Comparison of Objective and Perceived Access to Food Stores Associated with Intake Frequencies of Vegetables/Fruits and Meat/Fish among Community-Dwelling Older Japanese

 ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
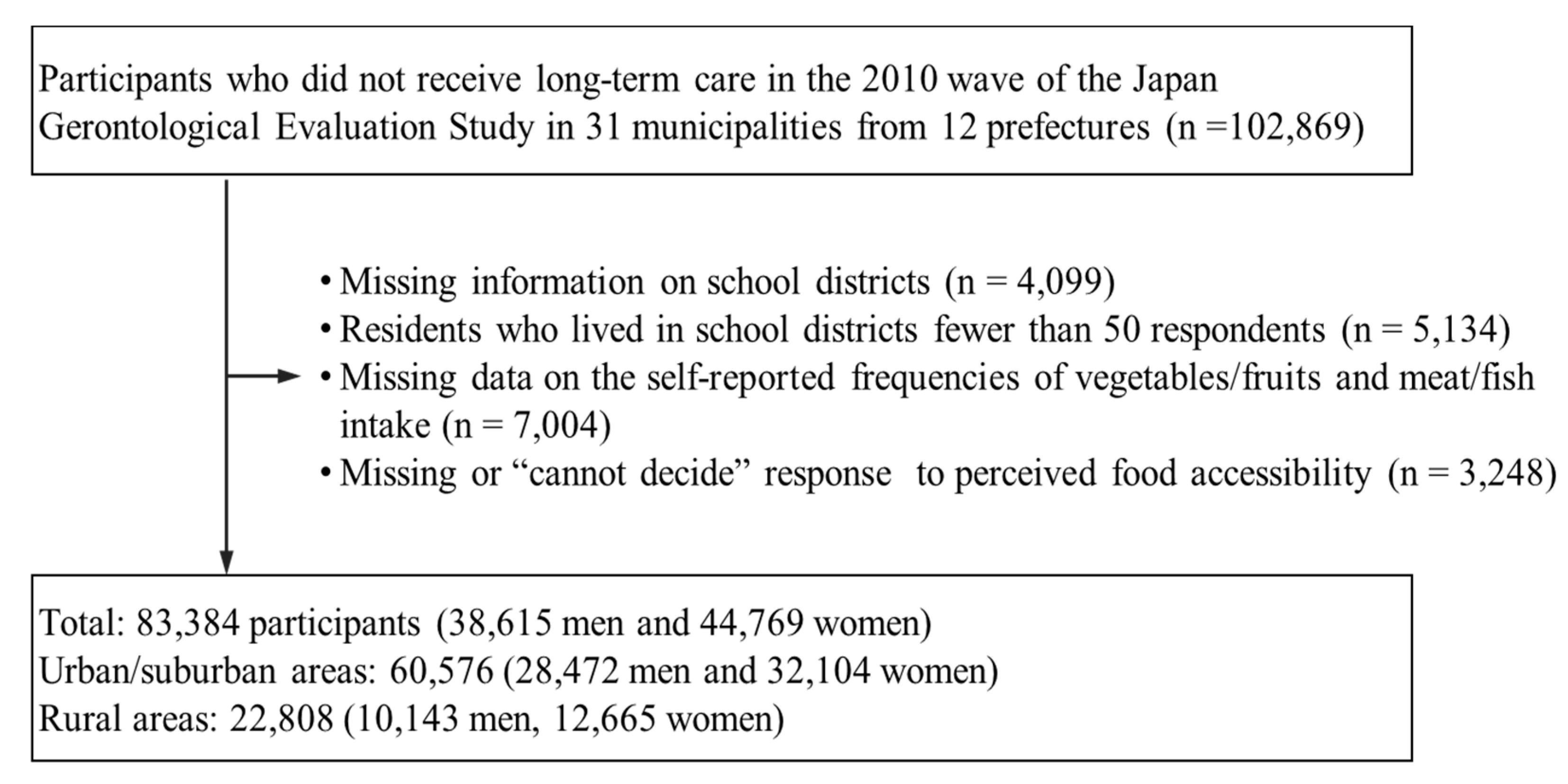
2.1. Study Participants
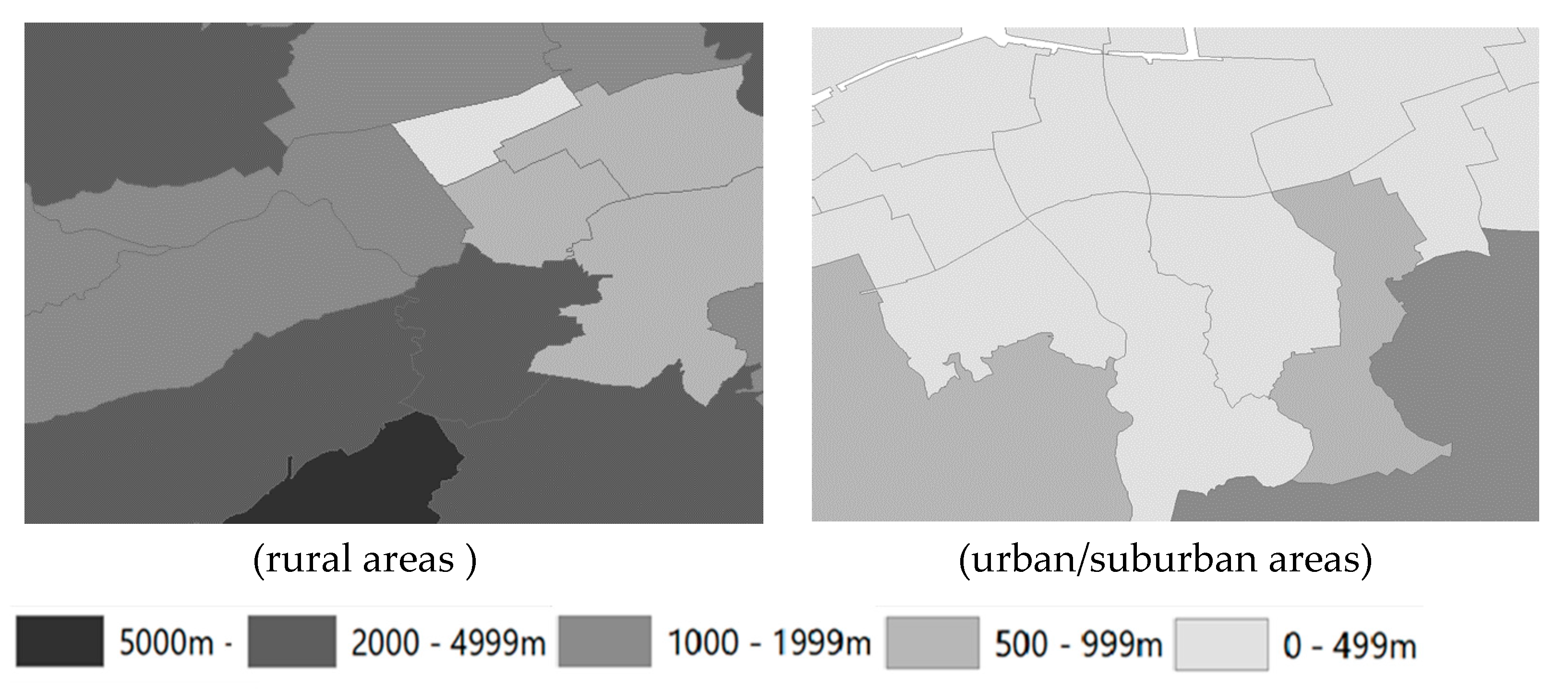
2.2. Objective Access
- the probability of the population accessing the nearest food stores located within a 50-m distance (i.e., midpoint of the radius between 0 and 100 m centered on the point of residence)over 0 m − over 100 m = 100% − 97.6% = 2.4%;
- the probability of the population accessing the nearest food stores located within 2.5 kmover 2 km − over 3 km = 12.0% − 9.4% = 2.6%;
- the probability of the population accessing the nearest food stores located within 65 kmover 60 km − over 70 km = 0.1% − 0.0% = 0.1%;
- and the weighted average of the distance to the nearest stores within the half-grid square= (50 m × 2.4% + 2.5 km × 2.6%+ 65 km × 0.1%)/(50 m + 2.5 km + 65 km).
2.3. Perceived Access
2.4. Intake Frequencies of Vegetables/Fruits and Meat/Fish
2.5. Covariates
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- White, M. Food access and obesity. Obes. Rev. 2007, 8 (Suppl. 1), 99–107. [Google Scholar] [CrossRef] [PubMed]
- Ford, P.B.; Dzewaltowski, D.A. Disparities in obesity prevalence due to variation in the retail food environment: Three testable hypotheses. Nutr. Rev. 2008, 66, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Ikejima, Y. The Reality of Food Deserts in a Large Japanese City and Their Resolution Using Urban. Agriculture; Springer Science + Business Media Singapore: Singapore, 2015. [Google Scholar]
- Iwama, N.; Asakawa, T.; Tanaka, K.; Komaki, N. Analysis of the factors that disrupt dietary habits in the elderly: A case study of a Japanese food desert. Urban. Stud. 2016, 54, 3560–3578. [Google Scholar] [CrossRef]
- Yakushiji, T.; Asakawa, T.; Iwama, N.; Takahashi, K.; Tanaka, K. Difficulties in Accessing Grocery Stores in a Super-Aged Society; Harvest-Sha: Tokyo, Japan, 2015. [Google Scholar]
- Yakushiji, T.; Takahashi, K.; Koichi, T. Accessibility to Grocery Stores in Japan A Comparison between Urban and Rural Areas by Measuring the Distance to Stores. Jpn. J. Agric. Econ. 2013, 85, 45–60. [Google Scholar]
- Ishiguro, K. Food Access Among Elderly Japanese People. Asian Soc. Work Policy Rev. 2014, 8, 275–279. [Google Scholar] [CrossRef]
- Aggarwal, A.; Cook, A.J.; Jiao, J.; Seguin, R.A.; Vernez Moudon, A.; Hurvitz, P.M.; Drewnowski, A. Access to supermarkets and fruit and vegetable consumption. Am. J. Public Health 2014, 104, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Kawachi, I.; Subramanian, S.V.; Adamkiewicz, G.; Sorensen, G. The relationship between diet and perceived and objective access to supermarkets among low-income housing residents. Soc. Sci Med. 2012, 75, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Filomena, S. The utilization of local food environments by urban seniors. Prev. Med. 2008, 47, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Lucan, S.C.; Hillier, A.; Schechter, C.B.; Glanz, K. Objective and self-reported factors associated with food-environment perceptions and fruit-and-vegetable consumption: A multilevel analysis. Prev. Chronic Dis. 2014, 11, E47. [Google Scholar] [CrossRef] [PubMed]
- Bodor, J.N.; Rose, D.; Farley, T.A.; Swalm, C.; Scott, S.K. Neighbourhood fruit and vegetable availability and consumption: The role of small food stores in an urban environment. Public Health Nutr. 2008, 11, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lee, C.K.; Seo, D.Y. Food deserts in Korea? A GIS analysis of food consumption patterns at sub-district level in Seoul using the KNHANES 2008-2012 data. Nutr. Res. Pract. 2016, 10, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Hiscock, R.; Blakely, T.; Witten, K. The contextual effects of neighbourhood access to supermarkets and convenience stores on individual fruit and vegetable consumption. J. Epidemiol. Community Health 2008, 62, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, J.R.; Johnson, C.M.; Dean, W.R. Food access and perceptions of the community and household food environment as correlates of fruit and vegetable intake among rural seniors. BMC Geriatr. 2010, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Yamada, Y.; Nanri, H.; Nozawa, Y.; Itoi, A.; Yoshimura, E.; Watanabe, Y.; Yoshida, T.; Yokoyama, K.; Goto, C.; et al. Association between the Frequency of Protein-Rich Food Intakes and Kihon-Checklist Frailty Indices in Older Japanese Adults: The Kyoto-Kameoka Study. Nutrients 2018, 10, 84. [Google Scholar] [CrossRef] [PubMed]
- Nicklett, E.J.; Kadell, A.R. Fruit and vegetable intake among older adults: A scoping review. Maturitas 2013, 75, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Hanibuchi, T.; Kondo, K.; Nakaya, T.; Nakade, M.; Ojima, T.; Hirai, H.; Kawachi, I. Neighborhood food environment and body mass index among Japanese older adults: Results from the Aichi Gerontological Evaluation Study (AGES). Int. J. Health Geogr. 2011, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Nakamura, M.; Okada, E.; Ojima, T.; Kondo, K. Association of food access and neighbor relationships with diet and underweight among community-dwelling older Japanese. J. Epidemiol. 2017, 27, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Tani, Y.; Suzuki, N.; Fujiwara, T.; Hanazato, M.; Kondo, N.; Miyaguni, Y.; Kondo, K. Neighborhood food environment and mortality among older Japanese adults: Results from the JAGES cohort study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 101. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K. Health Inequalities in Japan: An Empirical Study of Older People; Trans Pacific Press: Melbourne, Australia, 2010. [Google Scholar]
- Kondo, K. Progress in Aging Epidemiology in Japan: The JAGES Project. J. Epidemiol. 2016, 26, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Kondo, N.; Aida, J.; Kawachi, I.; Koyama, S.; Ojima, T.; Kondo, K. Development of an instrument for community-level health related social capital among Japanese older people: The JAGES Project. J. Epidemiol. 2017, 27, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Aida, J.; Hanibuchi, T.; Nakade, M.; Hirai, H.; Osaka, K.; Kondo, K. The different effects of vertical social capital and horizontal social capital on dental status: A multilevel analysis. Soc. Sci. Med. 2009, 69, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Statistics Bureau of Japan (SBJ). Population Census. Tokyo, 2010. Available online: http://www.stat.go.jp/english/data/kokusei/pdf/20111026.pdf (accessed on 1 December 2018).
- Ministry of Economy Trade and Industry. Census of Commerce. 2007 Census of Commerce. Available online: http://www.meti.go.jp/english/statistics/tyo/syougyo/index.html (accessed on 1 December 2018).
- Statistics Bureau. What is a Densely Inhabited District? Geographic Information. 1996. Available online: http://www.stat.go.jp/english/data/chiri/did/1-1.htm (accessed on 1 December 2018).
- Fujiwara, T.; Takamoto, I.; Amemiya, A.; Hanazato, M.; Suzuki, N.; Nagamine, Y.; Sasaki, Y.; Tani, Y.; Yazawa, A.; Inoue, Y.; et al. Is a hilly neighborhood environment associated with diabetes mellitus among older people? Results from the JAGES 2010 study. Soc. Sci. Med. 2017, 182, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Land, Infrastructure, Transport and Tourism. National Land Numerical Information Elevation, Degree of Slope 5th Mesh Data. 2016. Available online: http://nlftp.mlit.go.jp/ksj-e/gml/datalist/KsjTmplt-L03-a.html (accessed on 1 December 2018).
- Hanibuchi, T.; Kawachi, I.; Nakaya, T.; Hirai, H.; Kondo, K. Neighborhood built environment and physical activity of Japanese older adults: Results from the Aichi Gerontological Evaluation Study (AGES). BMC Public Health 2011, 11, 657. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Land, Infrastructure, Transport and Tourism. National Land Numerical Information Elevation, Degree of Slope 5th Mesh Data. 2011. Available online: http://nlftp.mlit.go.jp/ksj-e/gml/datalist/KsjTmplt-G04-a.html (accessed on 1 December 2018).
- Ishizaki, T.; Kobayashi, Y.; Kai, I. Functional transitions in instrumental activities of daily living among older Japanese. J. Epidemiol. 2000, 10, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Tani, Y.; Kondo, N.; Takagi, D.; Saito, M.; Hikichi, H.; Ojima, T.; Kondo, K. Combined effects of eating alone and living alone on unhealthy dietary behaviors, obesity and underweight in older Japanese adults: Results of the JAGES. Appetite 2015, 95, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Merlo, J.; Chaix, B.; Yang, M.; Lynch, J.; Rastam, L. A brief conceptual tutorial of multilevel analysis in social epidemiology: Linking the statistical concept of clustering to the idea of contextual phenomenon. J. Epidemiol. Community Health 2005, 59, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Kamiyama, C.; Hashimoto, S.; Hsaka, R.; Saito, O. Non-market food provisioning services via homegardens and communal sharing in satoyama socio-ecological production landscapes on Japan’s Noto peninsula. Ecosyst. Serv. 2016, 17, 185–196. [Google Scholar] [CrossRef]
- Plieninger, T.; Kohsaka, R.; Bieling, C.; Hashimoto, S.; Kamiyama, C.; Kizos, T.; Penker, M.; Kieninger, P.; Shaw, B.J.; Sioen, G.B.; et al. Fostering biocultural diversity in landscapes through place-based food networks: A “solution scan” of European and Japanese models. Sustain. Sci. 2018, 13, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Sproesser, G.; Imada, S.; Furumitsu, I.; Rozin, P.; Ruby, M.B.; Arbit, N.; Fischler, C.; Schupp, H.T.; Renner, B. What Constitutes Traditional and Modern Eating? The Case of Japan. Nutrients 2018, 10, 118. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Ogawa, H.; Yoshihara, A.; Yamaga, T.; Takiguchi, T.; Wada, T.; Sakamoto, R.; Ishimoto, Y.; Fukutomi, E.; Chen, W.; et al. Evaluation of chewing ability and its relationship with activities of daily living, depression, cognitive status and food intake in the community-dwelling elderly. Geriatr. Gerontol. Int. 2013, 13, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.V.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total a n = 83,384 | Poor Objective Access n = 30,383 | Poor Perceived Access n = 21,105 | |
|---|---|---|---|
| Objective access: poor, n (%) | 30,383 | - | 10,696 (50.7) |
| Perceived access: poor, n (%) | 21,105 | 10,696 (35.2) | - |
| Age (years), mean (SD) | 73.9 (6.2) | 74.5 (6.4) | 74.2 (6.4) |
| Men, n (%) | 38,615 | 13,604 (44.8) | 8954 (42.3) |
| Family structure, n (%) | |||
| Alone | 9896 | 3513 (11.6) | 2849 (13.5) |
| With their spouse | 31,151 | 10,876 (35.8) | 7463 (35.4) |
| With others | 41,139 | 15,485 (51.0) | 10,456 (49.5) |
| Unknown | 1198 | 509 (1.7) | 337 (1.6) |
| Marital status, n (%) | |||
| Married | 59,313 | 21,227 (69.9) | 14,199 (67.3) |
| Divorced or widowed | 20,740 | 7926 (26.1) | 6005 (28.5) |
| Never married or others | 2036 | 616 (2.0) | 544 (2.6) |
| Unknown | 1295 | 614 (2.0) | 357 (1.7) |
| Body mass index (kg/m2), n (%) | |||
| <18.5 | 5759 | 1987 (6.5) | 1556 (7.4) |
| 18.5–24.9 | 56,671 | 20,316 (66.9) | 14,138 (67.0) |
| ≥25 | 15,917 | 6572 (21.6) | 4396 (20.8) |
| Unknown | 1665 | 1508 (5.0) | 1015 (4.8) |
| Activity daily living (units), n (%) | |||
| <5 | 16,926 | 6430 (21.2) | 4944 (23.4) |
| ≥5 | 64,453 | 23,071 (75.9) | 15,577 (73.8) |
| Unknown | 2005 | 882 (2.9) | 584 (2.8) |
| Remaining teeth (number), n (%) | |||
| <20 | 54,238 | 21,697 (71.4) | 14,407 (68.3) |
| ≥20 | 27,535 | 8040 (26.5) | 6267 (29.7) |
| Unknown | 1611 | 646 (2.1) | 431 (2.0) |
| Comorbidity, n (%) | |||
| No | 11,491 | 4107 (13.5) | 3052 (14.5) |
| Yes | 52,049 | 19,206 (63.2) | 13,409 (63.5) |
| Unknown | 19,844 | 7070 (23.3) | 4644 (22.0) |
| Smoking status | |||
| Current | 8735 | 2977 (9.8) | 2125 (10.1) |
| Past or never | 69,660 | 25,041 (82.4) | 17,496 (82.9) |
| Unknown | 4989 | 2365 (7.8) | 1484 (7.0) |
| Household income (million yen/year), n (%) | |||
| <2.00 | 34,481 | 13,887 (45.7) | 9266 (43.9) |
| 2.00–3.99 | 26,667 | 8442 (27.8) | 6136 (29.1) |
| ≥4.00 | 7649 | 2048 (6.7) | 1669 (7.9) |
| Unknown | 14,587 | 6006 (19.8) | 4034 (19.1) |
| Years of schooling (years), n (%) | |||
| ≤9 | 38,634 | 15,225 (50.1) | 10,336 (49.0) |
| 10–12 | 28,557 | 10,058 (33.1) | 7012 (33.2) |
| ≥13 | 14,267 | 4328 (14.2) | 3201 (15.2) |
| Unknown | 1926 | 772 (2.5) | 556 (2.6) |
| Car use, n (%) | |||
| Yes | 61,925 | 26,125 (86.0) | 16,270 (77.1) |
| No | 12,550 | 3729 (12.3) | 3099 (14.7) |
| Unknown | 8909 | 529 (1.7) | 1736 (8.2) |
| Community level | |||
| Urban/suburban area, n (%) | 60,576 | 11,107 (36.6) | 13,044 (61.8) |
| Convenience stores (number), mean (SD) | 3.6 (3.1) | 2.3 (2.1) | 3.0 (3.0) |
| Land slope (degree), mean (SD) | 4.9 (5.9) | 9.4 (7.0) | 6.7 (7.2) |
| Vegetables/fruits intake (times/day), mean (SD) | 1.4 (0.6) | 1.4 (0.6) | 1.3 (0.6) |
| Meat/fish intake (times/day), mean (SD) | 0.8 (0.5) | 0.8 (0.5) | 0.7 (0.5) |
| Objective Access | Perceived Access | |||
|---|---|---|---|---|
| β (SE) | p-Value | β (SE) | p-Value | |
| Vegetables/fruits | ||||
| Poor access (vs. good access) | 0.086 (0.021) | <0.001 | −0.093 (0.009) | <0.001 |
| Age | 0.018 (0.001) | <0.001 | 0.018 (0.001) | <0.001 |
| Men (vs. women) | −0.376 (0.009) | <0.001 | −0.379 (0.009) | <0.001 |
| Living alone (vs. with others) | 0.041 (0.014) | 0.004 | 0.042 (0.014) | 0.003 |
| Never married or others (vs. married) | −0.184 (0.026) | <0.001 | −0.182 (0.026) | <0.001 |
| BMI (vs. 18.5–24.9 kg/m2) | ||||
| <18.5 | −0.010 (0.015) | 0.494 | −0.010 (0.015) | 0.528 |
| ≥25 | −0.096 (0.009) | <0.001 | −0.096 (0.009) | <0.001 |
| Activity daily living, <5 units (vs. ≥5) | −0.137 (0.010) | <0.001 | −0.132 (0.010) | <0.001 |
| Remaining teeth, <20 tooth (vs. ≥20) | −0.217 (0.009) | <0.001 | −0.215 (0.009) | <0.001 |
| Comorbidity, yes (vs. no) | −0.028 (0.011) | 0.015 | −0.028 (0.011) | 0.013 |
| Current smoking (vs. never) | −0.243 (0.012) | <0.001 | −0.243 (0.012) | <0.001 |
| Household income, <2.00 million yen/year (vs. 2.00–3.99) | −0.173 (0.009) | <0.001 | −0.171 (0.009) | <0.001 |
| Years of schooling, <9 years (vs. 10–12) | −0.133 (0.009) | <0.001 | −0.131 (0.009) | <0.001 |
| No car-use (vs. use) | −0.133 (0.011) | <0.001 | −0.135 (0.011) | <0.001 |
| Urban/suburban area (vs. rural area) | 0.004 (0.023) | 0.850 | −0.050 (0.021) | 0.017 |
| Convenience store | −0.002 (0.002) | 0.276 | −0.003 (0.002) | 0.145 |
| Land slope | −0.001 (0.001) | 0.346 | 0.001 (0.001) | 0.319 |
| Var RE (SE) | ICC (SE) | Var RE (SE) | ICC (SE) | |
| 0.008 (0.001) | 0.008 (0.001) | 0.010 (0.001) | 0.010 (0.001) | |
| Meat/fish | ||||
| Poor access (vs. good access) | 0.021 (0.014) | 0.130 | −0.029 (0.004) | <0.001 |
| Age | 0.005 (0.0003) | <0.001 | 0.005 (0.0003) | <0.001 |
| Men (vs. women) | −0.075 (0.004) | <0.001 | −0.076 (0.004) | <0.001 |
| Living alone (vs. with others) | −0.025 (0.007) | <0.001 | −0.025 (0.007) | <0.001 |
| Never married or others (vs. married) | −0.057 (0.012) | <0.001 | −0.057 (0.012) | <0.001 |
| BMI (vs. 18.5–24.9 kg/m2) | ||||
| <18.5 | 0.005 (0.007) | 0.486 | 0.005 (0.007) | 0.459 |
| ≥25 | −0.019 (0.004) | <0.001 | −0.019 (0.004) | <0.001 |
| Activity daily living, <5 units (vs. ≥5) | −0.042 (0.005) | <0.001 | −0.040 (0.005) | <0.001 |
| Remaining teeth, <20 tooth (vs. ≥20) | −0.082 (0.004) | <0.001 | −0.082 (0.004) | <0.001 |
| Comorbidity, yes (vs. no) | −0.008 (0.005) | 0.135 | −0.008 (0.005) | 0.126 |
| Current smoking (vs. never) | −0.014 (0.006) | 0.017 | −0.014 (0.006) | 0.018 |
| Household income, <2.00 million yen/year (vs. 2.00–3.99) | −0.080 (0.004) | <0.001 | −0.079 (0.004) | <0.001 |
| Years of schooling, <9 years (vs. 10–12) | −0.081 (0.004) | <0.001 | −0.081 (0.004) | <0.001 |
| No car-use (vs. use) | −0.020 (0.005) | <0.001 | −0.021 (0.005) | <0.001 |
| Urban/suburban area (vs. rural area) | 0.037 (0.015) | 0.014 | 0.023 (0.013) | 0.080 |
| Convenience store | −0.0004 (0.001) | 0.704 | −0.001 (0.001) | 0.596 |
| Land slope | 0.001 (0.001) | 0.102 | 0.002 (0.001) | 0.011 |
| Var RE (SE) | ICC (SE) | Var RE (SE) | ICC (SE) | |
| 0.005 (0.0005) | 0.019 (0.002) | 0.005 (0.0005) | 0.019 (0.002) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, M.; Takahashi, K.; Hanazato, M.; Suzuki, N.; Kondo, K.; Kondo, N. Comparison of Objective and Perceived Access to Food Stores Associated with Intake Frequencies of Vegetables/Fruits and Meat/Fish among Community-Dwelling Older Japanese. Int. J. Environ. Res. Public Health 2019, 16, 772. https://doi.org/10.3390/ijerph16050772
Yamaguchi M, Takahashi K, Hanazato M, Suzuki N, Kondo K, Kondo N. Comparison of Objective and Perceived Access to Food Stores Associated with Intake Frequencies of Vegetables/Fruits and Meat/Fish among Community-Dwelling Older Japanese. International Journal of Environmental Research and Public Health. 2019; 16(5):772. https://doi.org/10.3390/ijerph16050772
Chicago/Turabian StyleYamaguchi, Miwa, Katsuya Takahashi, Masamichi Hanazato, Norimichi Suzuki, Katsunori Kondo, and Naoki Kondo. 2019. "Comparison of Objective and Perceived Access to Food Stores Associated with Intake Frequencies of Vegetables/Fruits and Meat/Fish among Community-Dwelling Older Japanese" International Journal of Environmental Research and Public Health 16, no. 5: 772. https://doi.org/10.3390/ijerph16050772
APA StyleYamaguchi, M., Takahashi, K., Hanazato, M., Suzuki, N., Kondo, K., & Kondo, N. (2019). Comparison of Objective and Perceived Access to Food Stores Associated with Intake Frequencies of Vegetables/Fruits and Meat/Fish among Community-Dwelling Older Japanese. International Journal of Environmental Research and Public Health, 16(5), 772. https://doi.org/10.3390/ijerph16050772