The Relationship between Different Types of Alarm Sounds and Children’s Perceived Risk Based on Their Physiological Responses

 , ,
, ,
Abstract
1. Introduction
1.1. Evacuation Behaviours
1.2. Alarm Sounds
1.3. Risk Perception of Evacuees
1.4. Physiological Responses
1.5. Aims and Contributions
- What is the significance of the effects of different types of alarm sounds on the physiological indicators of children?
- What are the effects of three different types of alarm sounds (voice alert, warning alarm and combined) on the physiological responses of children, and which type of alarm sound is more effective in alerting children to perceive risks?
- Does age/gender have an influence on children’s reception of alarm sound signals to perceive risks?
2. Methods
2.1. Experimental Setting
2.2. Participants
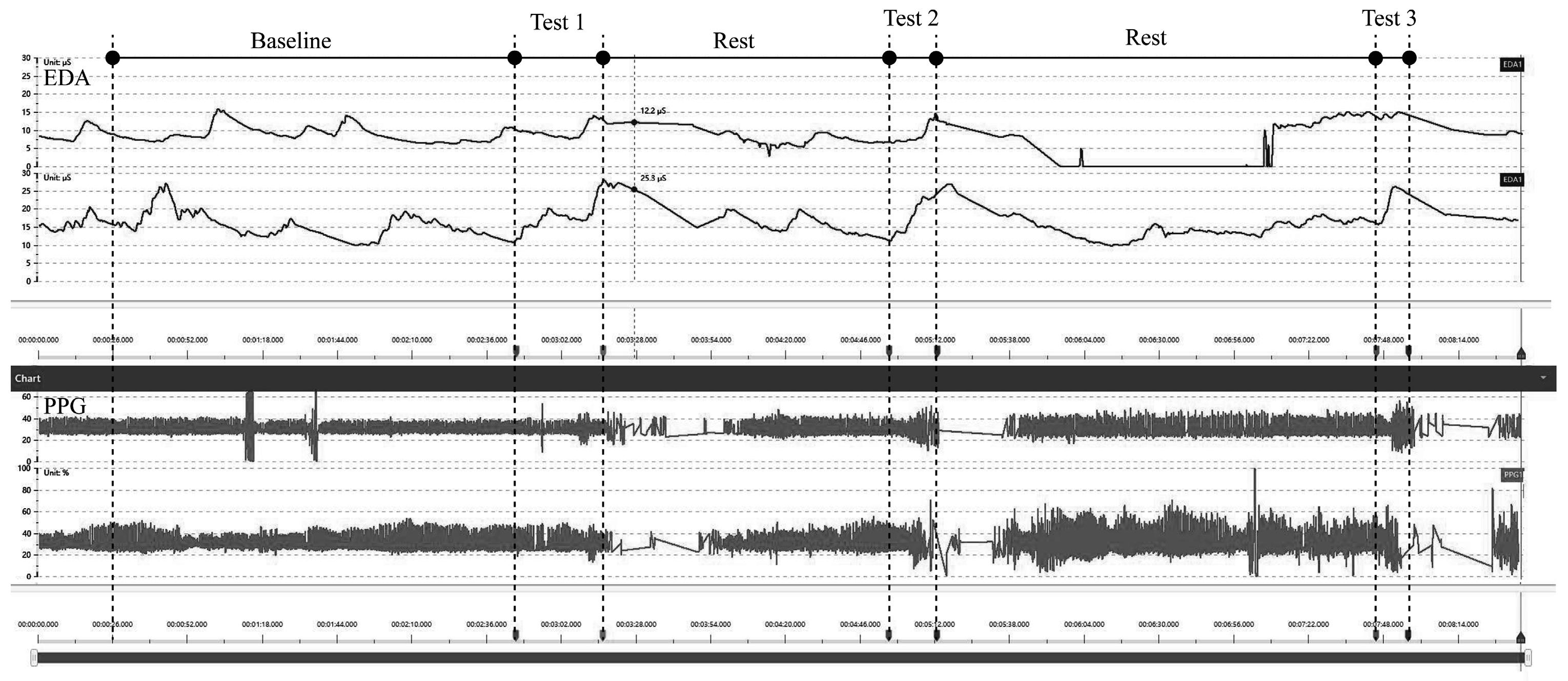
2.3. Physiological Measurements
2.4. Experimental Procedure
2.5. Data Analysis
- By repeating the measurement, based on paired t-tests 95% confidence level, the statistical significance of the differences between the scores was further evaluated to determine the differences among the physiological data corresponding to different types of alarm sounds.
- Normalisation was performed of the baseline data of all data points relative to the resting state and all individual differences between subjects were eliminated, so that the processed data could be compared to the results obtained without alarm sound stimulation.
3. Results
3.1. The Significance of the Influence of Alarm Sound on Different Physiological Indicators
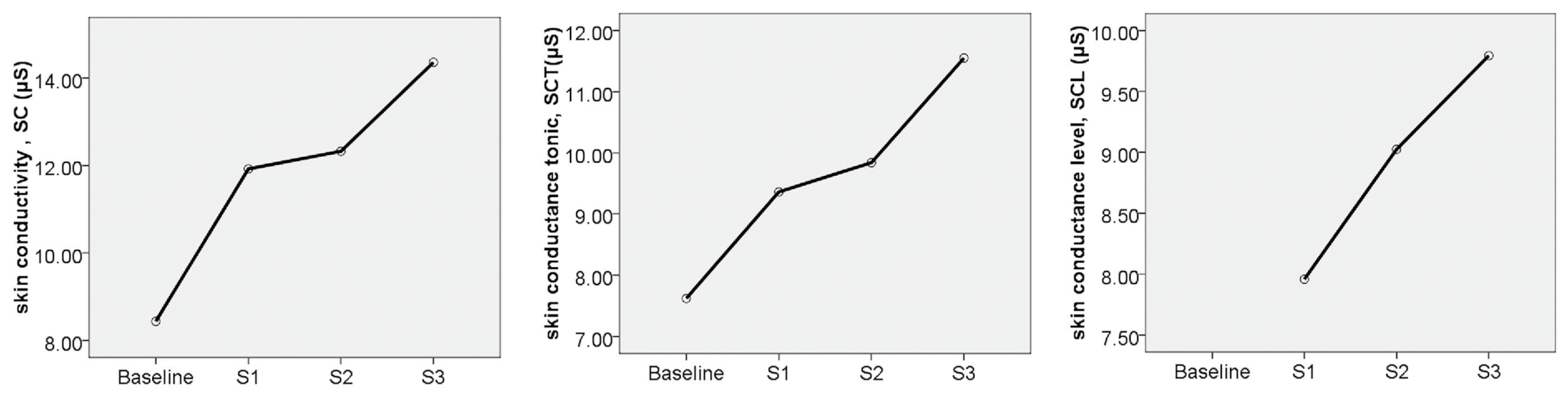
3.1.1. Electrodermal Activity, EDA
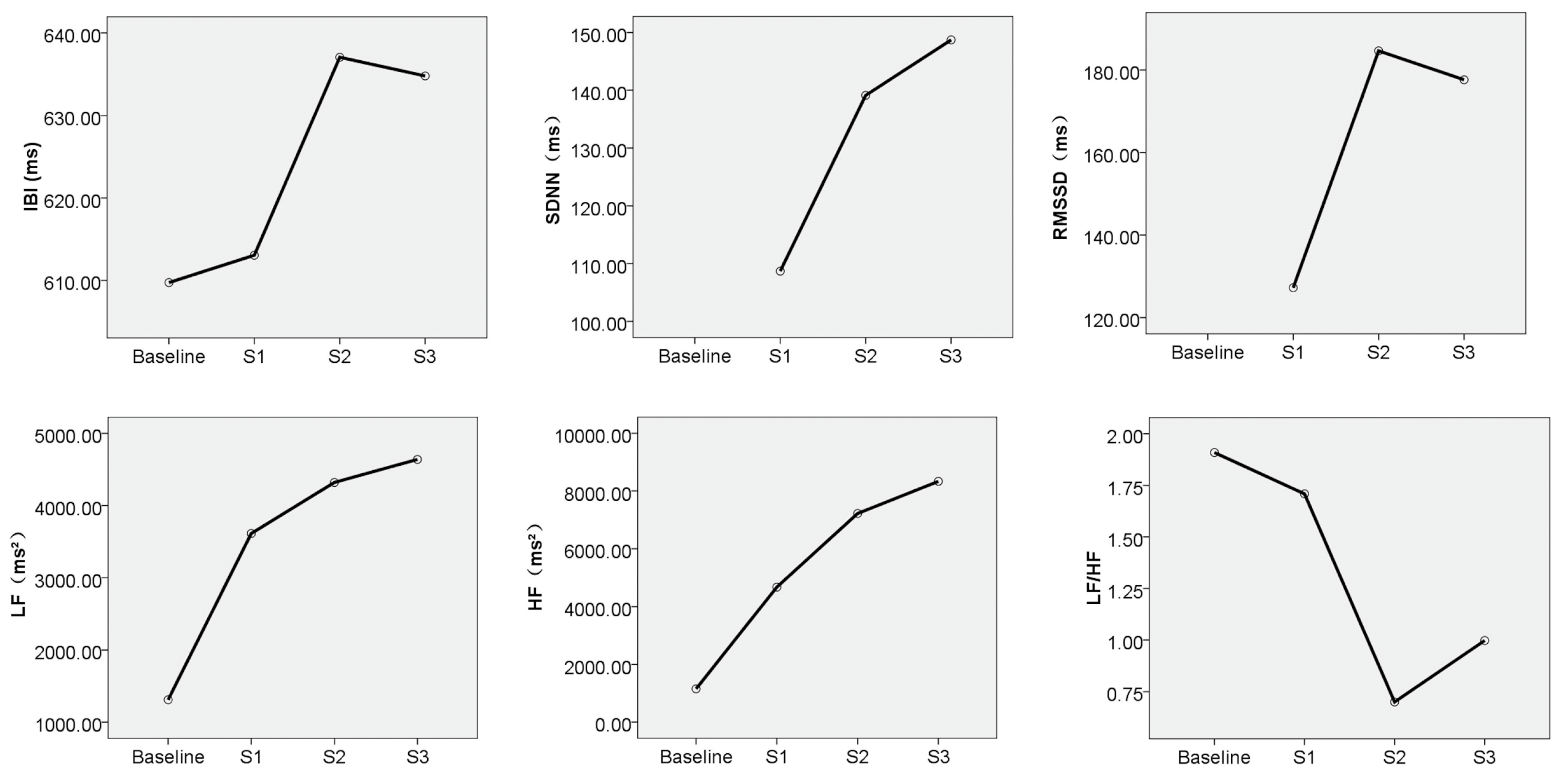
3.1.2. Heart Rate Variability, HRV
3.2. Effects of the Alarm Sound Types on Children’s Perceived Risk
3.3. Effects of Gender/Age on Children’s Risk Perception
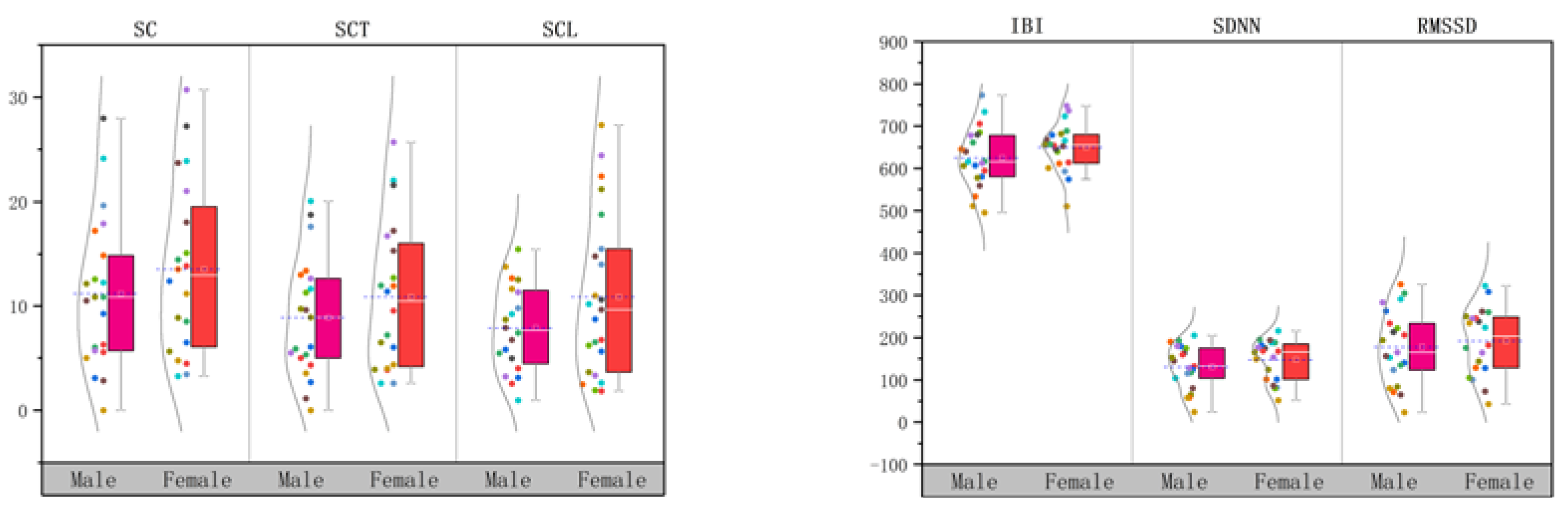
3.3.1. Gender
3.3.2. Age
4. Discussion and Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mytton, J.; Goodenough, T.; Novak, C. Children and young people’s behaviour in accidental dwelling fires: A systematic review of the qualitative literature. Saf. Sci. 2017, 96, 143–149. [Google Scholar] [CrossRef]
- Kholshevnikov, V.V.; Samoshin, D.A.; Parfenenko, A.P. Pre-school and school children building evacuation. In Proceedings of the Fourth International Symposium on Human Behaviour in Fire 2009, Cambridge, UK, 13–15 July 2019; pp. 243–254. [Google Scholar]
- Kholshchevnikov, V.V.; Samoshin, D.A.; Parfyonenko, A.P.; Belosokhov, I.P. Study of children evacuation from pre-school education institutions. Fire Mater. 2012, 36, 349–366. [Google Scholar] [CrossRef]
- Cuesta, A.; Gwynne, S.M.V. The collection and compilation of school evacuation data for model use. Saf. Sci. 2016, 84, 24–36. [Google Scholar] [CrossRef]
- Fang, Z.M.; Jiang, L.X.; Li, X.L.; Qi, W.; Chen, L.Z. Experimental study on the movement characteristics of 5–6 years old Chinese children when egressing from a pre-school building. Saf. Sci. 2019, 113, 264–275. [Google Scholar] [CrossRef]
- Chu, H.; Yu, J.; Wen, J.; Yi, M.; Chen, Y. Emergency Evacuation Simulation and Management Optimization in Urban Residential Communities. Sustainability 2019, 11, 795. [Google Scholar] [CrossRef]
- van der Wal, C.N.; Formolo, D.; Robinson, M.A.; Minkov, M.; Bosse, T. Simulating crowd evacuation with socio-cultural, cognitive, and emotional elements. In Transactions on Computational Collective Intelligence XXVII; Springer: Cham, Germany, 2017; pp. 139–177. [Google Scholar]
- Larusdottir, A.R.; Dederichs, A.S. A step towards including children’s evacuation parameters and behavior in fire safe building design. Fire Saf. Sci. 2011, 10, 187–195. [Google Scholar] [CrossRef]
- Larusdottir, A.R.; Dederichs, A.S. Evacuation dynamics of children–walking speeds, flows through doors in daycare centers. In Pedestrian and Evacuation Dynamics; Springer: Boston, MA, USA, 2011; pp. 139–147. [Google Scholar]
- Larusdottir, A.R.; Dederichs, A.S. Evacuation of children: Movement on stairs and on horizontal plane. Fire Technol. 2012, 48, 43–53. [Google Scholar] [CrossRef]
- Li, H.; Zhang, J.; Yang, L.; Song, W.; Yuen, K.K.R. A comparative study on the bottleneck flow between preschool children and adults under different movement motivations. Saf. Sci. 2020, 121, 30–41. [Google Scholar] [CrossRef]
- Hamilton, G.N.; Lennon, P.F.; O’Raw, J. Human behaviour during evacuation of primary schools: Investigations on pre-evacuation times, movement on stairways and movement on the horizontal plane. Fire Saf. J. 2017, 91, 937–946. [Google Scholar] [CrossRef]
- Najmanová, H.; Ronchi, E. An experimental data-set on pre-school children evacuation. Fire Technol. 2017, 53, 1509–1533. [Google Scholar] [CrossRef]
- Wu, Y.; Kang, J.; Wang, C. A crowd route choice evacuation model in large indoor building spaces. Front. Archit. Res. 2018, 7, 135–150. [Google Scholar] [CrossRef]
- Purser, D.A.; Bensilum, M. Quantification of behaviour for engineering design standards and escape time calculations. Saf. Sci. 2001, 38, 157–182. [Google Scholar] [CrossRef]
- Purser, D. Comparisons of evacuation efficiency and pre-travel activity times in response to a sounder and two different voice alarm messages. In Pedestrian and Evacuation Dynamics 2010; Springer: Berlin/Heidelberg, Germany, 2008; pp. 121–134. [Google Scholar]
- Fire, D.B.S.B.D. Safety Engineering in Buildings. In Part 1: Guide to the Application of Fire Safety Engineering Principles; British Standards Institution: London, UK, 1997. [Google Scholar]
- Bellamy, L.L.; Geyer, T.A.W. Experimental Programme to Investigate Informative Fire Warning Characteristics for Motivating Fast Evacuation; Building Research Establishment: London, UK, 1990. [Google Scholar]
- Cable, E.A. Cry wolf syndrome: Radical changes solve the false alarm problem. In Proceedings of the Fouth National Symposium Trade Exhibition on Health Care Safety and the Enviornment, London, UK, 1994. [Google Scholar]
- Proulx, G.; Sime, J.D. To prevent’ panic’ in an underground emergency: Why not tell people the truth? Fire Saf. Sci. 1991, 3, 843–852. [Google Scholar] [CrossRef]
- Bryan, J.L. A Study of the Survivors Reports on the Panic in the Fire at the Arundel Park Hall in Brooklyn, Maryland on 29 January 1956; University of Maryland: College Park, MD, USA, 1957. [Google Scholar]
- Baek, C.H.; Park, S.M.; Choi, B.J. Analysis of the Relationship between Human Risk Factors and Evacuation Behavior for Tunnel Safety. J. Korea Acad. Ind. Coop. Soc. 2019, 20, 535–546. [Google Scholar]
- Tong, D.; Canter, D. The decision to evacuate: A study of the motivations which contribute to evacuation in the event of fire. Fire Saf. J. 1985, 9, 257–265. [Google Scholar] [CrossRef]
- Urbina, E.; Wolshon, B. National review of hurricane evacuation plans and policies: A comparison and contrast of state practices. Transp. Res. Part A Policy Pract. 2003, 37, 257–275. [Google Scholar] [CrossRef]
- Montz, B.E.; Tobin, G.A.; Hagelman, R.R. Natural Hazards: Explanation and Integration; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Kinateder, M.; Ronchi, E.; Nilsson, D.; Kobes, M.; Müller, M.; Pauli, P.; Mühlberger, A. Virtual reality for fire evacuation research. In Proceedings of the 2014 Federated Conference on Computer Science and Information Systems, Warsaw, Poland, 7–10 September 2014; pp. 313–321. [Google Scholar]
- Zou, H.; Li, N.; Cao, L. Emotional response–based approach for assessing the sense of presence of subjects in virtual building evacuation studies. J. Comput. Civ. Eng. 2017, 31, 04017028. [Google Scholar] [CrossRef]
- Medvedev, O.; Shepherd, D.; Hautus, M.J. The restorative potential of soundscapes: A physiological investigation. Appl. Acoust. 2015, 96, 20–26. [Google Scholar] [CrossRef]
- Chuen, L.; Sears, D.; McAdams, S. Psychophysiological responses to auditory change. Psychophysiology 2016, 53, 891–904. [Google Scholar] [CrossRef]
- Kang, J.; Aletta, F.; Gjestland, T.T.; Brown, L.A.; Botteldooren, D.; Schulte-Fortkamp, B.; Coelho, J.L.B. Ten questions on the soundscapes of the built environment. Build. Environ. 2016, 108, 284–294. [Google Scholar] [CrossRef]
- Li, Z.; Kang, J. Sensitivity analysis of changes in human physiological indicators observed in soundscapes. Landsc. Urban Plan. 2019, 190, 103593. [Google Scholar] [CrossRef]
- Wilson, G.M.; Sasse, M.A. Do Users Always Know What’s Good for Them? Utilising Physiological Responses to Assess Media Quality. People and Computers XIV—Usability or Else; Springer: London, UK, 2000. [Google Scholar]
- Ravaja, N.; Kallinen, K.; Saari, T.; Keltikangas-Jarvinen, L. Suboptimal exposure to facial expressions when viewing video messages from a small screen: Effects on emotion, attention, and memory. J. Exp. Psychol. Appl. 2004, 10, 120. [Google Scholar] [CrossRef] [PubMed]
- Doorley, R.; Pakrashi, V.; Byrne, E.; Comerford, S.; Ghosh, B.; Groeger, J.A. Analysis of heart rate variability amongst cyclists under perceived variations of risk exposure. Transp. Res. Part F Traffic Psychol. Behav. 2015, 28, 40–54. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Luecken, L.J. Heart rate variability as an index of regulated emotional responding. Rev. Gen. Psychol. 2006, 10, 229–240. [Google Scholar] [CrossRef]
- Dishman, R.K.; Nakamura, Y.; Garcia, M.E.; Thompson, R.W.; Blair, S.N. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int. J. Psychophysiol. 2000, 37, 121–133. [Google Scholar] [CrossRef]
- Choi, B.; Jebelli, H.; Lee, S. Feasibility analysis of electrodermal activity EDA acquired from wearable sensors to assess construction workers’ perceived risk. Saf. Sci. 2019, 115, 110–120. [Google Scholar] [CrossRef]
- Suied, C.; Susini, P.; Mcadams, S. Evaluating warning sound urgency with reaction times. J. Exp. Psychol. Appl. 2008, 14, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Houtkamp, J.M.; Toet, A.; Bos, F.A. Task-relevant sound and user experience in computer-mediated firefighter training. Simul. Gaming 2012, 43, 778–802. [Google Scholar] [CrossRef]
- Allanson, J.; Fairclough, S.H. A research agenda for physiological computing. Interact. Comput. 2004, 16, 857–878. [Google Scholar] [CrossRef]
- Kennedy, D.K.; Hughes, B.M. The optimism-neuroticism question: An evaluation based on cardiovascular reactivity in female college students. Psychol. Rec. 2004, 54, 373–386. [Google Scholar] [CrossRef]
- Erfanian, M.; Mitchell, A.J.; Kang, J.; Aletta, F. The Psychophysiological Implications of Soundscape: A Systematic Review of Empirical Literature and a Research Agenda. Int. J. Environ. Res. Public Health 2019, 16, 3533. [Google Scholar] [CrossRef] [PubMed]
- Meehan, M.; Razzaque, S.; Insko, B.; Whitton, M.; Brooks, F.P. Review of four studies on the use of physiological reaction as a measure of presence in stressful virtual environments. Appl. Psychophysiol. Biofeedback 2005, 30, 239–258. [Google Scholar] [CrossRef] [PubMed]
- Picard, R.W.; Fedor, S.; Ayzenberg, Y. Multiple arousal theory and daily-life electrodermal activity asymmetry. Emot. Rev. 2016, 8, 62–75. [Google Scholar] [CrossRef]
- Fowles, D.C.; Kochanska, G.; Murray, K. Electrodermal activity and temperament in preschool children. Psychophysiology 2000, 37, 777–787. [Google Scholar] [CrossRef]
- The Effects of A Pressure Vest on Task Engagement, Challenging Behavior, and a Physiological Measure of Stress for a Child with Intellectual Disability. Available online: http://hdl.handle.net/2142/79051 (accessed on 13 December 2019).
- Lindquist, M.; Lange, E.; Kang, J. From 3D landscape visualization to environmental simulation: The contribution of sound to the perception of virtual environments. Landsc. Urban Plan. 2016, 148, 216–231. [Google Scholar] [CrossRef]
- Cadena, L.F.H.; Soares, A.C.L.; Pavón, I.; Coelho, L.B. Assessing soundscape: Comparison between in situ and laboratory methodologies. Noise Mapp. 2017, 4, 57–66. [Google Scholar] [CrossRef]
- Alvarsson, J.J.; Wiens, S.; Nilsson, M.E. Stress recovery during exposure to nature sound and environmental noise. Int. J. Environ. Res. Public Health 2010, 7, 1036–1046. [Google Scholar] [CrossRef]
- Kang, J.; Zhang, M. Semantic differential analysis of the soundscape in urban open public spaces. Build. Environ. 2010, 45, 150–157. [Google Scholar] [CrossRef]
- Ba, M.; Kang, J. Effect of a fragrant tree on the perception of traffic noise. Build. Environ. 2019, 156, 147–155. [Google Scholar] [CrossRef]
- Fuller, B.F. The effects of stress-anxiety and coping styles on heart rate variability. Int. J. Psychophysiol. 1992, 12, 81–86. [Google Scholar] [CrossRef]
- Fabes, R.A.; Eisenberg, N.; Eisenbud, L. Behavioral and physiological correlates of children’s reactions to others in distress. Dev. Psychol. 1993, 29, 655. [Google Scholar] [CrossRef]
- Gorman, J.M.; Sloan, R.P. Heart rate variability in depressive and anxiety disorders. Am. Heart J. 2000, 140, S77–S83. [Google Scholar] [CrossRef] [PubMed]
- Sgoifo, A.; Braglia, F.; Costoli, T.; Musso, E.; Meerlo, P.; Ceresini, G.; Troisi, A. Cardiac autonomic reactivity and salivary cortisol in men and women exposed to social stressors: Relationship with individual ethological profile. Neurosci. Biobehav. Rev. 2003, 271, 179–188. [Google Scholar] [CrossRef]
- Murakami, H.; Ohira, H. Influence of attention manipulation on emotion and autonomic responses. Percept. Mot. Skills 2007, 105, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Hume, K.; Ahtamad, M. Physiological responses to and subjective estimates of soundscape elements. Appl. Acoust. 2013, 74, 275–281. [Google Scholar] [CrossRef]
- Proulx, G. Evacuation time and movement in apartment buildings. Fire Saf. J. 1995, 24, 229–246. [Google Scholar] [CrossRef]
- Rundmo, T. Perceived risk, health and consumer behaviour. J. Risk Res. 1999, 2, 187–200. [Google Scholar] [CrossRef]
- Drottz, B.M. Perception of Risk: Studies of Risk Attitudes, Perceptions and Definitions; Center for Risk Research, Stockholm School of Economics: Stockholm, Sweden, 1991. [Google Scholar]
- Di Bona, G.; Silvestri, A.; Forcina, A.; Petrillo, A. Total efficient risk priority number TERPN: A new method for risk assessment. J. Risk Res. 2018, 21, 1384–1408. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Age (years) | Number | Male | Female |
|---|---|---|---|---|
| Junior | 3–4 | 14 | 7 | 7 |
| Middle | 4–5 | 14 | 8 | 6 |
| Senior | 5–6 | 14 | 8 | 6 |
| Type | S1 | S2 | S3 |
|---|---|---|---|
| LAeq (dB) | 88.13 dB | 87.32 dB | 88.11dB |
| Description | Voice alert (loop play of Chinese words: “Fire, run”) | Warning alarm (commonly used alarm in fire drills) | Combined voice alert and warning alarm (Chinese voice alert is inserted in warning alarm) |
| Alarm duration: | From the beginning of the experiment, until children are completely evacuated from the activity room | ||
| Duration between each of the alarm type (min) | 10 min | ||
| LAeq is the A-weighted equivalent continuous sound level in decibels measured over a stated period of time | |||
| Physiological Indicators | Baseline | S1 | S2 | S3 | |
|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | ||
| EDA | SC (μS) | 8.43 | 11.92 | 12.33 | 14.36 |
| SCT (μS) | 7.60 | 9.36 | 9.84 | 11.55 | |
| SCP (μS) | 0.82 | 2.56 | 2.49 | 2.81 | |
| LATENCY (s) | 1.97 | 1.97 | 1.96 | ||
| AMP (μS) | 1.94 | 1.75 | 1.93 | ||
| SCL (μS) | 7.96 | 9.46 | 9.79 | ||
| HRV | IBI (ms) | 607.89 | 613.07 | 637.05 | 634.78 |
| SDNN (ms) | 59.77 | 108.70 | 139.12 | 148.71 | |
| RMSSD (ms) | 63.74 | 127.25 | 184.63 | 177.63 | |
| SDSD (ms) | 63.93 | 129.92 | 189.37 | 181.94 | |
| ULF (ms²) | 45.10 | 50.55 | 51.03 | 69.94 | |
| VLF (ms²) | 596.22 | 727.55 | 856.21 | 1034.14 | |
| LF (ms²) | 1288.74 | 3612.94 | 4318.82 | 4637.84 | |
| HF (ms²) | 1132.01 | 4673.58 | 7220.49 | 8331.11 | |
| LF/HF | 1.89 | 1.71 | 0.70 | 1.00 | |
| Physiological Indicators | S1-Baseline | S2-Baseline | S3-Baseline | S1-S2-S3 | |
|---|---|---|---|---|---|
| Sig. | Sig. | Sig. | Sig. | ||
| EDA | SC (μS) | 0.000 | 0.000 | 0.000 | 0.000 |
| SCT (μS) | 0.003 | 0.001 | 0.000 | 0.000 | |
| SCP (μS) | 0.000 | 0.000 | 0.000 | 0.060 | |
| LATENCY (s) | 0.996 | ||||
| AMP (μS) | 0.752 | ||||
| SCL (μS) | 0.000 | ||||
| HRV | IBI (ms) | 0.652 | 0.021 | 0.021 | 0.000 |
| ULF (ms²) | 0.626 | 0.641 | 0.054 | 0.000 | |
| VLF (ms²) | 0.263 | 0.079 | 0.025 | 0.000 | |
| LF (ms²) | 0.000 | 0.000 | 0.000 | 0.000 | |
| HF (ms²) | 0.000 | 0.000 | 0.000 | 0.000 | |
| LF/HF | 0.703 | 0.000 | 0.005 | 0.000 | |
| Physiological Indicators | Baseline (Mean) | S2 (Mean) | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | △Male | Relative Change M (%) | Female | △Female | Relative Change F (%) | |
| SC | 8.16 | 8.71 | 11.18 | 3.02 | 37.00 | 13.53 | 4.82 | 55.33 |
| SCT | 7.29 | 7.93 | 8.87 | 1.58 | 21.67 | 10.86 | 2.93 | 36.94 |
| SCP | 0.87 | 0.77 | 2.31 | 1.44 | 165.51 | 2.67 | 1.9 | 246.75 |
| SCL | 7.78 | 10.85 | ||||||
| IBI | 603.2 | 612.82 | 624.6 | 21.4 | 3.54 | 650.11 | 37.29 | 6.08 |
| SDNN | 61.12 | 58.36 | 131.14 | 70.02 | 114.56 | 147.49 | 89.13 | 152.72 |
| RMSSD | 68.79 | 58.44 | 177.81 | 109.02 | 158.48 | 191.79 | 133.35 | 228.18 |
| LF | 1419.52 | 1151.43 | 3611 | 2191.48 | 154.38 | 5062.04 | 3910.61 | 339.63 |
| HF | 1351.72 | 901.31 | 6313.2 | 4961.48 | 367.04 | 8173.14 | 7271.83 | 806.80 |
| LF/HF | 1.74 | 2.05 | 0.76 | −0.98 | −56.32 | 0.64 | −1.41 | −68.78 |
| Physiological Indicators | t | Sig. |
|---|---|---|
| SC | −8.546 | 0.000 |
| SCT | −7.918 | 0.000 |
| SCP | −1.299 | 0.201 |
| Physiological Indicators | Baseline | S2 | Relative Change | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Junior | Middle | Senior | Junior | △Junior | Middle | △Middle | Senior | △Senior | Junior (%) | Middle (%) | Senior (%) | |
| SC | 9.43 | 7.23 | 8.54 | 12.65 | 3.22 | 10.51 | 3.29 | 13.69 | 5.15 | 34.12 | 45.47 | 60.37 |
| SCT | 8.17 | 6.64 | 7.93 | 9.52 | 1.35 | 8.66 | 2.02 | 11.25 | 3.32 | 16.51 | 30.39 | 41.87 |
| SCP | 1.26 | 0.58 | 0.61 | 3.13 | 1.87 | 1.85 | 1.27 | 2.44 | 1.83 | 48.20 | 217.40 | 302.15 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, J.; Jia, X.; Xu, G.; Jia, J.; Hai, R.; Gao, C.; Zhang, S. The Relationship between Different Types of Alarm Sounds and Children’s Perceived Risk Based on Their Physiological Responses. Int. J. Environ. Res. Public Health 2019, 16, 5091. https://doi.org/10.3390/ijerph16245091
Zhou J, Jia X, Xu G, Jia J, Hai R, Gao C, Zhang S. The Relationship between Different Types of Alarm Sounds and Children’s Perceived Risk Based on Their Physiological Responses. International Journal of Environmental Research and Public Health. 2019; 16(24):5091. https://doi.org/10.3390/ijerph16245091
Chicago/Turabian StyleZhou, Jiaxu, Xiaohu Jia, Guoqiang Xu, Junhan Jia, Rihan Hai, Chongsen Gao, and Shuo Zhang. 2019. "The Relationship between Different Types of Alarm Sounds and Children’s Perceived Risk Based on Their Physiological Responses" International Journal of Environmental Research and Public Health 16, no. 24: 5091. https://doi.org/10.3390/ijerph16245091
APA StyleZhou, J., Jia, X., Xu, G., Jia, J., Hai, R., Gao, C., & Zhang, S. (2019). The Relationship between Different Types of Alarm Sounds and Children’s Perceived Risk Based on Their Physiological Responses. International Journal of Environmental Research and Public Health, 16(24), 5091. https://doi.org/10.3390/ijerph16245091