Spatial Analysis of Socio-Economic and Demographic Factors Associated with Contraceptive Use among Women of Childbearing Age in Rwanda

Abstract
1. Introduction
2. Materials and Methods
2.1. Source of Data
2.1.1. Outcome Variable
2.1.2. Independent Variables
2.2. Statistical Model
2.2.1. Parameter Estimation
2.2.2. Posterior and Inferences
2.2.3. Model Selection
2.2.4. Model Building
3. Results
3.1. Descriptive Analysis
3.2. Fixed Effect
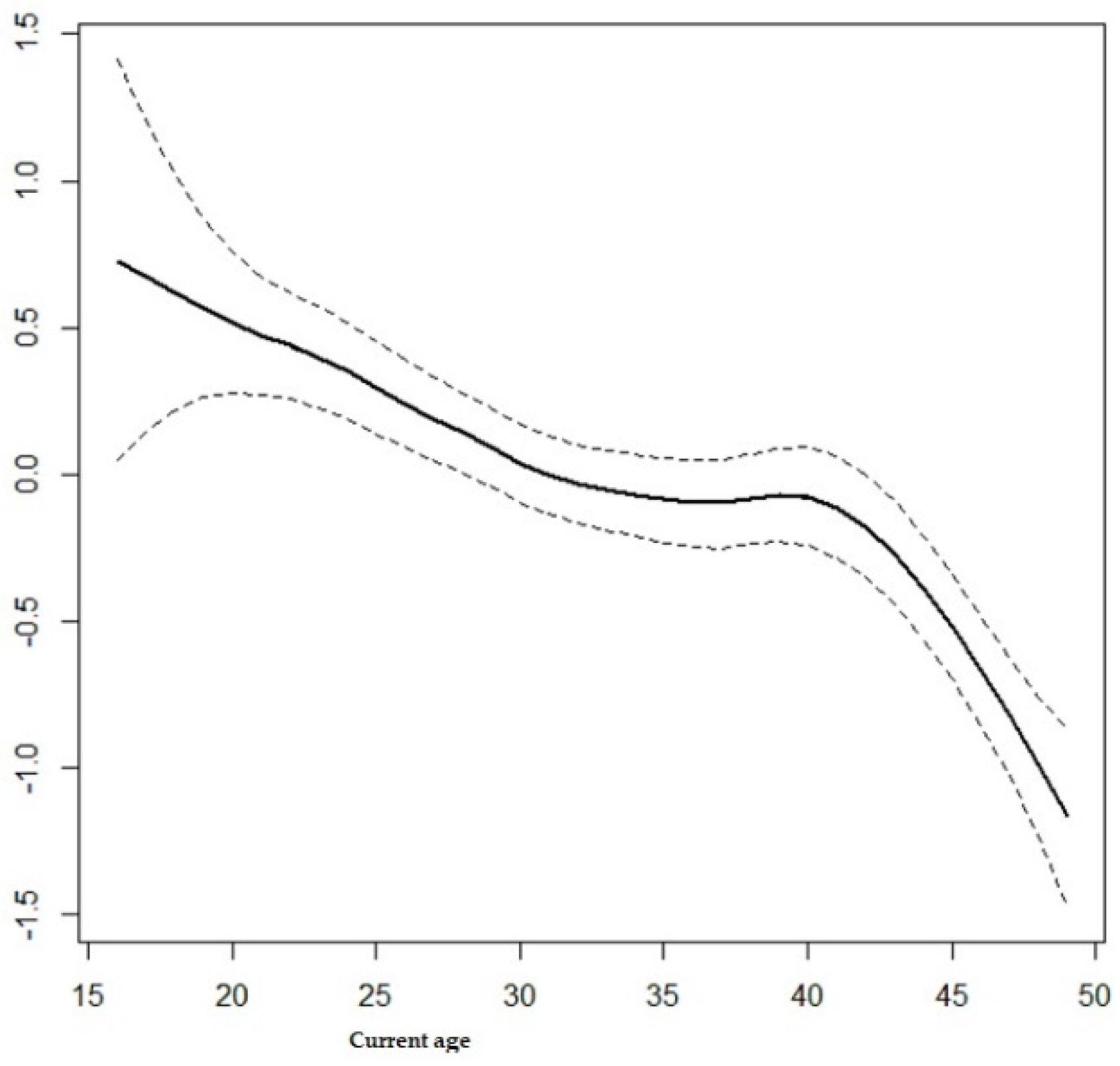
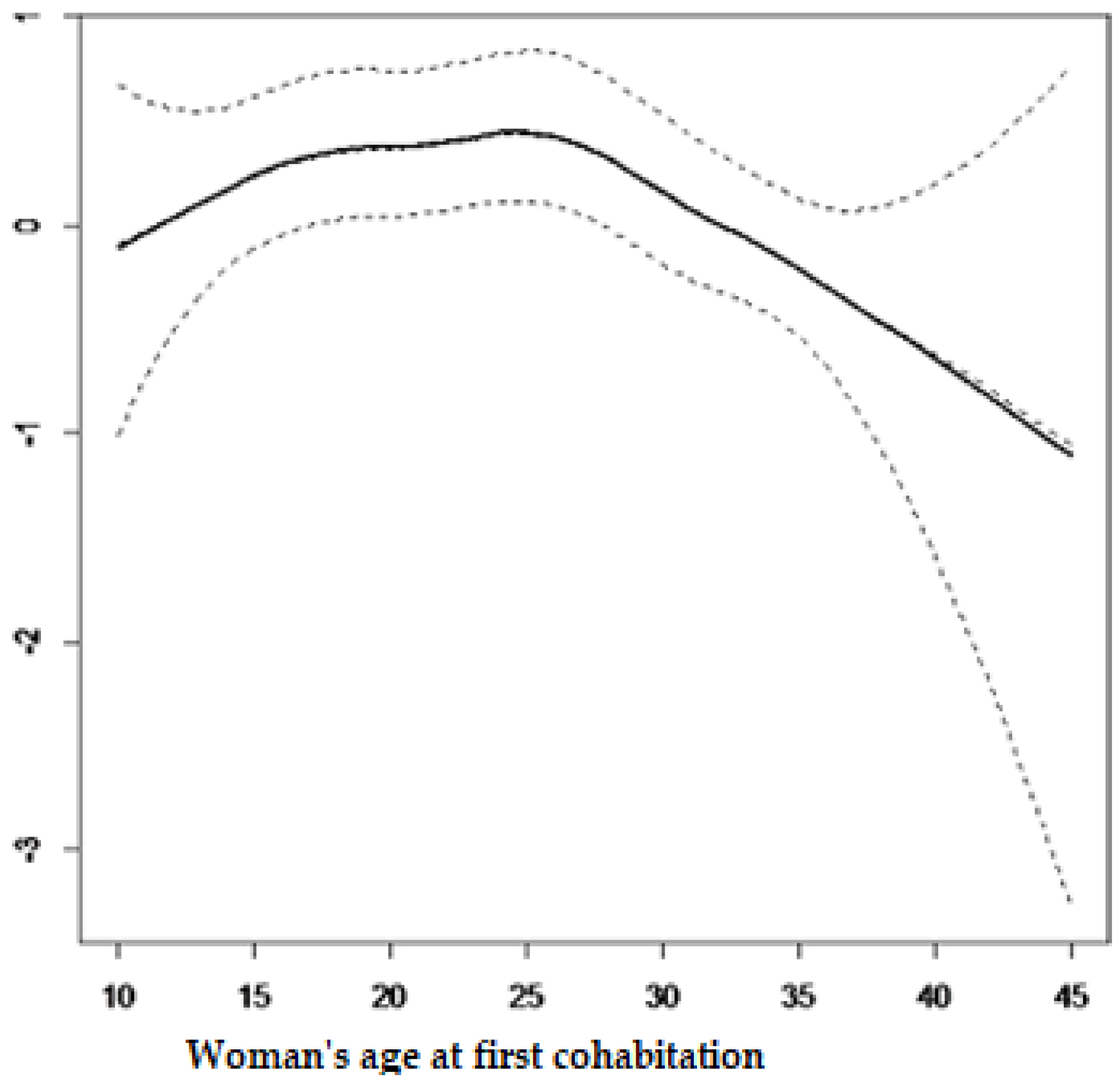
3.3. Non-Linear Effect
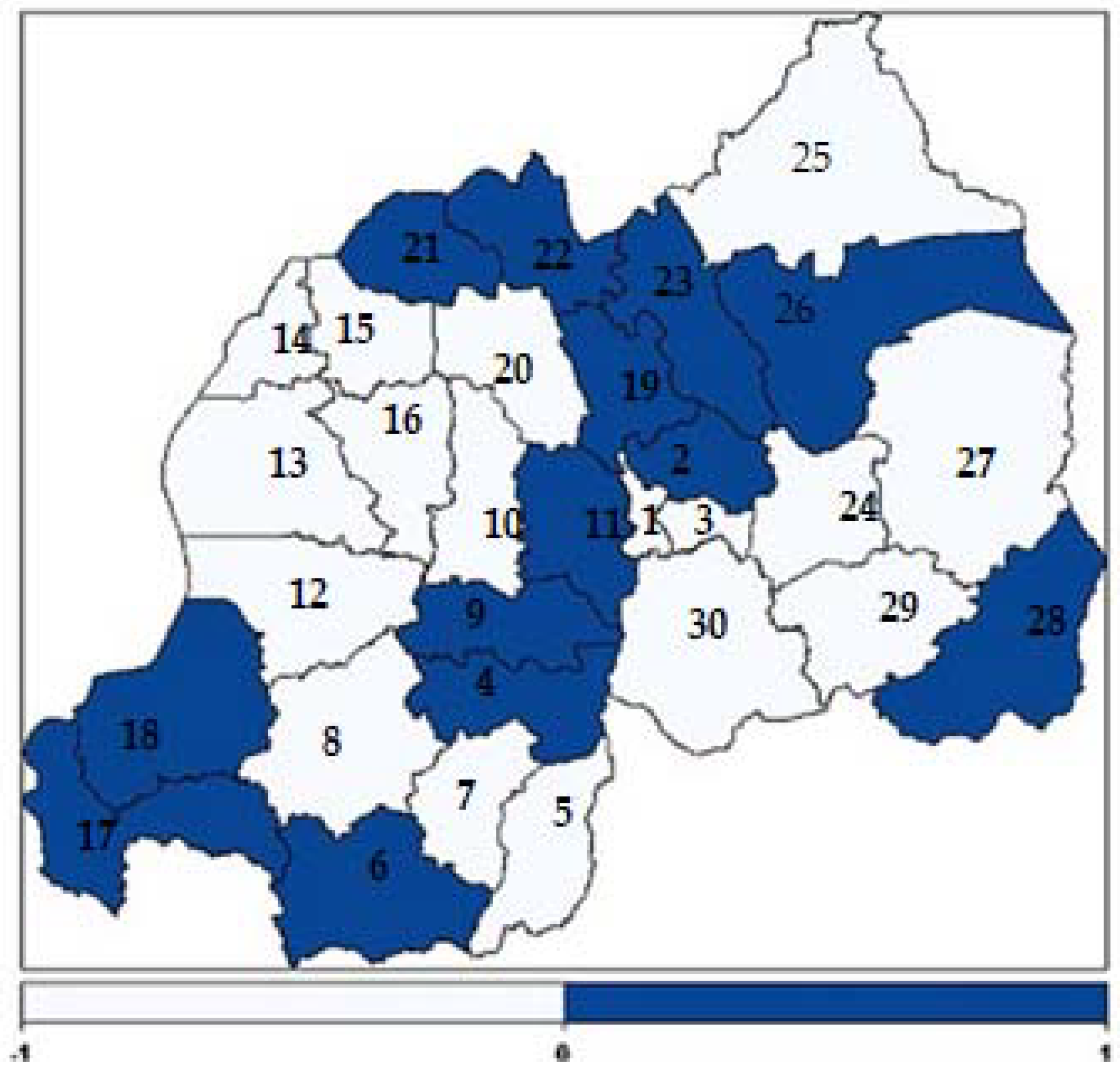
3.4. Spatial Effects
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Kayode, G.A.; Adekanmbi, V.T.; Uthman, O.A. Risk factors and a predictive model for under-five mortality in Nigeria: Evidence from Nigeria demographic and health survey. BMC Pregnancy Childbirth 2012, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Palloni, A.; Pinto Aguirre, G.; Lastiri, S. The effects of breast-feeding and the pace of childbearing on early childhood mortality in Mexico. Bull. Pan. Am. Health Organ. 1994, 28, 93–111. [Google Scholar] [PubMed]
- Westoff, C.F. Unmet Need at the End of the Century; DHS Comparative Reports No. 1; ORC Macro. Inc.: Calverton, MD, USA, 2001. [Google Scholar]
- Sinding, S.W.; Ross, J.A.; Rosenfield, A.G. Seeking common ground: Unmet need and demographic goals. Int. Fam. Plan. Perspect. 1994, 1, 23–32. [Google Scholar] [CrossRef]
- Blanc, A.K.; Tsui, A.O.; Croft, T.N.; Trevitt, J.L. Patterns and trends in adolescents’ contraceptive use and discontinuation in developing countries and comparisons with adult women. Int. Perspect. Sex. Reprod. Health 2009, 35, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Bernstein, S.; Ezeh, A.; Foundes, A.; Glasier, A.; Innis, J. Family planning: The unfinished agenda. Lancet 2006, 368, 1810–1827. [Google Scholar] [CrossRef]
- Singh, S.; Darroch, J.E. Adding it up: Costs and Benefits of Contraceptive Services; Guttmacher Institute and UNFPA: New York, NY, USA, 2012. [Google Scholar]
- National Institute of Statistics of Rwanda (NISR) [Rwanda]; Ministry of Health(MoH) [Rwanda]; ICF International. Rwanda Demographic and Health Survey 2014–15; NISR: Rockville, MD, USA; MoH: Rockville, MD, USA; ICF International: Rockville, MD, USA, 2015.
- KNBS. Kenya Demographic and Health Survey 2008–09; KNBS: Nairobi, Kenya, 2010. [Google Scholar]
- Ministry of Health, Community Development; Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland]; Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS); Office of the Chief Government Statistician (OCGS); ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015–16; MoHCDGEC: Dar es Salaam, Tanzania; Rockville, MD, USA; MoH: Dar es Salaam, Tanzania; Rockville, MD, USA; NBS: Dar es Salaam, Tanzania; Rockville, MD, USA; OCGS: Dar es Salaam, Tanzania; Rockville, MD, USA; ICF: Dar es Salaam, Tanzania; Rockville, MD, USA, 2016.
- UBOS; ICF International Inc. Uganda Demographic and Health Survey 2011; Uganda Bureau of Statistics: Kampala, Uganda; ICF International Inc.: Claverton, UK, 2012. [Google Scholar]
- Ministère à la présidence chargé de la Bonne Gouvernance et du Plan[Burundi] (MPBGP); Ministère de la santé Publique et de la lutte contre le sida [Burundi] (MSPLS); Institut de Statistiques et d’Etudes Economiques du Burundi (ISTEEBU), et ICF International. Triosième Enquête Démographique et de Santé; ISTEEBU, MSPLS, et ICF International: Bujumbura, Burundi, 2017.
- Wang, W.; Alva, S.; Winter, R.; Burgert, C. Contextual Influences of Modern Contraceptive Use among Rural Women in Rwanda and Nepal, DHS Analytical Studies No 41; ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- Brunie, A.; Tolley, E.E.; Ngabo, F.; Wesson, J.; Chen, M. Getting to 70%: Barriers to modern contraceptive use for women in Rwanda. Int. J. Gynecol. Obstet. 2013, 123, e11–e15. [Google Scholar] [CrossRef] [PubMed]
- Frederic, T.M.; Phoibe, K.; Ntaganira, J. Assessment of Knowledge, Attitudes, and Practice on Contraceptive Use among Women Attending Family Planning Services in Some Health Centers of Muhima District Hospital, Rwanda. Open Sci. J. 2017, 2. [Google Scholar] [CrossRef]
- Adeyemi, A.S.; Olugbenga-Bello, A.I.; Adeoye, O.; Salawu, M.; Aderinoye, A.; Agbaje, M. Contraceptive prevalence and determinants among women of reproductive age group in Ogbomoso, Oyo state, nigeria. Open Access J. Contracept. 2016, 7, 33–41. [Google Scholar] [PubMed]
- Hailu, T.G. Determinants and Cross-Regional Variations of Contraceptive Prevalence Rate in Ethiopia: A Multilevel Modeling Approach. Am. J. Math. Stat. 2015, 5, 95–110. [Google Scholar]
- Nonvignon, J.; Novignon, J. Trend and determinants of contraceptive use among women of reproductive age in Ghana. Etude De La Popul. Afr. 2014, 28, 956–967. [Google Scholar] [CrossRef]
- Osmani, A.K.; Reyer, J.A.; Osmani, A.R.; Hamajiman, N. Factors influencing contraceptive use among women in Afghanistan: Secondary analysis of Afghanistan Health Survey 2012. Nagoya J. Med Sci. 2015, 77, 551–561. [Google Scholar] [PubMed]
- Wecker, W.E.; Ansley, C.F. The signal extraction approach to nonlinear regression and spline smoothing. J. Am. Stat. Assoc. 1983, 78, 81–89. [Google Scholar] [CrossRef]
- Besag, J.; Green, P.J. Spatial statistics and Bayesian computation. J. R. Stat. Soc. Ser. B (Methodol.) 1993, 55, 25–37. [Google Scholar]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van der Linde, A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. B 2002, 64, 583–639. [Google Scholar] [CrossRef]
- Best, N.; Richardson, S.; Thomson, A. A comparison of Bayesian spatial models for disease mapping. Stat. Methods Med. Res. 2005, 14, 35–59. [Google Scholar] [CrossRef] [PubMed]
- Okech, T.C.; Wawire, N.W.; Mburu, T.K. Contraceptive use among women of reproductive age in Kenya’s city slums. Int. J. Bus. Soc. Sci. 2011, 2, 22–43. [Google Scholar]
- Solanke, B.L. Factors influencing contraceptive use and non-use among women of advanced reproductive age in Nigeria. J. Heal. Popul. Nutr. 2017, 36, 1. [Google Scholar] [CrossRef] [PubMed]
- Nyarko, S.H. Prevalence and correlates of contraceptive use among female adolescents in Ghana. BMC Women’s Health 2015, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Tekelab, T.; Melka, A.S.; Wirtu, D. Predictors of modern contraceptive methods use among married women of reproductive age groups in Western Ethiopia: A community based cross-sectional study. BMC Women’s Health 2015, 15, 52. [Google Scholar] [CrossRef] [PubMed]
- Lasee, A.; McCormick, J.B. Demographic and socio-economic determinants of contraceptive use in a low income community of Karachi. J.-Pak. Med. Assoc. 1996, 46, 228–230. [Google Scholar] [PubMed]
- Hussain, N. Demographic, Socio-Economic and Cultural Factors Affecting Knowledge and Use of Contraception Differentials in Malda District, West Bengal. J. Community Med. Health Educ. 2011, 1, 2. [Google Scholar] [CrossRef]
- Anasel, M.G.; Mlinga, U.J. Determinants of contraceptive use among married women in Tanzania: Policy implication. Etude De La Popul. Afr. 2014, 28, 978–988. [Google Scholar] [CrossRef]
- Khraif, R.; Salam, A.A.; Elsegaey, I.; Ajumah, A. Dynamics of contraceptive use: A study of King Saud University women staff, Riyadh. Middle East Fertil. Soc. J. 2017, 22, 18–26. [Google Scholar] [CrossRef]
- Nketiah-Amponsah, E.; Arthur, E.; Abuosi, A. Correlates of contraceptive use among Ghanaian women of reproductive age (15–49 years). Afr. J. Reprod. Health 2012, 16, 154–169. [Google Scholar]
- Clements, S.; Madise, N. Who is being served least by family planning providers? A study of modern contraceptive use in Ghana, Tanzania and Zimbabwe. Afr. J. Reprod. Health 2004, 8, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Kayembe, P.K.; Fatuma, A.B.; Mapatano, M.A.; Mambu, T. Prevalence and determinants of the use of modern contraceptive methods in Kinshasa, Democratic Republic of Congo. Contraception 2006, 74, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Achana, F.S.; Jackson, E.F.; Welaga, P.; Awine, T.; Asuo-Mante, E.; Oduro, A.; Awoonor-William, J.K.; Phillips, J.F. Spatial and socio-demographic determinants of contraceptive use in the Upper East region of Ghana. Reprod. Health 2015, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Phillips, J.F.; Amin, S.; Kamal, G.M. The Determinants of Reproductive Change in Bangladesh; The World Bank: Washington, DC, USA, 1994. [Google Scholar]
- Stephenson, R.; Baschieri, A.; Clements, S.; Hennink, M.; Madise, N. Contextual influences on modern contraceptive use in sub-Saharan Africa. Am. J. Public Health 2007, 97, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Gayawan, E.; Arogundade, E.D.; Adebayo, S.B. Possible determinants and spatial patterns of anaemia among young children in Nigeria: A Bayesian semi-parametric modelling. Int. Health 2014, 6, 35–45. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Categories | % or M or Range |
|---|---|---|
| Current contraceptive use | Yes | 52.7 |
| No | 47.3 | |
| Respondent current age | Continuous | M = 32.81 (Minimum = 16, maximum = 49) |
| Age at first cohabitation | Continuous | M = 21.09 (Minimum = 10, Maximum = 95) |
| Place of residence | Urban | 17 |
| Rural | 83 | |
| Respondent education level | No education | 16.5 |
| Primary | 70.5 | |
| Secondary | 10.3 | |
| Tertiary | 2.7 | |
| Wealth index | Poorest | 18.8 |
| Poorer | 21.2 | |
| Middle | 20.9 | |
| Rich | 19.9 | |
| Richest | 19.3 | |
| Heard about family planning on the radio in last few months | Yes | 55 |
| No | 45 | |
| Heard about family planning on the TV in last few months | Yes | 7.1 |
| No | 92.8 | |
| Heard about family planning from newspapers/magazines in the last few months | Yes | 6.1 |
| No | 93.9 | |
| Visited by family planning worker in the last 12 months | Yes | 29.2 |
| No | 70.8 | |
| Visited health facility in the last 12 months | Yes | 71.8 |
| No | 28.2 | |
| At health facility, told of family planning | Yes | 46.3 |
| No | 53.7 | |
| Respondent currently working | Yes | 86.8 |
| No | 13.2 | |
| Husband/partner education level | No education | 16.9 |
| Primary | 70.1 | |
| Secondary | 9.2 | |
| Tertiary | 3.5 | |
| Do not know | 0.2 | |
| Number of living children | 0 | 5.2 |
| 1 | 17.9 | |
| 2 | 45.2 | |
| 3 | 17.4 | |
| 4 or more | 37.4 | |
| Religion | Catholic | 38.2 |
| Protestant | 45.6 | |
| Seventh Day Adventist | 12.8 | |
| Others | 3.2 |
| Current use by Method Type | N (%) |
|---|---|
| No method | 3237 (47.3) |
| Traditional method | 402 (5.9) |
| Modern method | 3208 (46.8) |
| Indicator Variable | Category | Contraceptive Use | p-Value | |
|---|---|---|---|---|
| No | Yes | |||
| Woman’s education level | No education | 596(52.7%) | 535(47.3%) | <0.001 |
| Primary | 2233(46.3%) | 2592(53.7%) | ||
| Secondary | 329(46.5%) | 379(53.5%) | ||
| Tertiary | 79(43.2%) | 104(56.8%) | ||
| Respondent currently working | Yes | 2755(46.4%) | 3183(53.6%) | <0.0001 |
| No | 481(53.0%) | 426(47.0%) | ||
| Heard about family planning | Yes | 1666(44.2%) | 2100(55.8%) | <0.0001 |
| on the radio in the last few months | No | 1571(51.0%) | 1509(49.0%) | |
| Heard about family planning | Yes | 150(36.1%) | 265(63.9%) | <0.0001 |
| from newspapers/magazines in the last 12 months | No | 3086(48.0%) | 3344(52.0%) | |
| Heard about family planning on TV in the last few months | Yes | 195(39.9%) | 294(60.1%) | 0.001 |
| No | 3042(47.9%) | 3314(52.1%) | ||
| Woman’s religious affiliation | Catholic | 1129(43.1%) | 1489(56.9%) | <0.0001 |
| Protestant | 1637(52.5%) | 1482(47.5%) | ||
| Seventh Day Adventist | 361(41.1%) | 517(58.9%) | ||
| Other | 103(46.6%) | 118(53.4%) | ||
| Visited by family planning worker in the last 12 months | Yes | 813(40.7%) | 1184(59.3%) | <0.0001 |
| No | 2424(50.0%) | 2426(50.0%) | ||
| Visited health facility in the last 12 months | Yes | 2379(48.4%) | 2539(51.6%) | 0.004 |
| No | 858(44.5%) | 1071(55.5%) | ||
| At health facility, told about family planning | Yes | 1081(47.5%) | 1194(52.5%) | 0.265 |
| No | 1298(49.1%) | 1345(50.9%) | ||
| Household wealth index | Poorest | 667(51.7%) | 622(48.3%) | <0.0001 |
| Poorer | 730(50.4%) | 719(49.6%) | ||
| Middle | 654(45.8%) | 774(54.2%) | ||
| Rich | 599(44.1%) | 760(55.9%) | ||
| richest | 586(44.4%) | 735(55.6%) | ||
| Place of residence | Urban | 516(44.3%) | 648(55.7%) | 0.028 |
| Rural | 2720(47.9%) | 2962(52.7%) | ||
| Number of living children | 0 | 349(98.3%) | 6(1.7%) | <0.0001 |
| 1 | 607(49.6%) | 618(50.4%) | ||
| 2 | 498(42.7%) | 867(57.3%) | ||
| 3 | 1137(4.3%) | 1427(55.7%) | ||
| Husband/partner desires children | Same number | 430(51.9%) | 398(48.1%) | <0.0001 |
| More | 1886(45.5%) | 2261(54.5%) | ||
| Fewer | 563(46.0%) | 660(54.0%) | ||
| Do not know | 358(55.2%) | 290(44.8%) | ||
| Husband/partner education | No education | 601(51.9%) | 558(48.1%) | 0.018 |
| Primary | 2222(46.3%) | 2579(53.7%) | ||
| Secondary | 295(47.0%) | 333(53.0) | ||
| Tertiary | 111(45.2%) | 132(54.2%) | ||
| Don’t know | 6(50.0) | 6(50.0%) | ||
| Statistics | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| DIC | 8488.64 | 8560.34 | 8465.45 | 8462.39 |
| 8428 | 8486.14 | 8388 | 8362.12 | |
| pD | 29.92 | 37.10 | 38.73 | 50.133 |
| Variable | Posterior Estimate of the Mean | Posterior Standard Error | Odds Ratio | 95% Credible Interval (CI) |
|---|---|---|---|---|
| Intercept | −5.3585 | 0.4743 | 0.0047 | (0.0017 0.0112) |
| Woman’s education (No education = reference) | 1.0000 | |||
| Tertiary | 0.5841 | 0.1909 | 1.7934 | (1.2355 2.61300) |
| Secondary | 0.3157 | 0.1193 | 1.3371 | (1.0853 1.7331) |
| Primary | 0.1600 | 0.0752 | 1.1735 | 1.0125 1.3599) |
| Wealth quintile (Poorest = reference) | 1.0000 | |||
| Richest | 0.3598 | 0.1023 | 1.4330 | (1.1727 1.7517) |
| Richer | 0.2998 | 0.0887 | 1.3496 | (1.1340 1.6063) |
| Middle | 0.2201 | 0.0857 | 1.2462 | (1.0533 1.4745) |
| Poorer | 0.0703 | 0.0834 | 1.0728 | (0.9107 1.2636) |
| Visited health facility in the last 12 months (No = reference) | ||||
| Yes | 0.1960 | 0.0598 | 1.2165 | (1.0820 1.3681) |
| Currently residing with husband (Living = reference) | ||||
| Stays elsewhere | −0.5811 | 0.0882 | 0.5593 | (0.4702 0.6647) |
| Number of living children (4 and more = reference) | ||||
| 3 | −0.1217 | 0.0837 | 0.8854 | (0.7512 1.0435) |
| 2 | −0.3055 | 0.0935 | 0.7368 | (0.6131 0.8848) |
| 1 | −0.8057 | 0.1176 | 0.4468 | (0.3544 0.5625) |
| 0 | −4.9371 | 0.4299 | 0.0072 | (0.0029 0.0156) |
| Religion (Others = reference) | ||||
| Catholic | −03459 | 0.0585 | 0.7047 | (0.6308 0.7936) |
| Protestant | 0.1338 | 0.0854 | 1.1432 | (0.967 1.3523) |
| Seventh Day Adventist | 0.0211 | 0.1513 | 1.0213 | (0.7600 1.3761) |
| Respondent currently working (No = reference) | ||||
| Yes | 0.2394 | 0.0795 | 1.2705 | (1.0868 1.4850) |
| Heard about family planning on the radio in the last few months (No = reference) | ||||
| Yes | 0.1109 | 0.0554 | 1.1173 | (1.0021 1.2455) |
| Visited by family planning worker in the last 12 months (Yes = reference) | ||||
| No | 0.1960 | 0.0598 | 1.21653 | (1.0812 1.3681) |
| Heard about family planning from newspapers/magazines (No = reference) | ||||
| Yes | 0.2884 | 0.1197 | 1.3343 | (1.0564 1.6896) |
| Province (West = reference) | ||||
| Kigali | 0.0548 | 0.1047 | 1.0563 | (0.4702 1.5038) |
| South | −0.1224 | 0.1066 | 0.8848 | (0.8601 1.2969) |
| North | 0.3580 | 0.1141 | 1.4305 | (1.1436 1.7898) |
| East | 0.1704 | 0.1051 | 1.1858 | (0.9649 1.4579) |
| Husband desires children (Same number = reference) | ||||
| More | 0.2622 | 0.0818 | 1.2998 | (1.1069 1.5258) |
| Fewer | −0.0456 | 0.1153 | 0.9554 | (0.7619 1.1979) |
| Do not know | 0.2073 | 0.0964 | 1.2304 | (1.0182 1.4866) |
| Code | District | Code | District | Code | District | Code | District |
|---|---|---|---|---|---|---|---|
| 1 | Nyarugenge | 9 | Ruhango | 17 | Rusizi | 24 | Rwamagana |
| 2 | Gasabo | 10 | Muhanga | 18 | Nyamasheke | 25 | Nyagatare |
| 3 | Kicukiro | 11 | Kamonyi | 19 | Rulindo | 26 | Gatsibo |
| 4 | Nyanza | 12 | Karongi | 20 | Gakenke | 27 | Kayonza |
| 5 | Gisagara | 13 | Rubavu | 21 | Musanze | 28 | Kirehe |
| 6 | Nyaruguru | 14 | Rubavu | 22 | Burera | 29 | Ngoma |
| 7 | Huye | 15 | Nyabihu | 23 | Gicumbi | 30 | Bugesera |
| 8 | Nyamagabe | 16 | Ngororero |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habyarimana, F.; Ramroop, S. Spatial Analysis of Socio-Economic and Demographic Factors Associated with Contraceptive Use among Women of Childbearing Age in Rwanda. Int. J. Environ. Res. Public Health 2018, 15, 2383. https://doi.org/10.3390/ijerph15112383
Habyarimana F, Ramroop S. Spatial Analysis of Socio-Economic and Demographic Factors Associated with Contraceptive Use among Women of Childbearing Age in Rwanda. International Journal of Environmental Research and Public Health. 2018; 15(11):2383. https://doi.org/10.3390/ijerph15112383
Chicago/Turabian StyleHabyarimana, Faustin, and Shaun Ramroop. 2018. "Spatial Analysis of Socio-Economic and Demographic Factors Associated with Contraceptive Use among Women of Childbearing Age in Rwanda" International Journal of Environmental Research and Public Health 15, no. 11: 2383. https://doi.org/10.3390/ijerph15112383
APA StyleHabyarimana, F., & Ramroop, S. (2018). Spatial Analysis of Socio-Economic and Demographic Factors Associated with Contraceptive Use among Women of Childbearing Age in Rwanda. International Journal of Environmental Research and Public Health, 15(11), 2383. https://doi.org/10.3390/ijerph15112383