
Continuous Monitoring of Positive Airway Pressure Therapy with a Smartphone-Based Home Sleep Apnea Test

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
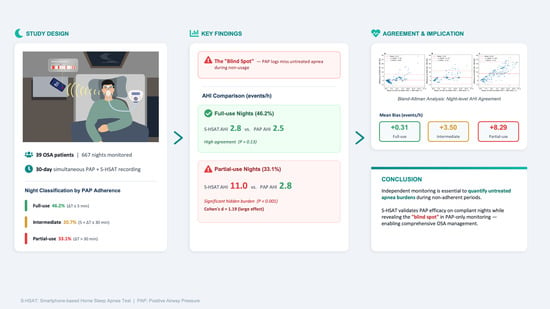
2.1. Study Design and Participants
2.2. S-HSAT and PAP Data Collection
2.3. Classification of PAP Adherence Levels
- Full-use nights ( ≤ 5 min): Nights where the PAP usage duration matched or exceeded the S-HSAT usage time, allowing for a negligible margin of ≤5 min. This indicates comprehensive therapeutic coverage, implying that PAP was used continuously throughout the entire sleep period.
- Intermediate-use nights (5 < ≤ 30 min): Nights in which PAP was worn for most, but not all, of the sleep period, resulting in a time difference of more than 5 min but no more than 30 min. This reflects brief lapses in PAP use during sleep.
- Partial-use nights ( > 30 min): Nights where PAP usage was shorter than the S-HSAT usage time by more than 30 min, indicating substantial periods of untreated sleep, typically due to early mask removal.
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. PAP Usage Patterns
3.3. AHI by Adherence Category
3.4. Agreement and Concordance
4. Discussion
4.1. PAP and S-HSAT Usage Patterns
4.2. Validation of AHI Estimation Under Full PAP Adherence
4.3. Quantification of Untreated Apnea Burden During Partial Adherence
4.4. Clinical Importance of Monitoring and Compliance
4.5. Implications for Long-Term Management, Behavior, and Device Optimization
4.6. Practical Barriers
4.7. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azagra-Calero, E.; Espinar-Escalona, E.; Barrera-Mora, J.M.; Llamas-Carreras, J.M.; Solano-Reina, E. Obstructive sleep apnea syndrome (OSAS). Review of the literature. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e925–e929. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Patel, S.R.; Kales, S.N.; Ayas, N.T.; Strohl, K.P.; Gozal, D.; Malhotra, A. An Official American Thoracic Society Statement: The Importance of Healthy Sleep. Recommendations and Future Priorities. Am. J. Respir. Crit. Care Med. 2015, 191, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnea-hypopnea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; O’Donnell, C.P. Pathophysiology of sleep apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef] [PubMed]
- Lv, R.; Liu, X.; Zhang, Y.; Dong, N.; Wang, X.; He, Y.; Yue, H.; Yin, Q. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct. Target. Ther. 2023, 8, 218. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, B.W.; Murariu, D.; Pang, K.P. Trends in CPAP adherence over twenty years of data collection: A flattened curve. J. Otolaryngol. Head Neck Surg. 2016, 45, 43. [Google Scholar] [CrossRef] [PubMed]
- Mak, S.; Ash, G.; Liang, L.J.; Der-McLeod, E.; Ghadimi, S.; Kewalramani, A.; Naeem, S.; Zeidler, M.; Fung, C. Testing a Consumer Wearables Program to Promote the Use of Positive Airway Pressure Therapy in Patients with Obstructive Sleep Apnea: Protocol for a Pilot Randomized Controlled Trial. JMIR Res. Protoc. 2024, 13, e60769. [Google Scholar] [CrossRef] [PubMed]
- Roeder, M.; Bradicich, M.; Schwarz, E.I.; Thiel, S.; Gaisl, T.; Held, U.; Kohler, M. Night-to-night variability of respiratory events in obstructive sleep apnea: A systematic review and meta-analysis. Thorax 2020, 75, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Chang, J.W.; Benjafield, A.V.; Crocker, M.E.; Kelly, C.; Becker, K.A.; Kim, J.B.; Woodrum, R.R.; Liang, J.; Derose, S.F. Effect of Telemedicine Education and Telemonitoring on Continuous Positive Airway Pressure Adherence. The Tele-OSA Randomized Trial. Am. J. Respir. Crit. Care Med. 2018, 197, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.W.; Jung, S.J.; Shin, J.H.; Won, T.B.; Rhee, C.S.; Kim, J.W. Evaluating Prediction Models of Sleep Apnea from Smartphone-Recorded Sleep Breathing Sounds. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Le, V.L.; Kim, D.; Cho, E.; Jang, H.; Reyes, R.D.; Kim, H.; Lee, D.; Yoon, I.-Y.; Hong, J.; Kim, J.-W. Real-Time Detection of Sleep Apnea Based on Breathing Sounds and Prediction Reinforcement Using Home Noises: Algorithm Development and Validation. J. Med. Internet Res. 2023, 25, e44818. [Google Scholar] [CrossRef] [PubMed]
- Han, S.C.; Kim, D.; Rhee, C.S.; Cho, S.W.; Le, V.L.; Cho, E.S.; Kim, H.; Yoon, I.Y.; Jang, H.; Hong, J.; et al. In-Home Smartphone-Based Prediction of Obstructive Sleep Apnea in Conjunction with Level 2 Home Polysomnography. JAMA Otolaryngol. Head Neck Surg. 2024, 150, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.C.; Unnikrishnan, D.; Schneider, H.; Kirkness, J.; Schwartz, A.R.; Smith, P.L.; Polotsky, V.Y. Effect of Acute Intermittent CPAP Depressurization during Sleep in Obese Patients. PLoS ONE 2016, 11, e0146606. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Weaver, T.E.; Maislin, G.; Dinges, D.F.; Bloxham, T.; George, C.F.; Greenberg, H.; Kader, G.; Mahowald, M.; Younger, J.; Pack, A.I. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep 2007, 30, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.A.; Capote, F.; Campos-Rodríguez, F.; Lloberes, P.; Díaz de Atauri, M.J.; Somoza, M.; Masa, J.F.; González, M.; Sacristán, L.; Barbé, F.; et al. Effect of CPAP on blood pressure in patients with obstructive sleep apnea and resistant hypertension: The HIPARCO randomized clinical trial. JAMA 2013, 310, 2407–2415. [Google Scholar] [CrossRef] [PubMed]
- Epstein, M.; Musa, T.; Chiu, S.; Costanzo, J.; Dunne, C.; Cerrone, F.; Capone, R. Use of the WatchPAT to detect occult residual sleep-disordered breathing in patients on CPAP for obstructive sleep apnea. J. Clin. Sleep Med. 2020, 16, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Escourrou, P.J.; Seailles, T.; De Roquefeuil, F.; Schmitt, E.; Blumen, M.; Aisenberg, N.; Felix, O.; Sabil, A.; Elie, V.; D’ACunto, M.; et al. Use of a non-intrusive under-mattress sleep analyzer in monitoring patients at home under Continuous Positive Airway Pressure. ERJ Open Res. 2023, 9, 104. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Monitoring overview | |
| Total analyzed nights | 667 |
| Nights per patient | 17.1 |
| Demographics | |
| Male sex, n (%) | 39 (100) |
| Age, years | 45.1 ± 11.1 |
| Body mass index, kg/m2 | 26.4 ± 5.2 |
| Baseline OSA severity | |
| Apnea–hypopnea index, events/h | 34.0 ± 18.6 |
| Severe OSA (≥30), n (%) | 20 (51.3) |
| Sleep-related questionnaires | |
| Pittsburgh Sleep Quality Index | 7.6 ± 3.2 |
| Epworth Sleepiness Scale | 8.9 ± 5.2 |
| Characteristic | Included (n = 39) | Excluded (n = 24) | p Value |
|---|---|---|---|
| Age, years | 45.1 ± 11.1 | 46.5 ± 10.0 | 0.61 |
| Sex, male n (%) | 39 (100) | 24 (100) | — |
| BMI, kg/m2 | 26.4 ± 5.2 | 27.6 ± 3.9 | 0.31 |
| PSG AHI, events/h | 34.0 ± 18.6 | 36.1 ± 24.1 | 0.72 |
| Pittsburgh Sleep Quality Index | 7.6 ± 3.2 | 8.5 ± 3.1 | 0.29 |
| Epworth Sleepiness Scale | 8.9 ± 5.2 | 11.1 ± 4.5 | 0.09 |
| Measurement | Full-Use (308 Nights) | Intermediate-Use (138 Nights) | Partial-Use (221 Nights) |
|---|---|---|---|
| AHI (events/h) | |||
| S-HSAT | 2.81 ± 4.28 | 7.30 ± 5.53 | 11.04 ± 7.41 |
| PAP | 2.51 ± 2.01 | 3.80 ± 3.31 | 2.75 ± 2.48 |
| p-value | 0.13 | <0.001 | <0.001 |
| Cohen’s d | 0.09 | 0.85 | 1.19 |
| Usage Time (min) | |||
| S-HSAT | 321.68 ± 69.86 | 333.81 ± 80.31 | 381.68 ± 93.54 |
| PAP | 343.82 ± 70.02 | 313.37 ± 80.82 | 259.77 ± 92.62 |
| p-value | <0.001 | <0.001 | <0.001 |
| Cohen’s d | −0.70 | 2.70 | 1.51 |
| Metric | Full-Use | Intermediate-Use | Partial-Use |
|---|---|---|---|
| Number of nights | 308 | 138 | 221 |
| Concordance correlation coefficient | 0.43 | 0.46 | 0.10 |
| Intraclass correlation coefficient (two-way random effects, single measurement) | 0.43 | 0.46 | 0.10 |
| Mean bias, events per hour * | 0.31 | 3.50 | 8.29 |
| 95% limits of agreement, events per hour | −6.66 to 7.28 | −4.53 to 11.52 | −5.33 to 21.90 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Heo, S.; Kim, S.; Moon, S.; Lee, S.; Lee, D.; Hong, J.; Chung, Y.-S.; Kim, H.J.; Hong, J.K.; Yoon, I.-Y.; et al. Continuous Monitoring of Positive Airway Pressure Therapy with a Smartphone-Based Home Sleep Apnea Test. Medicina 2026, 62, 1008. https://doi.org/10.3390/medicina62061008
Heo S, Kim S, Moon S, Lee S, Lee D, Hong J, Chung Y-S, Kim HJ, Hong JK, Yoon I-Y, et al. Continuous Monitoring of Positive Airway Pressure Therapy with a Smartphone-Based Home Sleep Apnea Test. Medicina. 2026; 62(6):1008. https://doi.org/10.3390/medicina62061008
Chicago/Turabian StyleHeo, Sungjin, Seunghun Kim, Sungeun Moon, Sujin Lee, Dongheon Lee, Joonki Hong, Yoo-Sam Chung, Hyun Jik Kim, Jung Kyung Hong, In-Young Yoon, and et al. 2026. "Continuous Monitoring of Positive Airway Pressure Therapy with a Smartphone-Based Home Sleep Apnea Test" Medicina 62, no. 6: 1008. https://doi.org/10.3390/medicina62061008
APA StyleHeo, S., Kim, S., Moon, S., Lee, S., Lee, D., Hong, J., Chung, Y.-S., Kim, H. J., Hong, J. K., Yoon, I.-Y., & Kim, J.-W. (2026). Continuous Monitoring of Positive Airway Pressure Therapy with a Smartphone-Based Home Sleep Apnea Test. Medicina, 62(6), 1008. https://doi.org/10.3390/medicina62061008