Depression Fully Mediates the Effect of Multimorbidity on Self-Rated Health for Economically Disadvantaged African American Men but Not Women



Abstract
1. Introduction
Aims
2. Methods
2.1. Design and Setting
2.2. Institutional Review Board (IRB)
2.3. Process and Data Collection
2.4. Participants
2.5. Measures
2.5.1. Dependent Variable
2.5.2. Mediator
2.5.3. Independent Variable
2.5.4. Confounders
2.5.5. Moderator
2.6. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Bivariate Correlations
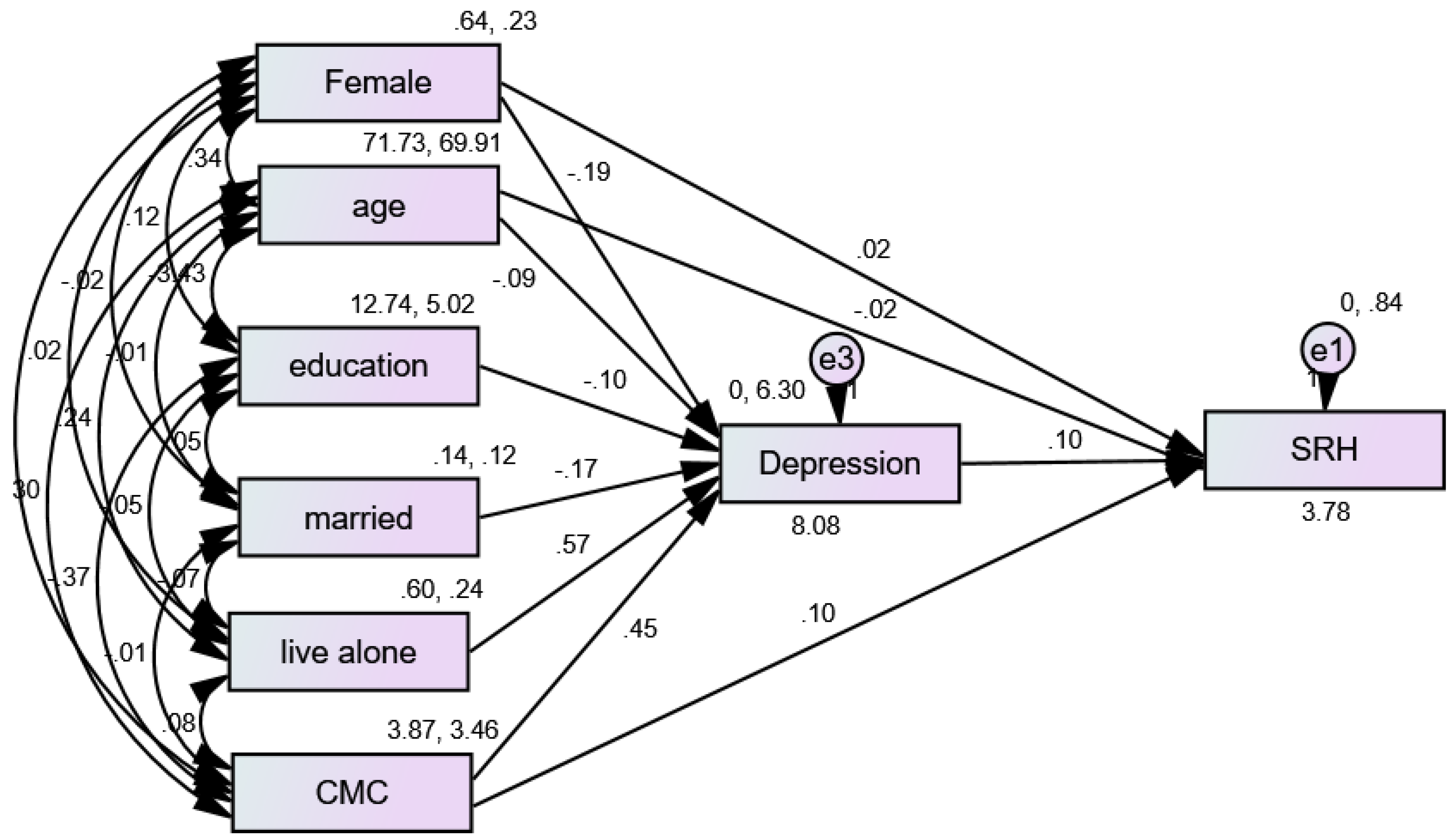
3.3. Structural Equation Modeling (SEM) in the Pooled Sample
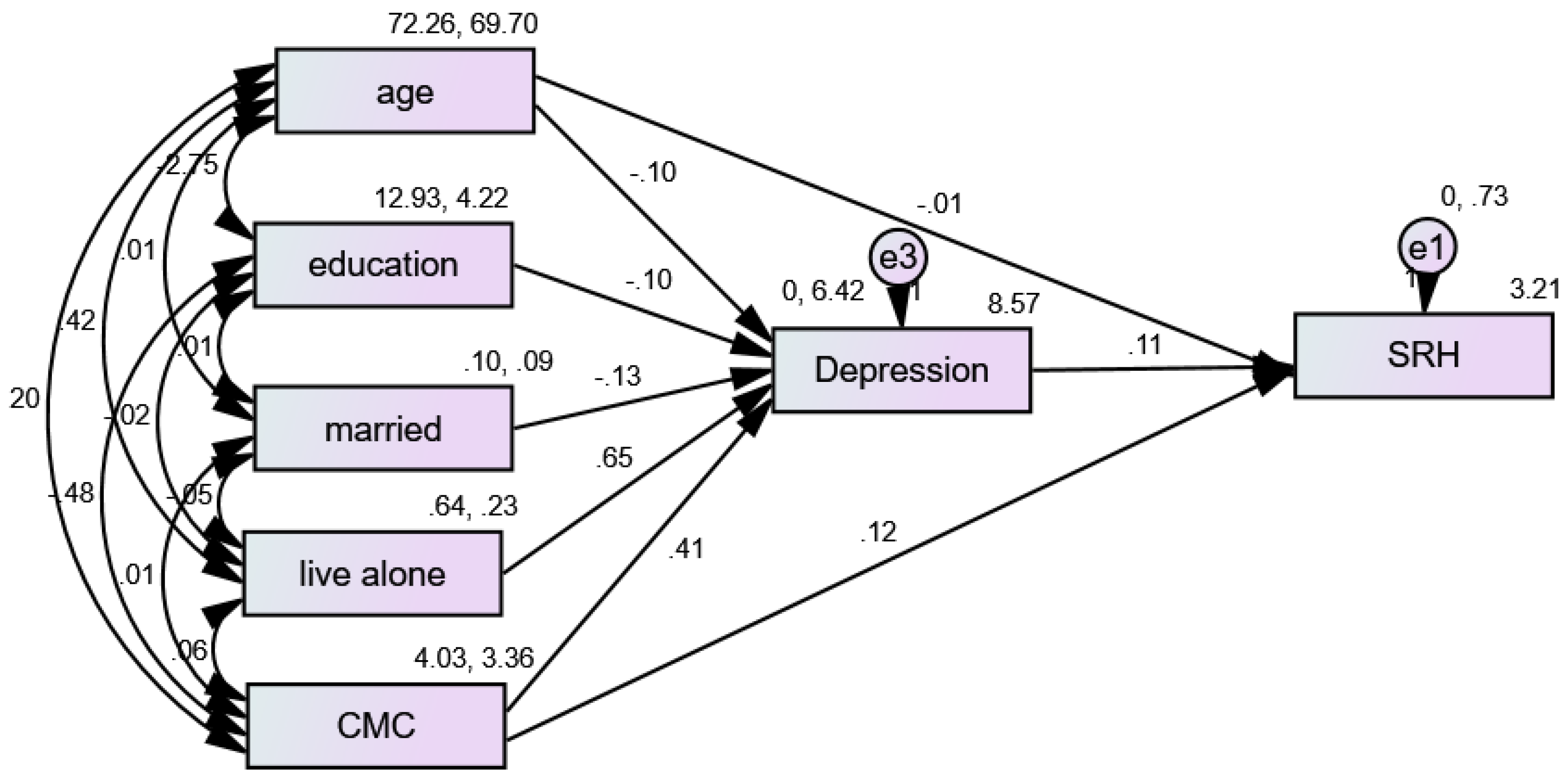
3.4. Structural Equation Modeling (SEM) in African American (AA) Men
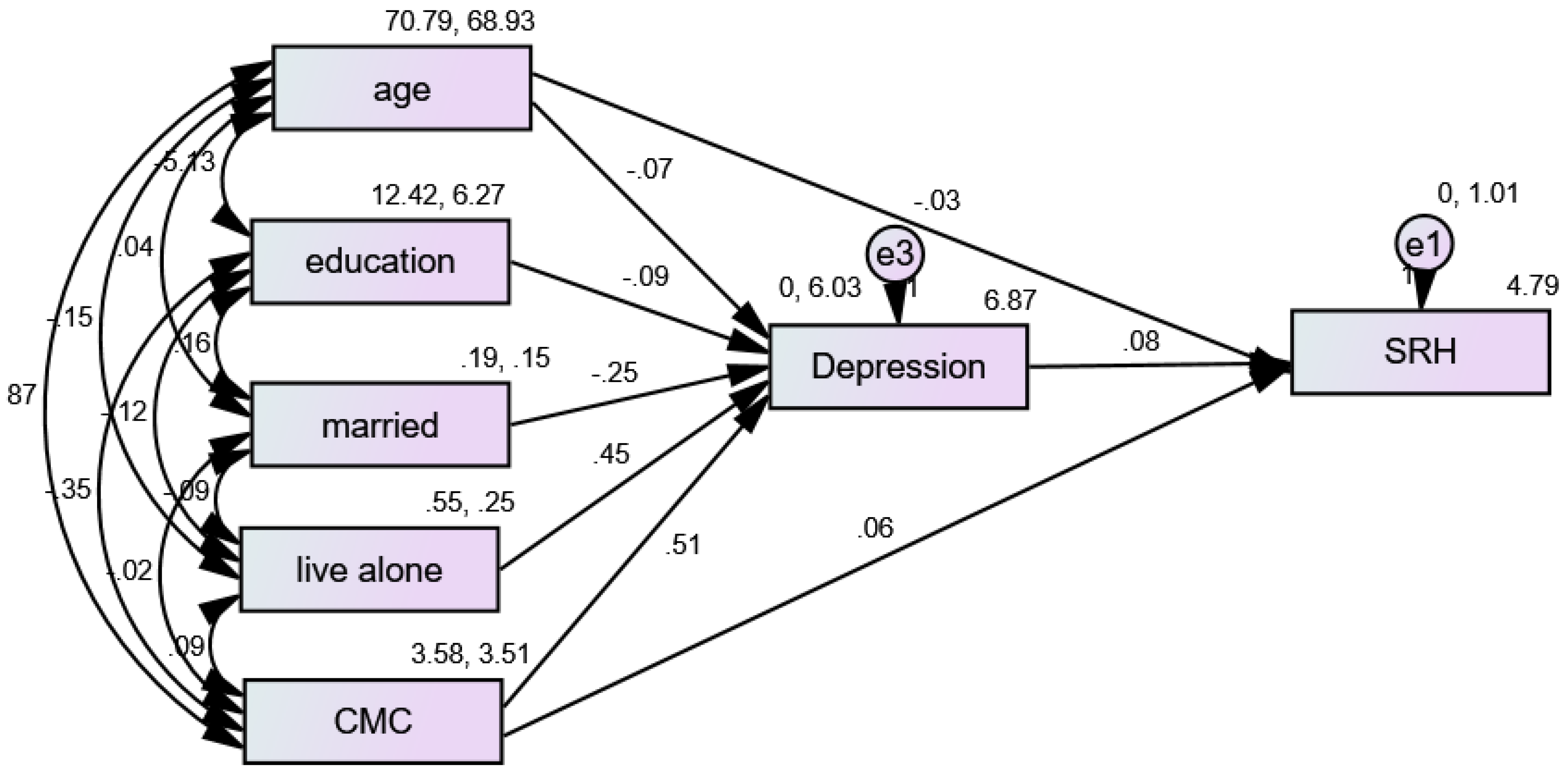
3.5. Structural Equation Modeling (SEM) in African American (AA) Women
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Assari, S. Self-rated Health and Mortality due to Kidney Diseases: Racial Differences in the United States. Adv. Biomed. Res. 2018, 7, 4. [Google Scholar] [CrossRef]
- Godaert, L.; Godard-Sebillotte, C.; Allard Saint-Albin, L.; Bousquet, L.; Bourdel-Marchasson, I.; Fanon, J.L.; Drame, M. Self-rated health as a predictor of mid-term and long-term mortality in older Afro-Caribbeans hospitalised via the emergency department. Qual. Life Res. 2018, 27, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Grove, B.E.; Schougaard, L.M.; Hjollund, N.H.; Ivarsen, P. Self-rated health, quality of life and appetite as predictors of initiation of dialysis and mortality in patients with chronic kidney disease stages 4-5: A prospective cohort study. BMC Res. Notes 2018, 11, 371. [Google Scholar] [CrossRef]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Nery Guimaraes, J.M.; Chor, D.; Werneck, G.L.; Carvalho, M.S.; Coeli, C.M.; Lopes, C.S.; Faerstein, E. Association between self-rated health and mortality: 10 years follow-up to the Pro-Saude cohort study. BMC Public Health 2012, 12, 676. [Google Scholar] [CrossRef] [PubMed]
- Phung, T.K.T.; Siersma, V.; Vogel, A.; Waldorff, F.B.; Waldemar, G. Self-rated versus Caregiver-rated Health for Patients with Mild Dementia as Predictors of Patient Mortality. Am. J. Geriatr. Psychiatry 2018, 26, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Schnittker, J.; Bacak, V. The increasing predictive validity of self-rated health. PLoS ONE 2014, 9, e84933. [Google Scholar] [CrossRef]
- Szybalska, A.; Broczek, K.; Puzianowska-Kuznicka, M.; Slusarczyk, P.; Chudek, J.; Skalska, A.; Mossakowska, M. Self-rated health and its association with all-cause mortality of older adults in Poland: The PolSenior project. Arch. Gerontol. Geriatr. 2018, 79, 13–20. [Google Scholar] [CrossRef]
- Thong, M.S.; Kaptein, A.A.; Benyamini, Y.; Krediet, R.T.; Boeschoten, E.W.; Dekker, F.W.; Netherlands Cooperative Study on the Adequacy of Dialysis Study Group. Association between a self-rated health question and mortality in young and old dialysis patients: A cohort study. Am. J. Kidney Dis. 2008, 52, 111–117. [Google Scholar] [CrossRef]
- Idler, E.L.; Angel, R.J. Self-rated health and mortality in the NHANES-I Epidemiologic Follow-up Study. Am. J. Public Health 1990, 80, 446–452. [Google Scholar] [CrossRef]
- Lainscak, M.; Farkas, J.; Frantal, S.; Singer, P.; Bauer, P.; Hiesmayr, M.; Schindler, K. Self-rated health, nutritional intake and mortality in adult hospitalized patients. Eur. J. Clin. Investig. 2014, 44, 813–824. [Google Scholar] [CrossRef]
- Wennberg, P.; Rolandsson, O.; Jerden, L.; Boeing, H.; Sluik, D.; Kaaks, R.; Teucher, B.; Spijkerman, A.; Bueno de Mesquita, B.; Dethlefsen, C.; et al. Self-rated health and mortality in individuals with diabetes mellitus: Prospective cohort study. BMJ Open 2012, 2, e000760. [Google Scholar] [CrossRef]
- Gonzalez, M.; Sjolin, I.; Back, M.; Ogmundsdottir Michelsen, H.; Tanha, T.; Sandberg, C.; Schiopu, A.; Leosdottir, M. Effect of a lifestyle-focused electronic patient support application for improving risk factor management, self-rated health, and prognosis in post-myocardial infarction patients: Study protocol for a multi-center randomized controlled trial. Trials 2019, 20, 76. [Google Scholar] [CrossRef]
- Duberg, A.; Hagberg, L.; Sunvisson, H.; Moller, M. Influencing self-rated health among adolescent girls with dance intervention: A randomized controlled trial. JAMA Pediatr. 2013, 167, 27–31. [Google Scholar] [CrossRef]
- Diaz, E.; Bruce, N.; Pope, D.; Diaz, A.; Smith, K.R.; Smith-Sivertsen, T. Self-rated health among Mayan women participating in a randomised intervention trial reducing indoor air pollution in Guatemala. BMC Int. Health Hum. Rights 2008, 8, 7. [Google Scholar] [CrossRef]
- Steptoe, A.; Perkins-Porras, L.; Hilton, S.; Rink, E.; Cappuccio, F.P. Quality of life and self-rated health in relation to changes in fruit and vegetable intake and in plasma vitamins C and E in a randomised trial of behavioural and nutritional education counselling. Br. J. Nutr. 2004, 92, 177–184. [Google Scholar] [CrossRef][Green Version]
- Mavaddat, N.; Kinmonth, A.L.; Sanderson, S.; Surtees, P.; Bingham, S.; Khaw, K.T. What determines Self-Rated Health (SRH)? A cross-sectional study of SF-36 health domains in the EPIC-Norfolk cohort. J. Epidemiol. Community Health 2011, 65, 800–806. [Google Scholar] [CrossRef]
- Westerlund, H.; Kivimaki, M.; Singh-Manoux, A.; Melchior, M.; Ferrie, J.E.; Pentti, J.; Jokela, M.; Leineweber, C.; Goldberg, M.; Zins, M.; et al. Self-rated health before and after retirement in France (GAZEL): A cohort study. Lancet 2009, 374, 1889–1896. [Google Scholar] [CrossRef]
- Delpierre, C.; Datta, G.D.; Kelly-Irving, M.; Lauwers-Cances, V.; Berkman, L.; Lang, T. What role does socio-economic position play in the link between functional limitations and self-rated health: France vs. USA? Eur. J. Public Health 2012, 22, 317–321. [Google Scholar] [CrossRef]
- Etherington, N. Re-evaluating gender differences in self-rated health: The importance of cohort. J. Women Aging 2017, 29, 150–162. [Google Scholar] [CrossRef]
- McDonough, P.; Berglund, P. Histories of poverty and self-rated health trajectories. J. Health Soc. Behav. 2003, 44, 198–214. [Google Scholar] [CrossRef]
- Lee, S.J.; Moody-Ayers, S.Y.; Landefeld, C.S.; Walter, L.C.; Lindquist, K.; Segal, M.R.; Covinsky, K.E. The relationship between self-rated health and mortality in older black and white Americans. J. Am. Geriatr. Soc. 2007, 55, 1624–1629. [Google Scholar] [CrossRef]
- Torsheim, T.; Nygren, J.M.; Rasmussen, M.; Arnarsson, A.M.; Bendtsen, P.; Schnohr, C.W.; Nielsen, L.; Nyholm, M. Social inequalities in self-rated health: A comparative cross-national study among 32,560 Nordic adolescents. Scand. J. Public Health 2018, 46, 150–156. [Google Scholar] [CrossRef]
- Lee, Y. Does Context Matter? Literacy Disparities in Self-rated Health Using Evidence from 17 Developed Countries. Am. J. Health Behav. 2017, 41, 287–300. [Google Scholar] [CrossRef]
- Kim, S.; Kim, C.Y.; You, M.S. Civic participation and self-rated health: A cross-national multi-level analysis using the world value survey. J. Prev. Med. Public Health 2015, 48, 18–27. [Google Scholar] [CrossRef]
- French, D.J.; Browning, C.; Kendig, H.; Luszcz, M.A.; Saito, Y.; Sargent-Cox, K.; Anstey, K.J. A simple measure with complex determinants: Investigation of the correlates of self-rated health in older men and women from three continents. BMC Public Health 2012, 12, 649. [Google Scholar] [CrossRef]
- Prus, S.G. Comparing social determinants of self-rated health across the United States and Canada. Soc. Sci. Med. 2011, 73, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Hanibuchi, T.; Nakaya, T.; Murata, C. Socio-economic status and self-rated health in East Asia: A comparison of China, Japan, South Korea and Taiwan. Eur. J. Public Health 2012, 22, 47–52. [Google Scholar] [CrossRef]
- Bardage, C.; Pluijm, S.M.F.; Pedersen, N.L.; Deeg, D.J.H.; Jylha, M.; Noale, M.; Blumstein, T.; Otero, A. Self-rated health among older adults: A cross-national comparison. Eur. J. Ageing 2005, 2, 149–158. [Google Scholar] [CrossRef]
- Gonzales, G.; Ehrenfeld, J.M. The Association between State Policy Environments and Self-Rated Health Disparities for Sexual Minorities in the United States. Int. J. Environ. Res. Public Health 2018, 15, 1136. [Google Scholar] [CrossRef]
- Dowling, A.; Enticott, J.; Russell, G. Measuring self-rated health status among resettled adult refugee populations to inform practice and policy—A scoping review. BMC Health Serv. Res. 2017, 17, 817. [Google Scholar] [CrossRef]
- Badland, H.; Mavoa, S.; Livingston, M.; David, S.; Giles-Corti, B. Testing spatial measures of alcohol outlet density with self-rated health in the Australian context: Implications for policy and practice. Drug Alcohol Rev. 2016, 35, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Spurling, G.; Hayman, N. Self-rated health status in an urban indigenous primary care setting: Implications for clinicians and public health policy. Aust. N. Z. J. Public Health 2010, 34, 598–601. [Google Scholar] [CrossRef]
- Kravitz-Wirtz, N. Cumulative Effects of Growing Up in Separate and Unequal Neighborhoods on Racial Disparities in Self-rated Health in Early Adulthood. J. Health Soc. Behav. 2016, 57, 453–470. [Google Scholar] [CrossRef] [PubMed]
- Sibai, A.M.; Rizk, A.; Chemaitelly, H. Self-rated health disparities among disadvantaged older adults in ethnically diverse urban neighborhoods in a Middle Eastern country. Ethn. Health 2017, 22, 490–509. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Racial/ethnic disparities in self-rated health status among adults with and without disabilities—United States, 2004–2006. MMWR Morb. Mortal. Wkly. Rep. 2008, 57, 1069–1073. [Google Scholar]
- Cagney, K.A.; Browning, C.R.; Wen, M. Racial disparities in self-rated health at older ages: What difference does the neighborhood make? J. Gerontol. B Psychol. Sci. Soc. Sci. 2005, 60, S181–S190. [Google Scholar] [CrossRef]
- Maguire, P.A.; Reay, R.E.; Raphael, B. Correlates of a single-item Self-Rated Mental Health Question in people with schizophrenia. Australas. Psychiatry 2016, 24, 473–477. [Google Scholar] [CrossRef]
- Chandola, T.; Jenkinson, C. Validating self-rated health in different ethnic groups. Ethn. Health 2000, 5, 151–159. [Google Scholar] [CrossRef]
- Meng, Q.; Xie, Z.; Zhang, T. A single-item self-rated health measure correlates with objective health status in the elderly: A survey in suburban beijing. Front. Public Health 2014, 2, 27. [Google Scholar] [CrossRef]
- Assari, S. Gender differences in the predictive role of self-rated health on short-term risk of mortality among older adults. SAGE Open Med. 2016, 4, 2050312116666975. [Google Scholar] [CrossRef]
- Assari, S.; Lankarani, M.M. Does Multi-morbidity Mediate the Effect of Socioeconomics on Self-rated Health? Cross-country Differences. Int. J. Prev. Med. 2015, 6, 85. [Google Scholar] [CrossRef]
- Assari, S. Psychiatric Disorders Differently Correlate with Physical Self-Rated Health across Ethnic Groups. J. Pers. Med. 2017, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Ethnic Groups Differ in How Poor Self-Rated Mental Health Reflects Psychiatric Disorders. J. Racial Ethn. Health Disparities 2018, 5, 728–736. [Google Scholar] [CrossRef]
- Zajacova, A.; Huzurbazar, S.; Todd, M. Gender and the structure of self-rated health across the adult life span. Soc. Sci. Med. 2017, 187, 58–66. [Google Scholar] [CrossRef] [PubMed]
- McAlpine, D.D.; McCreedy, E.; Alang, S. The Meaning and Predictive Value of Self-rated Mental Health among Persons with a Mental Health Problem. J. Health Soc. Behav. 2018, 59, 200–214. [Google Scholar] [CrossRef] [PubMed]
- Spuling, S.M.; Wolff, J.K.; Wurm, S. Response shift in self-rated health after serious health events in old age. Soc. Sci. Med. 2017, 192, 85–93. [Google Scholar] [CrossRef]
- Altman, C.E.; Van Hook, J.; Hillemeier, M. What Does Self-rated Health Mean? Changes and Variations in the Association of Obesity with Objective and Subjective Components Of Self-rated Health. J. Health Soc. Behav. 2016, 57, 39–58. [Google Scholar] [CrossRef]
- Lee, S.; Schwarz, N.; Goldstein, L.S. Culture-Sensitive Question Order Effects of Self-Rated Health Between Older Hispanic and Non-Hispanic Adults in the United States. J. Aging Health 2014, 26, 860–883. [Google Scholar] [CrossRef]
- Lee, S.; Schwarz, N. Question context and priming meaning of health: Effect on differences in self-rated health between Hispanics and non-Hispanic Whites. Am. J. Public Health 2014, 104, 179–185. [Google Scholar] [CrossRef]
- Peersman, W.; Cambier, D.; De Maeseneer, J.; Willems, S. Gender, educational and age differences in meanings that underlie global self-rated health. Int. J. Public Health 2012, 57, 513–523. [Google Scholar] [CrossRef] [PubMed]
- McMullen, C.K.; Luborsky, M.R. Self-rated health appraisal as cultural and identity process: African American elders’ health and evaluative rationales. Gerontologist 2006, 46, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Garbarski, D.; Dykema, J.; Croes, K.D.; Edwards, D.F. How participants report their health status: Cognitive interviews of self-rated health across race/ethnicity, gender, age, and educational attainment. BMC Public Health 2017, 17, 771. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T. Self-rated health and mortality with special reference to black-white difference. Ann. Epidemiol. 2017, 27, 295. [Google Scholar] [CrossRef]
- Alang, S.M.; McCreedy, E.M.; McAlpine, D.D. Race, Ethnicity, and Self-Rated Health Among Immigrants in the United States. J. Racial Ethn. Health Disparities 2015, 2, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M.; Burgard, S. Black-white difference in long-term predictive power of self-rated health on all-cause mortality in United States. Ann. Epidemiol. 2016, 26, 106–114. [Google Scholar] [CrossRef]
- Chand, R.; Parker, E.; Jamieson, L. Differences in, and Frames of Reference of, Indigenous Australians’ Self-rated General and Oral Health. J. Health Care Poor Underserved 2017, 28, 1087–1103. [Google Scholar] [CrossRef]
- Siordia, C.; Nguyen, H.T. The Comparative Frame of Reference in Self-Rated Health Questions Matters When Predicting Difficulty with Activities of Daily Living. J. Frailty Aging 2015, 4, 175–180. [Google Scholar] [CrossRef]
- Sargent-Cox, K.A.; Anstey, K.J.; Luszcz, M.A. Patterns of longitudinal change in older adults’ self-rated health: The effect of the point of reference. Health Psychol. 2010, 29, 143–152. [Google Scholar] [CrossRef]
- Sargent-Cox, K.A.; Anstey, K.J.; Luszcz, M.A. Determinants of self-rated health items with different points of reference: Implications for health measurement of older adults. J. Aging Health 2008, 20, 739–761. [Google Scholar] [CrossRef]
- Manderbacka, K.; Kareholt, I.; Martikainen, P.; Lundberg, O. The effect of point of reference on the association between self-rated health and mortality. Soc. Sci. Med. 2003, 56, 1447–1452. [Google Scholar] [CrossRef]
- Manderbacka, K.; Lundberg, O. Examining points of reference of self-rated health among Swedish oldest old. Arch. Gerontol. Geriatr. 1996, 23, 47–60. [Google Scholar] [CrossRef]
- Assari, S. Socioeconomic Status and Self-Rated Oral Health; Diminished Return among Hispanic Whites. Dent. J. 2018, 6, 11. [Google Scholar] [CrossRef]
- Assari, S.; Caldwell, C.H.; Mincy, R.B. Maternal Educational Attainment at Birth Promotes Future Self-Rated Health of White but Not Black Youth: A 15-Year Cohort of a National Sample. J. Clin. Med. 2018, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lapeyrouse, L.M.; Neighbors, H.W. Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans. Behav. Sci. 2018, 8, 50. [Google Scholar] [CrossRef]
- Assari, S.; Caldwell, C.H.; Zimmerman, M.A. Perceived Neighborhood Safety During Adolescence Predicts Subsequent Deterioration of Subjective Health Two Decades Later; Gender Differences in a Racially-Diverse Sample. Int. J. Prev. Med. 2015, 6, 117. [Google Scholar] [CrossRef]
- Assari, S.; Lankarani, M.M.; Piette, J.D.; Aikens, J.E. Self-Rated Health and Glycemic Control in Type 2 Diabetes: Race by Gender Differences. J. Racial Ethn. Health Disparities 2018, 5, 721–727. [Google Scholar] [CrossRef]
- Assari, S.; Dejman, M.; Neighbors, H.W. Ethnic Differences in Separate and Additive Effects of Anxiety and Depression on Self-rated Mental Health Among Blacks. J. Racial Ethn. Health Disparities 2016, 3, 423–430. [Google Scholar] [CrossRef]
- Okamoto, K.; Momose, Y.; Fujino, A.; Osawa, Y. Gender differences in the relationship between self-rated health (SRH) and 6-year mortality risks among the elderly in Japan. Arch. Gerontol. Geriatr. 2008, 47, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, A.M.; Bentley, R.; Turrell, G.; Broom, D.H.; Subramanian, S.V. Does gender modify associations between self rated health and the social and economic characteristics of local environments? J. Epidemiol. Community Health 2006, 60, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Spiers, N.; Jagger, C.; Clarke, M.; Arthur, A. Are gender differences in the relationship between self-rated health and mortality enduring? Results from three birth cohorts in Melton Mowbray, United Kingdom. Gerontologist 2003, 43, 406–411, discussion 372–405. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Smith, J.L.; Zimmerman, M.A.; Bazargan, M. Cigarette Smoking among Economically Disadvantaged African-American Older Adults in South Los Angeles: Gender Differences. Int. J. Environ. Res. Public Health 2019, 16, 1208. [Google Scholar] [CrossRef] [PubMed]
- Bazargan, M.; Smith, J.L.; Cobb, S.; Barkley, L.; Wisseh, C.; Ngula, E.; Thomas, R.J.; Assari, S. Emergency Department Utilization among Underserved African American Older Adults in South Los Angeles. Int. J. Environ. Res. Public Health 2019, 16, 1175. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, D.E.; Malmrose, L.C.; Blazer, D.G.; Gold, D.T.; Seeman, T.E. Self-rated health and mortality in the high-functioning elderly—A closer look at healthy individuals: MacArthur field study of successful aging. J. Gerontol. 1994, 49, M109–M115. [Google Scholar] [CrossRef]
- Heidrich, J.; Liese, A.D.; Lowel, H.; Keil, U. Self-rated health and its relation to all-cause and cardiovascular mortality in southern Germany. Results from the MONICA Augsburg cohort study 1984–1995. Ann. Epidemiol. 2002, 12, 338–345. [Google Scholar] [CrossRef]
- Moreno, X.; Huerta, M.; Albala, C. Global self-rated health and mortality in older people. Gac. Sanit. 2014, 28, 246–252. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dasbach, E.J.; Klein, R.; Klein, B.E.; Moss, S.E. Self-rated health and mortality in people with diabetes. Am. J. Public Health 1994, 84, 1775–1779. [Google Scholar] [CrossRef] [PubMed]
- Mavaddat, N.; Parker, R.A.; Sanderson, S.; Mant, J.; Kinmonth, A.L. Relationship of self-rated health with fatal and non-fatal outcomes in cardiovascular disease: A systematic review and meta-analysis. PLoS ONE 2014, 9, e103509. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Russell, L.B.; Davis, D. Survival, functional limitations, and self-rated health in the NHANES I Epidemiologic Follow-up Study, 1992. First National Health and Nutrition Examination Survey. Am. J. Epidemiol. 2000, 152, 874–883. [Google Scholar] [CrossRef]
- Kurlowicz, L. The Geriatric Depression Scale (GDS). Geriatr. Nurs. 1999, 20, 212–213. [Google Scholar] [CrossRef]
- Assari, S. Combined Racial and Gender Differences in the Long-Term Predictive Role of Education on Depressive Symptoms and Chronic Medical Conditions. J. Racial Ethn. Health Disparities 2017, 4, 385–396. [Google Scholar] [CrossRef]
- Martin, L.M.; Leff, M.; Calonge, N.; Garrett, C.; Nelson, D.E. Validation of self-reported chronic conditions and health services in a managed care population. Am. J. Prev. Med. 2000, 18, 215–218. [Google Scholar] [CrossRef]
- Agyemang, C.; Denktas, S.; Bruijnzeels, M.; Foets, M. Validity of the single-item question on self-rated health status in first generation Turkish and Moroccans versus native Dutch in the Netherlands. Public Health 2006, 120, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Radeos, M.S.; Cydulka, R.K.; Rowe, B.H.; Barr, R.G.; Clark, S.; Camargo, C.A., Jr. Validation of self-reported chronic obstructive pulmonary disease among patients in the ED. Am. J. Emerg. Med. 2009, 27, 191–196. [Google Scholar] [CrossRef]
- Pastorino, S.; Richards, M.; Hardy, R.; Abington, J.; Wills, A.; Kuh, D.; Pierce, M.; The National Survey of Health and Development Scientific and Data Collection Teams. Validation of self-reported diagnosis of diabetes in the 1946 British birth cohort. Prim. Care Diabetes 2015, 9, 397–400. [Google Scholar] [CrossRef]
- Vigen, C.; Kwan, M.L.; John, E.M.; Gomez, S.L.; Keegan, T.H.; Lu, Y.; Shariff-Marco, S.; Monroe, K.R.; Kurian, A.W.; Cheng, I.; et al. Validation of self-reported comorbidity status of breast cancer patients with medical records: The California Breast Cancer Survivorship Consortium (CBCSC). Cancer Causes Control 2016, 27, 391–401. [Google Scholar] [CrossRef]
- Fontanelli, M.M.; Teixeira, J.A.; Sales, C.H.; Castro, M.A.; Cesar, C.L.; Alves, M.C.; Goldbaum, M.; Marchioni, D.M.; Fisberg, R.M. Validation of self-reported diabetes in a representative sample of Sao Paulo city. Rev. Saude Publica 2017, 51, 20. [Google Scholar] [CrossRef]
- Nishi, A.; Kawachi, I.; Shirai, K.; Hirai, H.; Jeong, S.; Kondo, K. Sex/gender and socioeconomic differences in the predictive ability of self-rated health for mortality. PLoS ONE 2012, 7, e30179. [Google Scholar] [CrossRef] [PubMed]
- Unden, A.L.; Elofsson, S.; Andreasson, A.; Hillered, E.; Eriksson, I.; Brismar, K. Gender differences in self-rated health, quality of life, quality of care, and metabolic control in patients with diabetes. Gend. Med. 2008, 5, 162–180. [Google Scholar] [CrossRef]
- Rohlfsen, L.S.; Jacobs Kronenfeld, J. Gender Differences in Trajectories of Self-Rated Health in Middle and Old Age: An Examination of Differential Exposure and Differential Vulnerability. J. Aging Health 2014, 26, 637–662. [Google Scholar] [CrossRef]
- Wang, J.M.; Lee, L.O.; Spiro, A., 3rd. Gender differences in the impact of warfare exposure on self-rated health. Women’s Health Issues 2015, 25, 35–41. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Assari, S. Separate and Combined Effects of Anxiety, Depression and Problem Drinking on Subjective Health among Black, Hispanic and Non-Hispanic White Men. Int. J. Prev. Med. 2014, 5, 269–279. [Google Scholar]
- Assari, S. Suicide Attempts in Michigan HealthCare System; Racial Differences. Brain Sci. 2018, 8, 124. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Moazen-Zadeh, E. Ethnic Variation in the Cross-sectional Association between Domains of Depressive Symptoms and Clinical Depression. Front. Psychiatry 2016, 7, 53. [Google Scholar] [CrossRef]
- Assari, S. Cross-country variation in additive effects of socio-economics, health behaviors, and comorbidities on subjective health of patients with diabetes. J. Diabetes Metab. Disord. 2014, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Desesquelles, A.F.; Egidi, V.; Salvatore, M.A. Why do Italian people rate their health worse than French people do? An exploration of cross-country differentials of self-rated health. Soc. Sci. Med. 2009, 68, 1124–1128. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Drewnowski, A.; Moudon, A.V.; Aggarwal, A.; Oppert, J.M.; Charreire, H.; Chaix, B. The impact of area residential property values on self-rated health: A cross-sectional comparative study of Seattle and Paris. Prev. Med. Rep. 2016, 4, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.B.; Scott, J.W. The institutional decimation of Black American males. West. J. Black Stud. 1978, 2, 82. [Google Scholar]
- Curry, T.J. The Man-Not: Race, Class, Genre, and the Dilemmas of Black Manhood; Temple University Press: Philadelphia, PA, USA, 2017. [Google Scholar]
- Watkins, D.C.; Walker, R.L.; Griffith, D.M. A meta-study of Black male mental health and well-being. J. Black Psychol. 2010, 36, 303–330. [Google Scholar] [CrossRef]
- Watkins, D.C. Depression over the adult life course for African American men: Toward a framework for research and practice. Am. J. Men’s Health 2012, 6, 194–210. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.D.; Hammond, W.P.; Cole-Lewis, Y.; Nuru-Jeter, A.; Melvin, T. Racial Discrimination and Depressive Symptoms Among African-American Men: The Mediating and Moderating Roles of Masculine Self-Reliance and John Henryism. Psychol. Men Masc. 2013, 14, 35–46. [Google Scholar] [CrossRef]
- Hammond, W.P. Taking it like a man: Masculine role norms as moderators of the racial discrimination-depressive symptoms association among African American men. Am. J. Public Health 2012, 102 (Suppl. 2), S232–S241. [Google Scholar] [CrossRef]
- Hammond, P. Real men get depressed. Nurs. Times 1995, 91, 58. [Google Scholar]
- Sellers, S.L.; Neighbors, H.W.; Bonham, V.L. Goal-striving stress and the mental health of college-educated Black American men: The protective effects of system-blame. Am. J. Orthopsychiatry 2011, 81, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.M. “I AM a Man”: Manhood, Minority Men’s Health and Health Equity. Ethn. Dis. 2015, 25, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Gibbons, F.X.; Simons, R. Depression among Black Youth; Interaction of Class and Place. Brain Sci. 2018, 8, 108. [Google Scholar] [CrossRef]
- Assari, S. Educational Attainment Better Protects African American Women than African American Men Against Depressive Symptoms and Psychological Distress. Brain Sci. 2018, 8, 182. [Google Scholar] [CrossRef]
- Wang, J.; Mann, F.; Lloyd-Evans, B.; Ma, R.; Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 2018, 18, 156. [Google Scholar] [CrossRef]
- Snowden, M.B.; Steinman, L.E.; Carlson, W.L.; Mochan, K.N.; Abraido-Lanza, A.F.; Bryant, L.L.; Duffy, M.; Knight, B.G.; Jeste, D.V.; Leith, K.H.; et al. Effect of physical activity, social support, and skills training on late-life emotional health: A systematic literature review and implications for public health research. Front. Public Health 2014, 2, 213. [Google Scholar] [CrossRef] [PubMed]
- Haber, M.G.; Cohen, J.L.; Lucas, T.; Baltes, B.B. The relationship between self-reported received and perceived social support: A meta-analytic review. Am. J. Community Psychol. 2007, 39, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.J.; Chatters, L.M.; Lincoln, K.; Woodward, A.T. Church-Based Exchanges of Informal Social Support among African Americans. Race Soc. Probl. 2017, 9, 53–62. [Google Scholar] [CrossRef]
- Nguyen, A.W.; Taylor, R.J.; Chatters, L.M. Church-Based Social Support Among Caribbean Blacks in the United States. Rev. Relig. Res. 2016, 58, 385–406. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.W.; Chatters, L.M.; Taylor, R.J.; Mouzon, D.M. Social Support from Family and Friends and Subjective Well-Being of Older African Americans. J. Happiness Stud. 2016, 17, 959–979. [Google Scholar] [CrossRef]
- Cross, C.J.; Taylor, R.J.; Chatters, L.M. Family Social Support Networks of African American and Black Caribbean Adolescents. J. Child Fam. Stud. 2018, 27, 2757–2771. [Google Scholar] [CrossRef] [PubMed]
- Chatters, L.M.; Taylor, R.J.; Woodward, A.T.; Nicklett, E.J. Social support from church and family members and depressive symptoms among older African Americans. Am. J. Geriatr. Psychiatry 2015, 23, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Krause, N. Exploring the stress-buffering effects of church-based and secular social support on self-rated health in late life. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, S35–S43. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Moghani Lankarani, M. Secular and Religious Social Support Better Protect Blacks than Whites against Depressive Symptoms. Behav. Sci. 2018, 8, 46. [Google Scholar] [CrossRef]
- Assari, S. Race and Ethnicity, Religion Involvement, Church-based Social Support and Subjective Health in United States: A Case of Moderated Mediation. Int. J. Prev. Med. 2013, 4, 208–217. [Google Scholar]
- Lincoln, K.D.; Chatters, L.M.; Taylor, R.J. Psychological distress among black and white Americans: Differential effects of social support, negative interaction and personal control. J. Health Soc. Behav. 2003, 44, 390–407. [Google Scholar] [CrossRef]
- Krause, N. Church-based social support and health in old age: Exploring variations by race. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, S332–S347. [Google Scholar] [CrossRef]
- Sonnenberg, C.M.; Deeg, D.J.; van Tilburg, T.G.; Vink, D.; Stek, M.L.; Beekman, A.T. Gender differences in the relation between depression and social support in later life. Int. Psychogeriatr. 2013, 25, 61–70. [Google Scholar] [CrossRef]
- Sacco, P.; Bucholz, K.K.; Harrington, D. Gender differences in stressful life events, social support, perceived stress, and alcohol use among older adults: Results from a National Survey. Subst. Use Misuse 2014, 49, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Tanaka, Y. Gender differences in the relationship between social support and subjective health among elderly persons in Japan. Prev. Med. 2004, 38, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Landman-Peeters, K.M.; Hartman, C.A.; van der Pompe, G.; den Boer, J.A.; Minderaa, R.B.; Ormel, J. Gender differences in the relation between social support, problems in parent-offspring communication, and depression and anxiety. Soc. Sci. Med. 2005, 60, 2549–2559. [Google Scholar] [CrossRef]
- Honjo, K.; Kawakami, N.; Takeshima, T.; Tachimori, H.; Ono, Y.; Uda, H.; Hata, Y.; Nakane, Y.; Nakane, H.; Iwata, N.; et al. Social class inequalities in self-rated health and their gender and age group differences in Japan. J. Epidemiol. 2006, 16, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Brettschneider, C.; Lange, C.; Posselt, T.; Wiese, B.; Steinmann, S.; Weyerer, S.; Werle, J.; Pentzek, M.; Fuchs, A.; et al. Gender differences in the effect of social support on health-related quality of life: Results of a population-based prospective cohort study in old age in Germany. Qual. Life Res. 2016, 25, 1159–1168. [Google Scholar] [CrossRef]
- Cross, C.J.; Taylor, R.J.; Chatters, L.M. Ethnic and Gender Differences in Family Social Support among Black Adolescents. Healthcare 2018, 6, 20. [Google Scholar] [CrossRef]
- Cheng, S.T.; Chan, A.C. Social support and self-rated health revisited: Is there a gender difference in later life? Soc. Sci. Med. 2006, 63, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Kanaan, C.; Beydoun, H.; Chaaya, M.; Kanaan, M.; Sibai, A.M. The role of gender in the association of social capital, social support, and economic security with self-rated health among older adults in deprived communities in Beirut. Qual. Life Res. 2013, 22, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Caetano, S.C.; Silva, C.M.; Vettore, M.V. Gender differences in the association of perceived social support and social network with self-rated health status among older adults: A population-based study in Brazil. BMC Geriatr. 2013, 13, 122. [Google Scholar] [CrossRef]
- Berard, D.M.; Vandenkerkhof, E.G.; Harrison, M.; Tranmer, J.E. Gender differences in the influence of social support on one-year changes in functional status in older patients with heart failure. Cardiol. Res. Pract. 2012, 2012, 616372. [Google Scholar] [CrossRef] [PubMed]
- Bartley, M.; Martikainen, P.; Shipley, M.; Marmot, M. Gender differences in the relationship of partner’s social class to behavioural risk factors and social support in the Whitehall II study. Soc. Sci. Med. 2004, 59, 1925–1936. [Google Scholar] [CrossRef] [PubMed]
- Cobb, S.; Assari, S. Self-Rated Health in African American Men and Women; Evidence for Sponge Hypothesis. Int. J. Environ. Res. Public Health. 2019. Under Review. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| All n = 740 | African American Men n = 262 | African American Women n = 474 | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age * | 71.73 | 8.37 | 70.79 | 8.32 | 72.26 | 8.36 |
| Educational Attainment * | 12.74 | 2.24 | 12.42 | 2.51 | 12.93 | 2.06 |
| Number of CMCs (Multimorbidity) * | 3.86 | 1.86 | 3.58 | 1.88 | 4.03 | 1.83 |
| Depression | 2.47 | 2.77 | 2.53 | 2.76 | 2.43 | 2.79 |
| Self-Rated Health (SRH) | 3.13 | 1.02 | 3.12 | 1.09 | 3.14 | 0.97 |
| n | % | n | % | n | % | |
| Married * | ||||||
| No | 640 | 86.5 | 215 | 80.8 | 425 | 89.7 |
| Yes | 100 | 13.5 | 51 | 19.2 | 49 | 10.3 |
| Living Alone * | ||||||
| No | 294 | 39.7 | 121 | 45.5 | 173 | 36.5 |
| Yes | 446 | 60.3 | 145 | 54.5 | 301 | 63.5 |
| Characteristics | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| All | ||||||||
| 1 Gender (Female) | 1 | 0.08 * | 0.11 ** | −0.12 ** | 0.09 * | 0.12 ** | −0.02 | 0.01 |
| 2 Age | −0.18 ** | −0.00 | 0.06 | −0.02 | −0.25 ** | −0.22 ** | ||
| 3 Education | 1 | 0.06 | −0.04 | −0.09 * | −0.07 | −0.03 | ||
| 4 Married | 1 | −0.41 ** | −0.02 | −0.07 | −0.08 * | |||
| 5 Living alone | 1 | 0.09 * | 0.12 ** | 0.08 * | ||||
| 6 Number of CMCs (Multimorbidity) | 1 | 0.32 ** | 0.27 ** | |||||
| 7 Depression | 1 | 0.37 ** | ||||||
| 8 Self-Rated Health (SRH) | 1 | |||||||
| AA Men | ||||||||
| 2 Age | 1 | −0.25 ** | 0.01 | −0.04 | −0.06 | −0.23 ** | −0.28 ** | |
| 3 Education | 1 | 0.16 ** | −0.10 | −0.07 | −0.06 | −0.04 | ||
| 4 Married | 1 | −0.48 ** | −0.03 | −0.10 | −0.11 | |||
| 5 Living alone | 1 | 0.10 | 0.15 * | 0.12 | ||||
| 6 Number of CMCs (Multimorbidity) | 1 | 0.38 ** | 0.19 ** | |||||
| 7 Depression | 1 | 0.30 ** | ||||||
| 8 Self-Rated Health (SRH) | ||||||||
| AA Women | ||||||||
| 2 Age | 1 | −0.16 ** | 0.00 | 0.10 * | −0.01 | −0.27 ** | −0.19 ** | |
| 3 Education | 0.01 | −0.02 | −0.12 ** | −0.07 | −0.03 | |||
| 4 Married | 1 | −0.35 ** | 0.02 | −0.05 | −0.06 | |||
| 5 Living alone | 1 | 0.06 | 0.11 * | 0.05 | ||||
| 6 Number of CMCs (Multimorbidity) | 1 | 0.29 ** | 0.32 ** | |||||
| 7 Depression | 1 | 0.41 ** | ||||||
| 8 Self-Rated Health (SRH) | 1 |
| Characteristics | Estimate (S.E.) | p |
|---|---|---|
| → Depression | ||
| Gender (female) | −0.19 (0.20) | 0.340 |
| Marital status (married) | −0.17 (0.30) | 0.559 |
| Number of CMCs (multimorbidity) | 0.45 (0.05) | <0.001 |
| Living alone | 0.57 (0.21) | 0.006 |
| Age | −0.09 (0.01) | <0.001 |
| Education | −0.10 (0.04) | 0.022 |
| → Self-Rated Health (SRH) | ||
| Gender (female) | 0.02 (0.07) | 0.795 |
| Age | −0.02 (0.00) | <0.001 |
| Number of CMCs (multimorbidity) | 0.10 (0.02) | <0.001 |
| Depression | 0.10 (0.01) | <0.001 |
| Characteristics | Estimate (S.E.) | p | Estimate (S.E.) | p |
|---|---|---|---|---|
| Men | Women | |||
| → Depression | ||||
| Marital status (married) | −0.25 (0.44) | 0.571 | −0.13 (0.41) | 0.752 |
| Number of CMCs (multimorbidity) | 0.51 (0.08) | <0.001 | 0.41 (0.06) | <0.001 |
| Living alone | 0.45 (0.35) | 0.193 | 0.65 (0.26) | 0.012 |
| Age | −0.07 (0.02) | <0.001 | −0.10 (0.01) | <0.001 |
| → Self-Rated Health (SRH) | ||||
| Education | −0.09 (0.06) | 0.162 | −0.10 (0.06) | 0.078 |
| Age | −0.03 (0.01) | <0.001 | −0.01 (0.01) | 0.021 |
| Number of CMCs (multimorbidity) | 0.06 (0.04) | 0.115 | 0.12 (0.02) | <0.001 |
| Depression | 0.09 (0.03) | <0.001 | 0.11 (0.02) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assari, S.; Smith, J.; Bazargan, M. Depression Fully Mediates the Effect of Multimorbidity on Self-Rated Health for Economically Disadvantaged African American Men but Not Women. Int. J. Environ. Res. Public Health 2019, 16, 1670. https://doi.org/10.3390/ijerph16101670
Assari S, Smith J, Bazargan M. Depression Fully Mediates the Effect of Multimorbidity on Self-Rated Health for Economically Disadvantaged African American Men but Not Women. International Journal of Environmental Research and Public Health. 2019; 16(10):1670. https://doi.org/10.3390/ijerph16101670
Chicago/Turabian StyleAssari, Shervin, James Smith, and Mohsen Bazargan. 2019. "Depression Fully Mediates the Effect of Multimorbidity on Self-Rated Health for Economically Disadvantaged African American Men but Not Women" International Journal of Environmental Research and Public Health 16, no. 10: 1670. https://doi.org/10.3390/ijerph16101670
APA StyleAssari, S., Smith, J., & Bazargan, M. (2019). Depression Fully Mediates the Effect of Multimorbidity on Self-Rated Health for Economically Disadvantaged African American Men but Not Women. International Journal of Environmental Research and Public Health, 16(10), 1670. https://doi.org/10.3390/ijerph16101670