A Systematic Review of Polyvictimization among Children with Attention Deficit Hyperactivity or Autism Spectrum Disorder


Abstract
:1. Rationale
1.1. Vulnerability to Different Forms of Victimization
1.2. Polyvictimization
1.3. Study Design and the Use of Different Informants
2. Objectives
3. Methods
3.1. Protocol and Registration
3.2. Eligibility Criteria
3.2.1. Inclusion Criteria
3.2.2. Exclusion Criteria
3.3. Information Sources and Search Strategy
3.4. Study Selection and Data Collection Process
3.5. Data Items
3.6. Quality Assessment
4. Results
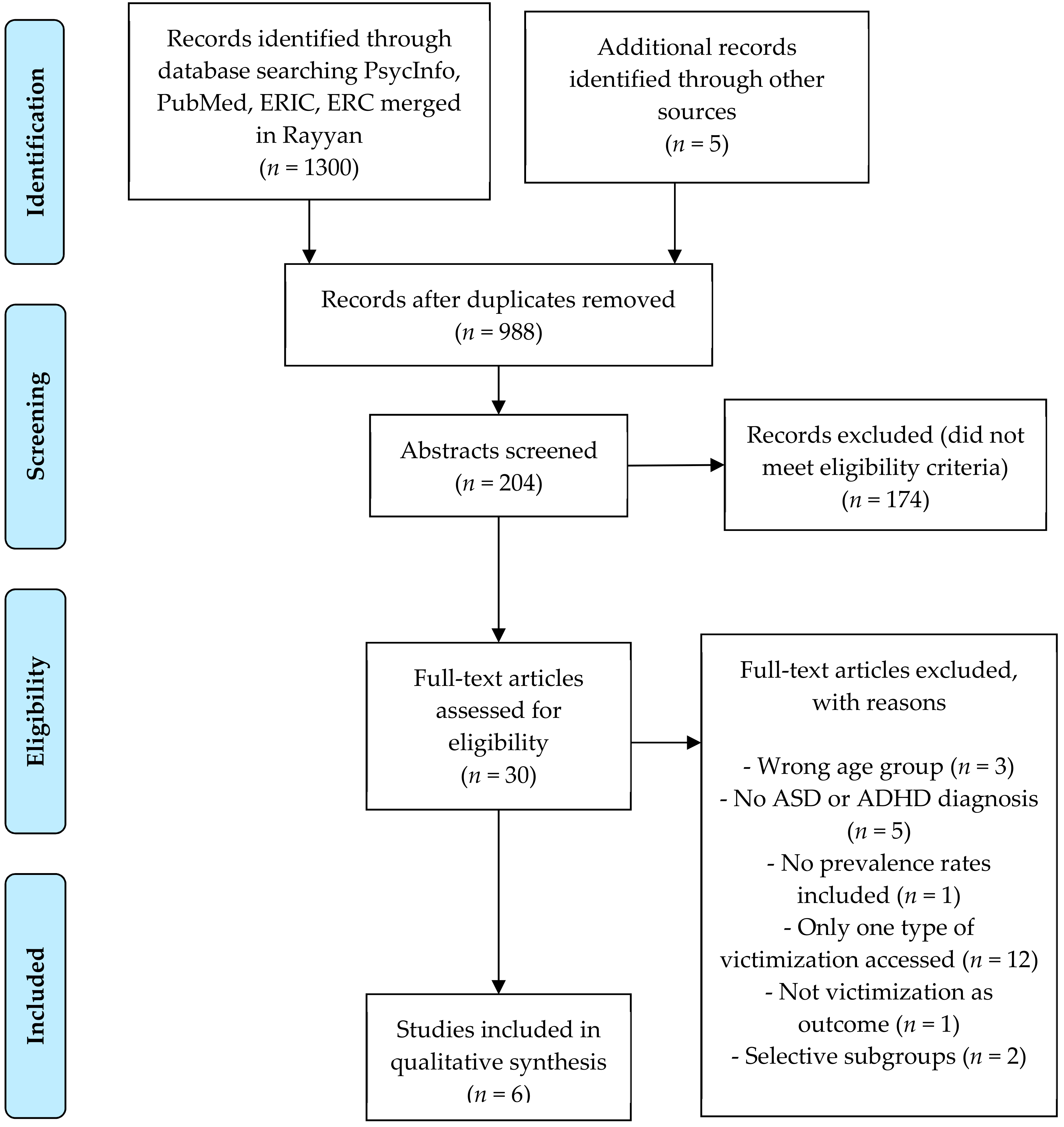
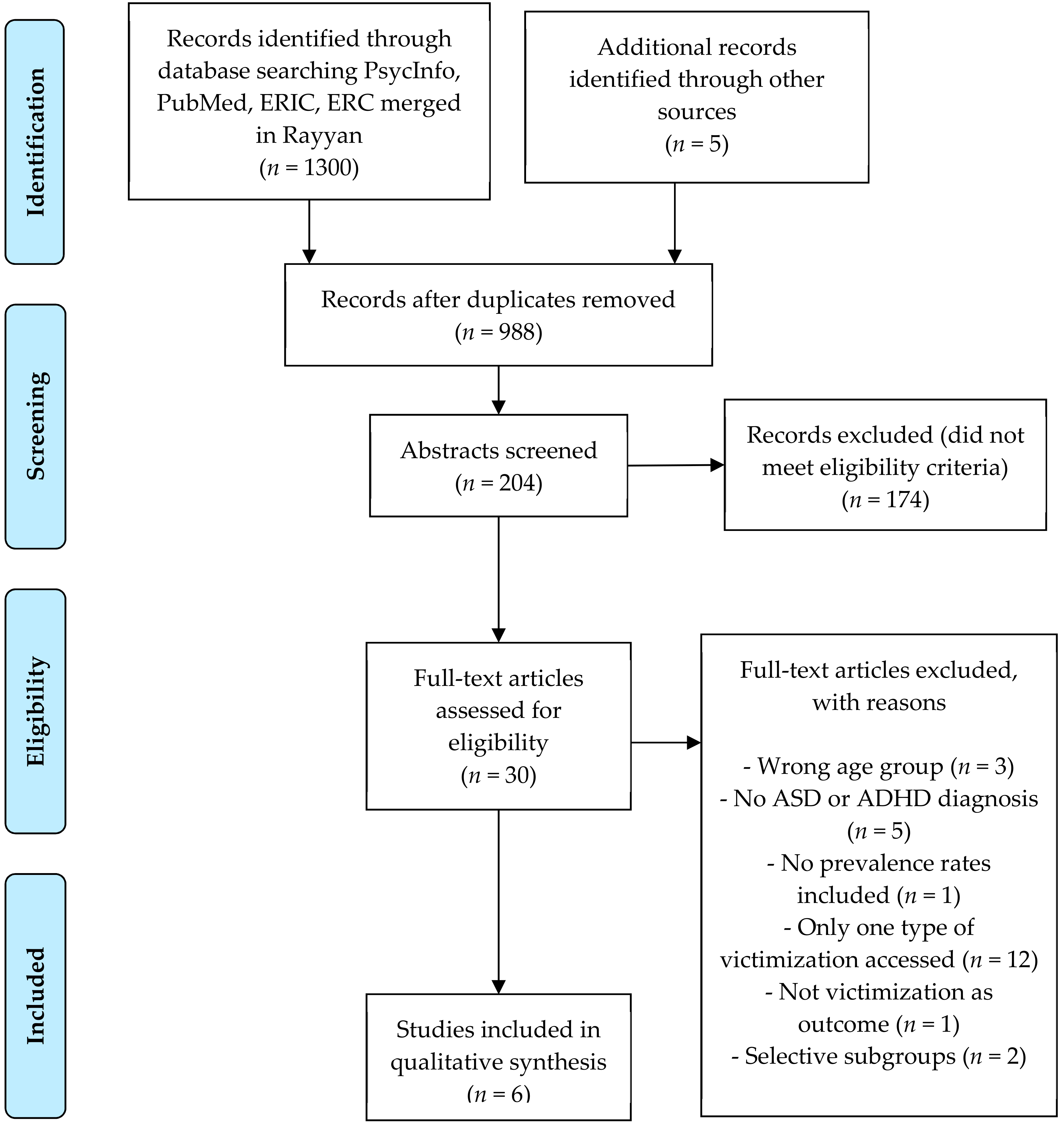
4.1. Study Selection
4.2. Study Characteristics
4.2.1. Study Settings
4.2.2. Study Design
4.2.3. Place of Sample Recruitment and Informants
4.2.4. Types of Diagnosis Examined
4.2.5. Measures Used for Assessment of Polyvictimization
4.2.6. Types of Victimization Examined
4.3. Risk of Bias Within Studies
4.4. Results of Individual Studies and Synthesis of Results
4.4.1. Prevalence of Specific Forms of Victimization
4.4.1.1 Conventional Crime
4.4.1.2. Child Maltreatment
4.4.1.3. Peer and Sibling Victimization
4.4.1.4. Sexual Victimization
4.4.1.5. Witnessing and Indirect Victimization
4.4.1.6. Polyvictimization
5. Discussion
5.1. Polyvictimization
5.2. Different Forms of Victimization
5.3. Type of Respondents
6. Limitations
7. Conclusions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| PubMed (2019-03-04) | ||
|---|---|---|
| Search | Search terms | Number of hits |
| #1 Children and Adolescents | “Child”[Mesh] OR “Adolescent”[Mesh] OR “Minors”[Mesh] OR “Puberty”[Mesh] OR “Pediatrics”[Mesh] OR child*[Title/Abstract] OR Pediatric*[Title/Abstract] OR Paediatric*[Title/Abstract] OR adolescen*[Title/Abstract] OR teen*[Title/Abstract] OR young*[Title/Abstract] OR youth*[Title/abstract] OR puberty[Title/Abstract] OR minor*[Title/Abstract] OR juvenile*[Title/Abstract] OR school-age*[Title/Abstract] OR boy*[Title/Abstract] OR girl*[Title/Abstract] | 4,028,357 |
| #2 ASD or ADHD | “Neurodevelopmental Disorders”[Mesh]) OR Neurodevelopmental Disorder*[Title/Abstract] OR ADHD[Title/Abstract] OR Attention deficit disorder*[Title/Abstract] OR Autis*[Title/Abstract] OR ASD[Title/Abstract] OR Asperger*[Title/Abstract] | 198,221 |
| #3 Polyvictimization/ victimization | “Crime Victims” [Mesh] OR “Exposure to violence” [Mesh] OR victim*[Title/Abstract] OR Exposure to violence*[Title/Abstract] | 54,149 |
| #4 | #1 AND #2 AND #3 | 752 |
| PsycInfo (2019-03-01) | ||
| Search | Search terms | Number of hits |
| #1 Children and Adolescents | MAINSUBJECT.EXACT(“Elementary School Students”) OR MAINSUBJECT.EXACT(“Primary School Students”) OR MAINSUBJECT.EXACT(“Junior High School Students”) OR MAINSUBJECT.EXACT(“Middle School Students”) OR MAINSUBJECT.EXACT(“High School Students”) OR MAINSUBJECT.EXACT(“Kindergarten Students”) OR MAINSUBJECT.EXACT(“Preschool Students”) OR child* OR adolescen* OR youth OR teen* OR minor* OR young* OR juvenile OR “Elementary School” OR “Primary School” OR “Junior High School” OR “Middle School” OR “High School” OR Kindergarten OR Preschool OR “secondary school” | 1,732,513 |
| #2 ASD or ADHD | MAINSUBJECT.EXACT(“Attention Deficit Disorder with Hyperactivity”) OR MAINSUBJECT.EXACT(“Neurodevelopmental Disorders”) OR MAINSUBJECT.EXACT(“Autism Spectrum Disorders”) OR autis* OR adhd OR “Attention Deficit Disorder with Hyperactivity” OR “neurodevelopmental disorder*” OR Asperger OR “Neuropsychiatric disorder*” | 134,188 |
| #3 Polyvictimization/ victimization | Polyvictimization OR “poly victimization” OR polyvictimisation OR “poly victimisation” OR MAINSUBJECT.EXACT(“Victimization”) OR MAINSUBJECT.EXACT(“Exposure to Violence”) OR MAINSUBJECT.EXACT(“crime victims”) OR “exposure to violence” OR victimization OR victimisation OR “crime victims” OR victim* | 29,595 |
| #4 | #1 AND #2 AND #3 | 346 |
| ERIC via EBSCO (2019-03-01) | ||
| Search | Search terms | Number of hits |
| #1 Children and Adolescents | DE “Children” OR DE “Youth” OR DE “Adolescents” OR child* OR youth OR minor* OR teen* OR young* OR adolescen* OR DE “Elementary School Students” OR DE “Middle School Students” OR DE “Students” OR DE “Junior High School Students” OR DE “High School Students” OR DE “Preschool Children” OR DE “Secondary School Students” OR DE “Kindergarten” OR preschool* OR “Elementary School*” OR “Middle School*” OR “primary school” OR “high school” OR “secondary school” OR kindergarten | 667,578 |
| #2 ASD or ADHD | DE “Attention Deficit Hyperactivity Disorder” OR DE “Pervasive Developmental Disorders” OR DE “Autism” OR DE “Asperger Syndrome” OR “Attention Deficit Hyperactivity Disorder*” OR “Pervasive Developmental Disorder*” OR autis* OR adhd OR “neurodevelopmental disorder*” OR “neuropsychiatric disorder*” OR Asperger* | 30,406 |
| #3 Polyvictimization/ victimization | DE “Victims of Crime” OR DE “Victims” OR polyvictimization OR “poly victimization” OR polyvictimisation OR “poly victimisation” OR victim* | 9467 |
| #4 | #1 AND #2 AND #3 | 66 |
| ERC via EBESCO (2019-03-01) | ||
| Search | Search terms | Number of hits |
| #1 Children or Adolescents | DE “Children” OR DE “preschool children” OR DE “Kindergarten children” OR DE “Adolescence” OR DE “Teenagers” OR DE “Young adults” OR DE “Youth” DE “School children” OR DE “MIDDLE school students” OR DE “Students” OR DE “JUNIOR high school students” OR DE “High school students” OR DE “Secondary school students” de “Kindergarten children” OR DE “Elementary schools” OR DE “Primary schools” OR child* OR youth OR minor* OR teen* OR young* OR adolescen* OR preschool OR “Elementary School” OR “Middle School” OR “primary school” OR “high school” OR “secondary school” OR kindergarten | 1,128,748 |
| #2 ASD or ADHD | DE “Autism” OR DE “Autism spectrum disorders” OR DE “Autism in adolescence” OR DE “Autism in children” OR DE “Attention-deficit hyperactivity disorder” OR DE “Pervasive developmental disorder not otherwise specified” OR autis* OR adhd OR “attention deficit hyperactivity disorders” OR “neurodevelopmental disorder*” OR “neuropsychiatric disorder*” OR “Pervasive Developmental Disorder*” | 55,886 |
| #3 Polyvictimization/ victimization | polyvictimization OR “poly victimization” OR polyvictimisation OR “poly victimisation” OR victim* | 22,884 |
| #4 | #1 AND #2 AND #3 | 136 |
| Study | Ethics Approval | Criteria | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 a | 2 a | 3 a | 4 a | 8 a | 9 a | 10 a | 11 a | 12 a | 13 a | 14 a | Overall Score b | Average Score c | ||
| Aguado-Gracia et al. 2018 | ? | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 19 | 0.86 |
| Chan et al. 2018 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 1.00 |
| Greger et al. 2015 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 1.00 |
| Paul et al. 2018 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 18 | 0.82 |
| Pfeffer 2016 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 17 | 0.77 |
| Turner et al. 2011 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 1.00 |
References
- May, T.; Sciberras, E.; Brignell, A.; Williams, K. Autism spectrum disorder: Updated prevalence and comparison of two birth cohorts in a nationally representative australian sample. BMJ Open 2017, 7, e015549. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef] [PubMed]
- Association A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Mayes, S.D.; Calhoun, S.L.; Mayes, R.D.; Molitoris, S. Autism and adhd: Overlapping and discriminating symptoms. Res. Autism Spectr. Disord. 2012, 6, 277–285. [Google Scholar] [CrossRef]
- Adams, R.; Taylor, J.; Duncan, A.; Bishop, S. Peer victimization and educational outcomes in mainstreamed adolescents with autism spectrum disorder (ASD). J. Autism Dev. Disord. 2016, 46, 3557–3566. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Mehari, K.R.; Langberg, J.M.; Evans, S.W. Rates of peer victimization in young adolescents with adhd and associations with internalizing symptoms and self-esteem. Eur. Child Adolesc. Psychiatry 2017, 26, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Turner, H.A.; Vanderminden, J.; Finkelhor, D.; Hamby, S.; Shattuck, A. Disability and victimization in a national sample of children and youth. Child Maltreatment 2011, 16, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A.; Hamby, S.L. Measuring poly-victimization using the juvenile victimization questionnaire. Child Abuse Negl. 2005, 29, 1297–1312. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, D.; Turner, H.; Hamby, S.L.; Ormrod, R. Polyvictimization: Children’s exposure to multiple types of violence, crime, and abuse. Available online: https://www.ojjdp.gov/publications/PubAbstract.asp?pubi=257485 (accessed on 27 June 2019).
- Turner, H.A.; Shattuck, A.; Finkelhor, D.; Hamby, S. Polyvictimization and youth violence exposure across contexts. J. Adolesc. Health 2016, 58, 208–214. [Google Scholar] [CrossRef]
- Olweus, D. Bullying in School: What We Know and What We Can Do; Blackwell Publishers: Oxford, UK, 1993. [Google Scholar]
- Beckman, L.; Hagquist, C.; Hellström, L. Does the association with psychosomatic health problems differ between cyberbullying and traditional bullying? Emot. Behav. Diffic. 2012, 17, 421–434. [Google Scholar] [CrossRef]
- Maiano, C.; Normand, C.L.; Salvas, M.C.; Moullec, G.; Aimé, A. Prevalence of school bullying among youth with autism spectrum disorders: A systematic review and meta-analysis. Autism Res. 2016, 9, 601–615. [Google Scholar] [CrossRef]
- Little, L. Middle-class mothers’perceptions of peer and sibling victimization among children with asperger’s syndrome and nonverbal learning disorders. Issues Compr. Pediatr. Nurs. 2002, 25, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, J.H.; Cappadocia, M.C.; Bebko, J.M.; Pepler, D.J.; Weiss, J.A. Shedding light on a pervasive problem: A review of research on bullying experiences among children with autism spectrum disorders. J. Autism Dev. Disord. 2014, 44, 1520–1534. [Google Scholar] [CrossRef] [PubMed]
- Zablotsky, B.; Bradshaw, C.P.; Anderson, C.; Law, P. Involvement in bullying among children with autism spectrum disorders: Parents’ perspectives on the influence of school factors. Behav. Disord. 2012, 37, 179–191. [Google Scholar] [CrossRef]
- Heiman, T.; Olenik-Shemesh, D. Cyberbullying experience and gender differences among adolescents in different educational settings. J. Learn. Disabil. 2015, 48, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Beckman, L.; Hellström, L.; von Kobyletzki, L. Cyber bullying among children with neurodevelopmental disorders: A systematic review. Scand. J. Psychol. 2019. [Google Scholar] [CrossRef]
- Kok, F.M.; Groen, Y.; Fuermaier, A.B.; Tucha, O. Problematic peer functioning in girls with adhd: A systematic literature review. PLoS ONE 2016, 11, e0165119. [Google Scholar] [CrossRef]
- Lucas, S.; Jernbro, C.; Tindberg, Y.; Janson, S. Bully, bullied and abused. Associations between violence at home and bullying in childhood. Scand. J. Public Health 2016, 44, 27–35. [Google Scholar] [CrossRef]
- WHO. Health Topics: Child Maltreatment. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment. (accessed on 17 May 2019).
- Hershkowitz, I.; Lamb, M.E.; Horowitz, D. Victimization of children with disabilities. Am. J. Orthopsychiatr. 2007, 77, 629–635. [Google Scholar] [CrossRef]
- Ethier, L.S.; Lemelin, J.P.; Lacharite, C. A longitudinal study of the effects of chronic maltreatment on children’s behavioral and emotional problems. Child Abuse Negl. 2004, 28, 1265–1278. [Google Scholar] [CrossRef]
- McDonnell, C.G.; Boan, A.D.; Bradley, C.C.; Seay, K.D.; Charles, J.M.; Carpenter, L.A. Child maltreatment in autism spectrum disorder and intellectual disability: Results from a population-based sample. J. Child Psychol. Psychiatr. 2018, 60, 576–584. [Google Scholar] [CrossRef]
- Guendelman, M.D.; Owens, E.B.; Galan, C.; Gard, A.; Hinshaw, S.P. Early-adult correlates of maltreatment in girls with attention-deficit/hyperactivity disorder: Increased risk for internalizing symptoms and suicidality. Dev. Psychopathol. 2016, 28, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, L.; Fang, X.; Mercy, J.; Perou, R.; Grosse, S.D. Attention-deficit/hyperactivity disorder symptoms and child maltreatment: A population-based study. J. Pediatr. 2008, 153, 851–856. [Google Scholar] [CrossRef]
- Theule, J.; Wiener, J.; Rogers, M.A.; Marton, I. Predicting parenting stress in families of children with adhd: Parent and contextual factors. J. Child Fam. Stud. 2011, 20, 640–647. [Google Scholar] [CrossRef]
- Wallander, J.L.; Noojin, A.B. Mothers’ report of stressful experiences related to having a child with a physical disability. Children’s Health Care 1995, 24, 245–256. [Google Scholar] [CrossRef]
- Graham-Bermann, S.; Seng, J. Violence exposure and traumatic stress symptoms as additional predictors of health problems in high-risk children. J. Pediatr. 2005, 146, 349–354. [Google Scholar] [CrossRef]
- Kitzmann, K.M.; Gaylord, N.K.; Holt, A.R.; Kenny, E.D. Child witnesses to domestic violence: A meta-analytic review. J. Consult. Clin. Psychol. 2003, 71, 339–352. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.; Schwebel, D.C.; Elliott, M.N.; Visser, S.N.; Toomey, S.L.; McLaughlin, K.A.; Cuccaro, P.; Tortolero Emery, S.; Banspach, S.W.; Schuster, M.A. The association between youth violence exposure and attention-deficit/hyperactivity disorder (ADHD) symptoms in a sample of fifth-graders. Am. J. Orthopsychiatr. 2015, 85, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.M.; Brown, S.N.; Briggs, R.D.; German, M.; Belamarich, P.F.; Oyeku, S.O. Associations between adverse childhood experiences and adhd diagnosis and severity. Acad. Pediatr. 2017, 17, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Fuller-Thomson, E.; Lewis, D.A. The relationship between early adversities and attention-deficit/hyperactivity disorder. Child Abuse Negl. 2015, 47, 94–101. [Google Scholar] [CrossRef]
- Le, M.T.; Holton, S.; Romero, L.; Fisher, J. Polyvictimization among children and adolescents in low-and lower-middle-income countries: A systematic review and meta-analysis. Trauma Violence Abuse 2018, 19, 323–342. [Google Scholar] [CrossRef]
- Dong, M.; Anda, R.F.; Felitti, V.J.; Dube, S.R.; Williamson, D.F.; Thompson, T.J.; Loo, C.M.; Giles, W.H. The interrelatedness of multiple forms of childhood abuse, neglect, and household dysfunction. Child Abuse Negl. 2004, 28, 771–784. [Google Scholar] [CrossRef]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A. Poly-victimization: A neglected component in child victimization. Child Abuse Negl. 2007, 31, 7–26. [Google Scholar] [CrossRef]
- Saunders, B. Understanding children exposed to violence: Toward an integration of overlapping fields. J. Interpers. Violence 2003, 18, 356–376. [Google Scholar] [CrossRef]
- Turner, H.A.; Finkelhor, D.; Ormrod, R. The effect of lifetime victimization on the mental health of children and adolescents. Soc. Sci. Med. 2006, 62, 13–27. [Google Scholar] [CrossRef]
- Ford, J.D.; Wasser, T.; Connor, D.F. Identifying and determining the symptom severity associated with polyvictimization among psychiatrically impaired children in the outpatient setting. Child Maltreatment 2011, 16, 216–226. [Google Scholar] [CrossRef]
- Finkelhor, D.; Ormrod, R.; Turner, H.; Holt, M. Pathways to poly-victimization. Child Maltreatment 2009, 14, 316–329. [Google Scholar] [CrossRef]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A. Polyvictimization and trauma in a national longitudinal cohort. Dev. Psychopathol. 2007, 19, 149–166. [Google Scholar] [CrossRef]
- Finkelhor, D.; Turner, H.; Ormrod, R.; Hamby, S.L. Violence, abuse, and crime exposure in a national sample of children and youth. Pediatrics 2009, 124, 1411. [Google Scholar] [CrossRef]
- Finkelhor, D.; Hamby, S.L.; Ormrod, R.; Turner, H. The juvenile victimization questionnaire: Reliability, validity, and national norms. Child Abuse Negl. 2005, 29, 383–412. [Google Scholar] [CrossRef]
- Cappadocia, M.C.; Weiss, J.A.; Pepler, D. Bullying experiences among children and youth with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 266–277. [Google Scholar] [CrossRef]
- Rowley, E.; Chandler, S.; Baird, G.; Simonoff, E.; Pickles, A.; Loucas, T.; Charman, T. The experience of friendship, victimization and bullying in children with an autism spectrum disorder: Associations with child characteristics and school placement. Res. Autism Spectr. Disord. 2012, 6, 1126–1134. [Google Scholar] [CrossRef]
- Loveland, K.A.; Pearson, D.A.; Tunali-Kotoski, B.; Ortegon, J.; Gibbs, M.C. Judgments of social appropriateness by children and adolescents with autism. J. Autism Dev. Disord. 2001, 31, 367–376. [Google Scholar] [CrossRef]
- Fisher, M.H.; Taylor, J.L. Let’s talk about it: Peer victimization experiences as reported by adolescents with autism spectrum disorder. Autism 2016, 20, 402–411. [Google Scholar] [CrossRef]
- Kloosterman, P.H.; Kelley, E.A.; Craig, W.M.; Parker, J.D.; Javier, C. Types and experiences of bullying in adolescents with an autism spectrum disorder. Res. Autism Spectr. Disord. 2013, 7, 824–832. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Fedina, C. Cyber bullying in adhd and asperger syndrome populations. Res. Autism Spectr. Disord. 2011, 5, 1201–1208. [Google Scholar] [CrossRef]
- Hebron, J.; Humphrey, N. Exposure to bullying among students with autism spectrum conditions: A multi-informant analysis of risk and protective factors. Autism 2014, 18, 618–630. [Google Scholar] [CrossRef]
- Adams, R.E.; Fredstrom, B.K.; Duncan, A.W.; Holleb, L.J.; Bishop, S.L. Using self-and parent-reports to test the association between peer victimization and internalizing symptoms in verbally fluent adolescents with asd. J. Autism Dev. Disord. 2014, 44, 861–872. [Google Scholar] [CrossRef]
- Li, Q. New bottle but old wine: A research of cyberbullying in schools. Comput. Hum. Behav. 2007, 23, 1777–1791. [Google Scholar] [CrossRef]
- Chan, K.L. Victimization and poly-victimization among school-aged chinese adolescents: Prevalence and associations with health. Prev. Med. 2013, 56, 207–210. [Google Scholar] [CrossRef]
- Soler, L.; Seguera, A.; Kirchner, T.; Forns, M. Polyvictimization and risk for suicidal phenomena in a community sample of spanish adolescents. Violence Vict. 2013, 28, 899. [Google Scholar] [CrossRef]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. HTA Initiative #13; Alberta Heritage Foundation for Medical Research (AHFMR): Edmonton, AB, Canada, 2004. [Google Scholar]
- Greger, H.K.; Myhre, A.K.; Lydersen, S.; Jozefiak, T. Previous maltreatment and present mental health in a high-risk adolescent population. Child Abuse Negl. 2015, 45, 122–134. [Google Scholar] [CrossRef]
- Pfeffer, R.D. Childhood victimization in a national sample of youth with autism spectrum disorders. J. Policy Pract. Intell. Disabil. 2016, 13, 311–319. [Google Scholar] [CrossRef]
- Aguado-Gracia, J.; Mundo-Cid, P.; Lopez-Seco, F.; Acosta-Garcia, S.; Cortes-Ruiz, M.; Vilella, E.; Masana-Marin, A. Lifetime victimization in children and adolescents with adhd. J. Interpers. Violence 2018. [Google Scholar] [CrossRef]
- Chan, K.L.; Lo, C.K.; Ip, P. Associating disabilities, school environments, and child victimization. Child Abuse Negl. 2018, 83, 21–30. [Google Scholar] [CrossRef]
- Paul, A.; Gallot, C.; Lelouche, C.; Bouvard, M.P.; Amestoy, A. Victimisation in a french population of children and youths with autism spectrum disorder: A case control study. Child Adolesc. Psychiatr. Ment. Health 2018, 12, 1–13. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Nilsson, D.; Nordenstam, C.; Green, S.; Wetterhall, A.; Lundin, T.; Svedin, C.G. Acute stress among adolescents and female rape victims measured by asc-kids: A pilot study. Nord. J. Psychiatr. 2015, 69, 539–545. [Google Scholar] [CrossRef]
- Compier-de Block, L.H.; Alink, L.R.; Linting, M.; van den Berg, L.J.; Elzinga, B.M.; Voorthuis, A.; Tollenaar, M.S.; Bakermans-Kranenburg, M.J. Parent-child agreement on parent-to-child maltreatment. J. Fam. Violence 2017, 32, 207–217. [Google Scholar] [CrossRef]
- Frith, U.; Hill, E.L. Autism: Mind and Brain; Oxford University Press: New York, NY, USA, 2004; Volume 358. [Google Scholar]
- Matson, J.L.; Nebel-Schwalm, M. Assessing challenging behaviors in children with autism spectrum disorders: A review. Res. Dev. Disabil. 2007, 28, 567–579. [Google Scholar] [CrossRef]
- Howlin, P. Autism and Asperger Syndrome: Preparing for Adulthood, 2nd ed.; Routledge: New York, NY, USA, 2004. [Google Scholar]
- Campbell, M.; Hwang, Y.-S.; Whiteford, C.; Dillon-Wallace, J.; Ashburner, J.; Saggers, B.; Carrington, S. Bullying prevalence in students with autism spectrum disorder. Australas. J. Spec. Educ. 2017, 41, 101–122. [Google Scholar] [CrossRef]
- Rose, C.A.; Espelage, D.L. Risk and protective factors associated with the bullying involvement of students with emotional and behavioral disorders. Behav. Disord. 2012, 37, 133–148. [Google Scholar] [CrossRef]
- Sreckovic, M.A.; Brunsting, N.C.; Able, H. Victimization of students with autism spectrum disorder: A review of prevalence and risk factors. Res. Autism Spectr. Disord. 2014, 8, 1155–1172. [Google Scholar] [CrossRef]
- Slaughter, V.; Dennis, M.J.; Pritchard, M. Theory of mind and peer acceptance in preschool children. Br. J. Dev. Psychol. 2002, 20, 545–564. [Google Scholar] [CrossRef]
- Waters, E.; Stewart-Brown, S.; Fitzpatrick, R. Agreement between adolescent self-report and parent reports of health and well-being: Results of an epidemiological study. Child Care Health Dev. 2003, 29, 501–509. [Google Scholar] [CrossRef]
- Bradshaw, C.P.; Sawyer, A.L.; O’Brennan, L.M. Bullying and peer victimization at school: Perceptual differences between students and school staff. School Psychol. Rev. 2007, 36, 361–382. [Google Scholar]
| Study ID | Country | Sample & Study Design | Sample Size | Diagnosis1 | Child/Adolescent Age Range (Years) | Questionnaire and Informants | Time Frame | Type of victimization Examined * | Prevalence Rates and Frequency * | Quality Assessment Score (out of 22) |
|---|---|---|---|---|---|---|---|---|---|---|
| Aguado-Gracia et al. 2018 | Spain | clinical sample | N = 106 (77.4% male) | ADHD | 6–18 (M = 11.2, SD = 2.63) | Self-report (age > 12) and parent-reports (age < 12) The Juvenile Victimization Questionnaire | Lifetime | CC, CM, PV, SA WIA | CC (75.5%); CM (29.2%); PV (67.9%); SV (6.6%), WIA (41.5%) | 19 |
| Chan et al. 2018 | Hong-Kong | Representative sample of school-aged children Cross-sectional | Total N = 4114 (ADHD N = 433) ASD (N = 330) No disabilities (N = 3013) | ADHD, ASD | 6–18 | Parental reports The Juvenile Victimization Questionnaire | Yearly | CC, CM, PV, SA WIA, B, CB | CC (ASD = 29.4% ADHD = 37.1%) CM (ASD = 23.5% ADHD = 30.0%) PV (ASD = 21.5% ADHD = 33.5%) SA (ASD = 2.8% ADHD = 8.1%) WIA (ASD = 5.9% ADHD = 14.0%) B (ASD = 21.0% ADHD = 32.1%) CB (ASD = 22.0% ADHD = 32.3%) Polyvictimization (odds) Any 1 type (ASD = 1.52 [1.11–2.08] ADHD = 1.31 [0.95–1.80]) 1–3 types (ASD = 1.43 [1.02–2.00] ADHD = 1.20 [0.84–1.72]) 4 types or more (ASD = 1.36 [0.79–2.36] ADHD = 2.62 [1.49–4.32]) | 22 |
| Greger et al. 2015 | Norway | Clinical sample (child welfare institutions) | N = 400 of which 23%, (N = 75) diagnosed with Asperger’s syndrome (ASD) and 32% (N = 106) diagnosed with ADHD | AS, ADHD | 13–23 | The Adverse Childhood Experiences (ACE) Self-report | Last three months | DM, NV, SA, WFV, WCV | DM (AS = 29.9% ADHD = 27.1%) NV (AS = 27.5% ADHD = 34.6%) SA (AS = 27.3% ADHD = 38.2%) WFV (AS = 30.0% ADHD = 47.6%) WCV (AS = 24.1% ADHD = 0.3%) | 22 |
| Paul et al. 2018 | France | Clinical sample (ASD expert center) | N = 92 of which 39 with ASD (84.6% male) and 53 TD (84.9% male). | ASD | 8–18 M = 13.23 (SD = 2.96) | The Juvenile Victimization Questionnaire Parental-report | Lifetime | CC, CM, PV, SA WIA (see article for prevalence rates of 34 forms of offenses) VAS, VAH, VE | VAS (75.7%) VAH (16.2%) VE (8.1%) Polyvictimization (23.1% ASD; 17% TD) | 18 |
| Pfeffer 2016 | USA | Population-based | N = 262 (82.3% male) | ASD | 5–18 M = 11.07 (SD = 3.58) | The Juvenile Victimization Questionnaire Parental-report | Lifetime, yearly | CC, CM, PV, SA WIA | CC (Yearly: 49.0% Lifetime: 64.2%) CM (Yearly: 36.0% Lifetime: 50.4%) PV (Yearly: 74.3% Lifetime: 83.8%) SA (Yearly: 7.6% Lifetime: 14.0%) WIA (Yearly: 20.4% Lifetime: 30.0%) Polyvictimization 76% yearly | 17 |
| Turner et al. 2011 | USA | Population-based | 4046 of which 6.7% (N =) w ADHD diagnosis | ADHD | 2–17 (M = 9.6) | The Juvenile Victimization Questionnaire Parental report (age < 10) Self-report (age < 10) | Yearly | CC, PV, SA, CM | CC (38.3%) CM (16.9%) PV (45.7%) SA (6.7%) | 22 |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hellström, L. A Systematic Review of Polyvictimization among Children with Attention Deficit Hyperactivity or Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2019, 16, 2280. https://doi.org/10.3390/ijerph16132280
Hellström L. A Systematic Review of Polyvictimization among Children with Attention Deficit Hyperactivity or Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2019; 16(13):2280. https://doi.org/10.3390/ijerph16132280
Chicago/Turabian StyleHellström, Lisa. 2019. "A Systematic Review of Polyvictimization among Children with Attention Deficit Hyperactivity or Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 16, no. 13: 2280. https://doi.org/10.3390/ijerph16132280
APA StyleHellström, L. (2019). A Systematic Review of Polyvictimization among Children with Attention Deficit Hyperactivity or Autism Spectrum Disorder. International Journal of Environmental Research and Public Health, 16(13), 2280. https://doi.org/10.3390/ijerph16132280