The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Participants
2.3. Measurements
2.3.1. Blood Pressure
2.3.2. Peak Oxygen Uptake
2.3.3. Heart Rate Variability
2.4. Exercise Interventions
2.5. Data Analysis
3. Results
3.1. Training Information
3.2. Changes in Blood Pressure
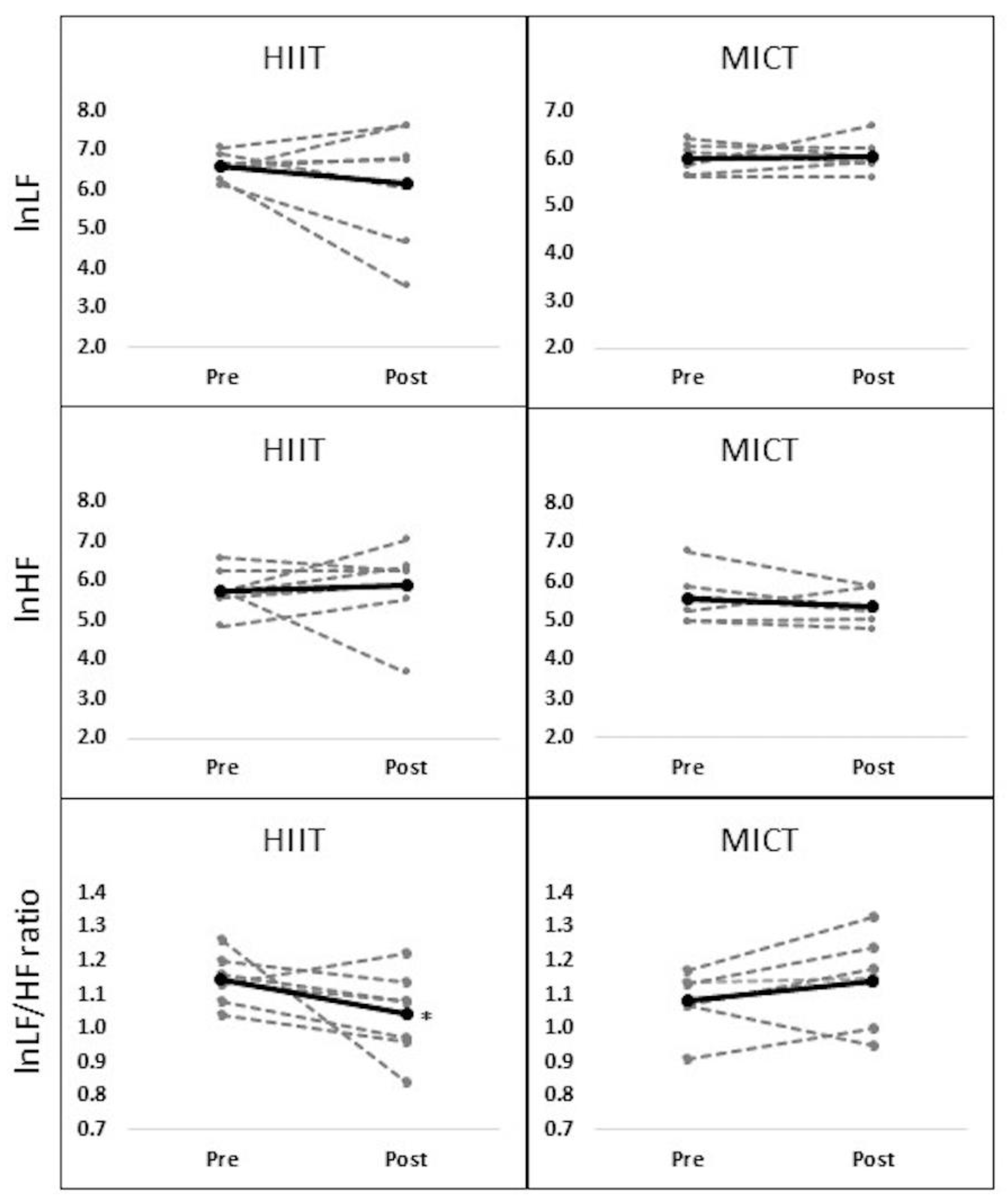
3.3. Changes in Heart Rate Variability
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Dumith, S.C.; Hallal, P.C.; Reis, R.S.; Kohl, H.W. Worldwide prevalence of physical inactivity and its association with human development index in 76 countries. J. Prev. Med. 2011, 53, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Clarke, T.C.; Ward, B.W.; Norris, T.; Schiller, J.S. Early release of selected estimates based on data from the January–September 2016 National Health Interview Survey; Center for Disease Control and Prevention: Atlanta, GA, USA, 2017; pp. 1–120. [Google Scholar]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, 1–68. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.T.; Wareham, N.; Bingham, S.; Welch, A.; Luben, R.; Day, N. Combined impact of health behaviors and mortality in men and women: the EPIC-Norfolk prospective population study. PLoS Med. 2008, 5, e12. [Google Scholar]
- US Department of Health and Human Services. 2008 physical activity guidelines for Americans. 2008. Available online: http://www. health.gov/paguidelines/ (accessed on 12 March 2018).
- Mullahy, J.; Robert, S.A. No time to lose: Time constraints and physical activity in the production of health. Rev. Econ. Househ. 2010, 8, 409–432. [Google Scholar] [CrossRef]
- Petersen, B.A.; Hastings, B.; Gottschall, J.S. High intensity interval cycling improves physical fitness in trained adults. J. Fitness Res. 2016, 5, 39–47. [Google Scholar]
- Ramírez-Vélez, R.; Tordécilla-Danders, A.; Tellez-T, L.A.; Camelo-Prieto, D.; Hernández-Quiňonez, P.A.; Correa-Bautista, J.E.; Garcia-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Effect of moderate versus high-intensity interval exercise training on heart rate variability parameters in inactive Latin American adults: a randomized clinical trial. J. Strength Cond. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Fan, X.; Sun, S.; Song, L.; Shi, Q.; Nie, J. Comparison of high-intensity interval training and moderate-to-vigorous continuous training for cardiometabolic health and exercise enjoyment in obese young women: A randomized controlled trial. PLoS ONE 2016, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology. Heart rate variability, standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Williams, D.P.; Cash, C.; Rankin, C.; Bernardi, A.; Koenig, J.; Thayer, J.F. Resting heart rate variability predicts self-reported difficulties in emotion regulation: A focus on different facets of emotion regulation. Front. Psychol. 2015, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guiraud, T.; Labrunee, M.; Gaucher-Cazalis, K.; Despas, F.; Meyer, P.; Osquet, L.; Gales, C.; Vaccaro, A.; Bousquet, M.; Galinier, M.; et al. High-intensity interval exercise improves vagal tone and decreases arrhythmias in chronic heart failure. Med. Sci. Sports. Exerc. 2013, 45, 1861–1867. [Google Scholar] [CrossRef] [PubMed]
- Munk, P.S.; Butt, N.; Larsen, A.I. High-intensity interval exercise training improves heart rate variability in patients following percutaneous coronary intervention for angina pectoris. Int. J. Cardiol. 2010, 145, 312–314. [Google Scholar] [CrossRef] [PubMed]
- Jurca, R.; Church, T.S.; Morss, G.M.; Jordan, A.N.; Earnest, C.P. Eight weeks of moderate-intensity exercise training increases heart rate variability in sedentary postmenopausal women. Am. Heart J. 2004, 147, e8–e15. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; Wood, R.; Welsch, M. Influence of short-term endurance exercise training on heart rate variability. Med. Sci. Sports Exerc. 2002, 34, S40. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2017. [Google Scholar]
- Bridget, A. Actiwave Cardio: The feasibility and validation of an innovative new ambulatory monitoring device. In Proceedings of the Australian Cardiovascular Health and Rehabilitation Association, Brisbane, Australia, 14 August 2012. [Google Scholar]
- Thompson, A.G.; Swain, D.P.; Branch, J.D.; Spina, R.J.; Grieco, C.R. Autonomic response to tactical pistol performance measured by heart rate variability. J. Strength Cond. Res. 2015, 29, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Lanzi, S.; Codecasa, F.; Cornacchia, M.; Maestrini, S.; Capodaglio, P.; Brunani, A.; Fanari, P.; Salvadori, A.; Malatesta, D. Short-tern HIIT and fatmax training increase aerobic and metabolic fitness in men with class II and III obesity. Obesity 2015, 23, 1987–1994. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Whyte, L.J.; Gill, J.M.; Cathcart, A.J. Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metab. Clin. Exp. 2010, 59, 1421–1438. [Google Scholar] [CrossRef] [PubMed]
- Ketelhut, S.; Milatz, F.; Heise, W.; Ketelhut, R.G. Influence of a high-intensity interval training session on peripheral and central blood pressure at rest and during stress testing in healthy individuals. Vasa 2016, 45, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Collier, S.R.; Kanaley, J.A.; Carhart, J.R.; Frechette, V.; Tobin, M.M.; Hall, A.K.; Luckenbaugh, A.N.; Fernhall, B. Effect of 4 weeks of aerobic or resistance exercise training on arterial stiffness, blood flow and blood pressure in pre-and stage-1 hypertensives. J. Hum. Hypertens. 2008, 22, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Fernhall, B. Advanced Cardiovascular Exercise Physiology; Human Kinetics: Champaign, IL, USA, 2011. [Google Scholar]
- Currie, K.D.; McKelvie, R.S.; MacDonald, M.J. Flow-mediated dilation is acutely improved after high-intensity interval exercise. Med. Sci. Sports Exerc. 2012, 44, 2057–2064. [Google Scholar] [CrossRef] [PubMed]
- Landers-Ramos, R.Q.; Corrigan, K.J.; Guth, L.M.; Altom, C.N.; Spangenburg, E.E.; Prior, S.J.; Hagberg, J.M. Short-term exercise training improves flow-mediated dilation and circulating angiogenic cell number in older sedentary adults. Appl. Physiol. Nutr. Metab. 2016, 41, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Goit, R.K.; Paudel, B.H.; Khadka, R.; Roy, R.K.; Shrewastwa, M.K. Mild-to-moderate intensity exercise improves cardiac autonomic drive in type 2 diabetes. J. Diabetes Investig. 2014, 5, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Earnest, C.P.; Lavie, C.J.; Blair, S.N.; Church, T.S. Heart rate variability characteristics in sedentary postmenopausal women following six months of exercise training: the DREW study. PLoS ONE 2008, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Leicht, A.S.; Allen, G.D.; Hoey, A.J. Influence of age and moderate-intensity exercise training on heart rate variability in young and mature adults. Can. J. Appl. Physiol. 2003, 28, 446–461. [Google Scholar] [CrossRef] [PubMed]
- Nummela, A.; Hynynen, E.; Kaikkonen, P.; Rusko, H. Endurance performance and nocturnal HRV indices. Int. J. Sports Med. 2009, 31, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, K.; Iwasaki, K.I.; Prasad, A.; Palmer, M.D.; Martini, E.R.; Fu, Q.; Arbab-Zadeh, A.; Zhang, R.; Levine, B.D. Dose-response relationship of endurance training for autonomic circulatory control in healthy seniors. J. Appl. Physiol. 2005, 99, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Boutcher, S.H. High-intensity intermittent exercise and fat loss. J. Obes. 2011, 2011, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hani, A.H.; Laursen, P.B.; Said, A.; Martin, B. Nocturnal heart rate variability following supramaximal intermittent exercise. Int. J. Sports Physiol. Perform. 2009, 4, 435–447. [Google Scholar] [CrossRef]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Fleg, J.L.; O’connor, F.; Gerstenblith, G.; Becker, L.C.; Clulow, J.; Schulman, S.P.; Lakatta, E.G. Impact of age on the cardiovascular response to dynamic upright exercise in healthy men and women. J. Appl. Phsiol. 1995, 78, 890–900. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Allen, R.P.; Roberson, D.W.; Jurancich, M.; Lewis, R.; McCarthy, K.; Trost, E. Adaptations to high-intensity training are independent of gender. Eur. J. Appl. Physiol. 2011, 111, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.E. Heart rate and blood pressure responses to exercise testing in relation to age in healthy men. Iraqi Postgrad. Med. J. 2009, 1, 14–20. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Mean ± SD |
|---|---|
| Age (yrs) | 27.5 ± 3.80 |
| Height (cm) | 173.9 ± 8.56 |
| Body weight (kg) | 90.2 ± 19.24 |
| Body mass index (kg/m2) | 29.7 ± 5.89 |
| Waist-hip ratio | 0.8 ± 0.03 |
| Systolic BP (mmHg) | 123.5 ± 4.60 |
| Diastolic BP (mmHg) | 75.4 ± 5.67 |
| HRrest (beat/min) | 67.5 ± 10.67 |
| HRpeak (beat/min) | 174.6 ± 20.72 |
| VO2peak (ml/kg/min) | 29.8 ± 6.40 |
| HIIT | MICT | |
|---|---|---|
| Completed session (n) | 8 | 8 |
| Exercise load (kp) | 5.0 ± 2.33 * | 1.2 ± 0.21 |
| Average heart rate (beat/min) | 159.8 ± 12.33 * | 139.3 ± 17.35 |
| Average RPE (score) | 15.6 ± 1.30 * | 11.0 ± 2.70 |
| Total exercise duration (min) | 159.4 ± 1.15 * | 305.4 ± 27.29 |
| PRE | POST | Group | Time | G × T | ||
|---|---|---|---|---|---|---|
| SYS BP (mmHg) | HIIT | 123.7 ± 4.57 | 118.0 ± 3.94 + | 0.726 | 14.495 * | 0.128 |
| MICT | 122.3 ± 5.11 | 115.4 ± 6.34 + | ||||
| DIA BP (mmHg) | HIIT | 73.6 ± 2.40 | 70.9 ± 6.6 | 0.651 | 2.148 | 0.007 |
| MICT | 75.5 ± 6.49 | 72.5 ± 3.59 |
| PRE | POST | Group | Time | G × T | ||
|---|---|---|---|---|---|---|
| R-R Intervals (n) | HIIT | 304.7 ± 36.49 | 286.0 ± 49.06 + | 4.035 | 8.437 * | 0.534 |
| MICT | 348.3 ± 23.15 | 318 ± 30.48 + | ||||
| IBI (sec) | HIIT | 1.0 ± 0.11 | 1.1 ± 0.17 + | 4.575 | 9.611 * | 0.032 |
| MICT | 0.9 ± 0.06 | 0.9 ± 0.09 + | ||||
| RMSSD | HIIT | 0.1 ± 0.02 | 0.1 ± 0.02 | 2.057 | 0.214 | 1.536 |
| MICT | 0.1 ± 0.04 | 0.1 ± 0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alansare, A.; Alford, K.; Lee, S.; Church, T.; Jung, H.C. The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. Int. J. Environ. Res. Public Health 2018, 15, 1508. https://doi.org/10.3390/ijerph15071508
Alansare A, Alford K, Lee S, Church T, Jung HC. The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. International Journal of Environmental Research and Public Health. 2018; 15(7):1508. https://doi.org/10.3390/ijerph15071508
Chicago/Turabian StyleAlansare, Abdullah, Ken Alford, Sukho Lee, Tommie Church, and Hyun Chul Jung. 2018. "The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults" International Journal of Environmental Research and Public Health 15, no. 7: 1508. https://doi.org/10.3390/ijerph15071508
APA StyleAlansare, A., Alford, K., Lee, S., Church, T., & Jung, H. C. (2018). The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. International Journal of Environmental Research and Public Health, 15(7), 1508. https://doi.org/10.3390/ijerph15071508