Mortality Risk and Risk Factors in Patients with Posttraumatic Epilepsy: A Population-Based Cohort Study


Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Patient Selection
2.3. Statistical Analysis
3. Results
3.1. Demographics of Study Cohorts
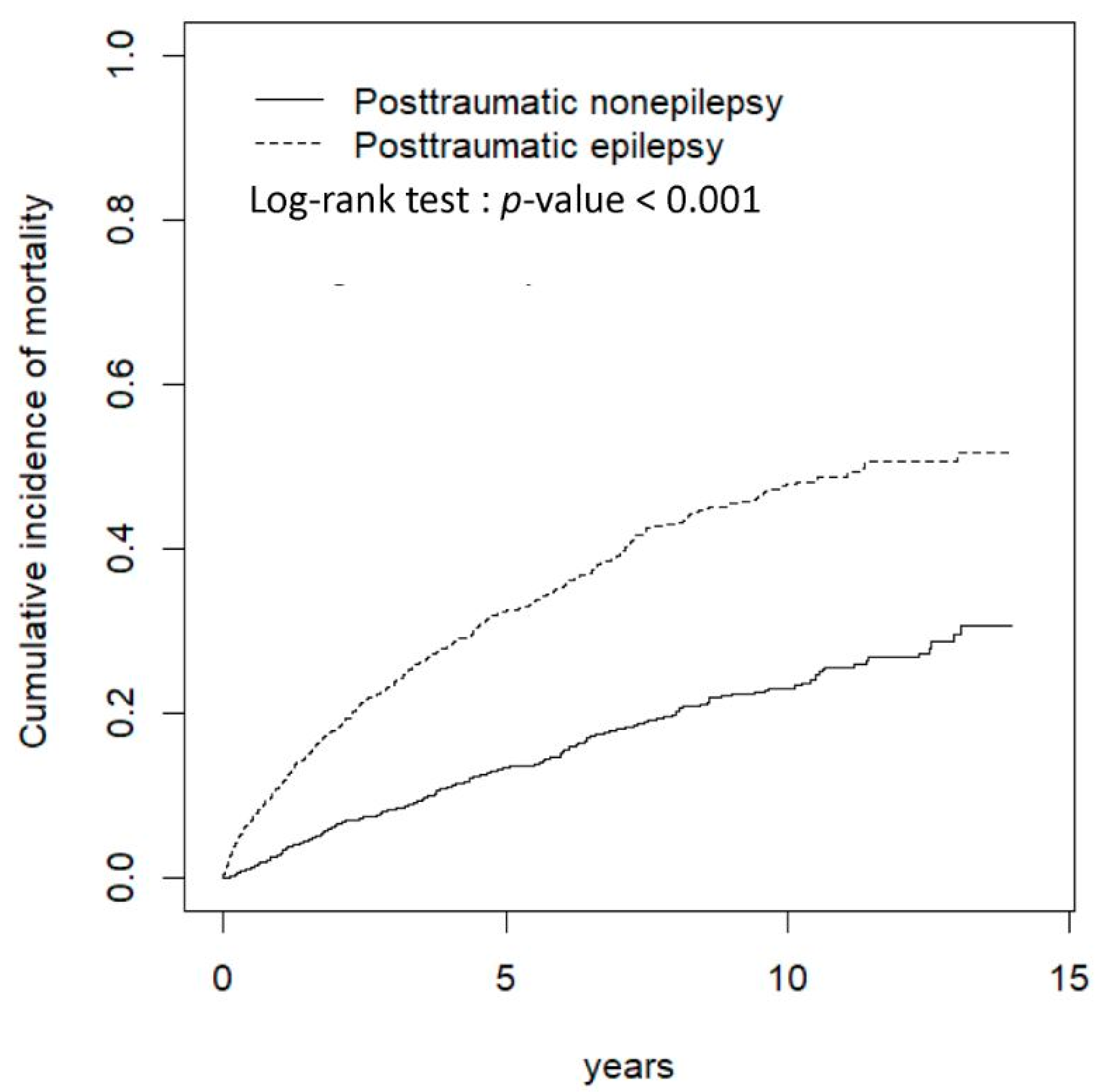
3.2. Mortality Risk in Patients with PTE
3.3. AED Use and Mortality Risk
3.4. Increased Medical Burden in Patients with PTE
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| aHR | adjusted hazard ratio |
| CI | confidence interval |
| NHIRD | National Health Insurance Research Database |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
References
- Centers for Disease Control and Prevention. Report to Congress. Traumatic brain injury in the United States: Epidemiology and rehabilitation. Atlanta: National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention. 2015. Available online: https://www.cdc.gov/traumaticbraininjury/pubs/congress_epi_rehab.html (accessed on 15 February 2019).
- Perry, D.C.; Sturm, V.E.; Peterson, M.J.; Pieper, C.F.; Bullock, T.; Boeve, B.F.; Miller, B.L.; Guskiewicz, K.M.; Berger, M.S.; Kramer, J.H.; et al. Association of traumatic brain injury with subsequent neurological and psychiatric disease: A meta-analysis. J. Neurosurg. 2016, 124, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Gulf war and health. In Volume 7: Long-Term Consequences of Traumatic Brain Injury; The National Academies Press: Washington, DC, USA, 2009; Available online: https://www.nap.edu/read/12436/chapter/9 (accessed on 15 February 2019).
- Ventura, T.; Harrison-Felix, C.; Carlson, N.; Diguiseppi, C.; Gabella, B.; Brown, A.; Devivo, M.; Whiteneck, G. Mortality after discharge from acute care hospitalization with traumatic brain injury: A population-based study. Arch. Phys. Med. Rehabil. 2010, 91, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Baguley, I.J.; Nott, M.T.; Howle, A.A.; Simpson, G.K.; Browne, S.; King, A.C.; Cotter, R.E.; Hodgkinson, A. Late mortality after severe traumatic brain injury in New South Wales: A multicentre study. Med. J. Aust. 2012, 196, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Hesdorffer, D.C.; Logroscino, G.; Benn, E.K.; Katri, N.; Cascino, G.; Hauser, W.A. Estimating risk for developing epilepsy: A population-based study in Rochester, Minnesota. Neurology 2011, 76, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Annegers, J.F.; Hauser, W.A.; Coan, S.P.; Rocca, W.A. A population-based study of seizures after traumatic brain injuries. N. Engl. J. 1998, 338, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Yu, X.; Ou, S.; Liu, X.; Yuan, J.; Huang, H.; Yang, J.; He, L.; Chen, Y. Risk factors for posttraumatic epilepsy: A systematic review and meta-analysis. Epilepsy Behav. 2017, 67, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.; Pedersen, M.G.; Pedersen, C.B.; Sidenius, P.; Olsen, J.; Vestergaard, M. Long-term risk of epilepsy after traumatic brain injury in children and young adults: A population-based cohort study. Lancet 2009, 373, 1105–1110. [Google Scholar] [CrossRef]
- Rao, V.; Parko, K. Clinical approach to posttraumatic epilepsy. Semin. Neurol. 2015, 35, 57–63. [Google Scholar] [PubMed]
- Mahler, B.; Carlsson, S.; Andersson, T.; Adelöw, C.; Ahlbom, A.; Tomson, T. Unprovoked seizures after traumatic brain injury: A population-based case-control study. Epilepsia 2015, 56, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Lhatoo, S.D.; Johnson, A.L.; Goodridge, D.M.; MacDonald, B.K.; Sander, J.W.; Shorvon, S.D. Mortality in epilepsy in the first 11 to 14 years after diagnosis: Multivariate analysis of a long-term, prospective, population-based cohort. Ann. Neurol. 2001, 49, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.W.; Han, M. Cultural orientation in Southeast Asian American young adults. Cultur. Divers. Ethn. Minor. Psychol. 2008, 14, 29–37. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Research Database. Available online: http://nhird.nhri.org.tw/en/index.html (accessed on 19 January 2019).
- Forsgren, L.; Hauser, W.A.; Olafsson, E.; Sander, J.W.; Sillanpää, M.; Tomson, T. Mortality of epilepsy in developed countries: A review. Epilepsia 2005, 46 (Suppl. 11), 18–27. [Google Scholar] [CrossRef] [PubMed]
- Levira, F.; Thurman, D.J.; Sander, J.W.; Hauser, W.A.; Hesdorffer, D.C.; Masanja, H.; Odermatt, P.; Logroscino, G.; Newton, C.R. Epidemiology Commission of the International League Against Epilepsy. Premature mortality of epilepsy in low- and middle-income countries: A systematic review from the Mortality Task Force of the International League Against Epilepsy. Epilepsia 2017, 58, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Lusardi, T.A.; Akula, K.K.; Coffman, S.Q.; Ruskin, D.N.; Masino, S.A.; Boison, D. Ketogenic diet prevents epileptogenesis and disease progression in adult mice and rats. Neuropharmacology 2015, 99, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Pitkänen, A.; Kharatishvili, I.; Karhunen, H.; Lukasiuk, K.; Immonen, R.; Nairismägi, J.; Gröhn, O.; Nissinen, J. Epileptogenesis in experimental models. Epilepsia 2017, 48 (Suppl. 2), 13–20. [Google Scholar] [CrossRef]
- Keezer, M.R.; Bell, G.S.; Neligan, A.; Novy, J.; Sander, J.W. Cause of death and predictors of mortality in a community-based cohort of people with epilepsy. Neurology 2016, 86, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Uski, J.; Lamusuo, S.; Teperi, S.; Löyttyniemi, E.; Tenovuo, O. Mortality after traumatic brain injury and the effect of posttraumatic epilepsy. Neurology 2018, 91, e878–e883. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.; Yip, W.; Chang, H.J.; Chou, Y.J. Trends in rural and urban differentials in incidence rates for ruptured appendicitis under the National Health Insurance in Taiwan. Public Health 2006, 120, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.C.; Lin, J.W.; Lin, Y.F.; Hsu, N.C.; Ko, W.J. Evaluating the performance of a hospitalist system in Taiwan: A pioneer study for nationwide health insurance in Asia. J. Hosp. Med. 2011, 6, 378–382. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Propensity Score Matched | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Posttraumatic Nonepilepsy n = 1425 | Posttraumatic Epilepsy n = 1425 | Posttraumatic Nonepilepsy n = 891 | Posttraumatic Epilepsy n = 891 | |||||||
| n | % | n | % | p-Value | n | % | n | % | p-Value | |
| Age, year | 0.99 | 0.98 | ||||||||
| 20–49 | 623 | 43.7 | 623 | 43.7 | 583 | 65.4 | 582 | 65.3 | ||
| 50–64 | 321 | 22.5 | 321 | 22.5 | 135 | 15.2 | 133 | 14.9 | ||
| 65+ | 481 | 33.8 | 481 | 33.8 | 173 | 19.4 | 176 | 19.8 | ||
| Mean (SD) § | 54.2 | 19.7 | 54.5 | 19.6 | 0.74 | 54.6 | 19.9 | 54.4 | 19.9 | 0.84 |
| Sex | 0.99 | 0.92 | ||||||||
| Female | 435 | 30.5 | 435 | 30.5 | 290 | 32.6 | 288 | 32.3 | ||
| Male | 990 | 69.5 | 990 | 69.5 | 601 | 67.5 | 603 | 67.7 | ||
| Comorbidity | ||||||||||
| Alcohol-related illness | 124 | 8.70 | 300 | 21.1 | <0.001 | 114 | 12.8 | 102 | 11.5 | 0.38 |
| Anxiety | 278 | 19.5 | 422 | 29.6 | <0.001 | 226 | 25.4 | 229 | 25.7 | 0.87 |
| Mental disorders | 547 | 38.4 | 890 | 62.5 | <0.001 | 448 | 50.3 | 443 | 49.7 | 0.81 |
| Insomnia | 722 | 50.7 | 1079 | 75.7 | <0.001 | 591 | 66.3 | 587 | 65.9 | 0.84 |
| Depression | 98 | 6.88 | 200 | 14.0 | <0.001 | 89 | 9.99 | 89 | 9.99 | 0.99 |
| Stroke | 136 | 9.54 | 393 | 27.6 | 0.06 | 127 | 14.3 | 133 | 14.9 | 0.69 |
| Chronic obstructive pulmonary disease (COPD) | 211 | 14.8 | 377 | 26.5 | <0.001 | 178 | 20.0 | 188 | 21.1 | 0.56 |
| Coronary artery disease (CAD) | 304 | 21.3 | 346 | 24.3 | <0.001 | 220 | 24.7 | 214 | 24.0 | 0.74 |
| Diabetes | 153 | 10.7 | 244 | 17.1 | <0.001 | 121 | 13.6 | 126 | 14.1 | 0.73 |
| Hypertension | 537 | 37.7 | 705 | 49.5 | <0.001 | 389 | 43.7 | 381 | 42.8 | 0.70 |
| Hyperlipidemia | 307 | 21.5 | 328 | 23.0 | 0.34 | 200 | 22.5 | 201 | 22.6 | 0.95 |
| Variable | Propensity Score Matched | |||
|---|---|---|---|---|
| Posttraumatic Nonepilepsy | Posttraumatic Epilepsy | Posttraumatic Nonepilepsy | Posttraumatic Epilepsy | |
| (n = 1425) | (n = 1425) | (n = 891) | (n = 891) | |
| Mortality | ||||
| Person-years | 9126 | 7438 | 5577 | 4846 |
| Follow-up time (y) | 6.40 ± 3.80 | 5.22 ± 3.79 | 4.36 ± 3.17 | 3.91 ± 2.97 |
| No. of event | 252 | 534 | 172 | 297 |
| Incidence rate | 27.6 | 71.8 | 30.8 | 61.3 |
| Crude HR (95% CI) | 1 (Reference) | 2.53 (2.18, 2.94) *** | 1 (Reference) | 1.96 (1.62, 2.36) *** |
| Adjusted HR a (95% CI) | 1 (Reference) | 2.31 (1.96, 2.73) *** | 1 (Reference) | 2.28 (1.88, 2.75) *** |
| Variable | Propensity Score Matched | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Posttraumatic Nonepilepsy | Posttraumatic Epilepsy | Posttraumatic Nonepilepsy | Posttraumatic Epilepsy | |||||||||
| n = 1425 | n = 1425 | n = 891 | n = 891 | |||||||||
| Event No. | Rate | Event No. | Rate | Crude HR (95% CI) | Adjusted HR a (95% CI) | Event No. | Rate | Event No. | Rate | Crude HR (95% CI) | Adjusted HR a (95% CI) | |
| Age, year | ||||||||||||
| 20–49 | 53 | 11.5 | 133 | 32.3 | 2.78 (2.02, 3.83) *** | 1.78 (1.23, 2.56) ** | 65 | 16.0 | 126 | 33.8 | 2.10 (1.56, 2.83) *** | 2.13 (1.57, 2.89) *** |
| 50–64 | 34 | 16.1 | 114 | 68.7 | 4.14 (2.82, 6.07) *** | 3.39 (2.25, 5.11) *** | 34 | 43.7 | 63 | 107.1 | 2.41 (1.59, 3.67) *** | 2.75 (1.74, 4.34) *** |
| 65+ | 165 | 68.6 | 287 | 172.5 | 2.48 (2.04, 3.00) *** | 2.00 (1.62, 2.45) *** | 73 | 99.6 | 108 | 203.0 | 2.05 (1.51, 2.77) *** | 2.17 (1.59, 2.98) *** |
| Sex | ||||||||||||
| Female | 71 | 26.6 | 160 | 74.9 | 2.74 (2.07, 3.63) *** | 2.54 (1.88, 3.44) *** | 53 | 31.0 | 96 | 66.0 | 2.11 (1.51, 2.94) *** | 2.42 (1.72, 3.42) *** |
| Male | 181 | 28.0 | 374 | 70.6 | 2.44 (2.05, 2.92) *** | 2.21 (1.82, 2.69) *** | 119 | 30.8 | 201 | 59.3 | 1.89 (1.51, 2.37) *** | 2.24 (1.78, 2.82) *** |
| Comorbidity | ||||||||||||
| None | 41 | 12.5 | 18 | 20.0 | 1.59 (0.92, 2.78) | 1.98 (1.12, 3.47) * | 15 | 11.9 | 18 | 20.0 | 1.64 (0.83, 3.26) | 1.67 (0.83, 3.33) |
| With any one | 211 | 36.2 | 516 | 78.9 | 2.15 (1.83, 2.53) *** | 2.71 (2.31, 3.19) *** | 157 | 36.4 | 279 | 70.7 | 1.92 (1.58, 2.34) *** | 2.20 (1.81, 2.68) *** |
| Variables | n | Event | Person-Years | Rate | Crude HR (95% CI) | Adjusted HR a (95% CI) | Crude HR (95% CI) | Adjusted HR a (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Posttraumatic nonepilepsy | 1425 | 252 | 9126 | 27.6 | 1(Reference) | 1(Reference) | ||
| Posttraumatic epilepsy | ||||||||
| Without antiepileptic drug | 42 | 5 | 289 | 17.3 | 0.63 (0.26, 1.55) | 0.83 (0.34, 2.01) | 1 (Reference) | 1 (Reference) |
| One antiepileptic drug | 219 | 68 | 1433 | 47.4 | 1.73 (1.32, 2.26) *** | 2.05 (1.56, 2.69) *** | 2.70 (1.09, 6.69) * | 2.48 (0.99, 6.18) |
| Two antiepileptic drugs | 515 | 198 | 2846 | 69.6 | 2.48 (2.06, 2.99) *** | 2.28 (1.87, 2.78) *** | 3.85 (1.58, 9.34) ** | 2.89 (1.18, 7.07) * |
| More than two antiepileptic drugs | 649 | 263 | 2870 | 91.6 | 3.13 (2.63, 3.72) *** | 2.63 (2.17, 3.19) *** | 4.78 (1.97, 11.6) *** | 3.30 (1.35, 8.08) ** |
| Variable | Parameter Estimate | Standard Error | 95% CI |
|---|---|---|---|
| Intercept | −27.9 | 5.28 | (−38.2, −17.5) *** |
| Posttraumatic epilepsy vs. Posttraumatic nonepilepsy | 28.2 | 2.72 | (22.9, 33.5) *** |
| Age | 0.51 | 0.08 | (0.35, 0.68) *** |
| Stroke | 12.8 | 4.19 | (4.57, 21.0) ** |
| Diabetes | 11.9 | 4.13 | (3.74, 20.0) ** |
| COPD | 10.2 | 3.79 | (2.78, 17.6) ** |
| Anxiety | −13.2 | 3.65 | (−20.4, −6.07) *** |
| Depression | 19.1 | 5.17 | (8.94, 29.2) *** |
| Sex (male vs. female) | 6.19 | 3.02 | (0.26, 12.1) * |
| Variable | Parameter Estimate | Standard Error | 95% CI |
|---|---|---|---|
| Intercept | 2.44 | 2.22 | (−1.91, 6.89) |
| Posttraumatic epilepsy vs. Posttraumatic nonepilepsy | 7.85 | 1.27 | (5.36, 10.3) *** |
| Age | 0.20 | 0.05 | (0.11, 0.29) *** |
| Hyperlipidemia | 5.82 | 1.75 | (2.38, 9.26) *** |
| CAD | 5.95 | 1.85 | (2.33, 9.58) *** |
| Insomnia | 5.68 | 1.46 | (2.81, 8.55) *** |
| Mental disorders | 4.15 | 1.43 | (1.35, 6.95) ** |
| Hypertension | 4.73 | 1.81 | (1.18, 8.28) ** |
| COPD | 5.17 | 1.78 | (1.67, 8.68) ** |
| Diabetes | 5.38 | 2.01 | (1.44, 9.32) ** |
| Depression | 5.06 | 2.26 | (0.63, 9.50) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, W.-J.; Harnod, T.; Lin, C.-L.; Kao, C.-H. Mortality Risk and Risk Factors in Patients with Posttraumatic Epilepsy: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 589. https://doi.org/10.3390/ijerph16040589
Lin W-J, Harnod T, Lin C-L, Kao C-H. Mortality Risk and Risk Factors in Patients with Posttraumatic Epilepsy: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(4):589. https://doi.org/10.3390/ijerph16040589
Chicago/Turabian StyleLin, Wei-Jun, Tomor Harnod, Cheng-Li Lin, and Chia-Hung Kao. 2019. "Mortality Risk and Risk Factors in Patients with Posttraumatic Epilepsy: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 16, no. 4: 589. https://doi.org/10.3390/ijerph16040589
APA StyleLin, W.-J., Harnod, T., Lin, C.-L., & Kao, C.-H. (2019). Mortality Risk and Risk Factors in Patients with Posttraumatic Epilepsy: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 16(4), 589. https://doi.org/10.3390/ijerph16040589