Association between Periodontal Disease and Subsequent Sjögren’s Syndrome: A Nationwide Population-Based Cohort Study

 ,
, 
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and DataBase
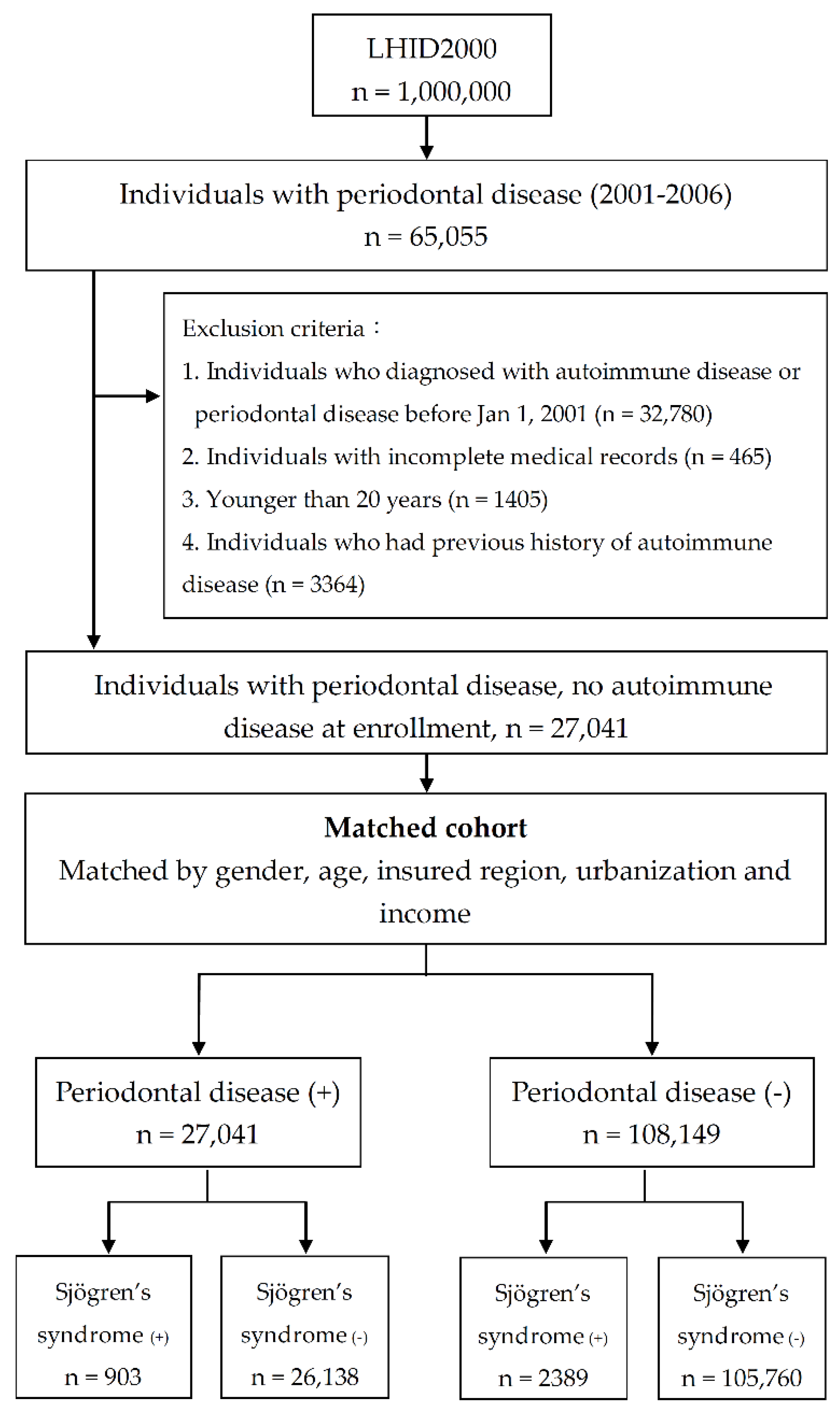
2.2. Selection Criteria and Study Flow Chart
2.3. Study Outcomes and Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Both, T.; Dalm, V.A.; van Hagen, P.M.; van Daele, P.L. Reviewing primary sjogren’s syndrome: Beyond the dryness—From pathophysiology to diagnosis and treatment. Int. J. Med Sci. 2017, 14, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American college of rheumatology/european league against rheumatism classification criteria for primary sjogren’s syndrome: A consensus and data-driven methodology involving three international patient cohorts. Ann. Rheum. Dis. 2017, 76, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Fairweather, D.; Rose, N.R. Women and autoimmune diseases. Emerg. Infect. Dis. 2004, 10, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Maciel, G.; Crowson, C.S.; Matteson, E.L.; Cornec, D. Prevalence of primary sjogren’s syndrome in a us population-based cohort. Arthritis Care Res. 2017, 69, 1612–1616. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Shahane, A. The epidemiology of sjögren’s syndrome. Clin. Epidemiol. 2014, 6, 247–255. [Google Scholar] [PubMed]
- Garcia-Carrasco, M.; Fuentes-Alexandro, S.; Escarcega, R.O.; Salgado, G.; Riebeling, C.; Cervera, R. Pathophysiology of sjogren’s syndrome. Arch. Med. Res. 2006, 37, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.Q.; Peck, A.B. Unraveling the pathophysiology of sjogren syndrome-associated dry eye disease. Ocul. Surf. 2009, 7, 11–27. [Google Scholar] [CrossRef]
- Matsui, K.; Sano, H. T helper 17 cells in primary sjögren’s syndrome. J. Clin. Med. 2017, 6, 65. [Google Scholar] [CrossRef] [PubMed]
- Malladi, A.S.; Sack, K.E.; Shiboski, S.C.; Shiboski, C.H.; Baer, A.N.; Banushree, R.; Dong, Y.; Helin, P.; Kirkham, B.W.; Li, M.; et al. Primary sjögren’s syndrome as a systemic disease: A study of participants enrolled in an international sjögren’s syndrome registry. Arthritis Care Res. 2012, 64, 911–918. [Google Scholar] [CrossRef] [PubMed]
- D’Arbonneau, F.; Ansart, S.; Le Berre, R.; Dueymes, M.; Youinou, P.; Pennec, Y.L. Thyroid dysfunction in primary sjogren’s syndrome: A long-term followup study. Arthritis Rheum. 2003, 49, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Bartoloni, E.; Baldini, C.; Schillaci, G.; Quartuccio, L.; Priori, R.; Carubbi, F.; Bini, V.; Alunno, A.; Bombardieri, S.; De Vita, S.; et al. Cardiovascular disease risk burden in primary sjogren’s syndrome: Results of a population-based multicentre cohort study. J. Intern. Med. 2015, 278, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Zintzaras, E.; Voulgarelis, M.; Moutsopoulos, H.M. The risk of lymphoma development in autoimmune diseases: A meta-analysis. Arch. Intern. Med. 2005, 165, 2337–2344. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Lertpimonchai, A.; Rattanasiri, S.; Arj-Ong Vallibhakara, S.; Attia, J.; Thakkinstian, A. The association between oral hygiene and periodontitis: A systematic review and meta-analysis. Int. Dent. J. 2017, 67, 332–343. [Google Scholar] [CrossRef] [PubMed]
- AlJehani, Y.A. Risk factors of periodontal disease: Review of the literature. Int. J. Dent. 2014, 2014, 182513. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.B.; Damoulis, P.D. The role of cytokines in the pathogenesis of periodontal disease. Curr. Opin. Periodontol. 1994, 39–53. Available online: https://www.ncbi.nlm.nih.gov/pubmed/8032465 (accessed on 3 March 2019).
- Figueredo, C.M.; Brito, F.; Barros, F.C.; Menegat, J.S.; Pedreira, R.R.; Fischer, R.G.; Gustafsson, A. Expression of cytokines in the gingival crevicular fluid and serum from patients with inflammatory bowel disease and untreated chronic periodontitis. J. Periodontal Res. 2011, 46, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Murakami, S. Cytokine expression in periodontal health and disease. Crit. Rev. Oral Biol. Med. 1998, 9, 248–266. [Google Scholar] [CrossRef] [PubMed]
- Badran, Z.; Struillou, X.; Verner, C.; Clee, T.; Rakic, M.; Martinez, M.C.; Soueidan, A. Periodontitis as a risk factor for systemic disease: Are microparticles the missing link? Med. Hypotheses 2015, 84, 555–556. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Castellani, S.; Gori, A.M.; Nieri, M.; Baldelli, G.; Abbate, R.; Pini-Prato, G.P. Severe periodontitis in young adults is associated with sub-clinical atherosclerosis. J. Clin. Periodontol. 2008, 35, 465–472. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, C.; Watt, R.; Hamer, M. Toothbrushing, inflammation, and risk of cardiovascular disease: Results from scottish health survey. BMJ (Clin. Res. Ed.) 2010, 340, c2451. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Tseng, K.S.; Liu, J.M.; Chuang, H.C.; Lien, C.H.; Chen, Y.C.; Lai, C.Y.; Yu, C.P.; Hsu, R.J. Increased risk of ulcerative colitis in patients with periodontal disease: A nationwide population-based cohort study. Int. J. Environ. Res. Public Health 2018, 15, 2602. [Google Scholar] [CrossRef] [PubMed]
- Antoniazzi, R.P.; Miranda, L.A.; Zanatta, F.B.; Islabao, A.G.; Gustafsson, A.; Chiapinotto, G.A.; Oppermann, R.V. Periodontal conditions of individuals with sjogren’s syndrome. J. Periodontol. 2009, 80, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Scardina, G.A.; Ruggieri, A.; Messina, P. Periodontal disease and sjogren syndrome: A possible correlation? Angiology 2010, 61, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A.; Portelli, M.; Marcolina, M.; Nocini, P.F.; Caldara, G.; Bertossi, D.; Lucchese, C.; Tacchino, U.; Manuelli, M. Effect of dental care on the oral health of sjogrens syndrome patients. J. Biol. Regul. Homeost. Agents 2018, 32, 37–43. [Google Scholar] [PubMed]
- de Goes Soares, L.; Rocha, R.L.; Bagordakis, E.; Galvao, E.L.; Douglas-de-Oliveira, D.W.; Falci, S.G.M. Relationship between sjogren syndrome and periodontal status: A systematic review. Oral Surg. Oral Med. 2018, 125, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Schiodt, M.; Christensen, L.B.; Petersen, P.E.; Thorn, J.J. Periodontal disease in primary sjogren’s syndrome. Oral Dis. 2001, 7, 106–108. [Google Scholar] [PubMed]
- Liu, Y.P.; Hsu, R.J.; Wu, M.H.; Peng, C.C.; Chang, S.T.; Lei, W.T.; Yeh, T.L.; Liu, J.M.; Lin, C.Y. Economic conditions may contribute to increased violence toward children: A nationwide population-based analysis of pediatric injuries in taiwanese emergency departments. Int. J. Environ. Res. Public Health 2018, 15, 182. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.M.; Chiu, F.H.; Lin, C.Y.; Chang, F.W.; Hsu, R.J. Incidence of autoimmune diseases in patients with scabies: A nationwide population-based study in Taiwan. Rheumatol. Int. 2017, 37, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Gualtierotti, R.; Marzano, A.V.; Spadari, F.; Cugno, M. Main oral manifestations in immune-mediated and inflammatory rheumatic diseases. J. Clin. Med. 2019, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Rachapalli, S. Periodontal disease in rheumatoid arthritis and sjogren’s syndrome: A modifiable risk factor for atherosclerosis? Rheumatol. Int. 2009, 29, 479. [Google Scholar] [CrossRef] [PubMed]
- Chang, G.H.; Chen, Y.C.; Lin, K.M.; Yang, Y.H.; Liu, C.Y.; Lin, M.H.; Wu, C.Y.; Hsu, C.M.; Tsai, M.S. Real-world database examining the association between sjogren’s syndrome and chronic rhinosinusitis. J. Clin. Med. 2019, 8, 155. [Google Scholar] [CrossRef] [PubMed]
- Ambrosio, L.M.; Rovai, E.S.; Franca, B.N.; Balzarini, D.A.; Abreu, I.S.; Lopes, S.B.; Nunes, T.B.; Lourenco, S.V.; Pasoto, S.G.; Saraiva, L.; et al. Effects of periodontal treatment on primary sjogren’s syndrome symptoms. Braz. Oral Res. 2017, 31, e8. [Google Scholar] [CrossRef] [PubMed]
- Jaedicke, K.M.; Preshaw, P.M.; Taylor, J.J. Salivary cytokines as biomarkers of periodontal diseases. Periodontology 2000 2016, 70, 164–183. [Google Scholar] [CrossRef] [PubMed]
- Menegat, J.S.; Lira-Junior, R.; Siqueira, M.A.; Brito, F.; Carvalho, A.T.; Fischer, R.G.; Figueredo, C.M. Cytokine expression in gingival and intestinal tissues of patients with periodontitis and inflammatory bowel disease: An exploratory study. Arch. Oral Biol. 2016, 66, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Choy, C.S.; Lai, Y.C.; Chang, C.C.; Teng, N.C.; Huang, W.T.; Lin, C.T.; Huang, Y.K. A cross-sectinal study of endogenous antioxidants and patterns of dental visits of periodontitis patients. Int. J. Environ. Res. Public Health 2019, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Roescher, N.; Tak, P.P.; Illei, G.G. Cytokines in sjogren’s syndrome. Oral Dis. 2009, 15, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Roescher, N.; Tak, P.P.; Illei, G.G. Cytokines in sjogren’s syndrome: Potential therapeutic targets. Ann. Rheum. Dis. 2010, 69, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Sjogren’s Syndrome Foundation. SSF launches 5-Year Breakthrough Goal. Moisture Seek. 2012. Available online: http://www.sjogrens.org/home/about-the-foundation/breakthrough-goal (accessed on 7 January 2019).
- Olsson, P.; Turesson, C.; Mandl, T.; Jacobsson, L.; Theander, E. Cigarette smoking and the risk of primary sjogren’s syndrome: A nested case control study. Arthritis Res. Ther. 2017, 19, 50. [Google Scholar] [CrossRef] [PubMed]
- Stone, D.U.; Fife, D.; Brown, M.; Earley, K.E.; Radfar, L.; Kaufman, C.E.; Lewis, D.M.; Rhodus, N.L.; Segal, B.M.; Wallace, D.J.; et al. Effect of tobacco smoking on the clinical, histopathological, and serological manifestations of sjogren’s syndrome. PLoS ONE 2017, 12, e0170249. [Google Scholar] [CrossRef] [PubMed]
- Reddy, N.S.; Reddy, N.A.; Narendra, R.; Reddy, S.D. Epidemiological survey on edentulousness. J. Contemp. Dent. Pract. 2012, 13, 562–570. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Number of Individuals | |||
|---|---|---|---|---|
| PD Cohort | Control Cohort | p Value | ||
| N = 27,041 | N = 108,149 | |||
| Gender | ||||
| Female | 13,068 (48.3%) | 52,267 (48.3%) | 0.995 | |
| Male | 13,973 (51.7%) | 55,882 (51.7%) | ||
| Age Groups | 1 | |||
| 20–29 | 4524 (16.7%) | 18,096 (16.7%) | ||
| 30–39 | 4567 (16.9%) | 18,268 (16.9%) | ||
| 40–49 | 6557 (24.2%) | 26,228 (24.3%) | ||
| 50–59 | 5746 (21.2%) | 22,972 (21.2%) | ||
| 60–69 | 3131 (11.6%) | 12,519 (11.6%) | ||
| ≥70 | 2516 (9.3%) | 10,066 (9.3%) | ||
| Income Groups | <0.001 | |||
| <20,000 | 17,429 (64.5%) | 78,921 (73%) | ||
| 20,000–39,999 | 4964 (18.4%) | 17,995 (16.6%) | ||
| 40,000–59,999 | 3032 (11.2%) | 8090 (7.5%) | ||
| ≥60,000 | 1616 (6%) | 3143 (2.9%) | ||
| Geography | <0.001 | |||
| North | 13,351 (49.4%) | 55,469 (51.3%) | ||
| Central | 5467 (20.2%) | 18,679 (17.3%) | ||
| South | 7570 (28%) | 31,141 (28.8%) | ||
| Other | 653 (2.4%) | 2860 (2.6%) | ||
| Urbanization level | <0.001 | |||
| 1 (highest) | 14,199 (52.5%) | 47,711 (44.1%) | ||
| 2 | 6613 (24.5%) | 28,190 (26.1%) | ||
| 3 | 4543 (16.8%) | 22,174 (20.5%) | ||
| 4 (lowest) | 1686 (6.2%) | 10,074 (9.3%) | ||
| Comorbid diseases | ||||
| Alcoholism | 494 (1.8%) | 2268 (2.1%) | <0.05 | |
| CAD | 5419 (20%) | 15,865 (14.7%) | <0.001 | |
| DM | 6214 (23%) | 18,835 (17.4%) | <0.001 | |
| Hyperlipidemia | 9711 (35.9%) | 28,319 (26.2%) | <0.001 | |
| Hypertension | 10,305 (38.1%) | 34,531 (31.9%) | <0.001 | |
| Obesity | 439 (1.6%) | 1318 (1.2%) | <0.001 | |
| Smoking | 4368 (16.2%) | 12,237 (11.3%) | <0.001 | |
| Stroke | 3447 (12.7%) | 10,921 (10.1%) | <0.001 | |
| Disease Incidence | Number of Individuals | |
|---|---|---|
| PD Cohort | Control Cohort | |
| N = 27,041 | N = 108,149 | |
| With Sjogren’s syndrome | 903 (3.34%) | 2389 (2.21%) |
| Without Sjogren’s syndrome | 26,138 (96.66%) | 105,760 (97.79%) |
| Crude hazard ratio | 1.52 (1.41 to 1.64) ‡ | |
| Variables | Crude | Adjusted | |
|---|---|---|---|
| HR (95% CI) | HR * (95% CI) | ||
| PD | 1.52 (1.41 to 1.64) ‡ | 1.47 (1.36 to 1.59) ‡ | |
| Gender | |||
| Female | 1 | 1 | |
| Male | 0.37 (0.34 to 0.4) ‡ | 0.36 (0.33 to 0.39) ‡ | |
| Age Groups | |||
| 20–29 | 1 | 1 | |
| 30–39 | 0.86 (0.75 to 0.98) † | 0.91 (0.8 to 1.04) | |
| 40–49 | 0.99 (0.88 to 1.11) | 1.17 (1.04 to 1.32) † | |
| 50–59 | 1.39 (1.24 to 1.55) ‡ | 1.75 (1.55 to 1.97) ‡ | |
| 60–69 | 1.62 (1.43 to 1.83) ‡ | 2.28 (1.99 to 2.61) ‡ | |
| ≥70 | 1.01 (0.88 to 1.18) | 1.64 (1.4 to 1.92) ‡ | |
| Income Groups | |||
| <20,000 | 1 | 1 | |
| 20,000–39,999 | 1.16 (1.06 to 1.26) † | 1.26 (1.14 to 1.38) ‡ | |
| 40,000–59,999 | 1.04 (0.91 to 1.18) | 1.34 (1.17 to 1.52) ‡ | |
| ≥60,000 | 1.2 (1.01 to 1.43) † | 1.58 (1.32 to 1.89) ‡ | |
| Geography | |||
| North | 1 | ||
| Central | 2.08 (1.93 to 2.25) ‡ | 2.24 (2.06 to 2.44) ‡ | |
| South | 0.78 (0.72 to 0.86) ‡ | 0.82 (0.75 to 0.9) ‡ | |
| Other | 0.73 (0.56 to 0.95) † | 0.81 (0.62 to 1.07) | |
| Urbanization level | |||
| 1 (highest) | 1 | 1 | |
| 2 | 0.91 (0.83 to 0.99) † | 0.84 (0.77 to 0.91) ‡ | |
| 3 | 0.93 (0.85 to 1.02) | 0.84 (0.77 to 0.93) † | |
| 4 | 0.89 (0.78 to 1.01) | 0.88 (0.77 to 1.01) | |
| Comorbid diseases | |||
| Alcoholism | 0.3 (0.19 to 0.45) ‡ | 0.48 (0.31 to 0.74) † | |
| CAD | 1.08 (0.99 to 1.18) | 1.07 (0.97 to 1.19) | |
| DM | 0.95 (0.87 to 1.03) | 0.92 (0.83 to 1.02) | |
| Hyperlipidemia | 0.96 (0.89 to 1.04) | 0.86 (0.79 to 0.95) † | |
| Hypertension | 0.96 (0.9 to 1.04) | 0.86 (0.78 to 0.94) † | |
| Obesity | 0.87 (0.63 to 1.2) | 0.86 (0.63 to 1.19) | |
| Smoking | 0.73 (0.65 to 0.82) ‡ | 0.82 (0.73 to 0.92) † | |
| Stroke | 0.86 (0.76 to 0.96) † | 0.82 (0.73 to 0.93) † | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Tseng, C.-F.; Liu, J.-M.; Chuang, H.-C.; Lei, W.-T.; Liu, L.Y.-M.; Yu, Y.-C.; Hsu, R.-J. Association between Periodontal Disease and Subsequent Sjögren’s Syndrome: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 771. https://doi.org/10.3390/ijerph16050771
Lin C-Y, Tseng C-F, Liu J-M, Chuang H-C, Lei W-T, Liu LY-M, Yu Y-C, Hsu R-J. Association between Periodontal Disease and Subsequent Sjögren’s Syndrome: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(5):771. https://doi.org/10.3390/ijerph16050771
Chicago/Turabian StyleLin, Chien-Yu, Chien-Fu Tseng, Jui-Ming Liu, Heng-Chang Chuang, Wei-Te Lei, Lawrence Yu-Min Liu, Yu-Chin Yu, and Ren-Jun Hsu. 2019. "Association between Periodontal Disease and Subsequent Sjögren’s Syndrome: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 16, no. 5: 771. https://doi.org/10.3390/ijerph16050771
APA StyleLin, C.-Y., Tseng, C.-F., Liu, J.-M., Chuang, H.-C., Lei, W.-T., Liu, L. Y.-M., Yu, Y.-C., & Hsu, R.-J. (2019). Association between Periodontal Disease and Subsequent Sjögren’s Syndrome: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 16(5), 771. https://doi.org/10.3390/ijerph16050771