How Does Household Residential Instability Influence Child Health Outcomes? A Quantile Analysis


Abstract
1. Introduction
- Is there a relationship between residential instability and children’s health?
- If so, does this effect vary by children’s initial health?
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


References
- Krieger, J.; Higgins, D.L. Housing and Health: Time Again for Public Health Action. Am. J. Public Health 2002, 92, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Engemann, K.; Pedersen, C.B.; Arge, L.; Tsirogiannis, C.; Mortensen, P.B.; Svenning, J.-C. Residential green space in childhood is associated with lower risk of psychiatric disorders from adolescence into adulthood. Proc. Natl. Acad. Sci. USA 2019, 116, 5188–5193. [Google Scholar] [CrossRef] [PubMed]
- Maggi, S.; Irwin, L.J.; Siddiqi, A.; Hertzman, C. The social determinants of early child development: An overview. J. Paediatr. Child Health 2010, 46, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G.; Marmot, M. (Eds.) Social Determinants of Health: The Solid Facts; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Kelly-Irving, K. Allostatic Load: How Stress in Childhood Affects Life-Course Health Outcomes, Health Foundation Working Paper. 2019. Available online: https://www.health.org.uk/sites/default/files/upload/publications/2019/Allostatic%20load%20how%20stress%20in%20childhood%20affects%20life%20course%20health%20outcomes.pdf (accessed on 29 October 2019).
- Cutts, D.B.; Meyers, A.F.; Black, M.M.; Casey, P.H.; Chilton, M.; Cook, J.T.; Geppert, J.; De Cuba, S.E.; Heeren, T.; Coleman, S.; et al. US Housing Insecurity and the Health of Very Young Children. Am. J. Public Health 2011, 101, 1508–1514. [Google Scholar] [CrossRef]
- Fowler, P.J.; Henry, D.B.; Schoeny, M.; Taylor, J.; Chavira, D. Developmental Timing of Housing Mobility: Longitudinal Effects on Externalizing Behaviors among At-Risk Youth. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 199–208. [Google Scholar] [CrossRef]
- Fowler, P.J.; Henry, D.B.; Marcal, K.E. Family and housing instability: Longitudinal impact on adolescent emotional and behavioral well-being. Soc. Sci. Res. 2015, 53, 364–374. [Google Scholar] [CrossRef]
- Desmond, M.; Kimbro, R.T. Eviction’s Fallout: Housing, Hardship, and Health. Soc. Forces 2015, 94, 295–324. [Google Scholar] [CrossRef]
- Jelleyman, T.; Spencer, N. Residential mobility in childhood and health outcomes: A systematic review. J. Epidemiol. Community Health 2008, 62, 584–592. [Google Scholar] [CrossRef]
- Adam, E.K. Beyond quality: Parental and residential stability and children’s adjustment. Curr. Dir. Psychol. Sci. 2004, 13, 210–213. [Google Scholar] [CrossRef]
- Coley, R.L.; Lynch, A.D.; Kull, M. Early Exposure to Environmental Chaos and Children’s Physical and Mental Health. Early Child. Res. Q. 2015, 32, 94–104. [Google Scholar] [CrossRef]
- Johnson, M.P.; Ladd, H.F.; Ludwig, J. The Benefits and Costs of Residential Mobility Programmes for the Poor. Hous. Stud. 2002, 17, 125–138. [Google Scholar] [CrossRef]
- Acevedo-Garcia, D.; Osypuk, T.L.; Werbel, R.E.; Meara, E.R.; Cutler, D.M.; Berkman, L.F. Does Housing Mobility Policy Improve Health? Hous. Policy Debate 2004, 15, 49–98. [Google Scholar] [CrossRef]
- Bambra, C.; Gibson, M.; Sowden, A.; Wright, K.; Whitehead, M.; Petticrew, M. Tackling the wider social determinants of health and health inequalities: Evidence from systematic reviews. J. Epidemiol. Community Health 2010, 64, 284. [Google Scholar] [CrossRef] [PubMed]
- Katz, L.F.; Kling, J.R.; Liebman, J.B. Moving to Opportunity in Boston: Early Results of a Randomized Mobility Experiment. Q. J. Econ. 2001, 116, 607–654. [Google Scholar] [CrossRef]
- Leventhal, T.; Brooks-Gunn, J. Moving to Opportunity: An Experimental Study of Neighborhood Effects on Mental Health. Am. J. Public Health 2003, 93, 1576–1582. [Google Scholar] [CrossRef]
- Chetty, R.; Hendren, N.; Katz, L.F. The Effects of Exposure to Better Neighborhoods on Children: New Evidence from the Moving to Opportunity Experiment. Am. Econ. Rev. 2016, 106, 855–902. [Google Scholar] [CrossRef]
- Wang, R.; Walter, R.; Arafat, A.; Song, J. Understanding the role of life events on residential mobility for low-income, subsidised households. Urban Stud. 2019, 56, 1628–1646. [Google Scholar] [CrossRef]
- Maher, C. Residential Mobility, Locational Disadvantage and Spatial Inequality in Australian Cities. Urban Policy Res. 1994, 12, 185–191. [Google Scholar] [CrossRef]
- Clark, W.A.V.; Onaka, J.L. Life Cycle and Housing Adjustment as Explanations for Residential Mobility. Urban Stud. 1983, 20, 47–57. [Google Scholar] [CrossRef]
- Kintrea, K.; Clapham, D. Housing Choice and Search Strategies within an Administered Housing System. Environ. Plan A Econ. Space 1986, 18, 1281–1296. [Google Scholar] [CrossRef]
- Baker, E. Improving Outcomes of Forced Residential Relocation: The Development of an Australian Tenants’ Spatial Decision Support System. Urban Stud. 2008, 45, 1712–1728. [Google Scholar] [CrossRef]
- Baker, E.; Bentley, R.; Lester, L.; Beer, A. Housing affordability and residential mobility as drivers of locational inequality. Appl. Geogr. 2016, 72, 65–75. [Google Scholar] [CrossRef]
- Ziol-Guest, K.M.; McKenna, C.C. Early childhood housing instability and school readiness. Child. Dev. 2014, 85, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Tucker, C.J.; Marx, J.; Long, L. Moving on: Residential mobility and children’s school lives. Sociol. Educ. 1998, 71, 111–129. [Google Scholar] [CrossRef]
- Baker, E.; Pham, N.T.A.; Daniel, L.; Bentley, R. New evidence on mental health and housing affordability in cities: A quantile regression approach. Cities 2020, 96, 102455. [Google Scholar] [CrossRef]
- Powell, D. Quantile Regression with Nonadditive Fixed Effects. Quantile Treatment Effects; Rand Corporation: Santa Monica, CA, USA, 2016. [Google Scholar]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL™ 4.0: Reliability and validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Gaylord, A.L.; Cowell, W.J. Impact of housing instability on child behavior at age 7 years. Int. Public Health J. 2018, 10, 287–295. [Google Scholar]
- Sandstrom, H.; Huerta, S. The Negative Effects of Instability on Child Development: A Research Synthesis; Urban Institute: Washington, DC, USA, 2013. [Google Scholar]
- Rumbold, A.R.; Giles, L.C.; Whitrow, M.J.; Steele, E.J.; E Davies, C.; Davies, M.J.; Moore, V.M. The effects of house moves during early childhood on child mental health at age 9 years. BMC Public Health 2012, 12, 583. [Google Scholar] [CrossRef]
- Metzger, M.W.; Fowler, P.J.; Anderson, C.L.; Lindsay, C.A. Residential mobility during adolescence: Do even “upward” moves predict dropout risk? Soc. Sci. Res. 2015, 53, 218–230. [Google Scholar] [CrossRef]
- Adam, E.K.; Chase-Lansdale, P.L. Home sweet home(s): Parental separations, residential moves, and adjustment problems in low-income adolescent girls. Dev. Psychol. 2002, 38, 792–805. [Google Scholar] [CrossRef]
- Nathan, K.; Robertson, O.; Carr, P.A.; Howden-Chapman, P.; Pierse, N. Residential mobility and socioemotional and behavioural difficulties in a preschool population cohort of New Zealand children. J. Epidemiol. Community Health 2019, 73, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Census of Population and Housing. 2016; Quickstats. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/036?opendocument 2019 (accessed on 29 October 2019).
- Scanlon, E.; Devine, K. Residential mobility and youth well-being: Research, policy and practice issues. J. Sociol. Soc. Welfare 2001, 28, 119–138. [Google Scholar]

{kind=link}
{kind=link}
| Variables | Number of House Moves | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2+ (Instability) | Mean Diff. 0 vs. 1 Move | Mean Diff. 1 vs. 2+ Move | Mean Diff. 0 vs. 2+ Move | |
| Children (observations) | 20,281 | 4199 | 763 | |||
| Health Summary Scores (mean) | ||||||
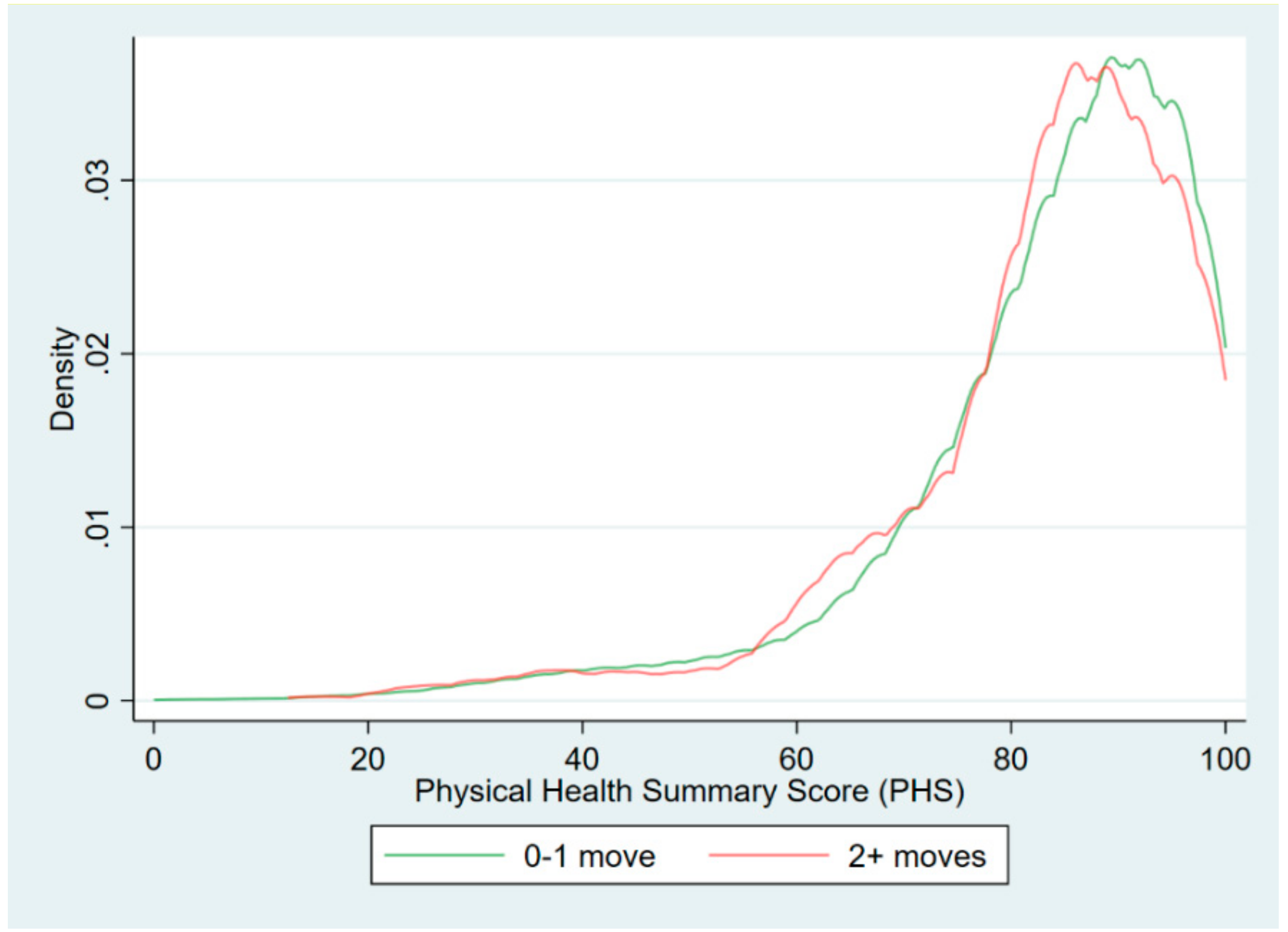
| Physical | 83.6 | 83.3 | 82.9 | |||
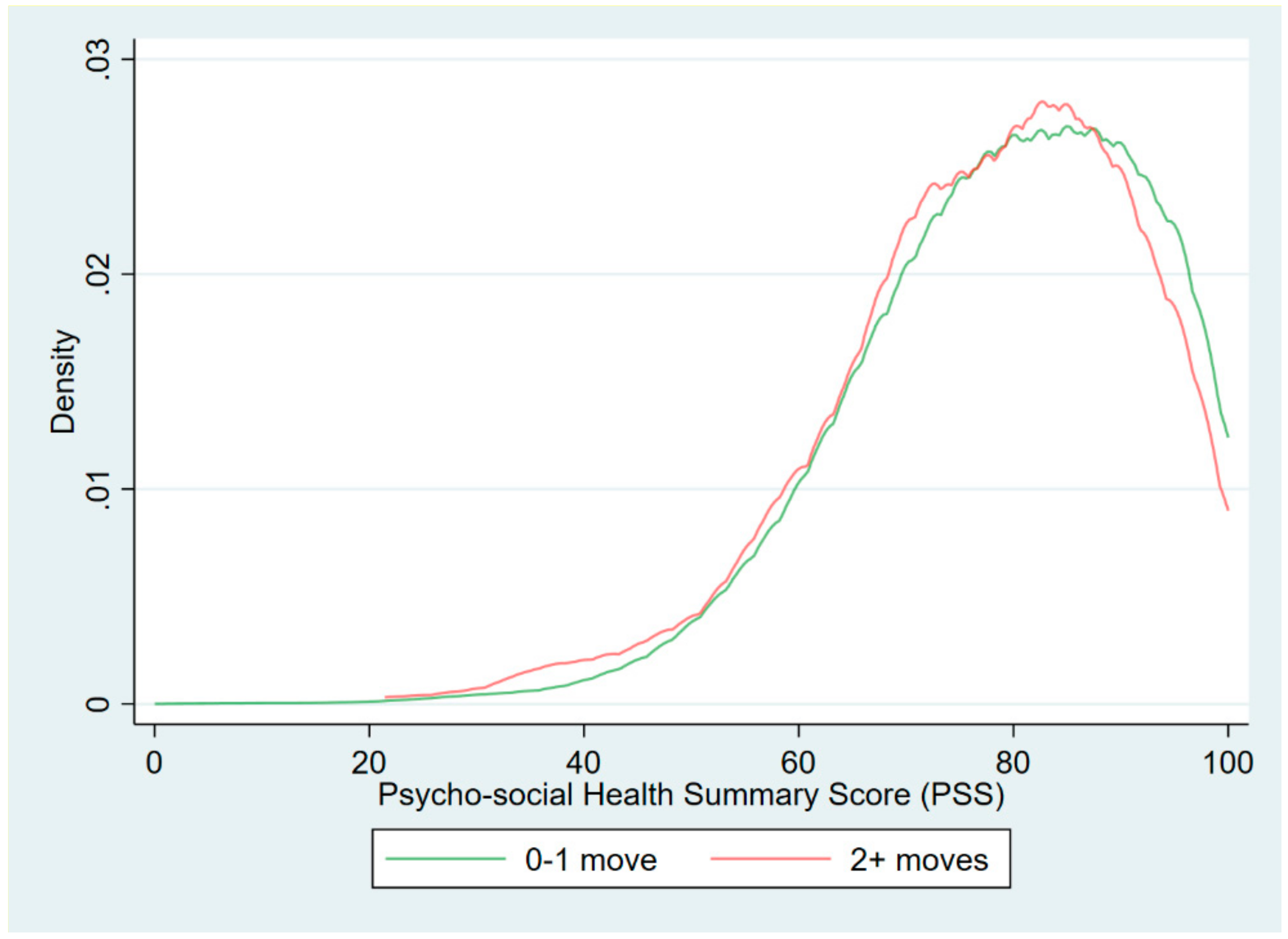
| Psycho-social | 79.1 | 78.6 | 77.2 | ** | ** | *** |
| Cohort (%) | ||||||
| Birth | 53.4 | 60.3 | 63.2 | *** | *** | |
| Kinder | 46.6 | 39.7 | 36.8 | *** | *** | |
| Average age of children (years) | 8.5 | 7.5 | 6.7 | *** | *** | *** |
| Primary care giver—Labour force status | ||||||
| Employed | 77.7 | 70.1 | 65.5 | *** | ** | *** |
| Unemployed | 1.6 | 2.4 | 2.8 | *** | ||
| Not in labor force | 20.7 | 27.5 | 31.7 | *** | ** | *** |
| Parent 2 Labour force status | ||||||
| Employed | 95.6 | 94.4 | 93.4 | *** | ** | |
| Unemployed | 1.3 | 1.8 | 2.2 | ** | ||
| Not in labor force | 3.1 | 3.8 | 4.3 | ** | ||
| Household weekly income ($ average) | 2397.2 | 2326.0 | 2207.0 | *** | ** | *** |
| Income quintile (%) | ||||||
| 1 | 10.4 | 10.7 | 10.1 | |||
| 2 | 19.2 | 19.4 | 19.7 | |||
| 3 | 22.5 | 22.0 | 21.8 | |||
| 4 | 24.0 | 22.2 | 25.0 | ** | * | |
| 5 | 23.9 | 25.8 | 23.5 | *** | ||
| Tenure (%) | ||||||
| Home owner | 91.7 | 65.0 | 58.7 | *** | *** | *** |
| Public renter | 0.9 | 0.7 | 1.7 | ** | * | |
| Private renter | 4.1 | 23.8 | 27.9 | *** | ** | *** |
| Remoteness (%) | ||||||
| City | 87.3 | 86.2 | 85.7 | * | ||
| Regional | 11.2 | 11.6 | 11.7 | |||
| Remote | 1.4 | 2.1 | 2.6 | *** | * | |
| Dwelling in fair/good condition (%) | 98.0 | 98.3 | 98.7 | |||
| Variable | Health Summary Score | |
|---|---|---|
| Physical [LCI; UCI] | Psycho-Social [LCI; UCI] | |
| Residential instability | −0.534 | −0.805 * |
| [−1.541; 0.472] | [−1.686; 0.077] | |
| Quantile Treatment Effect | ||||
|---|---|---|---|---|
| 0.05 | 0.25 | 0.5 | 0.75 | 0.95 |
| Physical Health Summary Score (PHS) | ||||
| 2.952 ** | 0.241 | −0.197 | −0.119 | 0.000 *** |
| [0.479; 5.425] | [−0.421; 0.903] | [−0.606; 0.212] | [−0.683; 0.444] | [0.000; 0.000] |
| Psycho-Social Health Score (PSS) | ||||
| −2.284 *** | −0.630 *** | −1.905 *** | 0.141 | −0.332 ** |
| [−2.864; −1.703] | [−0.997; −0.263] | [−2.849; −0.962] | [−0.078; 0.360] | [−0.638; −0.026] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baker, E.; Pham, N.T.A.; Daniel, L.; Bentley, R. How Does Household Residential Instability Influence Child Health Outcomes? A Quantile Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4189. https://doi.org/10.3390/ijerph16214189
Baker E, Pham NTA, Daniel L, Bentley R. How Does Household Residential Instability Influence Child Health Outcomes? A Quantile Analysis. International Journal of Environmental Research and Public Health. 2019; 16(21):4189. https://doi.org/10.3390/ijerph16214189
Chicago/Turabian StyleBaker, Emma, Ngoc Thien Anh Pham, Lyrian Daniel, and Rebecca Bentley. 2019. "How Does Household Residential Instability Influence Child Health Outcomes? A Quantile Analysis" International Journal of Environmental Research and Public Health 16, no. 21: 4189. https://doi.org/10.3390/ijerph16214189
APA StyleBaker, E., Pham, N. T. A., Daniel, L., & Bentley, R. (2019). How Does Household Residential Instability Influence Child Health Outcomes? A Quantile Analysis. International Journal of Environmental Research and Public Health, 16(21), 4189. https://doi.org/10.3390/ijerph16214189