Exercise as an Alternative Approach for Treating Smartphone Addiction: A Systematic Review and Meta-Analysis of Random Controlled Trials



Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Criteria for Study Selection
2.3. Data Extraction and Synthesis
2.4. Methodological Quality Assessment for Included Studies
2.5. Meta-analysis for Outcomes
2.6. Assessment of Certainty of Evidence for Meta-analysis Results
- I (high): the true effect is similar to the estimated effect with confidence;
- II (moderate): the true effect is most likely close to the estimated effect;
- III (low): the true effect might be markedly different from the estimated effect;
- IV (very low): the true effect is most likely markedly different from the estimated effect.
- Risk of bias: present if the risk of bias of included studies in meta-analysis is large in our judgement;
- Imprecision: present if sum of sample sizes of all individual studies included in meta-analysis is less than 500;
- Inconsistency: present if heterogeneity statistic I-squared in meta-analysis is greater than 50%;
- Indirectness: present if the intervention studied in meta-analysis is not directly relevant to the outcome;
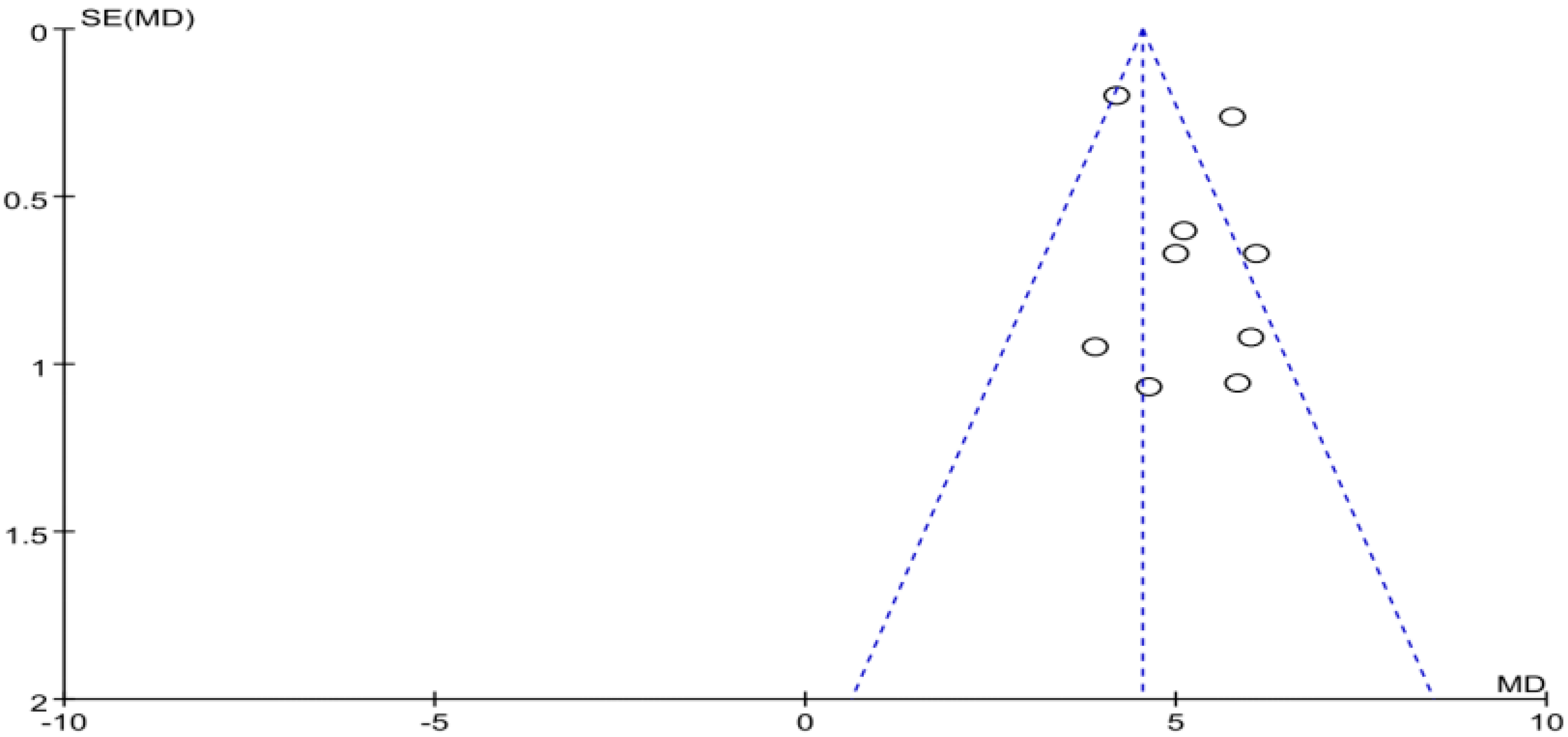
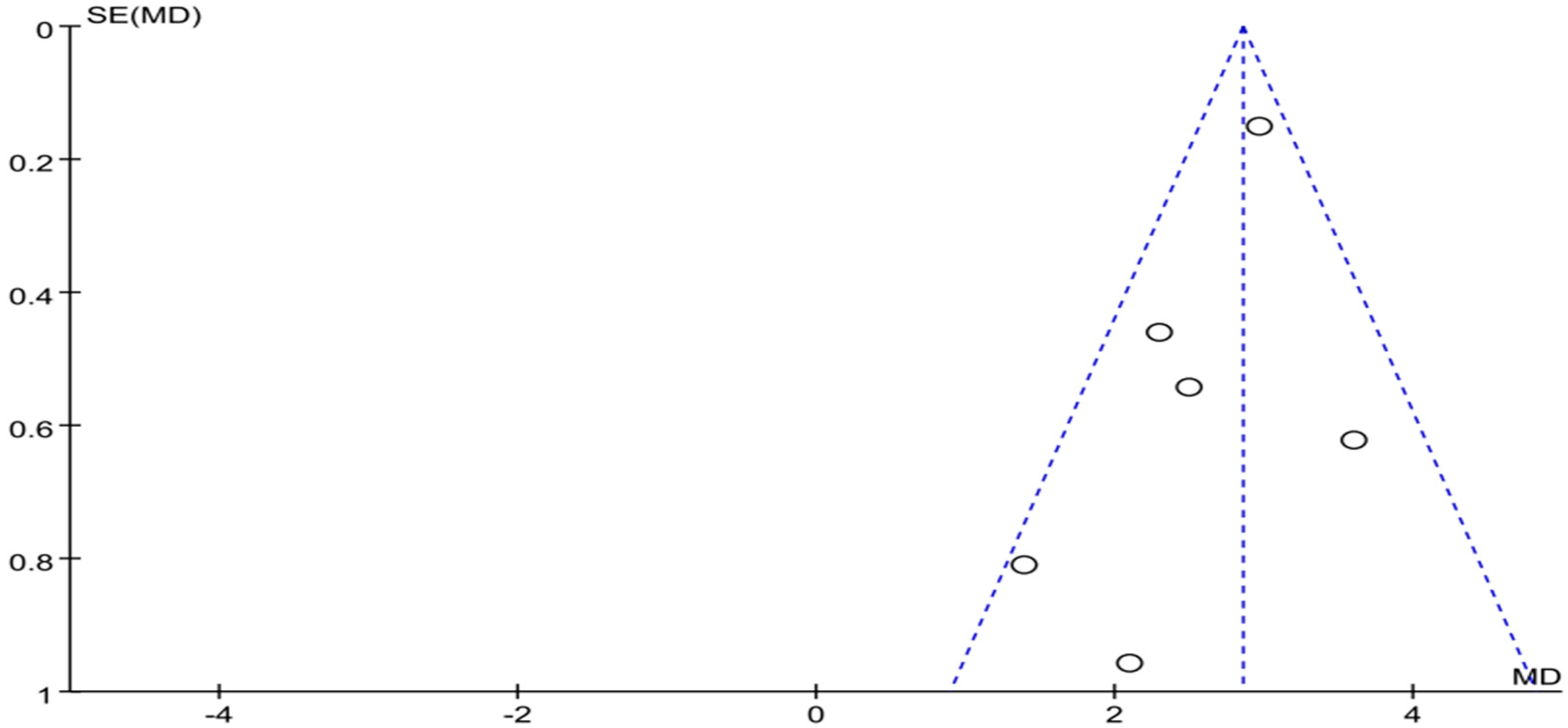
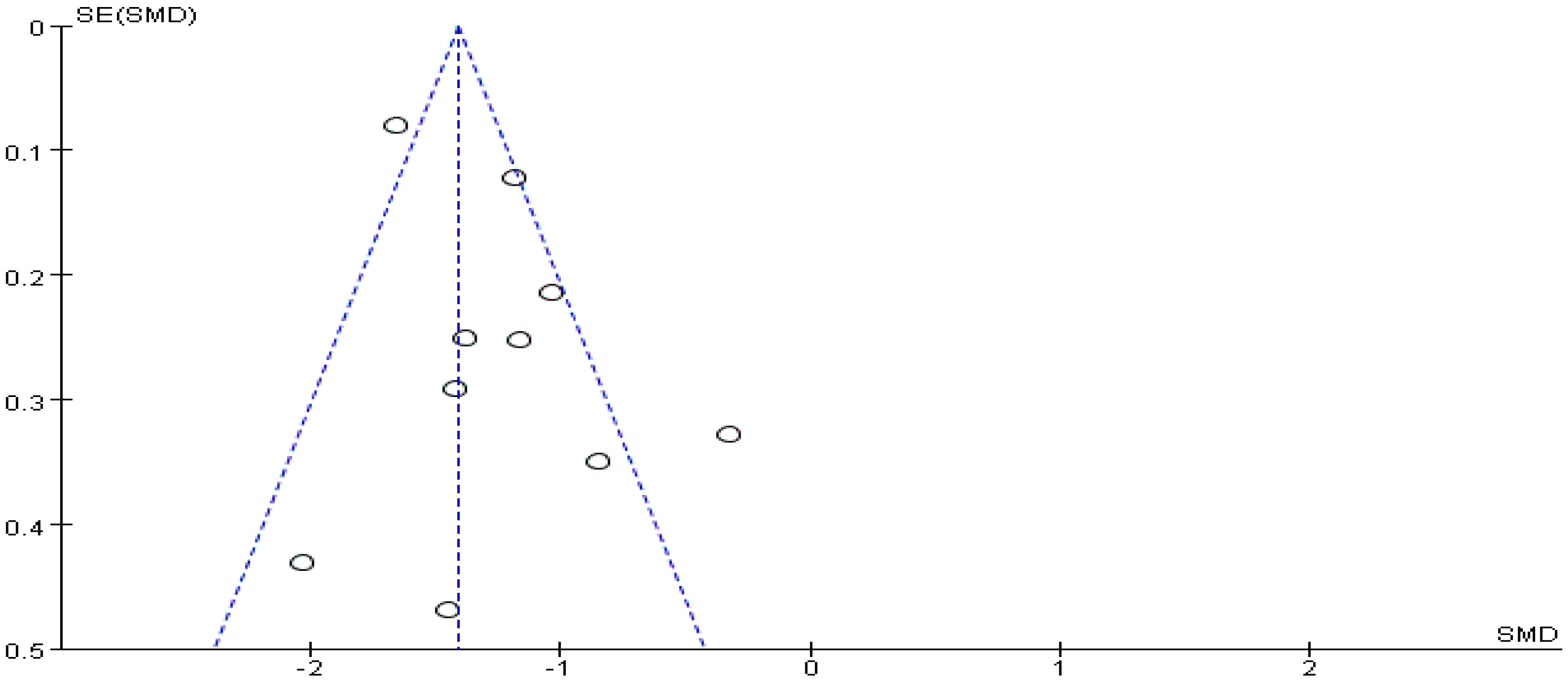
- Publication bias: present if the p-value of Begg’s test for the publication bias in meta-analysis is less than 0.05.
3. Results
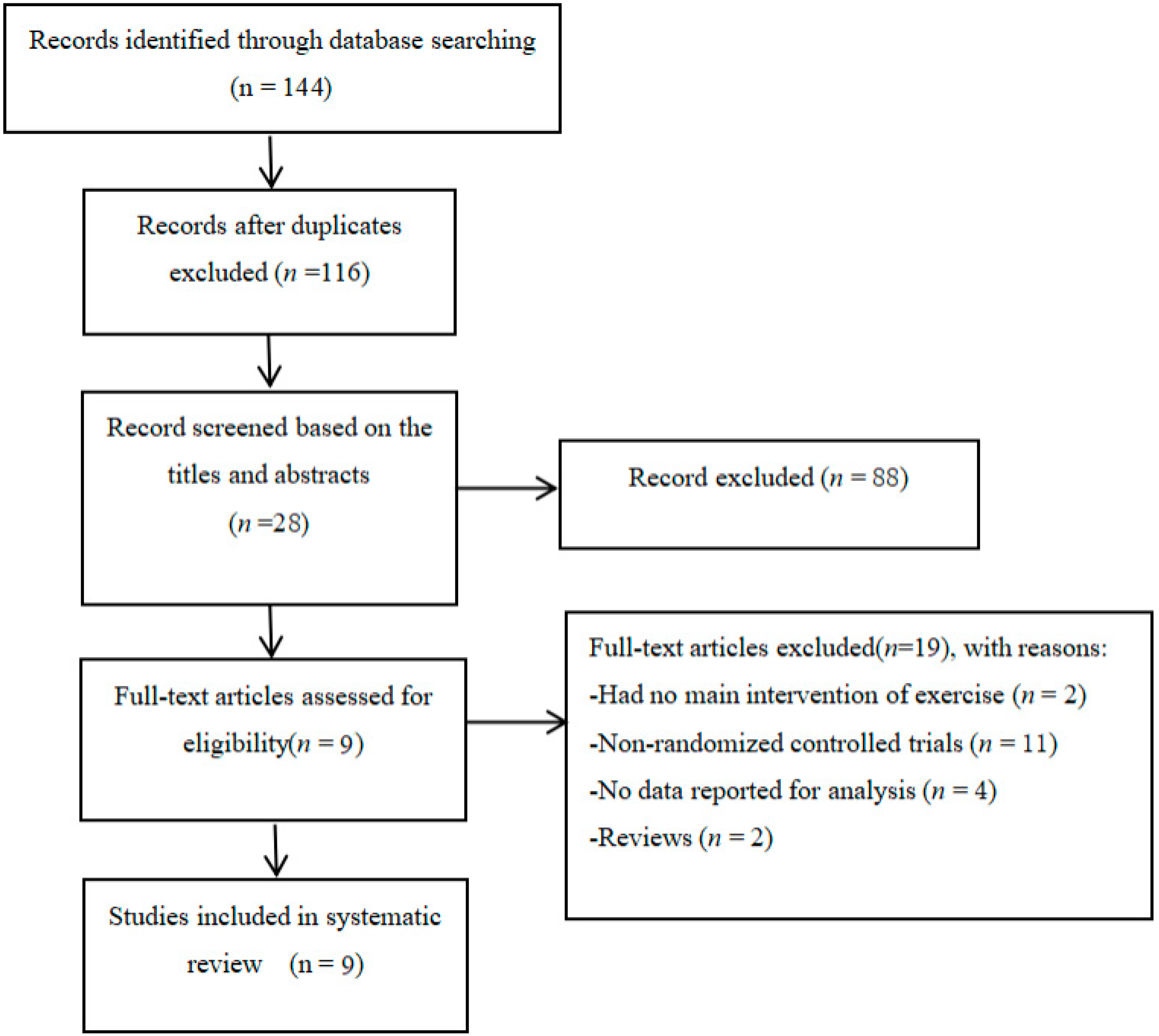
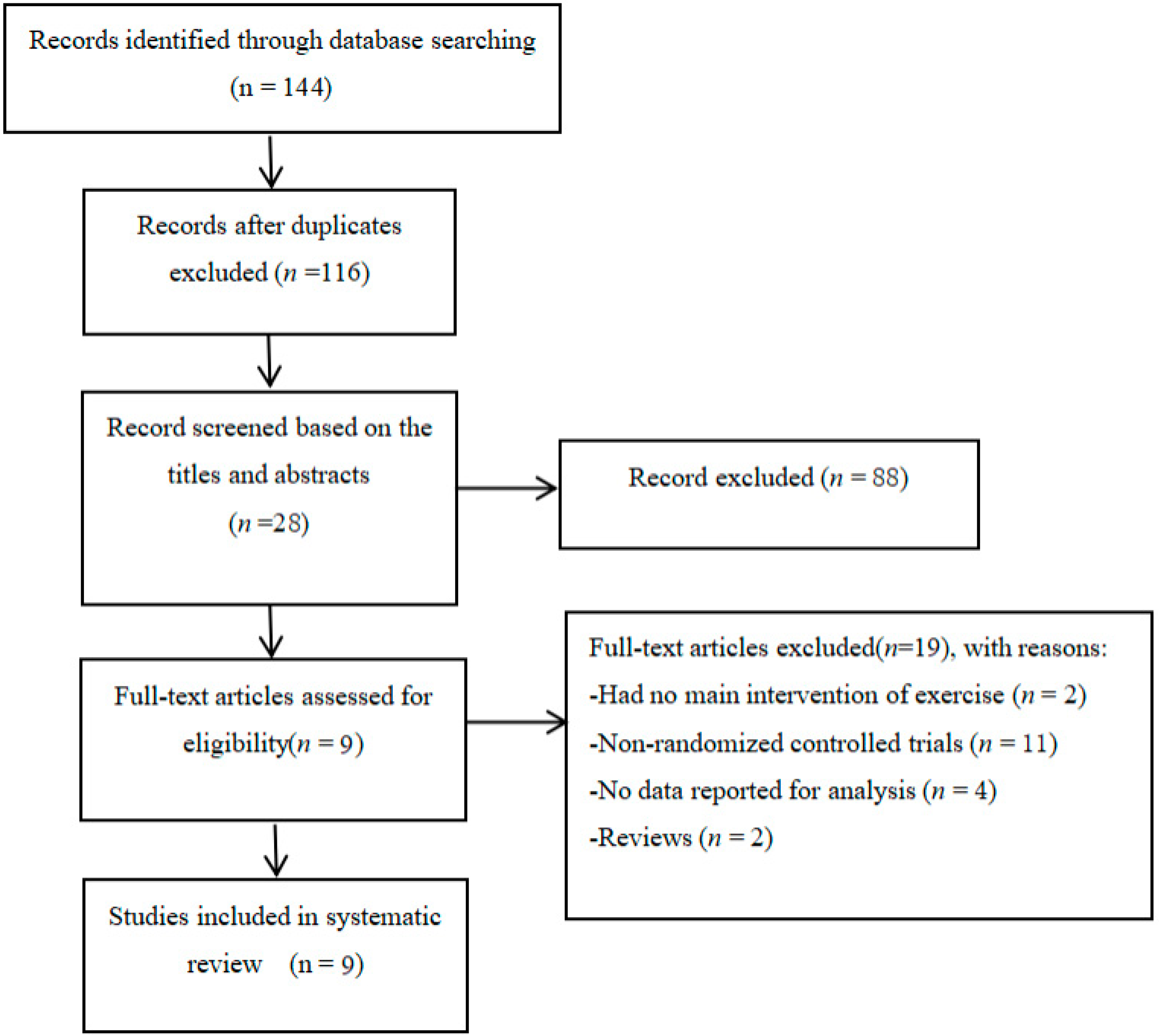
3.1. Study Selection
3.2. Characteristics of Eligible Studies
3.3. Methodological Quality Assessment
3.4. Data Synthesis of Behavioral Outcomes
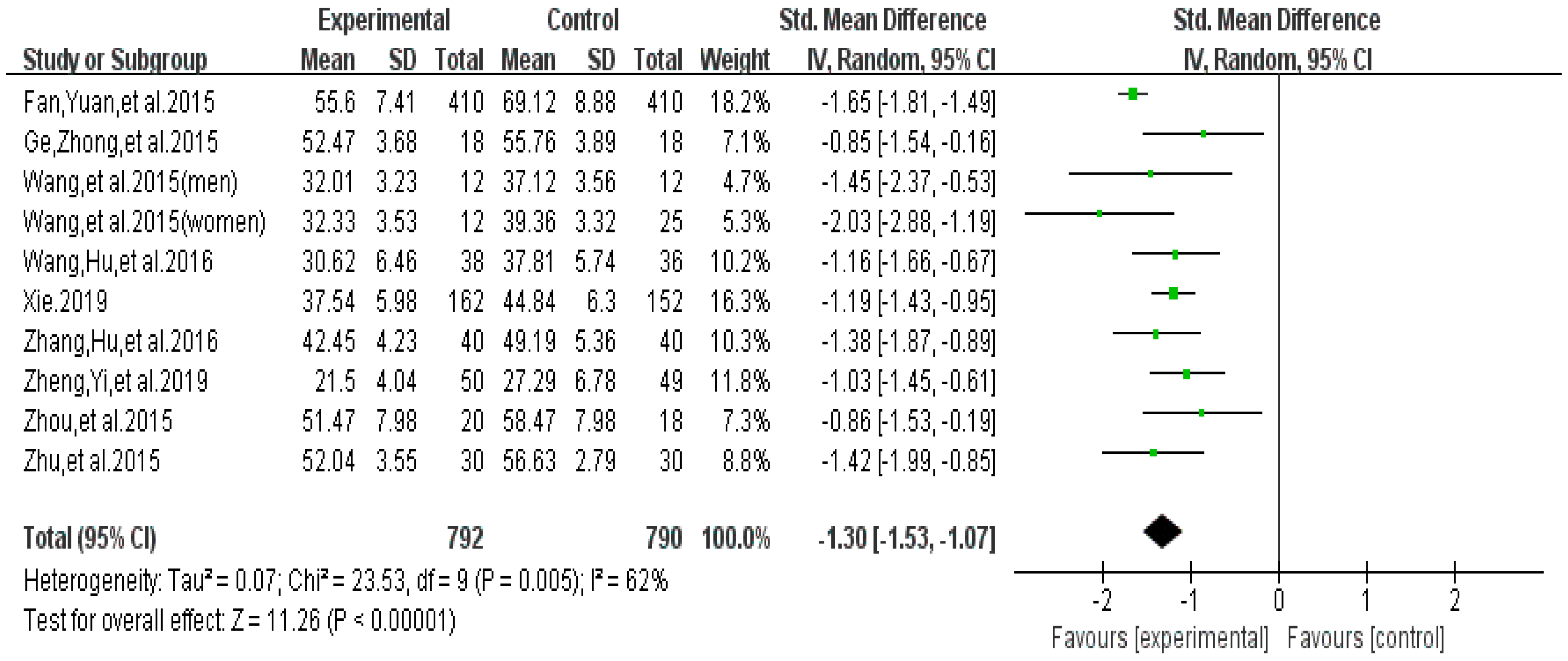
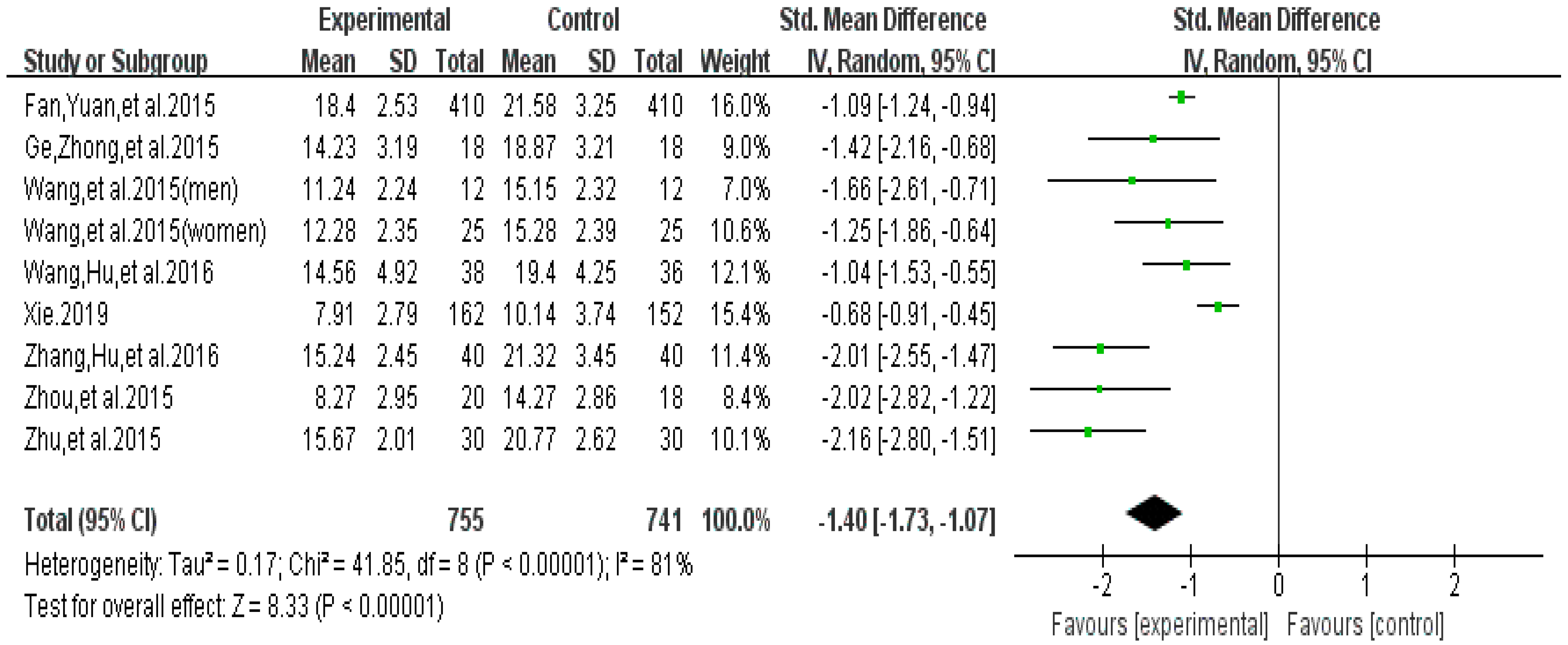
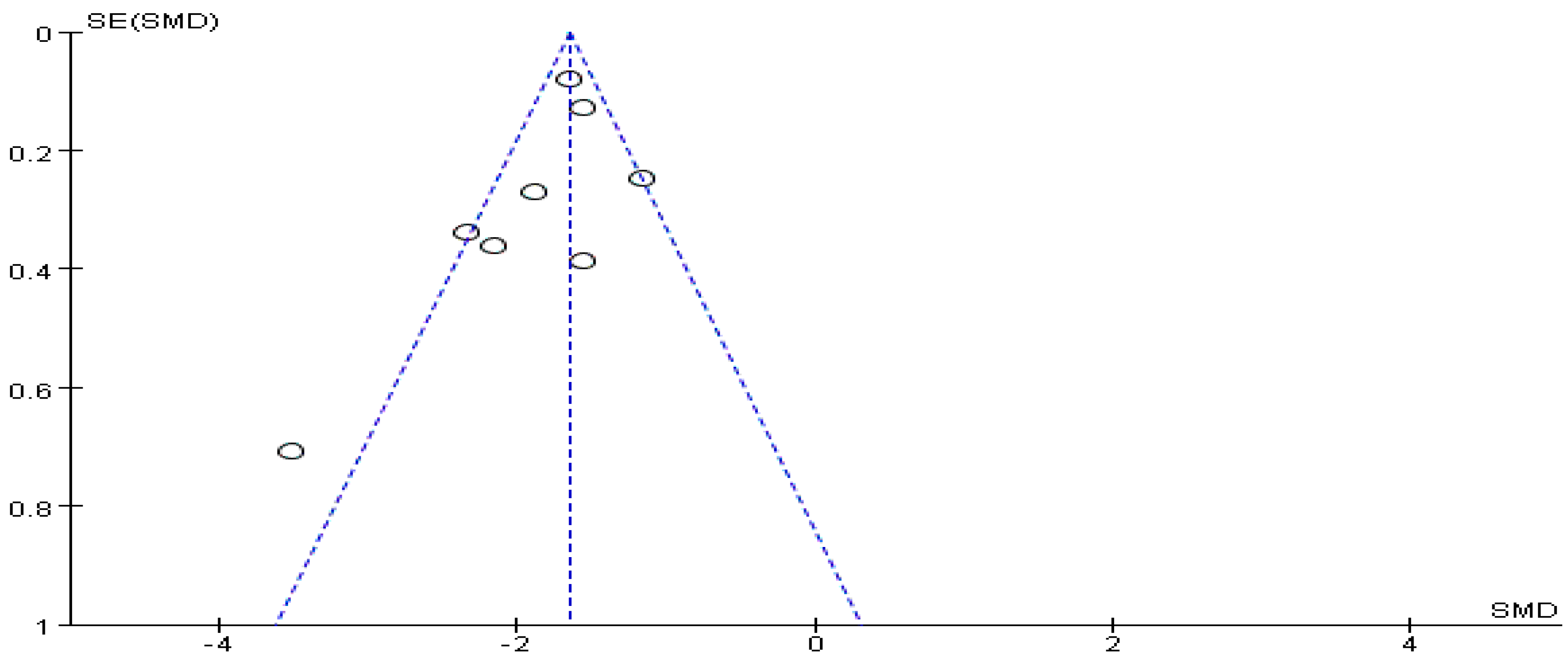
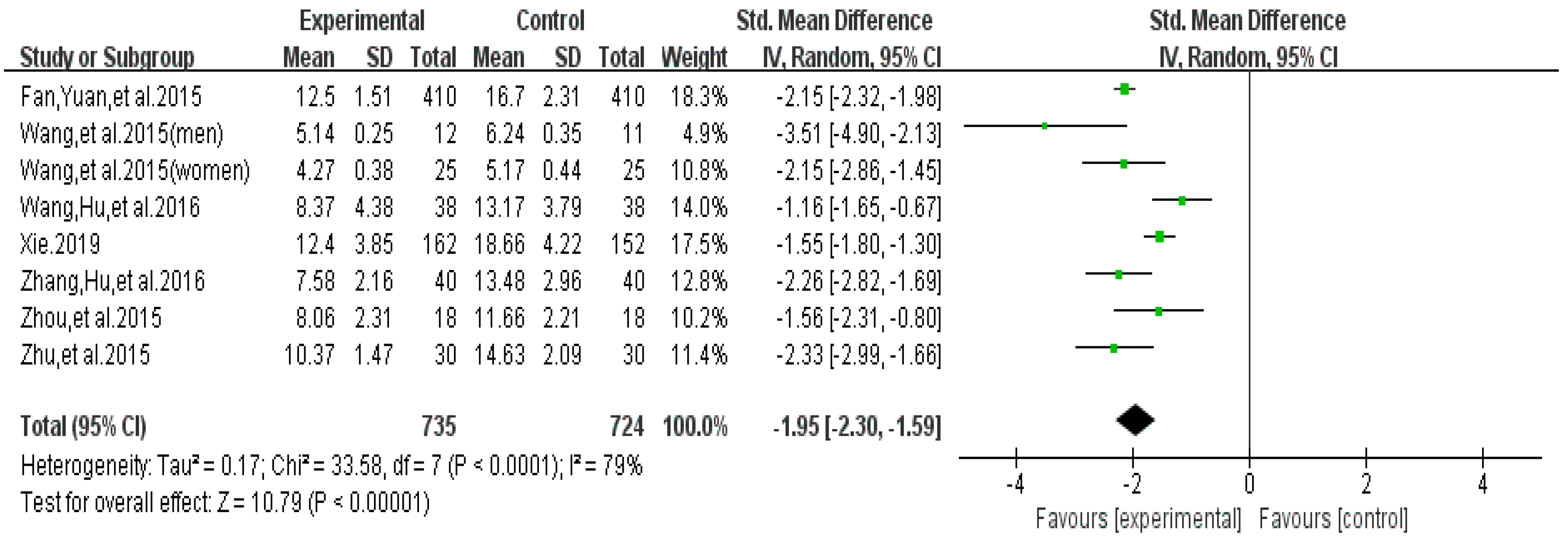
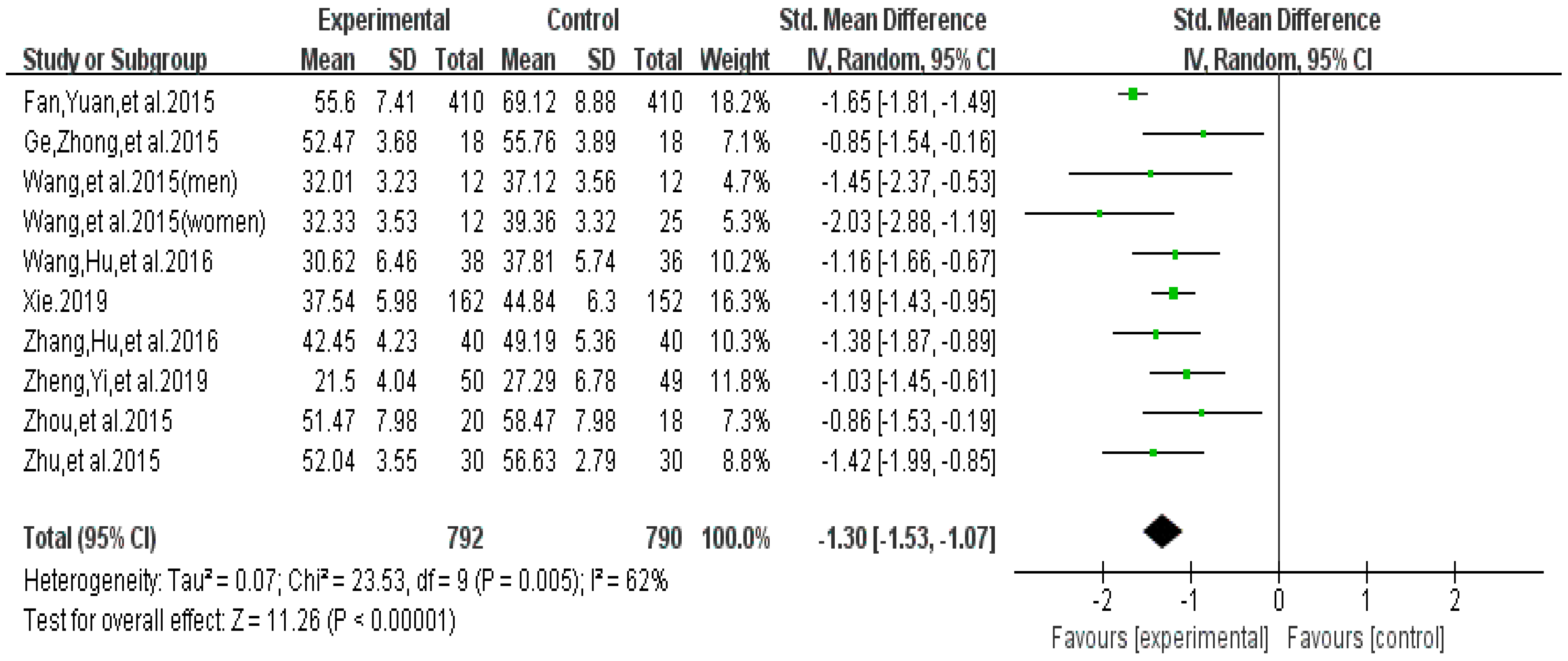
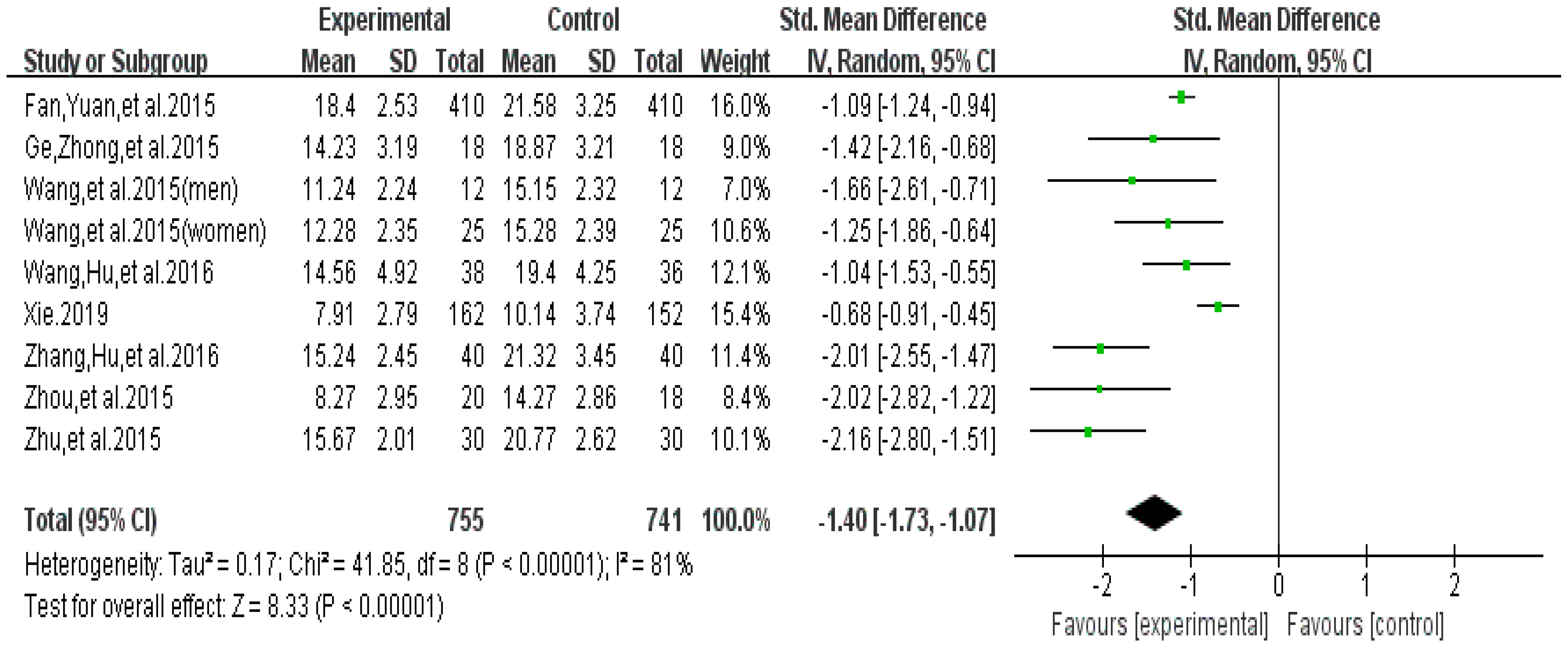
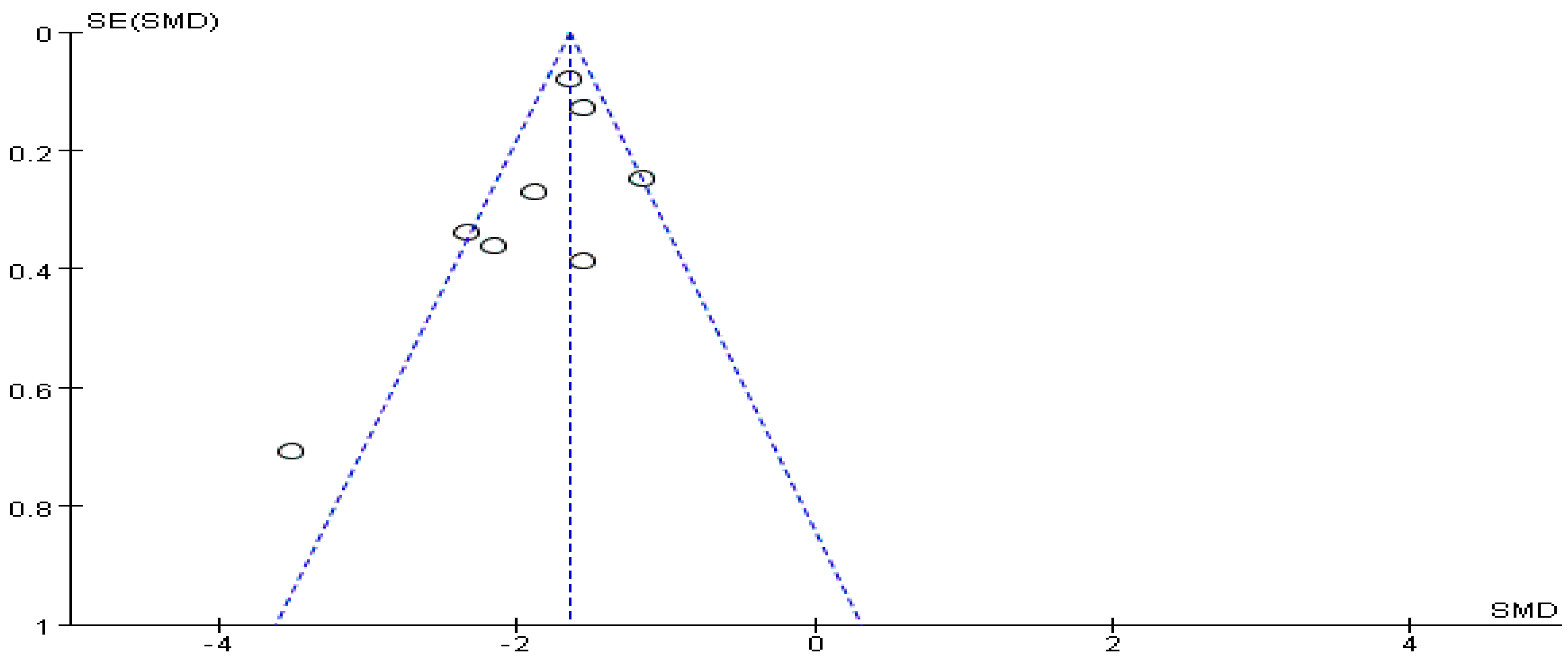
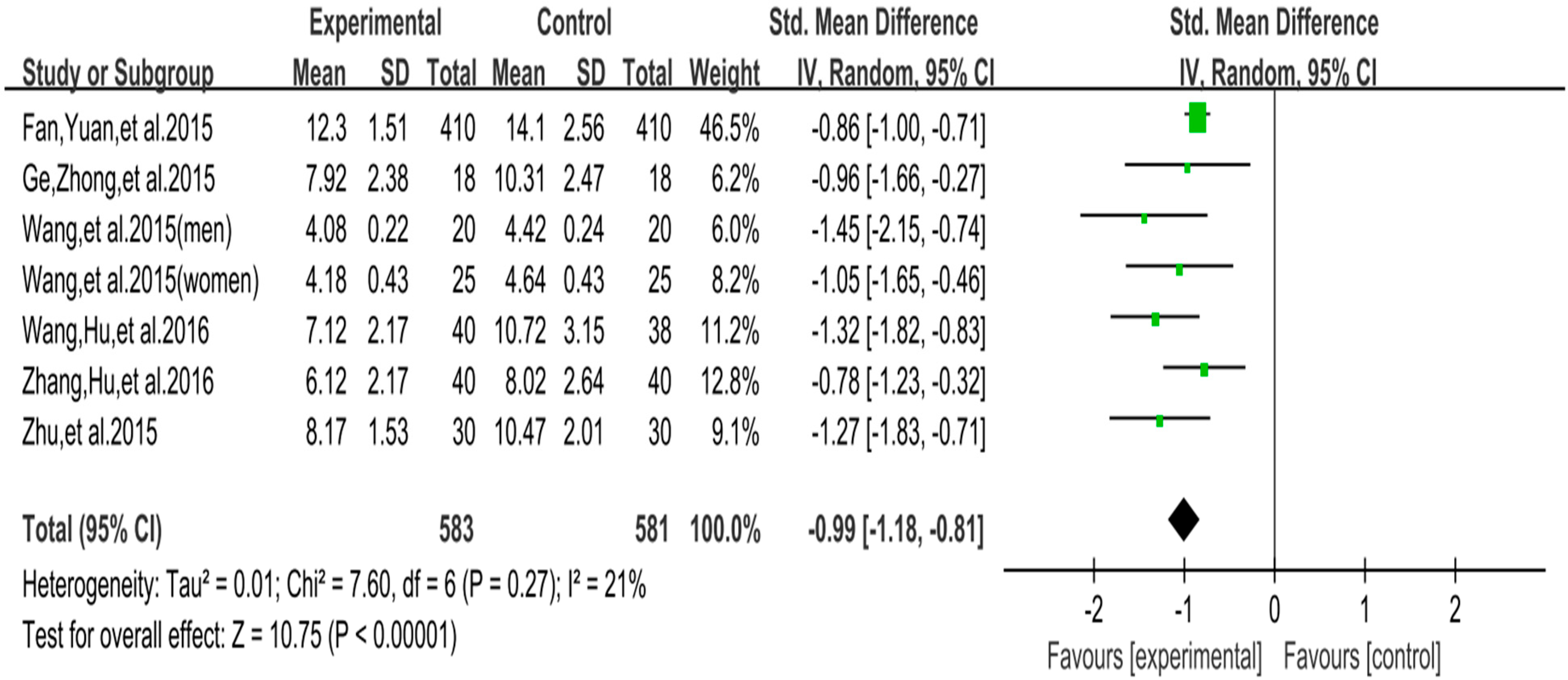
3.4.1. Effect of Exercise Interventions on Withdrawal Symptoms
3.4.2. Summary of Certainty of Evidence
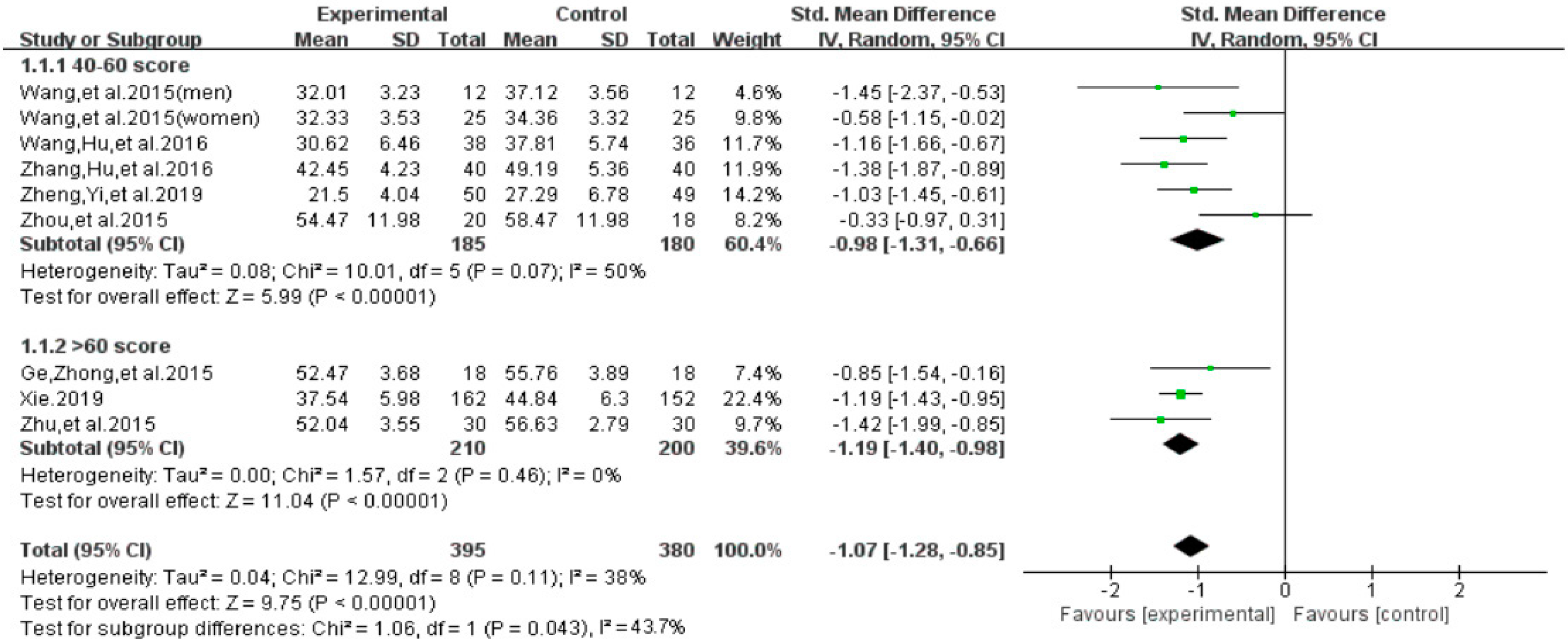
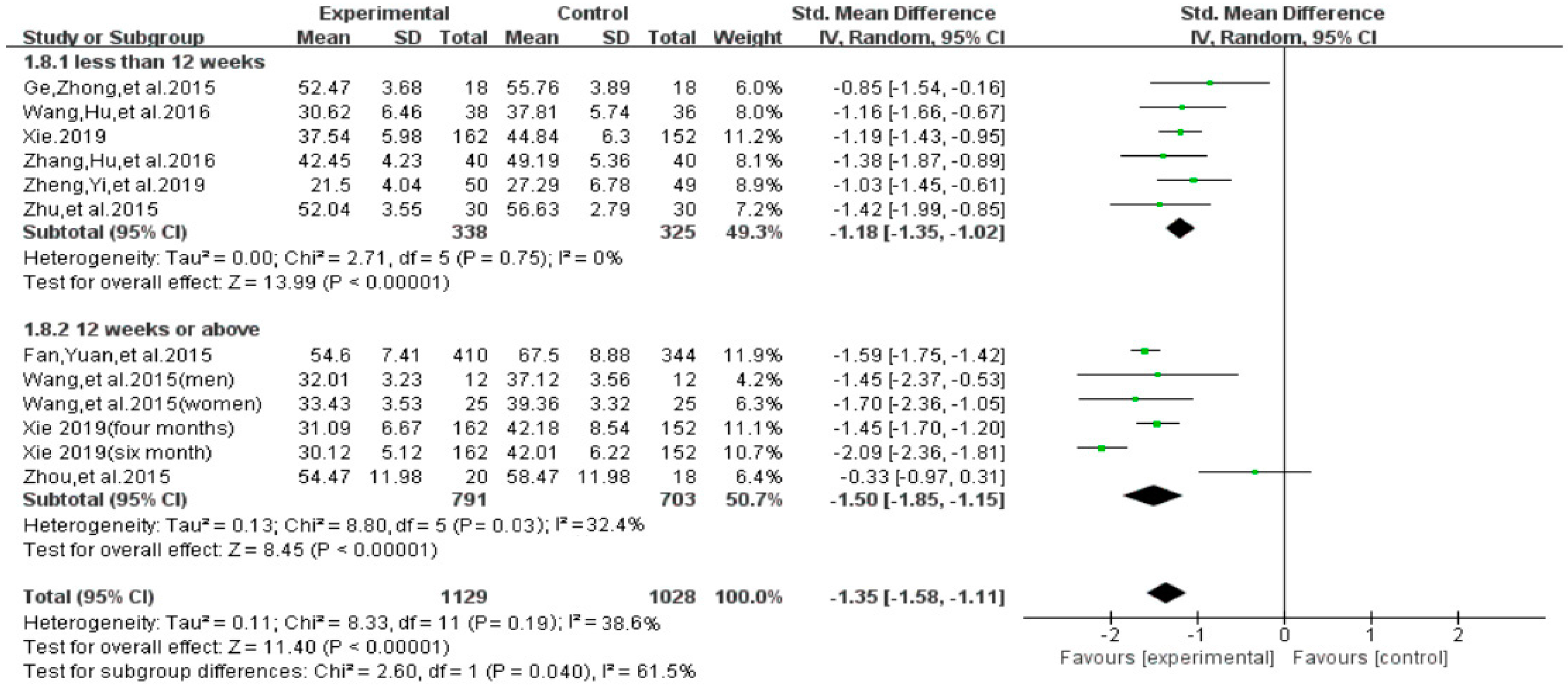
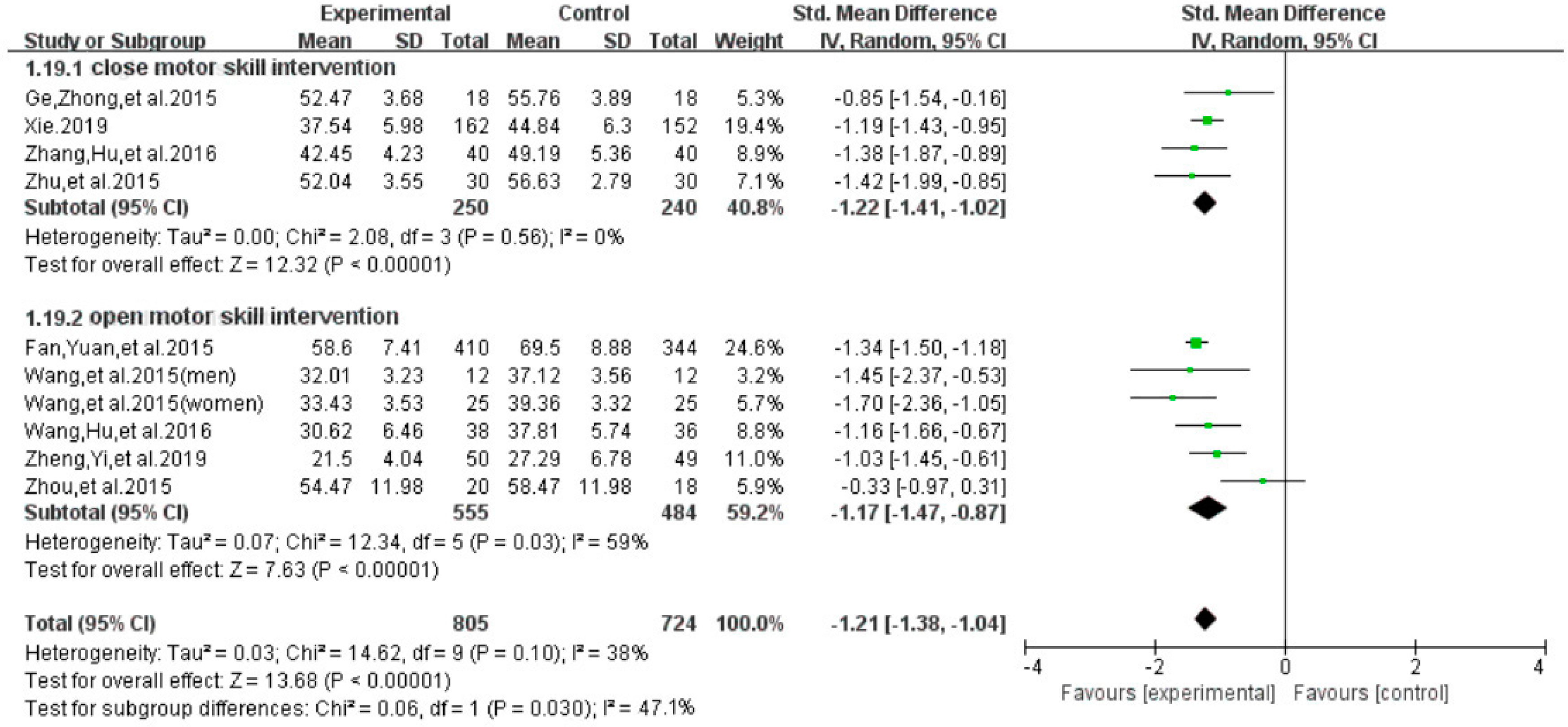
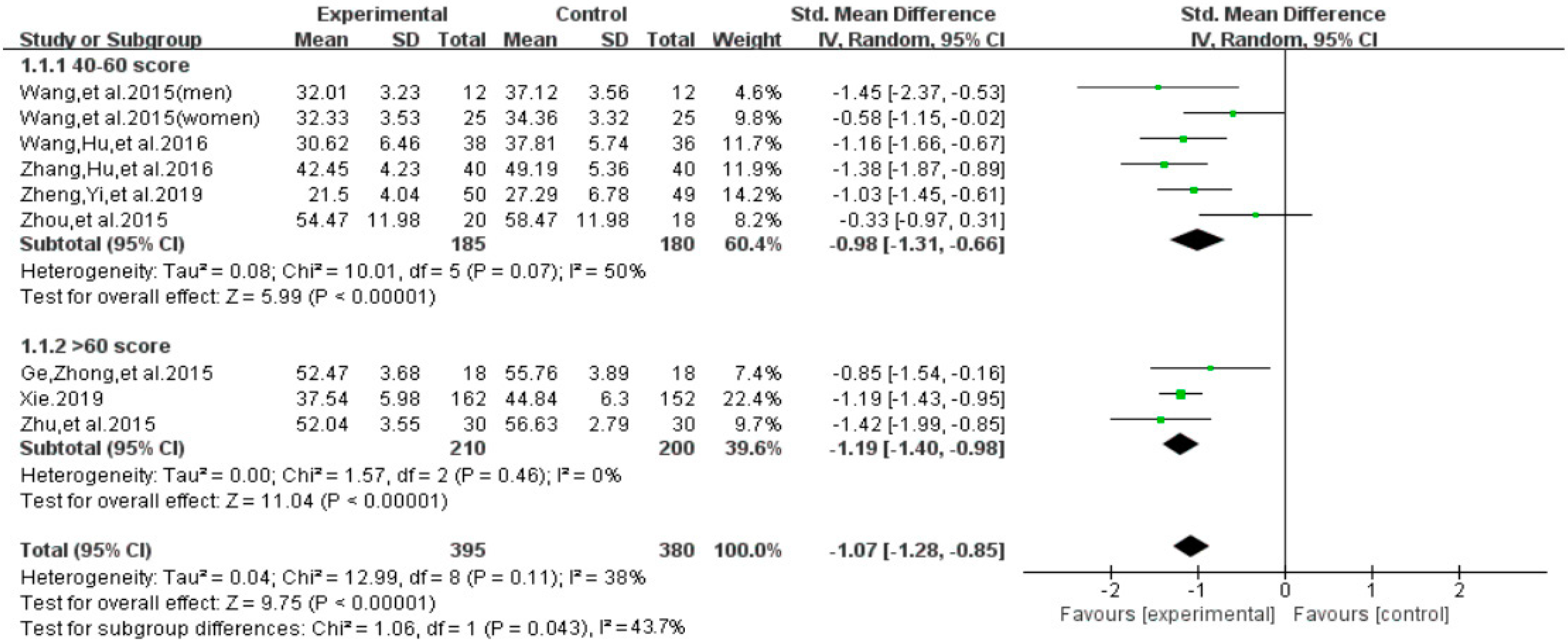
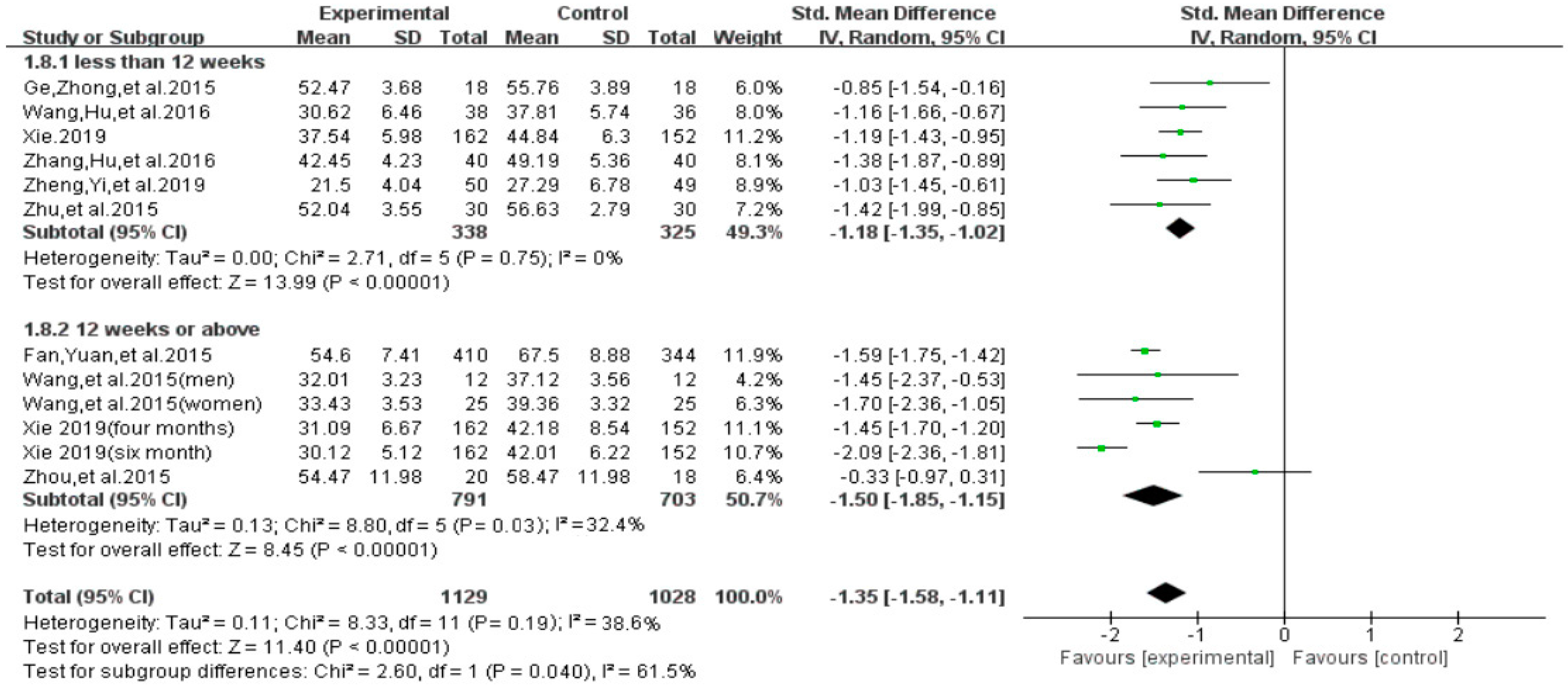
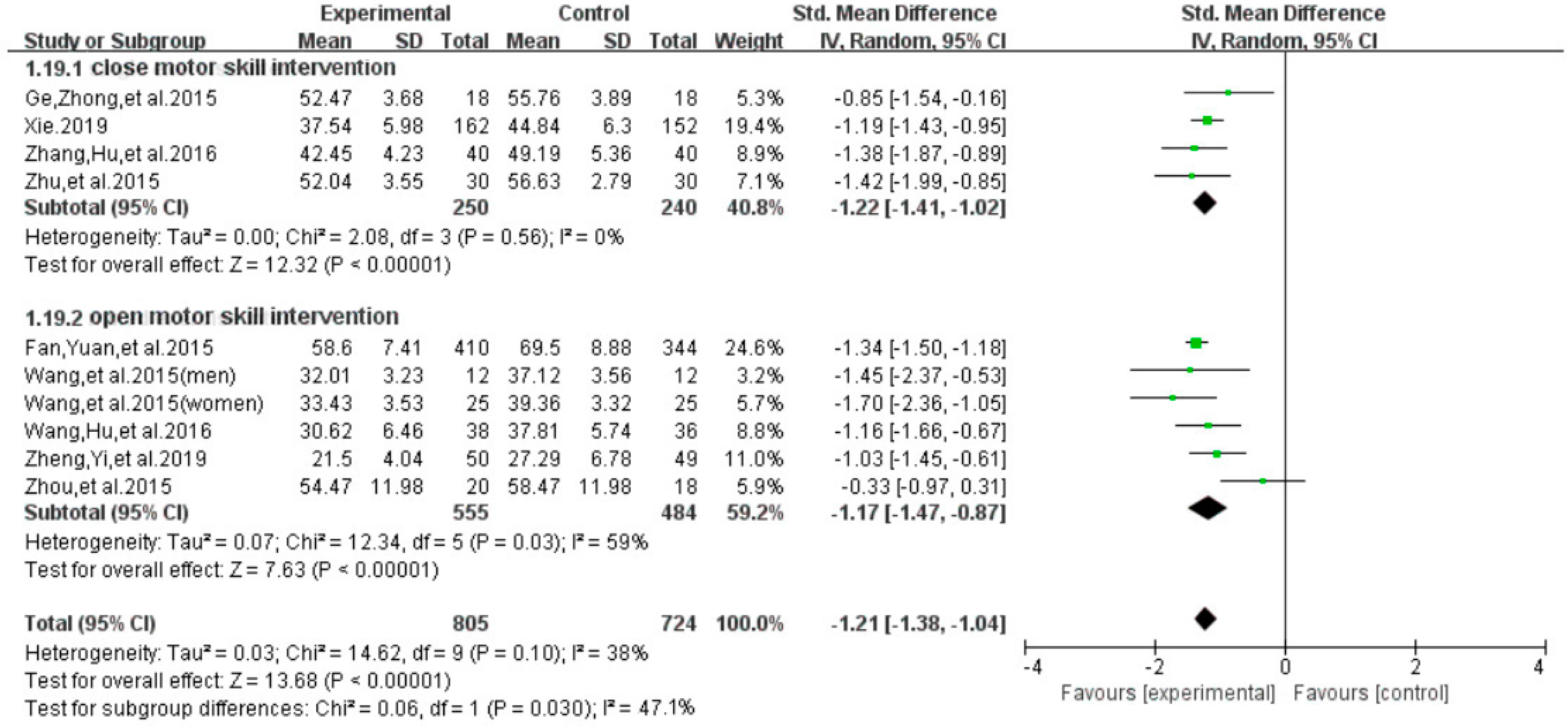
3.4.3. Subgroup Analysis for Total Score of Smartphone Addiction
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sally, A.; Ellis, D.A.; Heather, S. Beyond Self-Report: Tools to Compare Estimated and Real-World Smartphone Use. PLoS ONE 2015, 10, e0139004. [Google Scholar] [CrossRef]
- Seo, D.G.; Park, Y.; Kim, M.K. Mobile phone dependency and its impacts on adolescents’ social and academic behaviors. Comput. Hum. Behav. 2016, 63, 282–292. [Google Scholar] [CrossRef]
- Digital Minimalism: How to Hang up on Your Phone Addiction. Available online: https://www.npr.org/tags/320325126/smartphone-addiction (accessed on 18 September 2019).
- Chinese Spend 3 hours a Day on Their Smartphones, Ranking 2nd in the World: Survey. Available online: http://www.chinadaily.com.cn/china/2017-06/28/content_29916889.htm (accessed on 18 June 2019).
- A Statistical Report on the Development of the Internet in China. Available online: http://www.cnnic.net.cn/hlwfzyj/hlwxzbg/hlwtjbg/201902/t20190228_70645.htm (accessed on 18 June 2019).
- Lin, Y.H.; Lin, Y.C.; Lee, Y.H. Time distortion associated with smartphone addiction: Identifying smartphone addiction via a mobile application (App). J. Psychiatr. Res. 2015, 65, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Lin, Y.C.; Lin, S.H. To use or not to use, Compulsive behavior and its role in smartphone addiction. Transl. Psychiatry 2017, 7, e1030. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, J.S.; Valkenburg, P.M.; Peter, J. Development and Validation of a Game Addiction Scale for Adolescents. Media Psychol. 2009, 12, 77–95. [Google Scholar] [CrossRef]
- Mariano, C. Mobile phone addiction: Apoint issue. Addiction 2010, 105, 373–374. [Google Scholar] [CrossRef]
- Koo, H.Y. Development of a cell phone addiction scale for korean adolescents. J. Korean Acad. Nurs. 2009, 39, 818–828. [Google Scholar] [CrossRef]
- Leisure Boredom. Addiction Symptoms and Patterns of Cell Phone Useensation Seeking Self-Esteem. Available online: http: //www.com.cuhk.edu.hk (accessed on 18 June 2019).
- Xiong, J.; Zhou, Z.K. Compilation of mobile phone addiction tendency scale for college students. Chin. J. Ment. Health 2010, 26, 222–228. [Google Scholar] [CrossRef]
- Young, K.S. Psychology of computer use: XL. addictive use of the internet: A case that breaks the stereotype. Psychol. Rep. 1996, 79, 899–902. [Google Scholar] [CrossRef]
- Goldberg, I. Internet Addiction Disorder. Electronic Message Posted to Research Discussion List. 1996. Available online: http://users.rider.edu/,suler/psycyber/supportgp.html (accessed on 18 June 2019).
- Berolo, S.; Wells, R.P.; Amick, B.C., III. Musculoskeletal symptoms among mobile hand-held device users and their relationship to device use: A preliminary study in a Canadian university population. Appl. Ergon. 2011, 4, 371–377. [Google Scholar] [CrossRef]
- Mizuko, I. Symptoms of problematic cellular Phone use, functional impairment and its association with depression among adolescents in Southern Taiwan. J. Adolesc. 2009, 32, 863–873. [Google Scholar] [CrossRef]
- Matar-Boumosleh, J.; Jaalouk, D. Depression, anxiety, and smartphone addiction in university students—A cross sectional study. PLoS ONE 2017, 12, e0182239. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Min, J.Y.; Kim, H.J.; Min, K.B. Accident risk associated with smartphone addiction: A study on university students in Korea. J. Behav. Addict. 2017, 6, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Sugiyama, T.; Eakin, E.E. Adults’ Sedentary Behavior: Determinants and Interventions. Am. J. Prev. Med. 2011, 41, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.E.; Norman, G.J.; Wagner, N. Reliability and Validity of the Sedentary Behavior Questionnaire (SBQ) for Adults. J. Phys. Act. Health 2010, 7, 697–705. [Google Scholar] [CrossRef]
- Lepp, A.; Barkley, J.E.; Sanders, G.J. The relationship between cell phone use, physical and sedentary activity, and cardiorespiratory fitness in a sample of U.S. college students. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 79. [Google Scholar] [CrossRef]
- Kim, H. Exercise rehabilitation for smartphone addiction. J. Exerc. Rehabil. 2013, 9, 500–505. [Google Scholar] [CrossRef]
- Huang, L.N.; Chen, H.W.; Ye, X.Q.; Ji, L.H.; Xie, Y.M. Effects of percutaneous electrical nerve stimulation on surface emg signals in robot-assisted upper limb exercise training. Chin. J. Rehabil. Med. 2010, 25, 963–969. [Google Scholar]
- Ye, G.Z.; Liu, W.A.; Xu, X.M.; Chen, J.; Wu, G.Y. Quantitative analysis of rectus femoris, vastus medialis and vastus lateralis muscles under different exercise patterns in Chinese adults. Chin. J. Mod. Med. 2019, 9, 1–5. [Google Scholar]
- Zhu, Y.F. Intervention Study of Physical Exercise on College Students’ Mobile Addiction Tendency. Zhejiang Sports Sci. 2017, 6, 90–97. [Google Scholar]
- Zhang, J.S.; Hu, R.K.; Xu, Y.Q. Research on the Intervention of College Students’ Mobile Phone Dependence by Outdoor Development Movement. Sci. Technol. Vis. 2016, 321. [Google Scholar] [CrossRef]
- Zhou, L.R. Experimental Study on the Intervention of Aerobic Exercise on College Students’ Mobile Phone Dependence. Shaolin Taiji 2015, 7, 47–51. [Google Scholar]
- Wang, X.T.; Zhang, C. Research on the Exercise Intervention of Mental Health Level of Mobile Phone Addiction Medical Students. China High. Med Educ. 2016, 7, 29–30. [Google Scholar] [CrossRef]
- Fan, R.C.; Yuan, X.Y. Experimental Research on Sports Intervention on College Students’ Mobile Addiction. J. Contemp. Sports Sci. 2015, 5, 1–2. [Google Scholar]
- Wang, K. The Influence of Sports Intervention on the Degree of College Students’ Mobile Addiction. Sports Res. Educ. 2016, 8, 109–112. [Google Scholar] [CrossRef]
- Ge, R.Z.; Zhong, X.M.; Chen, R. Research on the Influence of Sports Intervention on College Students’ Mobile Phone Dependence. Mod. Prev. Med. 2015, 42, 3919–3921. [Google Scholar]
- Zheng, X.N.; Yi, S.M.; Chen, Y.; Liu, L.B.; Zhu, Y.C.; He, L.Y. Effects of exercise-oriented comprehensive intervention on college students’ mobile phone dependence and sleep quality. Health Vocat. Educ. 2019, 37, 125–127. [Google Scholar]
- Xie, F. Current Situation of Mobile Phone Addication in Nursing Students and Study on Baduanjin Health Education Intervention; Shanxi medical university: Shanxi, China, 2019. [Google Scholar]
- Gao, Y.Y.; Zhang, Y.; Chen, Z. Relationship between mobile phone dependence and positive and negative emotions of medical students. Health Vocat. Educ. 2017, 35, 119–121. [Google Scholar]
- Zou, L.; Zhang, Y.J.; Sasaki, J.F.; Yeung, A.S.; Yang, L.; Sun, J.; Liu, S.J.; Yu, J.J.; Sun, S.Y. Wuqinxi Qigong as an Alternative Exercise for Improving Risk Factors Associated with Metabolic Syndrome: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 1396. [Google Scholar] [CrossRef]
- Vrabel, M. Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Oncology Nursing Forum 2015, 18, e123. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Sultan, S.; Brozek, J.; Glasziou, P.; Alonso-Coello, P. GRADE guidelines: 11. Making an overall rating of confidence in effect estimates for a single outcome and for all outcomes. J. Clin. Epidemiol. 2013, 66, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.S.; Wang, Y.Q. Impact of Physical Exercise on Substance Use Disorders: A Meta-Analysis. PLoS ONE 2014, 9, e110728. [Google Scholar] [CrossRef] [PubMed]
- Linke, S.E.; Ussher, M. Exercise-based treatments for substance use disorders: Evidence, theory, and practicality. Am. J. Drug Alcohol Abus. 2015, 41, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Alissa, M.; Ben, J.; Dimmock, J.A. Exercise in the Treatment of Youth Substance Use Disorders: Review and Recommendations. Front. Psychol. 2017, 8, 1839–1849. [Google Scholar] [CrossRef]
- Kim, S.E.; Kim, J.W.; Jee, Y.S. Relationship between smartphone addiction and physical activity in Chinese international students in Korea. J. Behav. Addict. 2015, 4, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Haug, S.; Castro, R.P.; Min, K. Smartphone use and smartphone addiction among young people inSwitzerland. J. Behav. Addict. 2015, 4, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Katharine, B.; Masahiro, T. Phone-Reliant Britons in the Grip of Homophobia, the Independent. Available online: http://www.independent.co.UK/news/UK/home-news/phonereliant-nomophobia-802722 (accessed on 11 June 2019).
- Bechara, A. Decision making, impulse control and loss of willpower to resist drugs: A neurocognitive perspective. Nat. Neurosci. 2005, 8, 1458. [Google Scholar] [CrossRef]
- Bian, M.; Leung, L. Smartphone Addiction: Linking Loneliness, Shyness, Symptoms and Patterns of Use to Social Capital. Media Asia 2014, 41, 159–176. [Google Scholar] [CrossRef]
- Kamibeppu, K.; Sugiura, H. Impact of the Mobile Phone on Junior High-School Students Friendships in the Tokyo Metropolitan Area. Cyberpsychol. Behav. 2005, 8, 121–130. [Google Scholar] [CrossRef]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef]
- Ren, B. Analysis and Thinking of Physical Exercises Affecting College Students’ Mental Health Model. J. Beijing Sport Univ. 2008, 31, 644–646. [Google Scholar] [CrossRef]
- Weinstein, A.; Lejoyeux, M. New developments on the neurobiological and pharmaco-genetic mechanisms underlying internet and videogame addiction. Am. J. Addict. 2013, 24, 178–197. [Google Scholar] [CrossRef] [PubMed]
- Warlaumont, A.S.; Finnegan, M.K. Learning to Produce Syllabic Speech Sounds via Reward-Modulated Neural Plasticity. PLoS ONE 2016, 11, e0145096. [Google Scholar] [CrossRef] [PubMed]
- Fabian, Z.; Treuer, T.; Füredi, J. Internet addiction associated with features of impulse control disorder: Is it a real psychiatric disorder? J. Affect. Disord. 2001, 66, 283. [Google Scholar] [CrossRef]
- Xue, Y.; Yang, Y.X.; Huang, T. Effects of chronic exercise interventions on executive function among children and adolescents: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 24, 312–334. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Location (Language) | Participant Characteristics | Intervention Program | Motor Skill Training | Outcome Measured | Adverse Event; Follow-Up | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Smart Phone Addiction Level | Mean Age or Age Range | Frequency (weekly) | Time (min) | Duration (week) | |||||
| Zhu, et al. (2015) [25] | Zhejiang, China (Chinese) | 60 | Mild-to-moderate level | 20.72 ± 1.30 | EG: Taijiquan CG: Usual Care | 3 | 60 | 8 | MPATS (WS; SC; MC; HBsalience) | No No |
| Zhang, Hu, et al. (2016) [26] | Hunan, China (Chinese) | 80 | Mild-to-moderate level | 18–22 | EG: Run CG: Usual Care | 2 | 45 | 8 | MPATS (WS; SC; MC; HBsalience) | No No |
| Zhou, et al. (2015) [27] | Zhengzhou, China (Chinese) | 18 | Severe level | 20.33 ± 1.64 (freshman) | EG: Bicycle + Basketball + Badminton CG: Usual Care | 3 | 60 | 12 | MPAI (WS, HBuncontrolled) | No No |
| Wang, et al. (2015) [28] | Taiyuan, China (Chinese) | 73 | Mild-to-moderate level | 18–22 | EG: Basketball + Badminton + Football + Tennis CG: Usual Care | 3 | 45 | 12 | MPATS (WS; SC; MC; HBsalience) | No No |
| Fan, Yuan, et al. (2015) [29] | Nanjing, China (Chinese) | 754 | NR | 18–22 (freshman) | EG: Basketball + Badminton + Football + Tennis CG: Usual Care | 5 | 45–60 | 12 | MPATS (WS; SC; MC; HBsalience) | No No |
| Wang, Hu, et al. (2016) [30] | Shandong, China (Chinese) | 49 | Mild-to-moderate level | 19.71 ± 1.52 | EG: Basketball + Badminton + Dance CG: Usual Care | 3 | 90 | 10 | MPATS (WS; SC; MC; HBsalience) | No No |
| Ge, Zhong, et al. (2015) [31] | Nanchang, China (Chinese) | 36 | Severe level | 20.13 ± 1.35 | EG: Bicycle + Run CG: Usual Care | 3 | 120 | 10 | SAS-C (WS, SC, MC) | No No |
| Zheng, Yi, et al. (2019) [32] | Hunan, China (Chinese) | 99 | Mild-to-moderate level | 18–20 | EG: Basketball + Badminton + Football + Tennis CG: Usual Care | 4 | 60 | 8 | MPAI | No No |
| Xie (2019) [33] | Shangxi, China (Chinese) | 544 | Severe level | 18–22 | EG: Baduanjin CG: Usual Care | 4 | 40–60 | 8/16/24 | MPAI (WS, HBuncontrolled) | No Yes |
| Author [Reference] | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Zhu, et al. (2015) [25] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Zhang, Hu, et al. (2016) [26] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Zhou, et al. (2015) [27] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Wang, et al. (2015) [28] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Fan, Yuan, et al. (2015) [29] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Wang, Hu, et al. (2016) [30] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Ge, Zhong, et al. (2015) [31] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Zheng, Yi, et al. (2019) [32] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Xie (2019) [33] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Outcomes | Pairwise Comparison | Sample Size | Meta-Analysis | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
| Motor Skill Group | Control Group | SMD | 95% CI | p-Value | I2% | df (Q) | ||
| Total | 10 | 792 | 790 | −1.30 | −1.53 to −1.07 | 0.00 | 62% | 9 |
| WS | 9 | 755 | 741 | −1.40 | −1.73 to −1.07 | 0.00 | 81% | 8 |
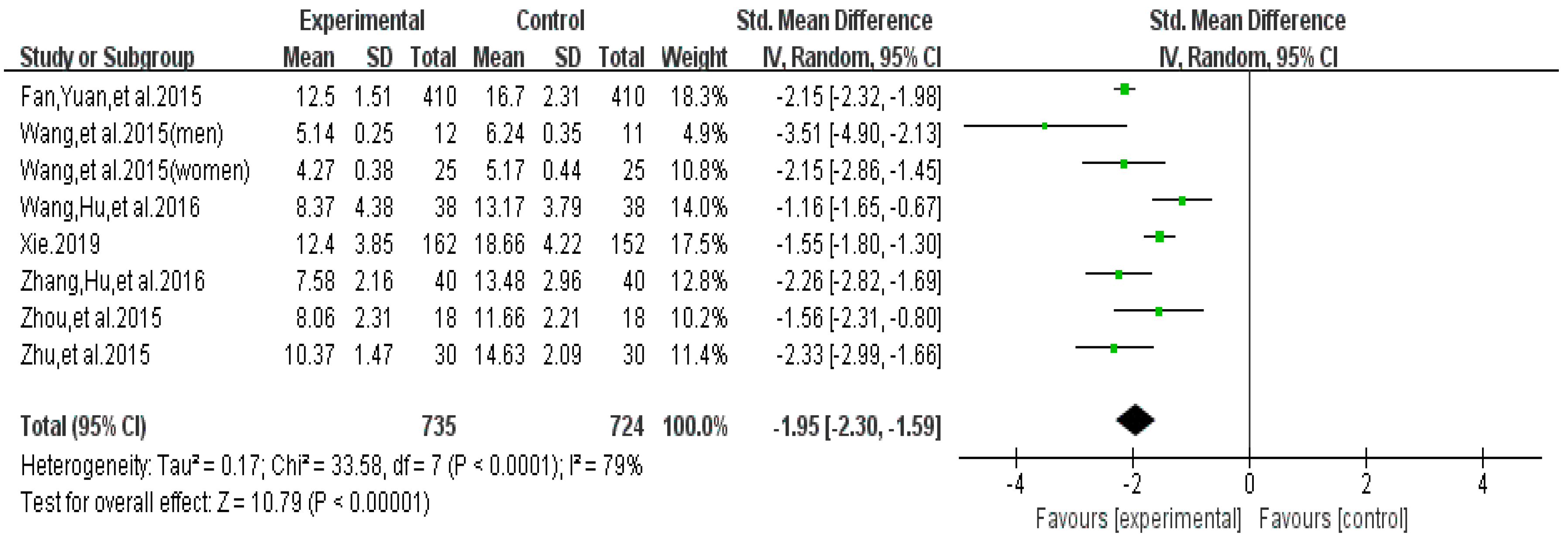
| HB | 8 | 735 | 724 | −1.95 | −2.30 to −1.59 | 0.00 | 79% | 7 |
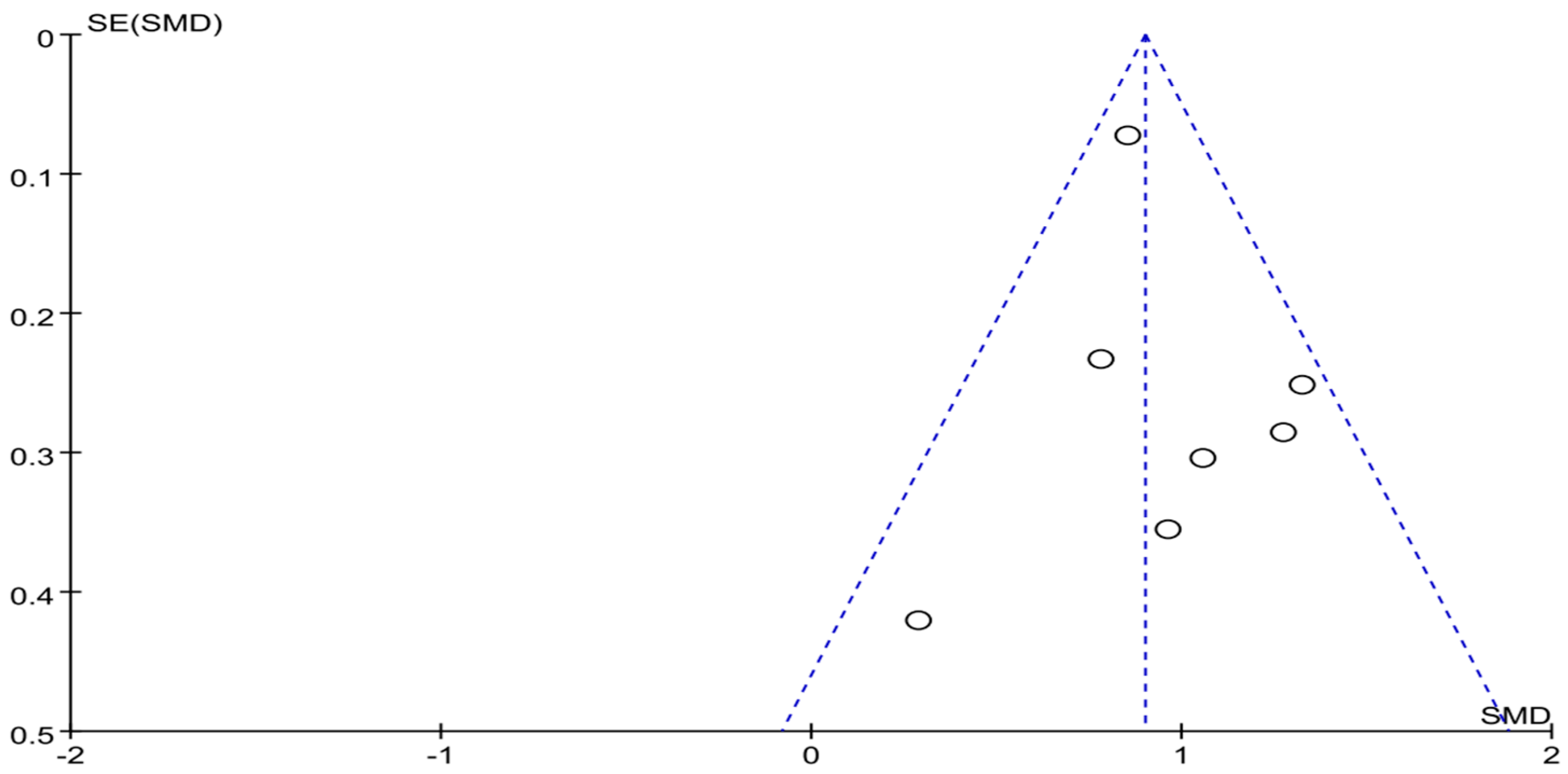
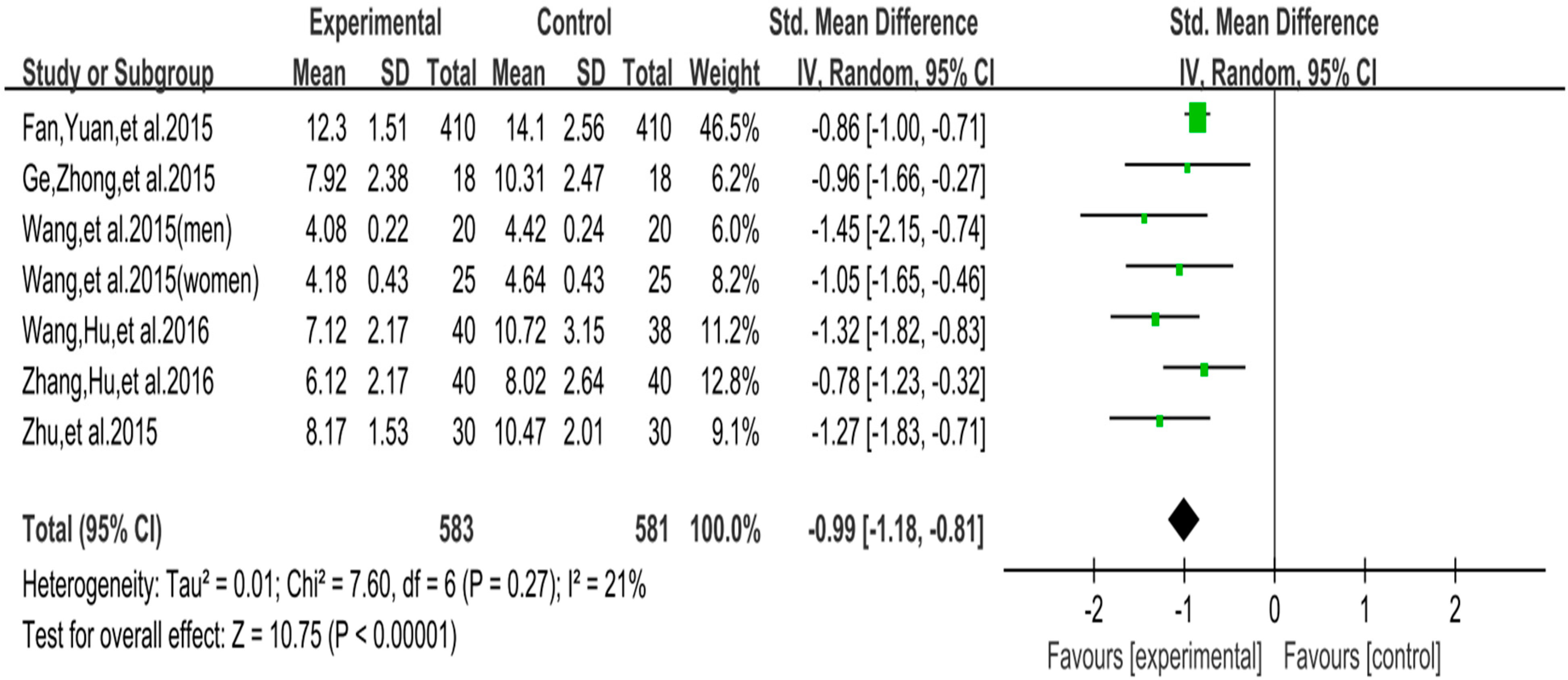
| SC | 7 | 583 | 581 | −0.99 | −1.18 to −0.81 | 0.00 | 21% | 6 |
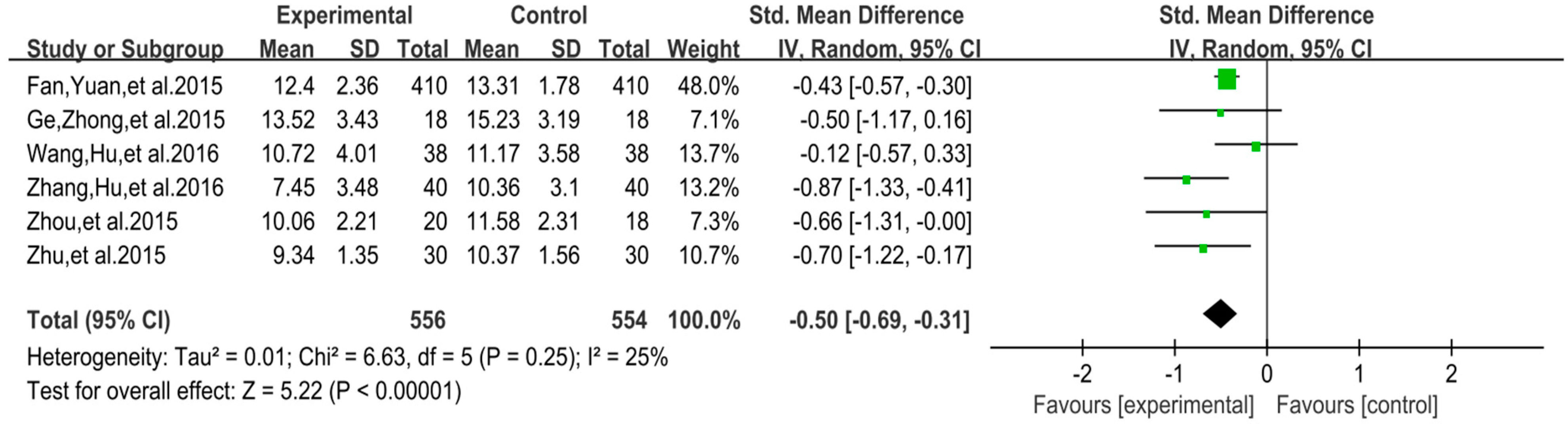
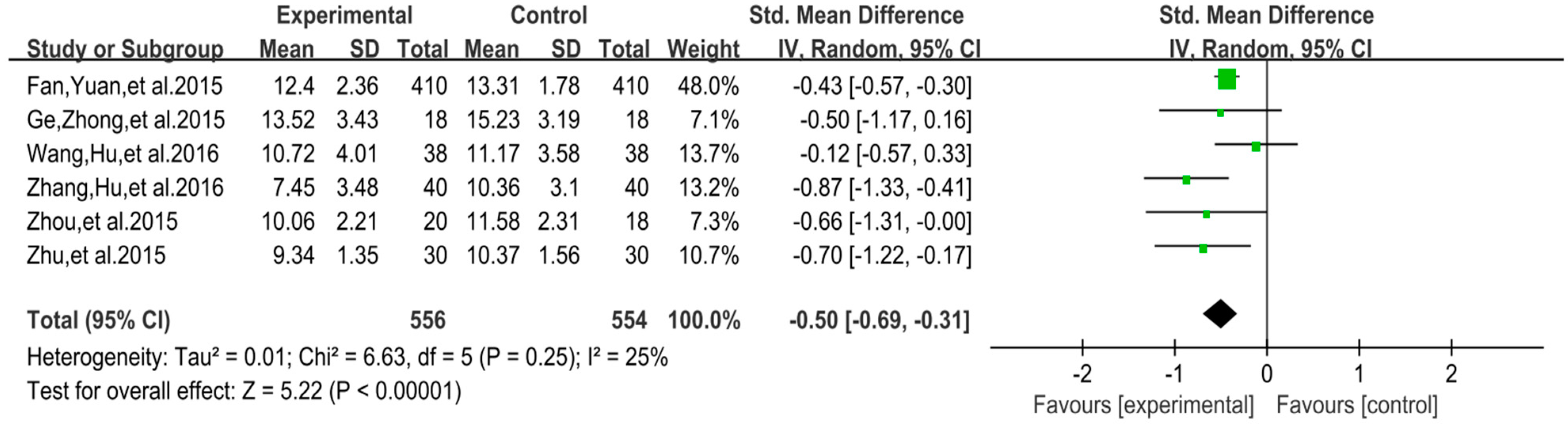
| MC | 6 | 556 | 554 | −0.50 | −0.69 to −0.31 | 0.00 | 25% | 5 |
| Outcomes | Presence of Downgrading Item of GRADE | Level of Certainty of Evidence | ||||
|---|---|---|---|---|---|---|
| Publication Bias | Inconsistency | Indirectness | Imprecision | Risk of Bias | ||
| Total | No | No | No | Yes | Yes | III (Low) |
| WS | No | No | No | Yes | Yes | III (Low) |
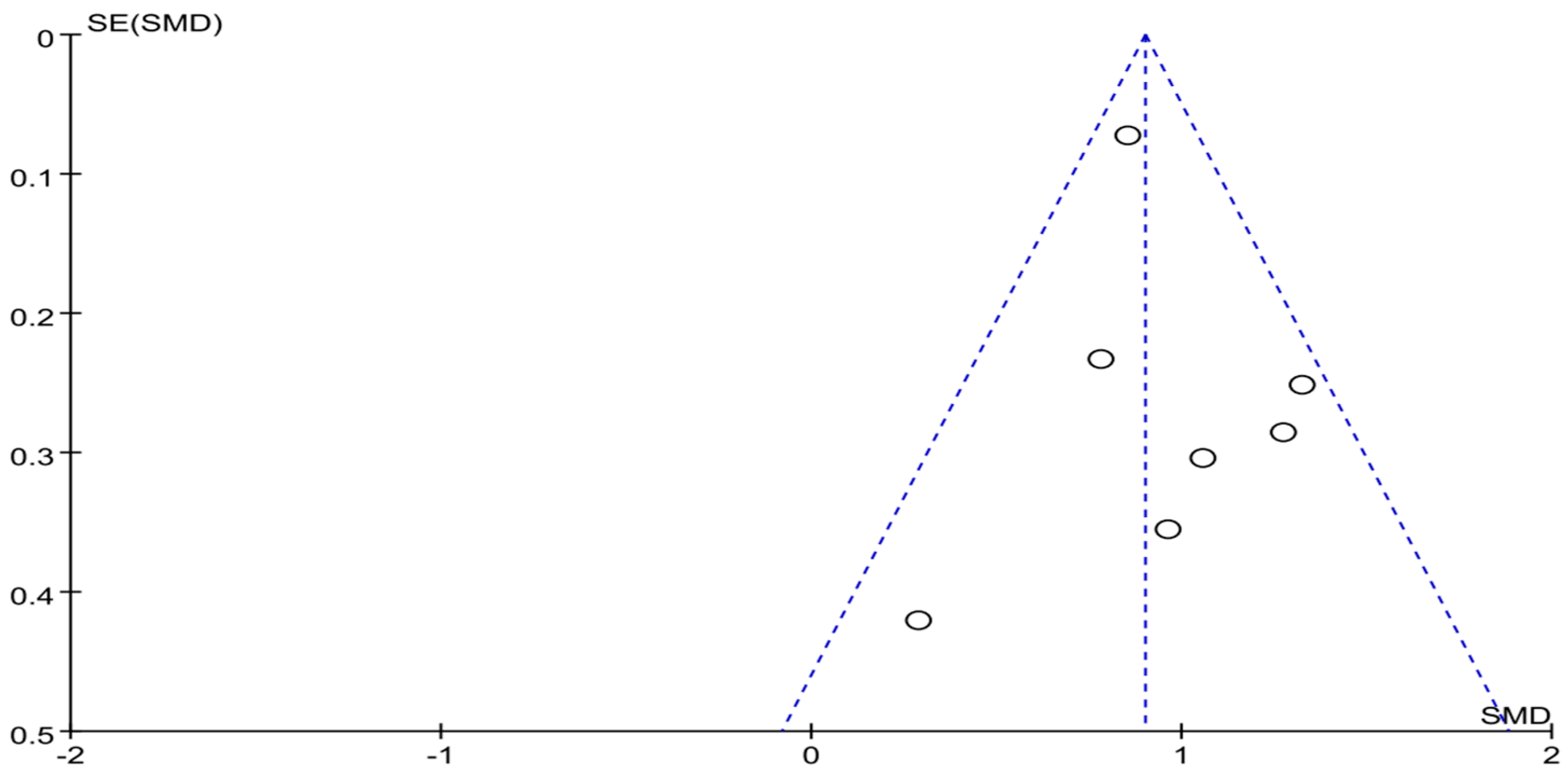
| HB | No | No | No | Yes | Yes | III (Low) |
| SC | No | No | No | No | Yes | II (Moderate) |
| MC | No | No | No | No | Yes | II (Moderate) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Xiao, T.; Yang, L.; Loprinzi, P.D. Exercise as an Alternative Approach for Treating Smartphone Addiction: A Systematic Review and Meta-Analysis of Random Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 3912. https://doi.org/10.3390/ijerph16203912
Liu S, Xiao T, Yang L, Loprinzi PD. Exercise as an Alternative Approach for Treating Smartphone Addiction: A Systematic Review and Meta-Analysis of Random Controlled Trials. International Journal of Environmental Research and Public Health. 2019; 16(20):3912. https://doi.org/10.3390/ijerph16203912
Chicago/Turabian StyleLiu, Shijie, Tao Xiao, Lin Yang, and Paul D. Loprinzi. 2019. "Exercise as an Alternative Approach for Treating Smartphone Addiction: A Systematic Review and Meta-Analysis of Random Controlled Trials" International Journal of Environmental Research and Public Health 16, no. 20: 3912. https://doi.org/10.3390/ijerph16203912
APA StyleLiu, S., Xiao, T., Yang, L., & Loprinzi, P. D. (2019). Exercise as an Alternative Approach for Treating Smartphone Addiction: A Systematic Review and Meta-Analysis of Random Controlled Trials. International Journal of Environmental Research and Public Health, 16(20), 3912. https://doi.org/10.3390/ijerph16203912