The Impacts of Prescribed Fire on PM2.5 Air Quality and Human Health: Application to Asthma-Related Emergency Room Visits in Georgia, USA


Abstract
1. Introduction
2. Materials and Methods
2.1. Burn Impact Exposure Fields
2.2. Health Impact Function
3. Results and Discussion
3.1. Total PM2.5 Concentrations and Fire Impact Exposure Fields from CMAQ and Data Fusion (DF)
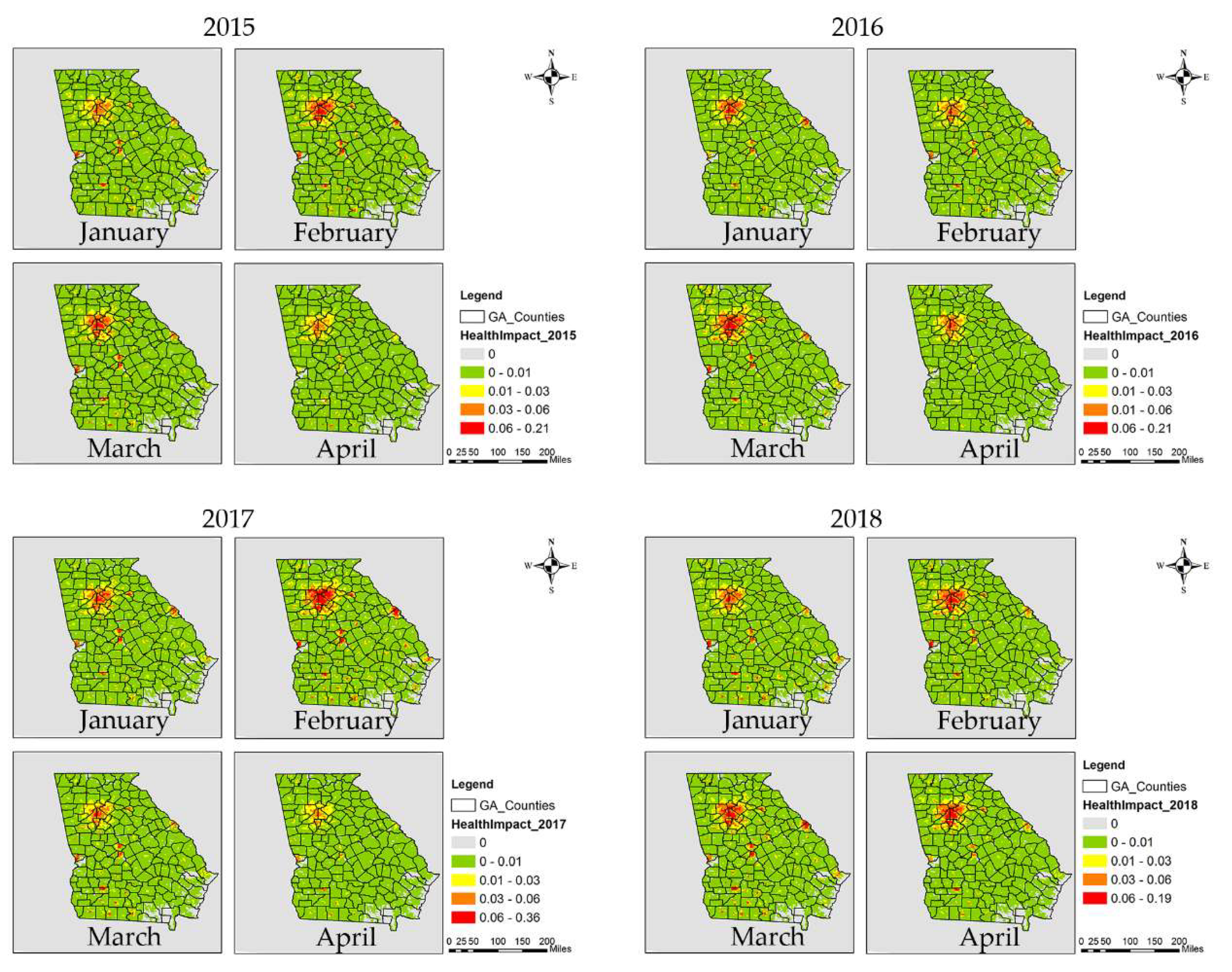
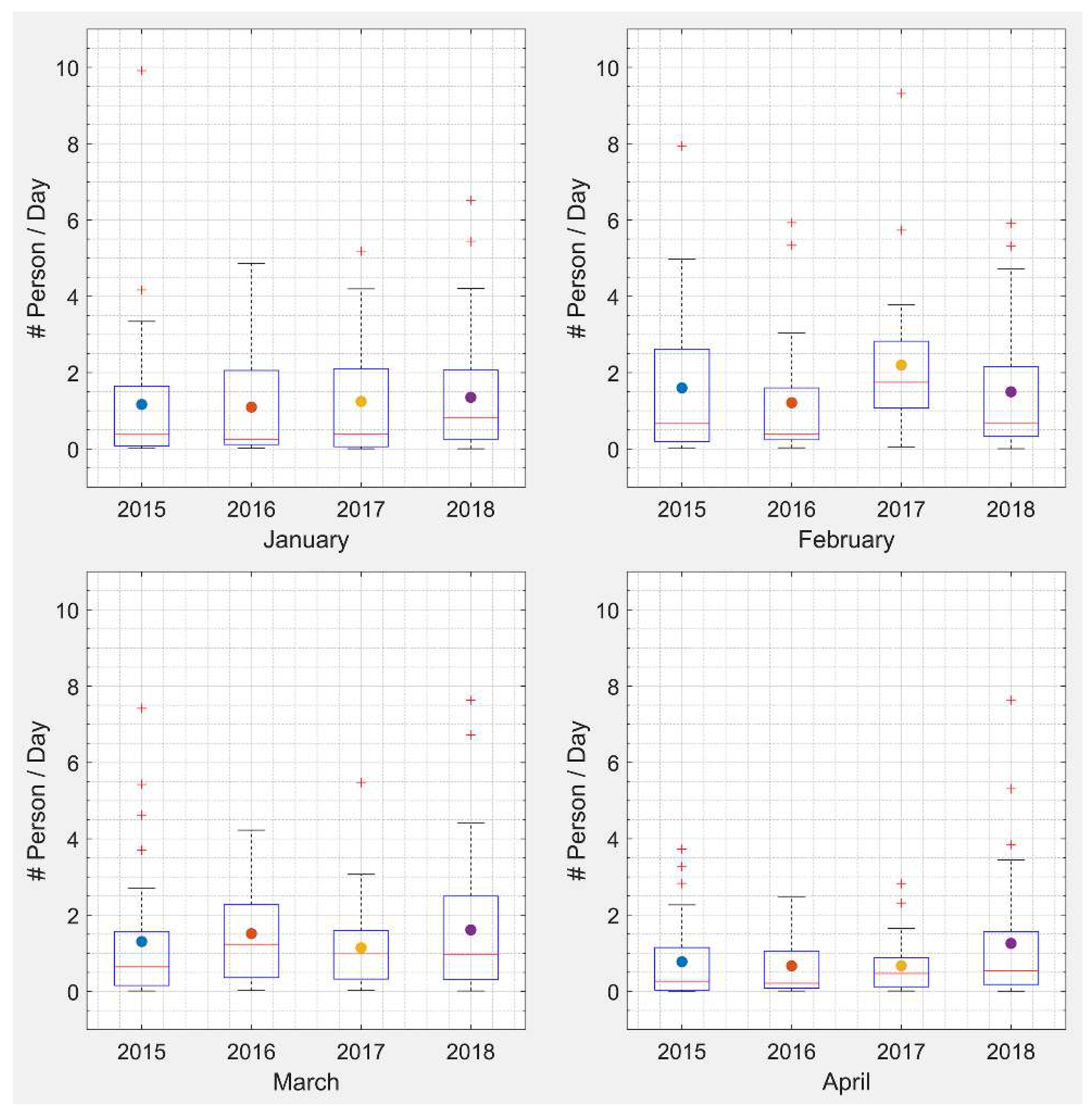
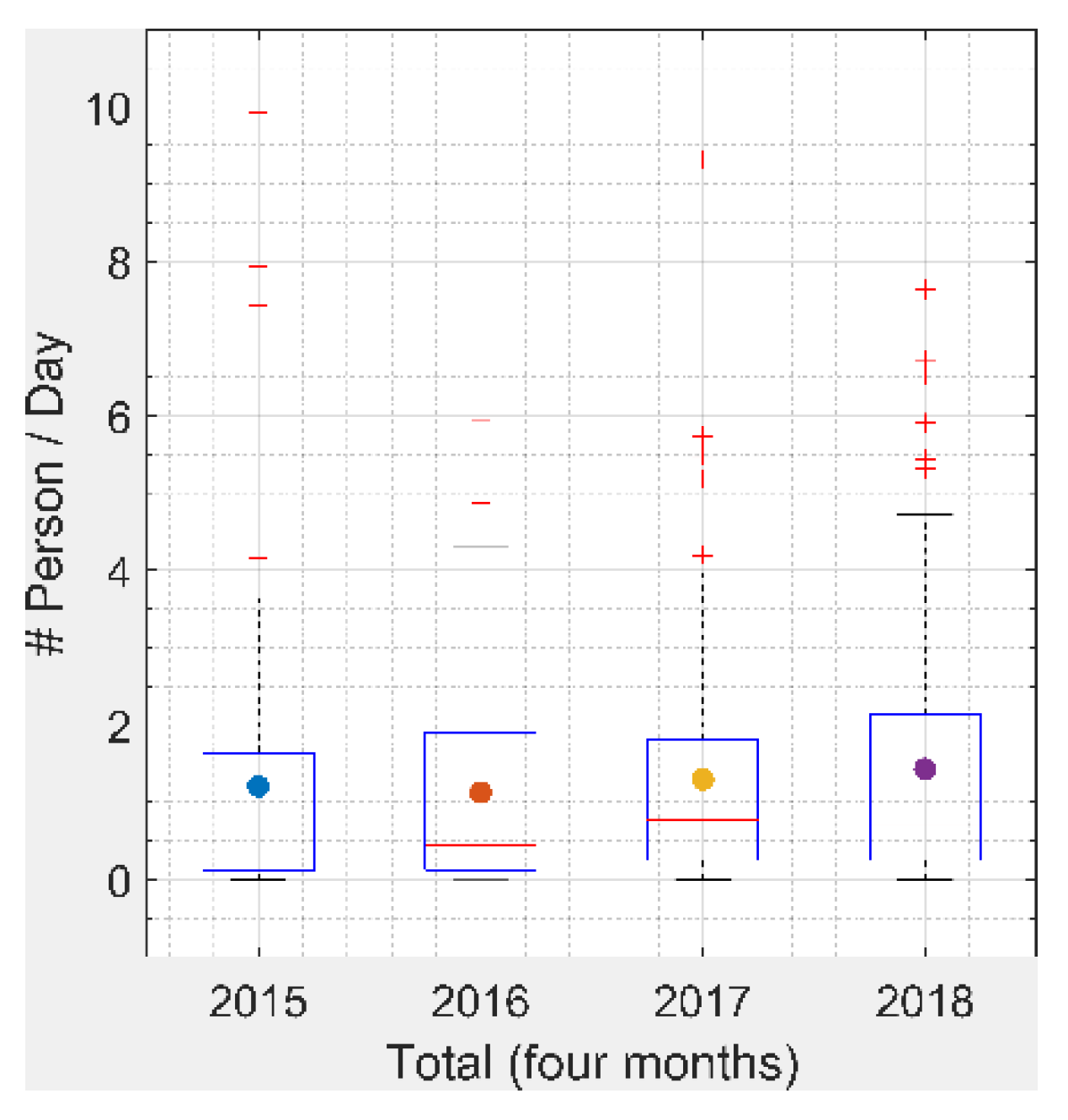
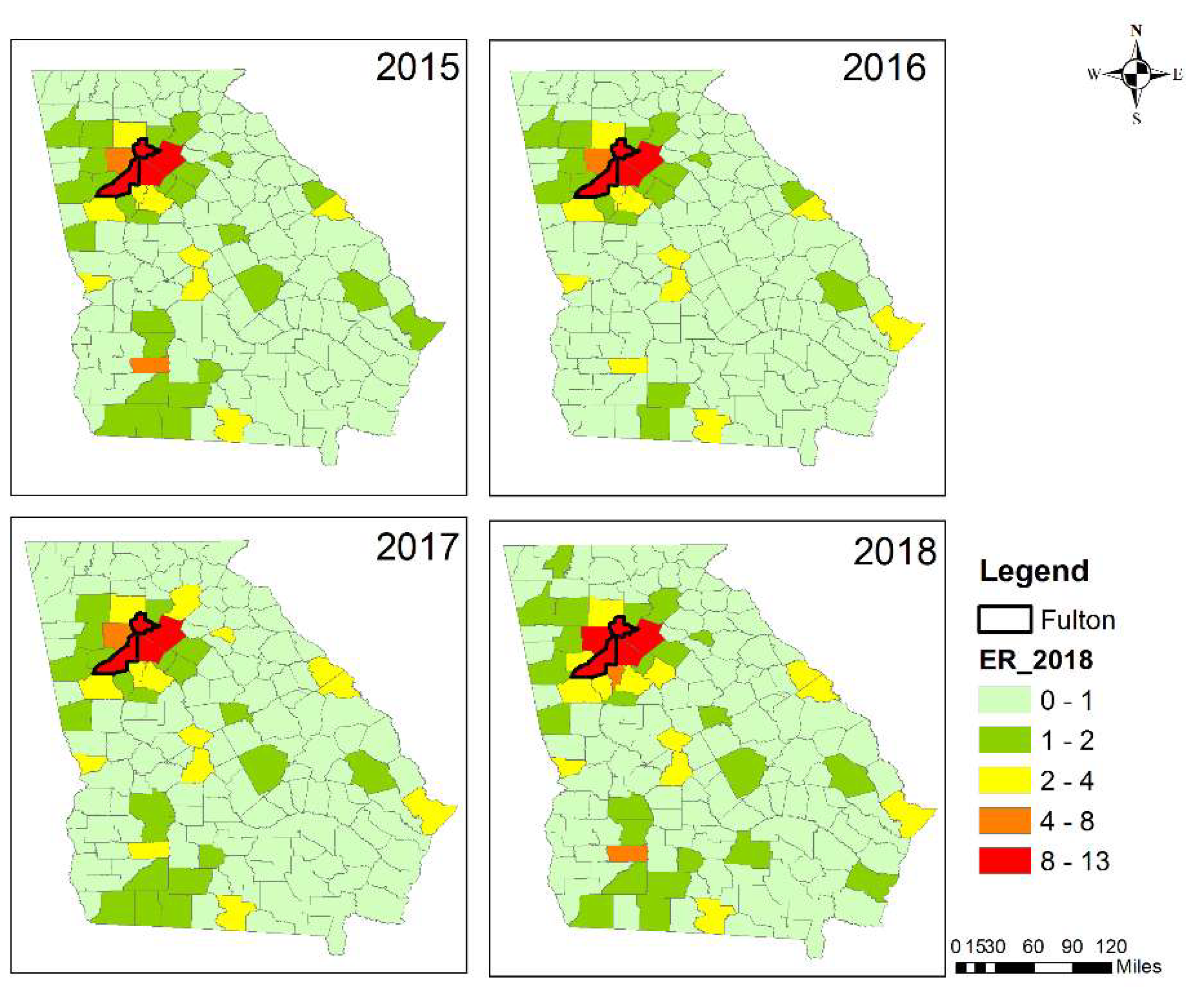
3.2. Health Impacts from Prescribed Burning
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- IARC: Outdoor Air Pollution A Leading Environmental Cause of Cancer Deaths. Available online: https://www.iarc.fr/wp-content/uploads/2018/07/pr221_E.pdf (accessed on 17 October 2013).
- Particulate Matter (PM) Basics. Available online: https://www.epa.gov/pm-pollution/particulate-matter-pm-basics (accessed on 26 June 2019).
- Dohrenwend, P.B.; Le, M.V.; Bush, J.A.; Thomas, C.F. The impact on emergency department visits for respiratory illness during the southern california wildfires. West. J. Emerg. Med. 2013, 14, 79–84. [Google Scholar] [CrossRef]
- Johnston, F.H.; Purdie, S.; Jalaludin, B.; Martin, K.L.; Henderson, S.B.; Morgan, G.G. Air pollution events from forest fires and emergency department attendances in Sydney, Australia 1996–2007: A case-crossover analysis. Environ. Health 2014, 13, 105. [Google Scholar] [CrossRef] [PubMed]
- Faustini, A.; Alessandrini, E.R.; Pey, J.; Perez, N.; Samoli, E.; Querol, X.; Cadum, E.; Perrino, C.; Ostro, B.; Ranzi, A.; et al. Short-term effects of particulate matter on mortality during forest fires in Southern Europe: Results of the MED-PARTICLES Project. Occup. Environ. Med. 2015, 72, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Linares, C.; Carmona, R.; Tobías, A.; Mirón, I.J.; Díaz, J. Influence of advections of particulate matter from biomass combustion on specific-cause mortality in Madrid in the period 2004–2009. Environ. Sci. Pollut. Res. 2015, 22, 7012–7019. [Google Scholar] [CrossRef] [PubMed]
- Rappold, A.G.; Stone, S.L.; Cascio, W.E.; Neas, L.M.; Kilaru, V.J.; Carraway, M.S.; Szykman, J.J.; Ising, A.; Cleve, W.E.; Meredith, J.T.; et al. Peat Bog Wildfire Smoke Exposure in Rural North Carolina Is Associated with Cardiopulmonary Emergency Department Visits Assessed through Syndromic Surveillance. Environ. Health Perspect. 2011, 119, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Eyamie, J.; Henderson, S.B. Evaluation of a spatially resolved forest fire smoke model for population-based epidemiologic exposure assessment. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 233–240. [Google Scholar] [CrossRef] [PubMed]
- States, U.; Lee, C.; Flickr, J. Wildfire, Wildlands, and People: Understanding and Preparing for Wildfire in the Wildland-Urban Interface; United States Department of Agriculture: Washington, DC, USA, 2013. [Google Scholar]
- US EPA 2014 National Emissions Inventory (NEI) Documentation. Available online: https://www.epa.gov/air-emissions-inventories/2014-national-emissions-inventory-nei-documentation (accessed on 21 July 2017).
- Rappold, A.G.; Reyes, J.; Pouliot, G.; Cascio, W.E.; Diaz-Sanchez, D. Community Vulnerability to Health Impacts of Wildland Fire Smoke Exposure. Environ. Sci. Technol. 2017, 51, 6674–6682. [Google Scholar] [CrossRef]
- Huang, R.; Zhang, X.; Chan, D.; Kondragunta, S.; Russell, A.G.; Odman, M.T. Burned Area Comparisons between Prescribed Burning Permits in Southeastern United States and Two Satellite-Derived Products. J. Geophys. Res. Atmos. 2018, 123, 4746–4757. [Google Scholar] [CrossRef]
- Darrow, L.A.; Klein, M.; Flanders, W.D.; Mulholland, J.A.; Tolbert, P.E.; Strickland, M.J. Air Pollution and Acute Respiratory Infections among Children 0–4 Years of Age: An 18-Year Time-Series Study. Am. J. Epidemiol. 2014, 180, 968–977. [Google Scholar] [CrossRef]
- Krall, J.R.; Mulholland, J.A.; Russell, A.G.; Balachandran, S.; Winquist, A.; Tolbert, P.E.; Waller, L.A.; Sarnat, S.E. Associations between Source-Specific Fine Particulate Matter and Emergency Department Visits for Respiratory Disease in Four U.S. Cities. Environ. Health Perspect. 2017, 125, 97–103. [Google Scholar] [CrossRef]
- Sarnat, J.A.; Marmur, A.; Klein, M.; Kim, E.; Russell, A.G.; Sarnat, S.E.; Mulholland, J.A.; Hopke, P.K.; Tolbert, P.E. Fine Particle Sources and Cardiorespiratory Morbidity: An Application of Chemical Mass Balance and Factor Analytical Source-Apportionment Methods. Environ. Health Perspect. 2008, 116, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Liu, Y.; Mulholland, J.A.; Russell, A.G.; Darrow, L.A.; Tolbert, P.E.; Strickland, M.J. Pediatric emergency department visits and ambient Air pollution in the U.S. State of Georgia: A case-crossover study. Environ. Health 2016, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Larkin, N.K.; O’Neill, S.M.; Solomon, R.; Raffuse, S.; Strand, T.; Sullivan, D.C.; Krull, C.; Rorig, M.; Peterson, J.; Ferguson, S.A. The BlueSky smoke modeling framework. Int. J. Wildl. Fire 2009, 18, 906–920. [Google Scholar] [CrossRef]
- Byun, D.; Schere, K.L. Review of the Governing Equations, Computational Algorithms, and Other Components of the Models-3 Community Multiscale Air Quality (CMAQ) Modeling System. Appl. Mech. Rev. 2006, 59, 51–77. [Google Scholar] [CrossRef]
- Dunker, A.M. The decoupled direct method for calculating sensitivity coefficients in chemical kinetics. J. Chem. Phys. 1984, 81, 2385–2393. [Google Scholar] [CrossRef]
- Friberg, M.D.; Zhai, X.; Holmes, H.A.; Chang, H.H.; Strickland, M.J.; Sarnat, S.E.; Tolbert, P.E.; Russell, A.G.; Mulholland, J.A. Method for Fusing Observational Data and Chemical Transport Model Simulations to Estimate Spatiotemporally Resolved Ambient Air Pollution. Environ. Sci. Technol. 2016, 50, 3695–3705. [Google Scholar] [CrossRef]
- Huang, R.; Zhai, X.; Ivey, C.E.; Friberg, M.D.; Hu, X.; Liu, Y.; Di, Q.; Schwartz, J.; Mulholland, J.A.; Russell, A.G. Air pollutant exposure field modeling using air quality model-data fusion methods and comparison with satellite AOD-derived fields: Application over North Carolina, USA. Air Qual. Atmos. Health 2018, 11, 11–22. [Google Scholar] [CrossRef]
- Napelenok, S.L.; Cohan, D.S.; Hu, Y.; Russell, A.G. Decoupled direct 3D sensitivity analysis for particulate matter (DDM-3D/PM). Atmos. Environ. 2006, 40, 6112–6121. [Google Scholar] [CrossRef]
- Environmental Benefits Mapping and Analysis Program—Community Edition. Available online: https://www.epa.gov/sites/production/files/2015-04/documents/benmap-ce_user_manual_appendices_march_2015.pdf (accessed on 26 June 2019).
- Alman, B.L.; Pfister, G.; Hao, H.; Stowell, J.; Hu, X.; Liu, Y.; Strickland, M.J. The association of wildfire smoke with respiratory and cardiovascular emergency department visits in Colorado in 2012: A case crossover study. Environ. Health 2016, 15, 64. [Google Scholar] [CrossRef]
- Sacks, J.D.; Lloyd, J.M.; Zhu, Y.; Anderton, J.; Jang, C.J.; Hubbell, B.; Fann, N. The Environmental Benefits Mapping and Analysis Program—Community Edition (BenMAP–CE): A tool to estimate the health and economic benefits of reducing air pollution. Environ. Model. Softw. 2018, 104, 118–129. [Google Scholar] [CrossRef]
- BenMAP Community Edition. Available online: https://www.epa.gov/benmap/benmap-community-edition (accessed on 15 February 2019).
- Williams, A.P.; Cook, B.I.; Smerdon, J.E.; Bishop, D.A.; Seager, R.; Mankin, J.S. The 2016 Southeastern U.S. Drought: An Extreme Departure from Centennial Wetting and Cooling. J. Geophys. Res. Atmos. 2017, 122, 10888–10905. [Google Scholar] [CrossRef] [PubMed]
- Ruthrof, K.X.; Fontaine, J.B.; Matusick, G.; Breshears, D.D.; Law, D.J.; Powell, S.; Hardy, G. How drought-induced forest die-off alters microclimate and increases fuel loadings and fire potentials. Int. J. Wildl. Fire 2016, 25, 819–830. [Google Scholar] [CrossRef]
- Emery, C.; Liu, Z.; Russell, A.G.; Odman, M.T.; Yarwood, G.; Kumar, N. Recommendations on statistics and benchmarks to assess photochemical model performance. J. Air Waste Manage. Assoc. 2017, 67, 582–598. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Cao, J.; Seto, E. A distributed network of low-cost continuous reading sensors to measure spatiotemporal variations of PM2.5 in Xi’an, China. Environ. Pollut. 2015, 199, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, S.; Quinn, C.; Miller-Lionberg, D.; Volckens, J. A low-cost particulate matter (PM2.5) monitor for wildland fire smoke. Atmos. Meas. Tech. 2018, 11, 1087–1097. [Google Scholar] [CrossRef]
- Zheng, T.; Bergin, M.H.; Johnson, K.K.; Tripathi, S.N.; Shirodkar, S.; Landis, M.S.; Sutaria, R.; Carlson, D.E. Field evaluation of low-cost particulate matter sensors in high and low concentration environments. Atmos. Meas. Tech. Discuss. 2018, 1–40. [Google Scholar] [CrossRef]
- Johnson, K.K.; Bergin, M.H.; Russell, A.G.; Hagler, G.S.W. Field Test of Several Low-Cost Particulate Matter Sensors in High and Low Concentration Urban Environments. Aerosol Air Qual. Res. 2018, 18, 565–578. [Google Scholar] [CrossRef]
- Davis, A.Y.; Ottmar, R.; Liu, Y.; Goodrick, S.; Achtemeier, G.; Gullett, B.; Aurell, J.; Stevens, W.; Greenwald, R.; Hu, Y.; et al. Fire emission uncertainties and their effect on smoke dispersion predictions: A case study at Eglin Air Force Base, Florida, USA. Int. J. Wildl. Fire 2015, 24, 276–285. [Google Scholar] [CrossRef]
- Garcia-Menendez, F.; Hu, Y.; Odman, M.T. Simulating smoke transport from wildland fires with a regional-scale air quality model: Sensitivity to spatiotemporal allocation of fire emissions. Sci. Total Environ. 2014, 493, 544–553. [Google Scholar] [CrossRef]
- Garcia-Menendez, F.; Hu, Y.; Odman, M.T. Simulating smoke transport from wildland fires with a regional-scale air quality model: Sensitivity to uncertain wind fields. J. Geophys. Res. Atmos. 2013, 118, 6493–6504. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PM2.5 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|
| Observation | 8.6 ± 4.3 | 8.3 ± 4.4 | 8.8 ± 5.3 | 8.7 ± 5 |
| CMAQ * | 6.6 ± 4.5 | 6.1 ± 4.3 | 6.3 ± 4 | 6.2 ± 4 |
| Burn impact (CMAQ) | 0.83 ± 2.82 | 0.76 ± 2.96 | 0.87 ± 1.62 | 0.97 ± 2.26 |
| Data fusion | 8.4 ± 3.8 | 8 ± 3.7 | 8.7 ± 4.6 | 8.2 ± 4.2 |
| Burn impact (data fusion) | 0.91 ± 1.97 | 0.86 ± 1.77 | 1.06 ± 1.77 | 1.24 ± 2.42 |
| PM2.5 | NRMSE | NME | ||||||
|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2015 | 2016 | 2017 | 2018 | |
| CMAQ | 0.57 | 0.64 | 0.59 | 0.62 | 0.23 | 0.26 | 0.28 | 0.28 |
| DF | 0.23 | 0.27 | 0.24 | 0.24 | 0.02 | 0.04 | 0.01 | 0.05 |
| DF (withholding) * | 0.40 | 0.40 | 0.42 | 0.36 | 0.01 | 0.04 | 0.01 | 0.05 |
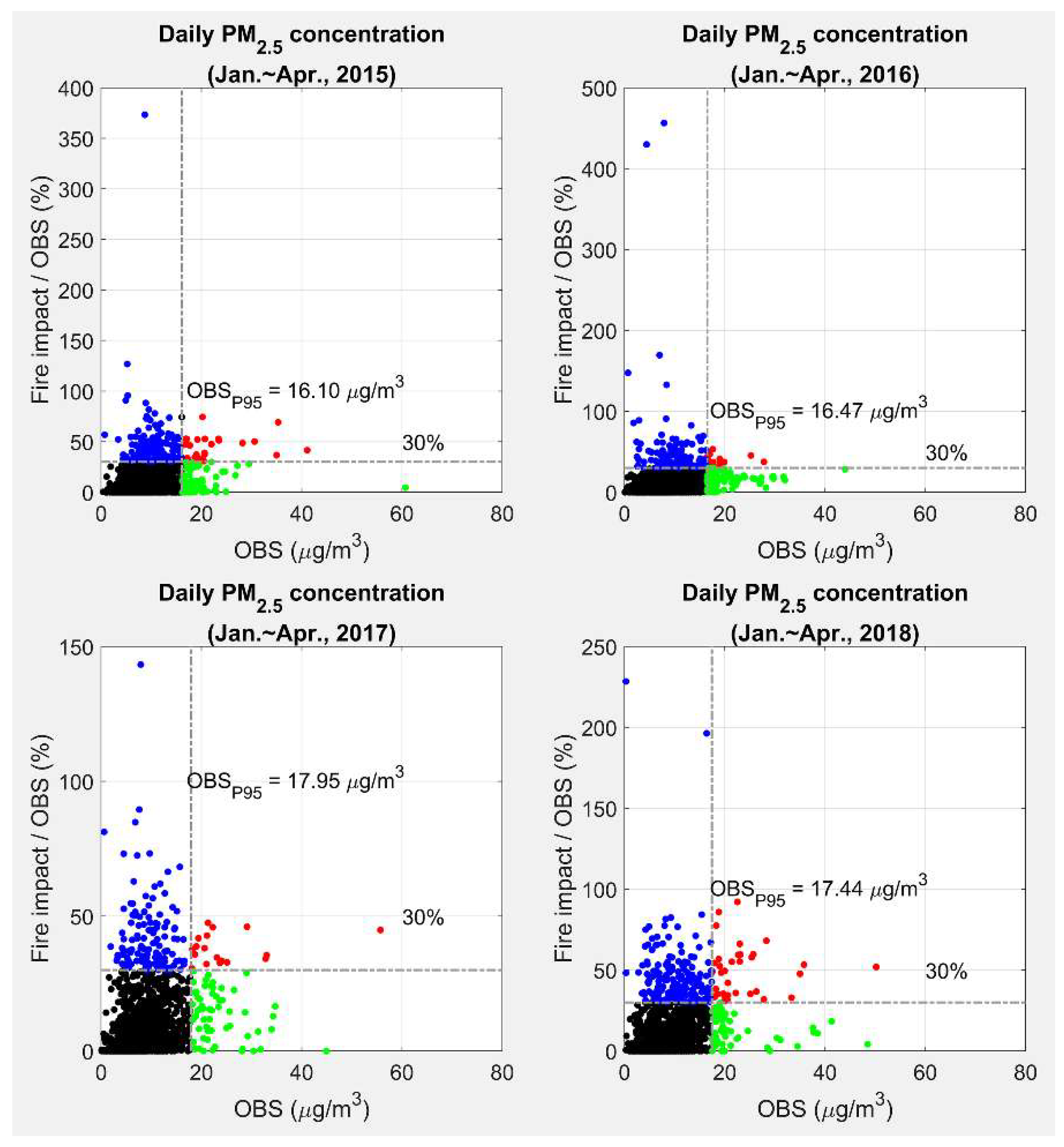
| Days | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|
| Total | 2069 | 2136 | 1565 | 1762 |
| High fire impact/High PM2.5 (Red) | 27 | 14 | 18 | 36 |
| High fire impact/Low PM2.5 (Blue) | 141 | 124 | 133 | 192 |
| Low fire impact/High PM2.5 (Green) | 75 | 93 | 60 | 52 |
| Low fire impact/Low PM2.5 (Black) | 1826 | 1905 | 1354 | 1482 |
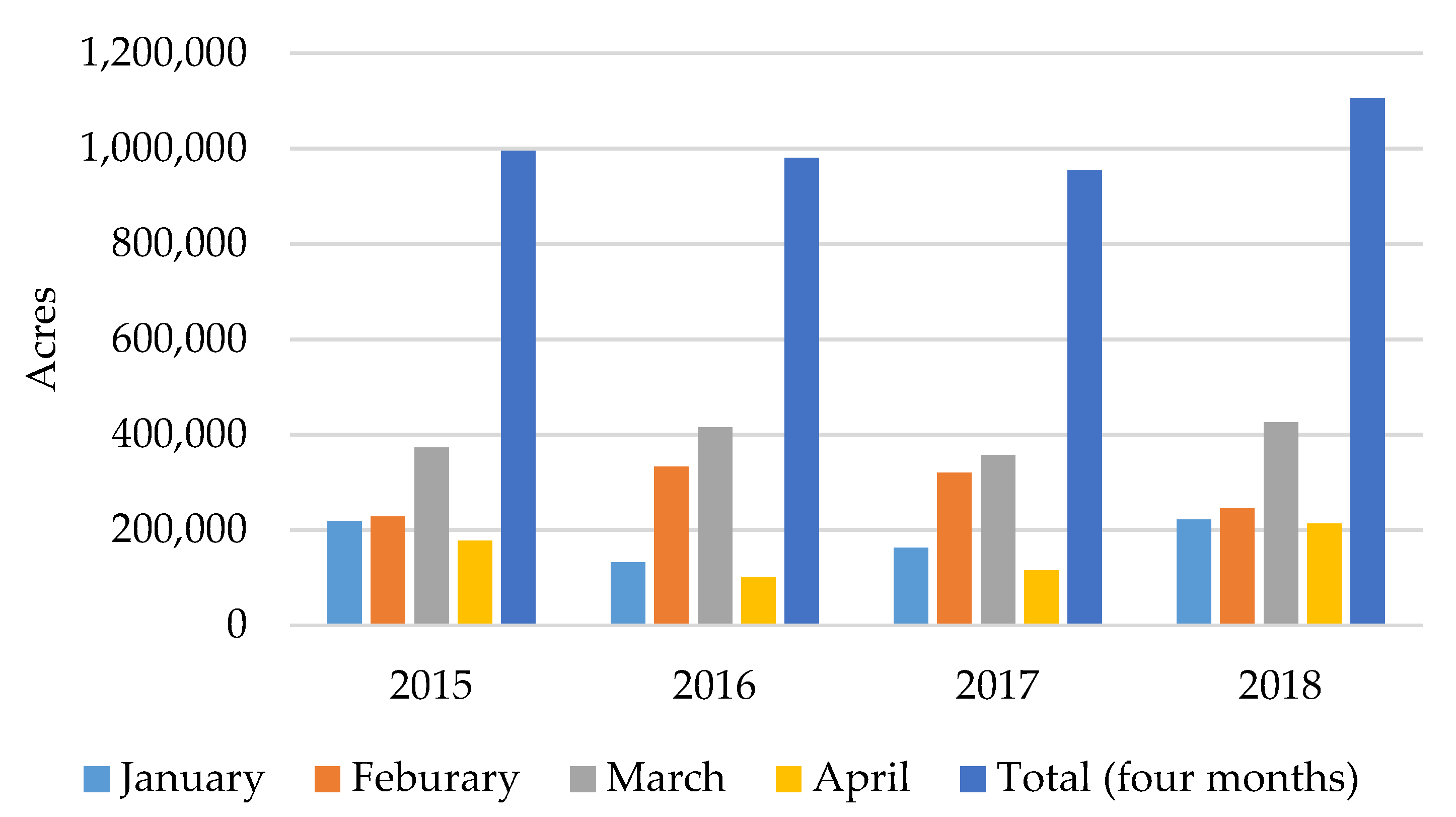
| Year | January | February | March | April | Total |
|---|---|---|---|---|---|
| 2015 | 36 ± 23 | 45 ± 27 | 41 ± 25 | 23 ± 16 | 145 ± 46 |
| 2016 | 34 ± 21 | 35 ± 20 | 47 ± 22 | 20 ± 14 | 136 ± 39 |
| 2017 | 39 ± 21 | 62 ± 30 | 35 ± 19 | 20 ± 11 | 156 ± 43 |
| 2018 | 42 ± 24 | 42 ± 23 | 50 ± 29 | 38 ± 26 | 171 ± 51 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, R.; Hu, Y.; Russell, A.G.; Mulholland, J.A.; Odman, M.T. The Impacts of Prescribed Fire on PM2.5 Air Quality and Human Health: Application to Asthma-Related Emergency Room Visits in Georgia, USA. Int. J. Environ. Res. Public Health 2019, 16, 2312. https://doi.org/10.3390/ijerph16132312
Huang R, Hu Y, Russell AG, Mulholland JA, Odman MT. The Impacts of Prescribed Fire on PM2.5 Air Quality and Human Health: Application to Asthma-Related Emergency Room Visits in Georgia, USA. International Journal of Environmental Research and Public Health. 2019; 16(13):2312. https://doi.org/10.3390/ijerph16132312
Chicago/Turabian StyleHuang, Ran, Yongtao Hu, Armistead G. Russell, James A. Mulholland, and M. Talat Odman. 2019. "The Impacts of Prescribed Fire on PM2.5 Air Quality and Human Health: Application to Asthma-Related Emergency Room Visits in Georgia, USA" International Journal of Environmental Research and Public Health 16, no. 13: 2312. https://doi.org/10.3390/ijerph16132312
APA StyleHuang, R., Hu, Y., Russell, A. G., Mulholland, J. A., & Odman, M. T. (2019). The Impacts of Prescribed Fire on PM2.5 Air Quality and Human Health: Application to Asthma-Related Emergency Room Visits in Georgia, USA. International Journal of Environmental Research and Public Health, 16(13), 2312. https://doi.org/10.3390/ijerph16132312