Emotional and Behavioral Problems Among 3- to 5-Year-Olds Left-Behind Children in Poor Rural Areas of Hunan Province: A Cross-Sectional Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Recruitment
2.3. Ethical Approval
2.4. Data Collection
2.5. Measures
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of LBC
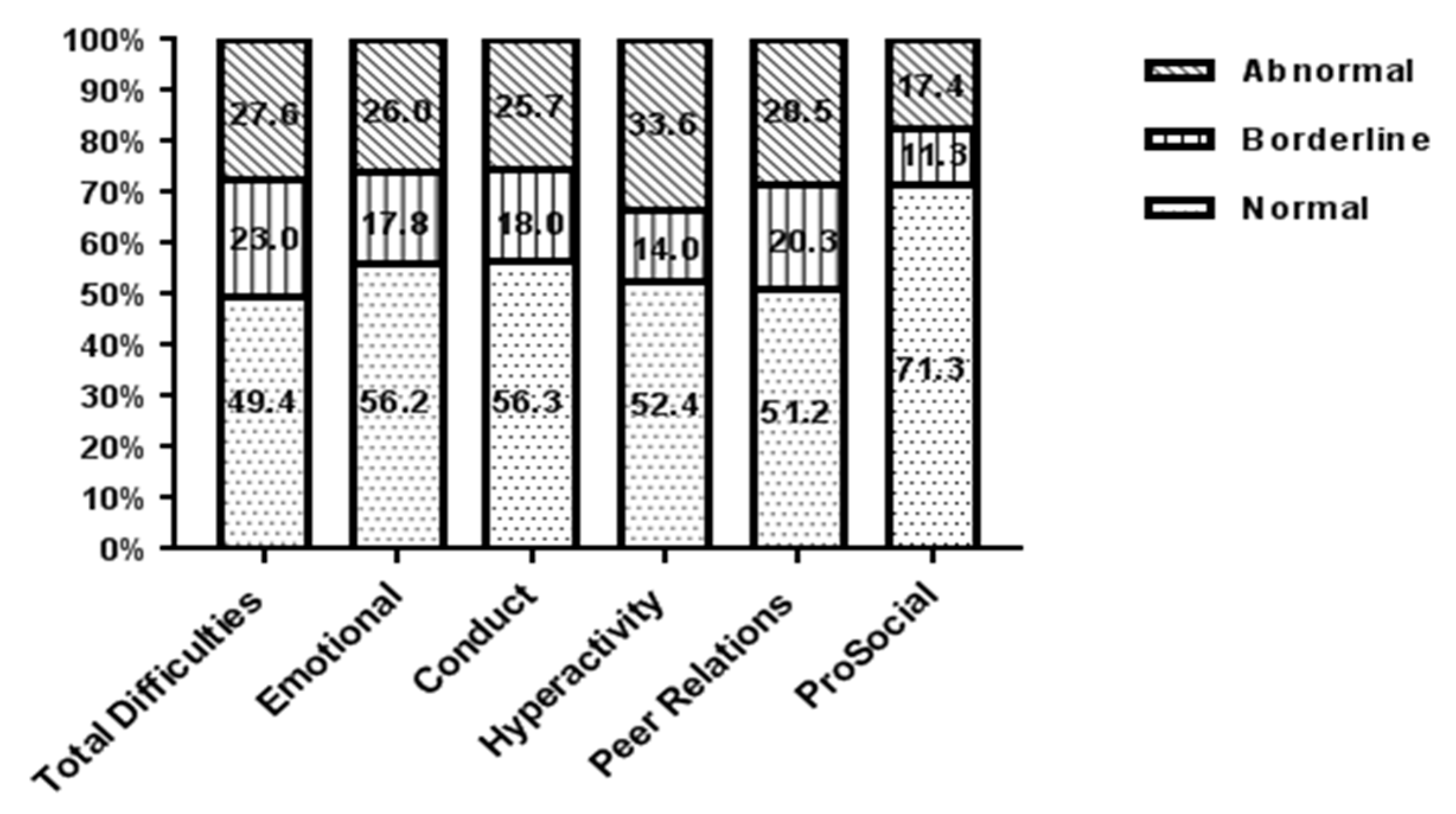
3.2. SDQ Banded Scores for LBC
3.3. Scores of SDQ Scales for LBC of Different Genders and Ages
3.4. Multivariate Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| LBC | Left-behind children |
| CLBC | Caregivers of left-behind children |
| SDQ | Strength and Difficulties Questionnaire |
| NGO | Non-governmental organizations |
| CBCL | Child Behavior Checklist |
References
- Duan, C.R.; Lai, M.H.; Qin, M. Research on the Changing Trend of Left-behind Children in Rural Areas in China since the 21st Century. China Youth Study 2017, 6, 52–60. (In Chinese) [Google Scholar]
- Ouyang, Y.; Zou, J.; Ji, M.; Zhang, Y.; Yuan, T.; Yang, L.; Lin, Q. Study on the Status of Health Service Utilization among 3(-)5 Years Old Left-Behind Children in Poor Rural Areas of Hunan Province, China: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2019, 16, 125. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Zhang, Y.; Zou, J.; Yuan, T.; Tang, A.; Deng, J.; Yang, L.; Li, M.; Chen, J.; Qin, H.; et al. Study on the Status of Health Service Utilization among Caregivers of Left-Behind Children in Poor Rural Areas of Hunan Province: A Baseline Survey. Int. J. Environ. Res. Public Health 2017, 14, 910. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.A. Family structure and children’s health: United States, 1988. In Vital and Health Statistics; U.S. Department of Health and Human Services: Hyattsville, MD, USA, 1991; Volume 178, pp. 1–47. [Google Scholar]
- Bramlett, M.D.; Blumberg, S.J. Family structure and children’s physical and mental health. Health Aff. 2007, 26, 549–558. [Google Scholar] [CrossRef]
- Newman, R.S. Social influences on the development of children’s adaptive help seeking: The role of parents, teachers, and peers. Dev. Rev. 2000, 20, 350–404. [Google Scholar] [CrossRef]
- Harris, T.; Brown, G.W.; Bifulco, A. Loss of parent in childhood and adult psychiatric disorder: The role of lack of adequate parental care. Psychol. Med. 1986, 16, 641–659. [Google Scholar] [CrossRef]
- Hetherington, E.M.; Bridges, M.; Insabella, G.M. What matters? What does not? Five perspectives on the association between marital transitions and children’s adjustment. Am. Psychol. 1998, 53, 167–184. [Google Scholar] [CrossRef]
- Elam, K.K.; Sandler, I.; Wolchik, S.; Tein, J.Y. Non-Residential Father-Child Involvement, Interparental Conflict and Mental Health of Children Following Divorce: A Person-Focused Approach. J. Youth Adolesc. 2016, 45, 581–593. [Google Scholar] [CrossRef]
- Nilsen, S.; Boe, T. Divorce and family structure in Norway—Associations to adolescent mental health. Eur. J. Public Health 2016, 26. [Google Scholar] [CrossRef]
- Astrup, A.; Pedersen, C.B.; Mok, P.L.H.; Carr, M.J.; Webb, R.T. Self-harm risk between adolescence and midlife in people who experienced separation from one or both parents during childhood. J. Affect. Disord. 2017, 208, 582–589. [Google Scholar] [CrossRef]
- Fan, F.; Su, L.; Gill, M.K.; Birmaher, B. Emotional and behavioral problems of Chinese left-behind children: A preliminary study. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Lin, L.; Xu, M.; Li, L.; Lu, J.; Zhou, X. Mental Health among Left-Behind Children in Rural China in Relation to Parent-Child Communication. Int. J. Environ. Res. Public Health 2019, 16, 1855. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Sun, X.; Huang, L.; Zhang, G.; Kenny, K.; Xue, H.; Auden, E.; Rozelle, S. Parental Migration and Left-Behind Children’s Depressive Symptoms: Estimation Based on a Nationally-Representative Panel Dataset. Int. J. Environ. Res. Public Health 2018, 15, 1069. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Gao, J.; Jiang, H.; Jiang, H.; Guo, S.; Chen, K.; Jin, K.; Qi, Y. A Comparative Study of Behavior Problems among Left-Behind Children, Migrant Children and Local Children. Int. J. Environ. Res. Public Health 2018, 15, 655. [Google Scholar] [CrossRef]
- Liu, Z.K.; Li, X.Y.; Ge, X.J. Left Too Early: The Effects of Age at Separation from Parents on Chinese Rural Children’s Symptoms of Anxiety and Depression. Am. J. Public Health 2009, 99, 2049–2054. [Google Scholar] [CrossRef]
- Adhikari, R.; Jampaklay, A.; Chamratrithirong, A.; Richter, K.; Pattaravanich, U.; Vapattanawong, P. The impact of parental migration on the mental health of children left behind. J. Immigr. Minor. Health 2014, 16, 781–789. [Google Scholar] [CrossRef]
- Balseviciene, B.; Sinkariova, L.; Grazuleviciene, R.; Andrusaityte, S.; Uzdanaviciute, I.; Dedele, A.; Nieuwenhuijsen, M.J. Impact of residential greenness on preschool children’s emotional and behavioral problems. Int. J. Environ. Res. Public Health 2014, 11, 6757–6770. [Google Scholar] [CrossRef]
- Hagan, J.F.; Foy, J.M.; Goldson, E.J.; Howard, B.J.; Navarro, A.; Sullivan, T.J.; Tanner, J.L.; Fa, C.P.A.C. The new morbidity revisited: A renewed commitment to the psychosocial aspects of pediatric care. Pediatrics 2001, 108, 1227–1230. [Google Scholar]
- Weitzman, C.; Wegner, L.; Pediat, S.D.B.; Fa, C.P.A.C.; Childhood, C.E.; Pediat, S.D.B. Promoting Optimal Development: Screening for Behavioral and Emotional Problems. Pediatrics 2015, 135, 384–395. [Google Scholar] [CrossRef]
- Slomski, A. Chronic Mental Health Issues in Children Now Loom Larger Than Physical Problems. JAMA 2012, 308, 223–225. [Google Scholar] [CrossRef]
- Teekavanich, S.; Chantaratin, S.; Sirisakpanit, S.; Tarugsa, J. Prevalence and Factors Related to Behavioral and Emotional Problems among Preschool Children in Bangkok, Thailand. J. Med. Assoc. Thail. 2017, 100, 175–182. [Google Scholar]
- Lahey, B.B.; Pelham, W.E.; Loney, J.; Kipp, H.; Ehrhardt, A.; Lee, S.S.; Willcutt, E.G.; Hartung, C.M.; Chronis, A.; Massetti, G. Three-year predictive validity of DSM-IV attention deficit hyperactivity disorder in children diagnosed at 4–6 years of age. Am. J. Psychiatry 2004, 161, 2014–2020. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, B.M.; Proczkowska-Bjorklund, M.; Gustafsson, P.A. Emotional and behavioural problems in Swedish preschool children rated by preschool teachers with the Strengths and Difficulties Questionnaire (SDQ). BMC Pediatr. 2017, 17, 110. [Google Scholar] [CrossRef] [PubMed]
- Garner, A.S.; Shonkoff, J.P.; Siegel, B.S.; Dobbins, M.I.; Earls, M.F.; Garner, A.S.; McGuinn, L.; Pascoe, J.; Wood, D.L.; Fa, C.P.A.C.; et al. Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science into Lifelong Health. Pediatrics 2012, 129, E224–E231. [Google Scholar] [PubMed]
- Zhang, L.S.; He, K.; Zhao, Y.X.; Zhang, D.D. A review of Screening and Assessment Tools for Children with Emotional and Behavioral Disorders. Chin. J. Spec. Educ. 2015, 2, 65–71. (In Chinese) [Google Scholar]
- Stone, L.L.; Otten, R.; Engels, R.C.; Vermulst, A.A.; Janssens, J.M. Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4- to 12-year-olds: A review. Clin. Child Fam. Psychol. Rev. 2010, 13, 254–274. [Google Scholar] [CrossRef]
- Kou, J.H.; Du, Y.S.; Xia, N.M. Reliability and validity of “children strengths and difficulties questionnaire” in Shanghai norm. Gen. Psychiatry 2005, 1, 25–28. (In Chinese) [Google Scholar]
- Achenbach, T.M.; Becker, A.; Dopfner, M.; Heiervang, E.; Roessner, V.; Steinhausen, H.C.; Rothenberger, A. Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: Research findings, applications, and future directions. J. Child Psychol. Psychiatry 2008, 49, 251–275. [Google Scholar] [CrossRef]
- Tian, X.; Ding, C.; Shen, C.; Wang, H. Does Parental Migration Have Negative Impact on the Growth of Left-Behind Children? New Evidence from Longitudinal Data in Rural China. Int. J. Environ. Res. Public Health 2017, 14, 1308. [Google Scholar] [CrossRef]
- Ma, S.; Jiang, M.; Wang, F.; Lu, J.; Li, L.; Hesketh, T. Left-Behind Children and Risk of Unintentional Injury in Rural China-A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2019, 16, 403. [Google Scholar] [CrossRef]
- Guan, H.; Wang, H.; Huang, J.; Du, K.; Zhao, J.; Boswell, M.; Shi, Y.; Iyer, M.; Rozelle, S. Health Seeking Behavior among Rural Left-Behind Children: Evidence from Shaanxi and Gansu Provinces in China. Int. J. Environ. Res. Public Health 2018, 15, 883. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Adab, P.; Hemming, K.; Yang, L.; Qin, H.; Li, M.; Deng, J.; Shi, J.; Chen, J. Health allowance for improving the nutritional status and development of 3-5-year-old left-behind children in poor rural areas of China: Study protocol for a cluster randomised trial. Trials 2015, 16, 361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ji, M.; Zou, J.; Yuan, T.; Deng, J.; Yang, L.; Li, M.; Qin, H.; Chen, J.; Lin, Q. Effect of a Conditional Cash Transfer Program on Nutritional Knowledge and Food Practices among Caregivers of 3-5-Year-Old Left-Behind Children in the Rural Hunan Province. Int. J. Environ. Res. Public Health 2018, 15, 525. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Vostanis, P. Strengths and Difficulties Questionnaire: Research and clinical applications. Curr. Opin. Psychiatry 2006, 19, 367–372. [Google Scholar] [CrossRef]
- Wang, X.L.; Li, P.F.; Peng, Y.; Liu, K. Emotional and behavioral problems of children-adolescents aged 4–18 in Changsha. Chin. Ment. Health J. 2012, 26, 775–779. (In Chinese) [Google Scholar]
- Chen, Y.X.; Erigene, X.Y.; Wu, K.; Huang, W.P.; Yu, S.H.; Chen, H.Y.; Ye, A.H.; Zhang, F.B.; Tao, F. Emotional and behavioral problems associated with sleep problems in preschool aged children. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 1191–1196. [Google Scholar]
- Elberling, H.; Linneberg, A.; Olsen, E.M.; Goodman, R.; Skovgaard, A.M. The prevalence of SDQ-measured mental health problems at age 5–7 years and identification of predictors from birth to preschool age in a Danish birth cohort: The Copenhagen Child Cohort 2000. Eur. Child Adolesc. Psychiatry 2010, 19, 725–735. [Google Scholar] [CrossRef]
- Marryat, L.; Thompson, L.; Minnis, H.; Wilson, P. Associations between social isolation, pro-social behaviour and emotional development in preschool aged children: A population based survey of kindergarten staff. BMC Psychol. 2014, 2, 44. [Google Scholar] [CrossRef]
- Fuchs, S.; Klein, A.M.; Otto, Y.; von Klitzing, K. Prevalence of emotional and behavioral symptoms and their impact on daily life activities in a community sample of 3 to 5-year-old children. Child Psychiatry Hum. Dev. 2013, 44, 493–503. [Google Scholar] [CrossRef]
- All-China Women’s Federation. Research Report on rural left-behind children and rural-urban migrant children in China. China Women’s Mov. 2013, 6, 30–34. (In Chinese) [Google Scholar]
- Li, S.J.; Chen, H.Y.; Fu, W.F. Investigation and consideration of labor force transfer in Pingjiang county. News Universe 2007, 1, 20–23. (In Chinese) [Google Scholar]
- Lu, J. The Research on the Land-lost Farmers’ Sustainable Livelihood in Tourism Developed Areas—A Case Study on Fenghuang county of Hunan Province. Master’s Thesis, South-Central University for Nationalities, Wuhan, China, 2013. (In Chinese). [Google Scholar]
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.C.; Palmieri, P.A. Risk of psychological difficulties among children raised by custodial grandparents. Psychiatr. Serv. 2007, 58, 1303–1310. [Google Scholar] [CrossRef]
- Sourander, A. Emotional and behavioural problems in a sample of Finnish three-year-olds. Eur. Child Adolesc. Psychiatry 2001, 10, 98–104. [Google Scholar] [CrossRef]
- Huang, G.W.; Wu, H.; Du, Q.Y.; Liu, Z.Y.; Huang, Q. Analysis of behavior problems in left-behind children aged 3 to 7 years in countryside of Hunan province. Chin. J. Child Health Care 2010, 18, 26–29. (In Chinese) [Google Scholar]
- Wichstrom, L.; Berg-Nielsen, T.S.; Angold, A.; Egger, H.L.; Solheim, E.; Sveen, T.H. Prevalence of psychiatric disorders in preschoolers. J. Child Psychol. Psychiatry 2012, 53, 695–705. [Google Scholar] [CrossRef]
- Taverna, L.; Bornstein, M.H.; Putnick, D.L.; Axia, G. Adaptive Behaviors in Young Children: A Unique Cultural Comparison in Italy. J. Cross Cult. Psychol. 2011, 42, 445–465. [Google Scholar] [CrossRef]
- Sun, K.X. Attaching importance to boys and despising girls has parents’invisible shadow behind them. Ment. Health Educ. Prim. Second. Sch. 2018, 12, 77–78. (In Chinese) [Google Scholar]
- Jiang, H. Study on the Dilemma of the Survival and Development of Left-behind Girls in Rural Areas. J. Ningde Norm. Univ. 2018, 1, 40–43. (In Chinese) [Google Scholar]
- Zhao, Q. Survival Dilemma of Left-behind Girls from the Perspective of Social Support Theory. Master’s Thesis, Capital University of Economics and Business, Beijing, China, 2016. (In Chinese). [Google Scholar]
- Huang, G.W.; Du, Q.Y.; Liu, Z.Y.; Liu, Y.P.; Huang, Q.; Wu, H.; Luo, J.Y.; Zhang, L.L. Analysis on influences of guardians on behavior of left-behind children aged 3 to 7 years in countryside. Zhonghua Er Ke Za Zhi 2010, 48, 390–394. (In Chinese) [Google Scholar] [PubMed]
- Keng, S.-L.; Lee, Y.; Drabu, S.; Hong, R.Y.; Chee, C.Y.; Ho, C.S.; Ho, R.C. Construct validity of the mclean screening instrument for borderline personality disorder in two singaporean samples. J. Personal. Disord. 2019, 33, 450–469. [Google Scholar] [CrossRef] [PubMed]
- Choo, C.; Diederich, J.; Song, I.; Ho, R. Cluster analysis reveals risk factors for repeated suicide attempts in a multi-ethnic Asian population. Asian J. Psychiatr. 2014, 8, 38–42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total Sample n (%) |
|---|---|
| LBC’s age (years) | |
| 3 | 175 (31.4) |
| 4 | 178 (32.0) |
| 5 | 204 (36.6) |
| LBC’s gender | |
| Boy | 296 (53.1) |
| Girl | 261 (46.9) |
| LBC’s ethnicity | |
| Han | 347 (62.3) |
| Minorities | 210 (37.7) |
| Left-behind status | |
| Father out | 111 (19.9) |
| Mother out | 27 (4.8) |
| Both parents out | 419 (75.3) |
| Number of LBC in the family (n, %) | |
| 1 | 150 (26.8) |
| 2 | 253 (45.6) |
| 3 and above | 154 (27.6) |
| CLBC’s age (years) | |
| 20–39 | 61 (11.0) |
| 40–59 | 261 (46.8) |
| 60+ | 235 (42.2) |
| CLBC’s gender | |
| Male | 223 (40.0) |
| Female | 334 (60.0) |
| CLBC’s education level | |
| No formal education | 172 (30.9) |
| Primary school | 271 (48.6) |
| Middle school | 93 (16.7) |
| High school | 21 (3.8) |
| CLBC’s relationship to LBC | |
| Father | 23 (4.1) |
| Mother | 51 (9.2) |
| Grandparent | 472 (84.7) |
| Other | 11 (2.0) |
| Sick person at home | |
| None | 452 (81.1) |
| 1 sick person | 95 (17.1) |
| 2 sick people | 10 (1.8) |
| CLBC’s willingness to take care of LBC | |
| Willing | 539 (96.8) |
| Unwilling | 18 (3.2) |
| CLBC felt burden to take care of LBC | |
| Having a burden | 439 (78.8) |
| No burden | 118 (21.2) |
| SDQ Domains | Age | Gender | |||
|---|---|---|---|---|---|
| 3y (n = 175) | 4y (n = 178) | 5y (n = 204) | Boy (n = 296) | Girl (n = 261) | |
| Emotional symptoms * | |||||
| Normal | 89 (50.9%) | 101 (56.7%) | 123 (60.3%) | 175 (59.1%) | 138 (52.9%) |
| Borderline | 34 (19.4%) | 33 (18.5%) | 32 (15.7%) | 57 (19.3%) | 42 (16.1%) |
| Abnormal | 52 (29.7%) | 44 (24.8%) | 49 (24.0%) | 64 (21.6%) | 81 (31.0%) |
| Conduct problems a | |||||
| Normal | 85 (48.6%) | 106 (59.6%) | 123 (60.3%) | 172 (58.1%) | 142 (54.4%) |
| Borderline | 31 (17.7%) | 32 (18.0%) | 37 (18.1%) | 45 (15.2%) | 55 (21.1%) |
| Abnormal | 59 (33.7%) | 40 (22.4%) | 44 (21.6%) | 79 (26.7%) | 64 (24.5%) |
| Hyperactivity **,a | |||||
| Normal | 79 (45.1%) | 98 (55.1%) | 115 (56.4%) | 136 (45.9%) | 156 (59.8%) |
| Borderline | 25 (14.3%) | 20 (11.2%) | 33 (16.2%) | 51 (17.3%) | 27 (10.3%) |
| Abnormal | 71 (40.6%) | 60 (33.7%) | 56 (27.4%) | 109 (36.8%) | 78 (29.9%) |
| Peer Problems | |||||
| Normal | 84 (48.0%) | 83 (46.6%) | 118 (57.8%) | 155 (52.4%) | 130 (49.8%) |
| Borderline | 34 (19.4%) | 43 (24.2%) | 36 (17.6%) | 62 (20.9%) | 51 (19.5%) |
| Abnormal | 57 (32.6%) | 52 (29.2%) | 50 (24.6%) | 79 (26.7%) | 80 (30.7%) |
| Prosocial behavior b | |||||
| Normal | 116 (66.3%) | 124 (69.6%) | 157 (77.0%) | 208 (70.3%) | 189 (72.4%) |
| Borderline | 23 (13.1%) | 17 (9.6%) | 23 (11.2%) | 36 (12.2%) | 27 (10.3%) |
| Abnormal | 36 (20.6%) | 37 (20.8%) | 24 (11.8%) | 52 (17.5%) | 45 (17.3%) |
| Variables | Adjusted OR (95% CI) | p-value |
|---|---|---|
| LBC’s age (years) | ||
| 4 y vs. 3 y | 0.623 (0.388–1.001) | 0.051 |
| 5 y vs. 3 y | 0.527 (0.330–0.842) | 0.007 |
| Sick person at home | ||
| 1 sick person vs. none | 1.401 (0.854–2.298) | 0.182 |
| 2 sick people vs. none | 12.56 (2.549–61.902) | 0.002 |
| CLBC’s willingness to take care of LBC | ||
| Unwilling vs. willing | 9.981 (3.172–31.411) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, J.; Zou, J.; Ji, M.; Yuan, T.; Sun, M.; Lin, Q. Emotional and Behavioral Problems Among 3- to 5-Year-Olds Left-Behind Children in Poor Rural Areas of Hunan Province: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 4188. https://doi.org/10.3390/ijerph16214188
Luo J, Zou J, Ji M, Yuan T, Sun M, Lin Q. Emotional and Behavioral Problems Among 3- to 5-Year-Olds Left-Behind Children in Poor Rural Areas of Hunan Province: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(21):4188. https://doi.org/10.3390/ijerph16214188
Chicago/Turabian StyleLuo, Jing, Jiaojiao Zou, Meimei Ji, Tong Yuan, Mei Sun, and Qian Lin. 2019. "Emotional and Behavioral Problems Among 3- to 5-Year-Olds Left-Behind Children in Poor Rural Areas of Hunan Province: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 21: 4188. https://doi.org/10.3390/ijerph16214188
APA StyleLuo, J., Zou, J., Ji, M., Yuan, T., Sun, M., & Lin, Q. (2019). Emotional and Behavioral Problems Among 3- to 5-Year-Olds Left-Behind Children in Poor Rural Areas of Hunan Province: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(21), 4188. https://doi.org/10.3390/ijerph16214188