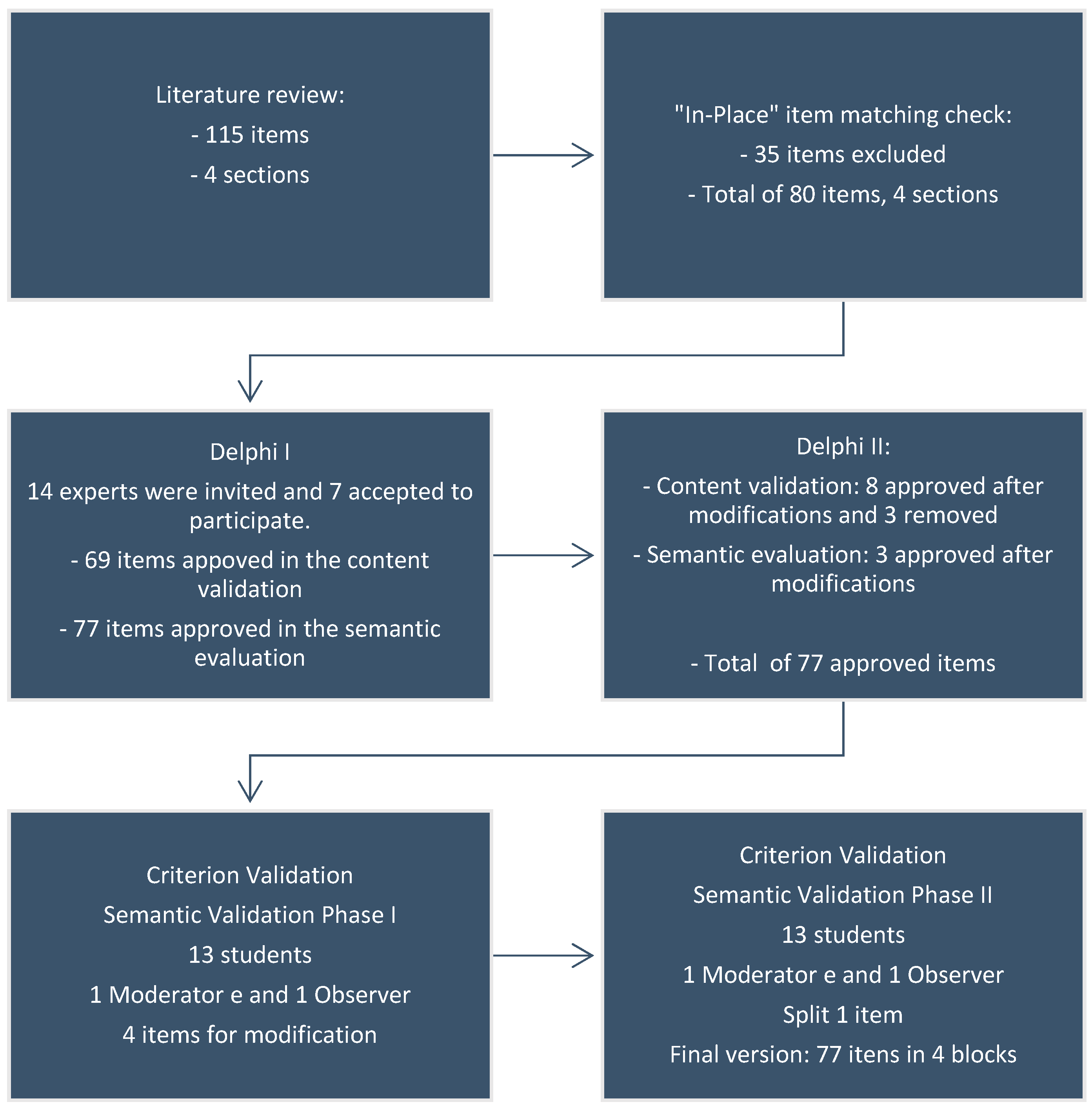
3. Results
3.1. Content Validation and Semantic Evaluation by Experts
3.1.1. Phase Delphi I
3.1.2. Phase Delphi II
3.2. Criteria Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
| Evaluation | Y | N | NA |
| 1. Construction and Facilities | |||
| 1.1 External Area | |||
| External area free of outbreaks of unhealthiness, garbage accumulation, stagnant water, among others. | |||
| Access roads with adequate sewage system. | |||
| 1.2 Internal Area | |||
| Kitchen free of obsolete objects or strangers to the environment. | |||
| Free of the presence of domestic animals. | |||
| 1.3 Floor | |||
| In good state of cleanliness. | |||
| Cleaned at least once a day. | |||
| Floor in material that facilitates its cleaning (ceramics or similar). | |||
| In suitable state of conservation (free of defects, cracks, cracks, holes, and others). | |||
| 1.4 Kitchen Ceiling | |||
| With appropriate ceiling material that facilitate cleaning (plaster, pvc, concrete, or similar). | |||
| In suitable state of conservation (free of cracks, humidity, mold, fungus, spider webs, paint peel, and others). | |||
| 1.5 Walls and Kitchen Divisions | |||
| In good state of cleanliness. | |||
| Built with material of easy cleansing. | |||
| In suitable state of conservation (free of cracks, humidity, paint peel, and others). | |||
| 1.6 Kitchen Door | |||
| In suitable state of conservation (free of cracks, humidity, paint peel, and others). | |||
| Built with material of easy cleansing. | |||
| 1.7 Windows and Other Kitchen Openings | |||
| In suitable state of conservation (free of cracks, humidity, paint peel, and others). | |||
| Built with material of easy cleansing. | |||
| 1.8 Toilets | |||
| Toilet with intact toilet seat and with lid. | |||
| Toilet with running water and connected to the sewage system or septic tank. | |||
| Toilet without direct link to the kitchen area and/or the dining room. | |||
| Toilet with bins with lids and pedal triggering. | |||
| 1.9 Lighting and kitchen electrical wiring | |||
| Recessed lighting or when external, covered by insulating pipes attached to walls and ceiling. | |||
| Bulbs and electric switches free of dirt. | |||
| Cleaning of lamps, outlets, and electric switches at least once a month. | |||
| 1.10 Ventilation and Acclimatization System of the Kitchen | |||
| Kitchen with ventilation and air circulation capable of thermal comfort. | |||
| Kitchen free of fungus, causing no harm to food. | |||
| 1.11 Urban Vector and Pest Control | |||
| Absence of urban vectors and pests or other evidences such as feces, nests, and other. | |||
| Disinfecting every six months. | |||
| 1.12 Water Supply | |||
| Water supply system connected to the public grid. | |||
| Proper, protected, covered, and distant from contamination water system. | |||
| Water tank with lid and in good state. | |||
| Cleaning of water tank every six months. | |||
| 1.13 Waste Management | |||
| Easy to clean and carry waste bins; in proper state and with appropriate garbage bags. | |||
| Covered waste bins with pedal triggering. | |||
| No waste bins over the sink. | |||
| Waste stored in appropriate areas. | |||
| 1.14 Sewage System: | |||
| Septic tank and sewage system connected to the public sewage. | |||
| Observations: | |||
| 2. Equipment, Furniture, and Kitchen Utensils. | |||
| 2.1 Equipment: | |||
| Evaluation | Y | N | NA |
| Fridge and stove in an area that permits adequate cleaning. | |||
| Conservation equipment for food (fridges, freezers, and others) in proper functioning. | |||
| Thermal food equipment (stove, oven, and/or microwave) in proper functioning. | |||
| 2.2 Furniture (tables, countermiddle, cupboard, shelves) | |||
| From resistant material with proper surface conditions. | |||
| Withdrawing that allows easy cleaning (smooth, without roughness, and chinks). | |||
| 2.3 Utensils: | |||
| Size and shape for easy cleaning and in proper state. | |||
| No wooden utensils or other materials of easy contamination. | |||
| Pans, pots, and trays in proper state. | |||
| Boards, knives, skimmers, and holders in proper state. | |||
| Slicers and squeezers in proper state. | |||
| Utensils (plates, silverware, bowls) in proper state. | |||
| 2.4 Equipment, Furniture, and Kitchen Utensils Cleaning | |||
| Fridges and freezers in proper state. | |||
| Fridges or freezers cleaned at least once a week. | |||
| The stove is cleaned when used. | |||
| Dishcloths in proper and cleaned state. | |||
| Dishrags or table rags in proper state. | |||
| Dishcloths are changed daily. | |||
| Dishrags are changed daily. | |||
| Cleaning sponges in proper hygiene and state. | |||
| Cleaning sponges changed weekly. | |||
| Cleaning products approved by the health department. | |||
| Cleaning products in their original packing and stored in proper location. | |||
| Equipment, furniture, and kitchen utensils in proper hygiene and state. | |||
| Water filters changed every six months. | |||
| No sponges from steel or wool. | |||
| Observations: | |||
| Evaluation | Y | N | NA |
| 3. Handlers | |||
| 3.1 Hygiene Habits | |||
| Personal cleaning, good appearance, clean hands, short nails, and unadorned (rings, earrings, bracelets, others). | |||
| Handlers with previous knowledge on hand washing. | |||
| 3.2 Health Condition | |||
| Absence of skin rash, wound, suppuration; absence of respiratory, eye, and gastric infections. | |||
| Observations: | |||
| Evaluation | Y | N | NA |
| 4.0 Food and Feedstock | |||
| 4.1 Food and Feedstock Origin | |||
| Food and feedstock with labels and packaging according to legislation. | |||
| Milk from a secure source. | |||
| Cheese from a secure source, packed and labeled. | |||
| Meat, chicken, or fish from proper establishments. | |||
| Filtered or boiled water consumption. | |||
| 4.2 Food Storage | |||
| Semi perishable food stored in adequate and organized area with air circulation and lighting. | |||
| Food prepared in advance before serving heated again. | |||
| Fridges and freezers organized in order to avoid cross contamination. | |||
| Feedstock not used completely are properly stored in clean and closed container. | |||
| Feedstock not used completely are identified with expiration date. | |||
| Perishable food stored in adequate temperature. | |||
| Packages well cleaned before used for fridge or freeze storage. | |||
| Leftovers stored under refrigeration and with bowls with lids. | |||
| Observations: | |||
References
- Parra, P.A.; Kim, H.; Shapiro, M.A.; Gravani, R.B.; Bradley, S.D. Home food safety knowledge, risk perception, and practices among Mexican-Americans. Food Control 2014, 37, 115–125. [Google Scholar] [CrossRef]
- Draeger, C.; Akutsu, R.; Zandonadi, R.; da Silva, I.; Botelho, R.; Araújo, W. Brazilian Foodborne Disease National Survey: Evaluating the Landscape after 11 Years of Implementation to Advance Research, Policy, and Practice in Public Health. Nutrients 2019, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Draeger, C.; Akutsu, R.; Araújo, W.; da Silva, I.; Botelho, R.; Zandonadi, R. Epidemiological Surveillance System on Foodborne Diseases in Brazil after 10-Years of Its Implementation: Completeness Evaluation. Int. J. Environ. Res. Public Health 2018, 15, 2284. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.K.; Murray, R.; Flockhart, L.; Pintar, K.; Fazil, A.; Nesbitt, A.; Marshall, B.; Tataryn, J.; Pollari, F. Estimates of Foodborne Illness–Related Hospitalizations and Deaths in Canada for 30 Specified Pathogens and Unspecified Agents. Foodborne Pathog. Dis. 2015, 12, 820–827. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Estimates of the Global Burden of Foodborne Diseases, 1st ed.; WHO Library Cataloguing-in-Publication Data, Ed.; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-156516-5. [Google Scholar]
- Scallan, E.; Hoekstra, R.M.; Angulo, F.J.; Tauxe, R.V.; Widdowson, M.-A.; Roy, S.L.; Jones, J.L.; Griffin, P.M. Foodborne illness acquired in the United States—Major pathogens. Emerg. Infect. Dis. 2011, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Scallan, E.; Griffin, P.M.; Angulo, F.J.; Tauxe, R.V.; Hoekstra, R.M. Foodborne Illness Acquired in the United States—Unspecified Agents. Emerg. Infect. Dis. 2011, 17, 16–22. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Salmonella enteritidis infections associated with foods purchased from mobile lunch trucks—Alberta, Canada, October 2010–February 2011. MMWR. Morb. Mortal. Wkly. Rep. 2013, 62, 567–569. [Google Scholar]
- Brasil 10 Passos para Investigação de Surtos. Available online: http://portal.saude.gov.br/portal/arquivos/pdf/10_passos_para_investigacao_surtos.pdf (accessed on 27 December 2018).
- Deon, B.C.; Medeiros, L.B.; Lúcia de Freitas Saccol, A.; Hecktheuer, L.H.; Saccol, S.; Naissinger, M. Good food preparation practices in households: A review. Trends Food Sci. Technol. 2014, 39, 40–46. [Google Scholar] [CrossRef]
- Zandonadi, R.P.; Botelho, R.B.A.; Sávio, K.E.O.; Akutsu, R.D.C.; Araújo, W.M.C. Atitudes de risco do consumidor em restaurantes de auto-serviço. Rev. Nutr. 2007, 20, 19–26. [Google Scholar] [CrossRef]
- de Oliveira, A.B.A.; da Cunha, D.T.; Stedefeldt, E.; Capalonga, R.; Tondo, E.C.; Cardoso, M.R.I. Hygiene and good practices in school meal services: Organic matter on surfaces, microorganisms and health risks. Food Control 2014, 40, 120–126. [Google Scholar] [CrossRef]
- Adane, M.; Teka, B.; Gismu, Y.; Halefom, G.; Ademe, M. Food hygiene and safety measures among food handlers in street food shops and food establishments of Dessie town, Ethiopia: A community-based cross-sectional study. PLoS ONE 2018, 13, e0196919. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Brasil Resolução RDC n. 216, de 15 de Setembro de 2004; Dispõe sobre regulamento técnico de boas práticas para serviços de alimentação; Diário Oficial [da] República Federativa do Brasil: Brasília, Brazil, 2004; pp. 1–14. [Google Scholar]
- Brazil RDC n. 275. Agência Nacional de Vigilância Sanitária. Resolução RDC n. 275, de 21 de Outubro de 2002; Diário Oficial da República Federativa do Brasil: Brasília, Brazil, 2003. [Google Scholar]
- International Organization for Standardization ISO 22000: Food Safety Management Systems—Requirements for Any Organization in the Food Chain. Available online: https://www.iso.org/obp/ui/#iso:std:iso:22000:ed-1:v1:en (accessed on 15 January 2019).
- OPAS/OMS/Brasil Codex Alimentarius—Higiene dos Alimentos. Available online: https://www.paho.org/bra/index.php?option=com_docman&view=document&layout=default&alias=286-codex-alimentarius-higiene-dos-alimentos-textos-basicos-6&category_slug=seguranca-alimentar-e-nutricao-997&Itemid=965 (accessed on 4 November 2018).
- Duprat Ceniccola, G.; Coelho Araújo, W.M.; Akutsu, R. Development of a tool for quality control audits in hospital enteral nutrition. Nutr. Hosp. 2014, 29, 102–120. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, T.G.; Botelho, R.B.A.; Akutsu, R.d.C.C.A.; Araújo, W.M.C. Conformity of food service units with legislation. J. Culin. Sci. Technol. 2016, 14, 75–89. [Google Scholar] [CrossRef]
- Wendisch, C. Avaliação da Qualidade de Unidades de Alimentação e Nutrição (UAN) Hospitalares: Construção de um instrumento; Fiocruz: Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Conti, M.A.; Scagliusi, F.; Kawamura De Oliveira Queiroz, G.; Hearst, N.; Cordás, T.A. Cross-cultural adaptation: Translation and Portuguese language content validation of the Tripartite Infl uence Scale for body dissatisfaction. Cad. Saude Publica 2010, 26, 503–513. [Google Scholar] [CrossRef] [PubMed]
- de Lima, T.C.; Gallani, M.C.B.J.; de Freitas, M.I.P. Content validation of an instrument to characterize people over 50 years of age living with human immunodeficiency virus/acquired immunodeficiency syndrome. Acta Paul. Enferm. 2012, 25, 4–10. [Google Scholar] [CrossRef]
- Legendre, P. Species associations: The Kendall coefficient of concordance revisited. J. Agric. Biol. Environ. Stat. 2005, 10, 226–245. [Google Scholar] [CrossRef]
- Pasquali, L. Instrumentos Psicológicos: Manual Prático De Elaboração; IBAPP: Brasília, Brazil, 1999. [Google Scholar]
- da Costa, G.A.C.; Akutsu, R.D.C.; Gallo, L.R.D.R.; Araújo, W.M.C. Knowledge and Consumer Behavior Related to Safe Practices of Food Handling. J. Saf. Stud. 2016, 2, 15. [Google Scholar] [CrossRef]
- Farage, P.; Zandonadi, R.P.; Ginani, V.C.; Gandolfi, L.; Pratesi, R.; de Medeiros Nóbrega, Y.K. Content validation and semantic evaluation of a check-list elaborated for the prevention of gluten cross-contamination in food services. Nutrients 2017, 9, 36. [Google Scholar] [CrossRef]
- Pasquali, L. Psicometria. Rev. Esc. Enferm. USP 2009, 43, 992–999. [Google Scholar] [CrossRef]
- Cunha Barreto De Mendonça, S.; Zanetti, M.L.; Sawada, N.O.; Daniel De Carvalho Barreto, I.; Santos De Andrade, J.; Otero, L.M. Construction and validation of the Self-care Assessment Instrument for patients with type 2 diabetes mellitus. Rev. Lat.-Am. Enferm. 2017. [Google Scholar] [CrossRef]
- de Freitas Saccol, A.L.; Serafim, A.L.; Hecktheuer, L.H.R.; Medeiros, L.B.; Spinelli, M.G.N.; de Abreu, E.S.; Chaud, D.M.A. Hygiene and sanitary conditions in self-service restaurants in São Paulo, Brazil. Food Control 2013, 33, 301–305. [Google Scholar] [CrossRef]
- Cortese, R.D.M.; Veiros, M.B.; Feldman, C.; Cavalli, S.B. Food safety and hygiene practices of vendors during the chain of street food production in Florianopolis, Brazil: A cross-sectional study. Food Control 2016, 62, 178–186. [Google Scholar] [CrossRef]
- Karabudak, E.; Bas, M.; Kiziltan, G. Food safety in the home consumption of meat in Turkey. Food Control 2008, 19, 320–327. [Google Scholar] [CrossRef]
- Jacob, C.J.; Powell, D.A. Where Does Foodborne Illness Happen-in the Home, at Foodservice, or Elsewhere-and Does It Matter? Foodborne Pathog. Dis. 2009, 6, 1121–1123. [Google Scholar] [CrossRef]
- Brazil. The Ministry of Health. Surtos de Doenças Transmitidas por Alimentos no Brasil; The Ministry of Health: Brasília, Brazil, 2016.
- Jevšnik, M.; Hlebec, V.; Raspor, P. Food safety knowledge and practices among food handlers in Slovenia. Food Control 2008, 19, 1107–1118. [Google Scholar] [CrossRef]
- Jevšnik, M.; Hoyer, S.; Raspor, P. Food safety knowledge and practices among pregnant and non-pregnant women in Slovenia. Food Control 2008, 19, 526–534. [Google Scholar] [CrossRef]
- Buffer, J.; Kendall, P.; Medeiros, L.; Schroeder, M.; Sofos, J. Nurses and Dietitians Differ in Food Safety Information Provided to Highly Susceptible Clients. J. Nutr. Educ. Behav. 2013, 45, 102–108. [Google Scholar] [CrossRef]
- Byrd-Bredbenner, C.; Berning, J.; Martin-Biggers, J.; Quick, V. Food safety in home kitchens: A synthesis of the literature. Int. J. Environ. Res. Public Health 2013, 10, 4060–4085. [Google Scholar] [CrossRef]
- Byrd-Bredbenner, C.; Maurer, J.; Wheatley, V.; Cottone, E.; Clancy, M. Food Safety Hazards Lurk in the Kitchens of Young Adults. J. Food Prot. 2007, 70, 991–996. [Google Scholar] [CrossRef]
- Anderson, J.B.; Shuster, T.A.; Hansen, K.E.; Levy, A.S.; Volk, A. A Camera’s view of consumer food-handling behaviors. J. Am. Diet. Assoc. 2004, 104, 186–191. [Google Scholar] [CrossRef]
- Fein, S.B.; Lando, A.M.; Levy, A.S.; Teisl, M.F.; Noblet, C. Trends in U.S. Consumers’ Safe Handling and Consumption of Food and Their Risk Perceptions, 1988 through 2010. J. Food Prot. 2011, 74, 1513–1523. [Google Scholar] [CrossRef]
- Taché, J.; Carpentier, B. Hygiene in the home kitchen: Changes in behaviour and impact of key microbiological hazard control measures. Food Control 2014, 35, 392–400. [Google Scholar] [CrossRef]
- Teisl, M.F.; Lando, A.M.; Levy, A.S.; Noblet, C.L. Importance of cohorts in analyzing trends in safe at-home food-handling practices. Food Control 2015, 62, 381–389. [Google Scholar] [CrossRef]


{kind=link}
| Construction and Facilities | ||||
|---|---|---|---|---|
| Section of the Check-List | Content Validation (Mean Grade ± SD *) | Content Validation (W-Values) | Semantic Validation (Mean Grade ± SD *) | Semantic Validation (W-Values) |
| Outdoor area | 3.86 ± 0.38 | 0.86 | 3.69 ± 0.48 | 0.70 |
| Indoor area | 3.86 ± 0.38 | 0.86 | 3.62 ± 0.50 | 0.70 |
| Kitchen floor | 3.71 ± 0.49 | 0.71 | 3.77 ± 0.44 | 0.77 |
| Kitchen ceiling | 4.00 ± 0.00 | 1.00 | 3.62 ± 0.50 | 0.70 |
| Walls and kitchen divisions | 4.00 ± 0.00 | 1.00 | 3.62 ± 0.50 | 0.70 |
| Kitchen door | 3.86 ± 0.38 | 0.86 | 3.54 ± 0.52 | 0.70 |
| Windows and other kitchen openings | 4.00 ± 0.00 | 1.00 | 3.69 ± 0.48 | 0.70 |
| Toilets | 3.86 ± 0.38 | 0.86 | 3.92 ± 0.28 | 0.92 |
| Lighting and kitchen electrical wiring | 3.86 ± 0.38 | 0.86 | 3.62 ± 0.50 | 0.70 |
| Ventilation and acclimatization system of the kitchen | 3.71 ± 0.49 | 0.71 | 3.69 ± 0.48 | 0.70 |
| Urban vector and pest control | 3.57 ± 0.53 | 0.70 | 3.77 ± 0.44 | 0.77 |
| Water supply | 3.57 ± 0.53 | 0.70 | 3.77 ± 0.44 | 0.77 |
| Waste management | 3.86 ± 0.38 | 0.86 | 3.77 ± 0.44 | 0.77 |
| Sanitary sewage | 3.57 ± 1.13 | 0.86 | 3.62 ± 0.50 | 0.70 |
| Total of the block | 3.88 ± 0.46 | 0.87 | 3.69 ± 0.48 | 0.70 |
| Equipment, furniture, and kitchen utensils | ||||
| Equipment | 4.00 ± 0.00 | 1.00 | 3.62 ± 0.50 | 0.70 |
| Furniture | 4.00 ± 0.00 | 1.00 | 3.69 ± 0.48 | 0.70 |
| Utensils | 3.86 ± 0.38 | 0.86 | 3.92 ± 0.28 | 0.92 |
| Equipment, furniture, and utensils hygiene | 4.00 ± 0.00 | 1.00 | 3.77 ± 0.44 | 0.77 |
| Total of the block | 3.92 ± 0.22 | 0.98 | 3.77 ± 0.44 | 0.77 |
| Handlers | ||||
| Hygiene habits | 3.86 ± 0.38 | 0.86 | 3.92 ± 0.28 | 0.92 |
| Health condition | 3.86 ± 0.38 | 0.86 | 3.85 ± 0.37 | 0.85 |
| Total of the block | 3.86 ± 0.38 | 0.86 | 3.96 ± 0.27 | 0.93 |
| Food and feedstock | ||||
| Food and feed stock origin | 4.00 ± 0.00 | 1.00 | 3.92 ± 0.28 | 0.92 |
| Food storage | 4.00 ± 0.00 | 1.00 | 3.92 ± 0.28 | 0.92 |
| Total of the block | 4.00 ± 0.00 | 1.00 | 3.92 ± 0.28 | 0.92 |
| Total of the instrument | 3.86 ± 0.38 | 0.86 | 3.62 ± 0.50 | 0.70 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Silva Farias, A.; Akutsu, R.d.C.C.d.A.; Botelho, R.B.A.; Zandonadi, R.P. Good Practices in Home Kitchens: Construction and Validation of an Instrument for Household Food-Borne Disease Assessment and Prevention. Int. J. Environ. Res. Public Health 2019, 16, 1005. https://doi.org/10.3390/ijerph16061005
da Silva Farias A, Akutsu RdCCdA, Botelho RBA, Zandonadi RP. Good Practices in Home Kitchens: Construction and Validation of an Instrument for Household Food-Borne Disease Assessment and Prevention. International Journal of Environmental Research and Public Health. 2019; 16(6):1005. https://doi.org/10.3390/ijerph16061005
Chicago/Turabian Styleda Silva Farias, Adenilma, Rita de Cassia Coelho de Almeida Akutsu, Raquel Braz Assunção Botelho, and Renata Puppin Zandonadi. 2019. "Good Practices in Home Kitchens: Construction and Validation of an Instrument for Household Food-Borne Disease Assessment and Prevention" International Journal of Environmental Research and Public Health 16, no. 6: 1005. https://doi.org/10.3390/ijerph16061005
APA Styleda Silva Farias, A., Akutsu, R. d. C. C. d. A., Botelho, R. B. A., & Zandonadi, R. P. (2019). Good Practices in Home Kitchens: Construction and Validation of an Instrument for Household Food-Borne Disease Assessment and Prevention. International Journal of Environmental Research and Public Health, 16(6), 1005. https://doi.org/10.3390/ijerph16061005