


Multifactorial Influences on Oxygen Consumption Recovery Post-High-Intensity Exercise in Adults: A Case-Control Study
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Ethical Considerations
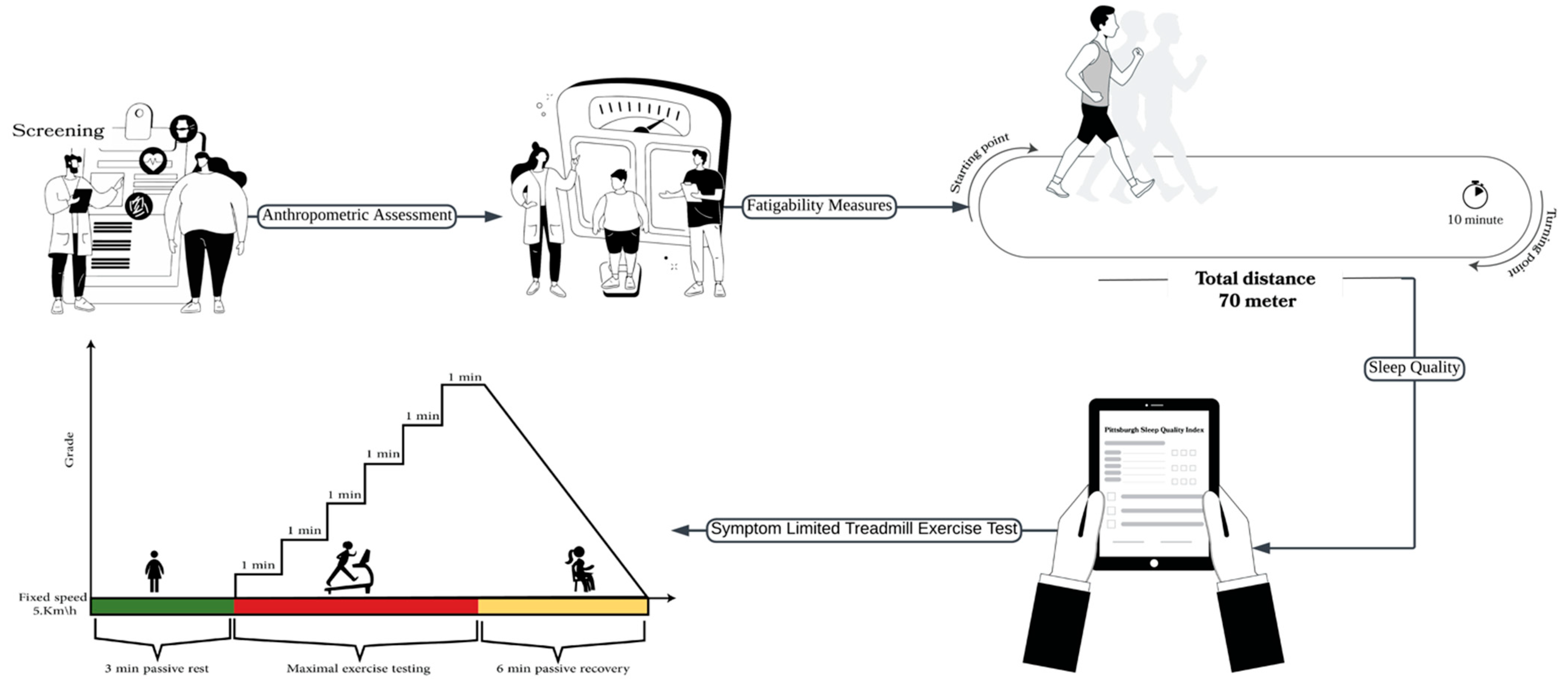
2.3. Study Procedures
2.3.1. Anthropometric Assessment
2.3.2. Sleep Quality
2.3.3. Fatigability Measures
2.3.4. Symptom-Limited Treadmill Exercise Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BIA | Bioelectrical impedance analysis |
| VO2peak | Peak oxygen consumption |
| T | Half-time |
| EPOC | Excess post-exercise oxygen consumption |
| CRF | Cardiorespiratory fitness |
| VO2 max | Maximal rate of oxygen consumption |
| BMI | Body mass index |
| HRR | Heart rate recovery |
| RER | Respiratory exchange ratio |
| PARQ+ | Physical Activity Readiness Questionnaire |
| PSQI | Pittsburgh Sleep Quality Index |
| 10 MWT | 10 min walk test |
| CPET | Cardiopulmonary exercise test |
References
- Peake, J.M. Recovery after Exercise: What Is the Current State of Play? Curr. Opin. Physiol. 2019, 10, 17–26. [Google Scholar] [CrossRef]
- Skorski, S.; Mujika, I.; Bosquet, L.; Meeusen, R.; Coutts, A.J.; Meyer, T. The Temporal Relationship between Exercise, Recovery Processes, and Changes in Performance. Int. J. Sports Physiol. Perform. 2019, 14, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Vianna, J.M.; Werneck, F.Z.; Coelho, E.F.; Damasceno, V.O.; Reis, V.M. Oxygen Uptake and Heart Rate Kinetics after Different Types of Resistance Exercise. J. Hum. Kinet. 2014, 42, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.R.; Stout, J.R.; Morton, A.B.; Jajtner, A.R.; Gonzalez, A.M.; Wells, A.J.; Mangine, G.T.; McCormack, W.P.; Emerson, N.S.; Robinson IV, E.H. Excess Post-Exercise Oxygen Consumption (EPOC) Following Multiple Effort Sprint and Moderate Aerobic Exercise. Kinesiology 2013, 45, 16. [Google Scholar]
- Mann, T.; Lamberts, R.; Nummela, A.; Lambert, M. Relationship between Perceived Exertion during Exercise and Subsequent Recovery Measurements. Biol. Sport 2017, 34, 3–9. [Google Scholar] [CrossRef]
- Campos, E.Z.; Bastos, F.N.; Papoti, M.; Freitas Junior, I.F.; Gobatto, C.A.; Balikian Junior, P. The Effects of Physical Fitness and Body Composition on Oxygen Consumption and Heart Rate Recovery after High-Intensity Exercise. Int. J. Sports Med. 2012, 33, 621–626. [Google Scholar] [CrossRef]
- Millet, G.Y.; Bertrand, M.F.; Lapole, T.; Féasson, L.; Rozand, V.; Hupin, D. Measuring Objective Fatigability and Autonomic Dysfunction in Clinical Populations: How and Why? Front. Sports Act. Living 2023, 5, 1140833. [Google Scholar] [CrossRef]
- Michalik, K.; Zatoń, M.; Hebisz, P.; Hebisz, R. Heart Rate and Oxygen Uptake Recovery and the Level of Aerobic Capacity in Mountain Bikers. Pol. J. Sport. Tour. 2017, 24, 242–246. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Fan, L.M.; Collins, A.; Geng, L.; Li, J.-M. Impact of Unhealthy Lifestyle on Cardiorespiratory Fitness and Heart Rate Recovery of Medical Science Students. BMC Public Health 2020, 20, 1012. [Google Scholar] [CrossRef]
- Cohen-Solal, A.; Laperche, T.; Morvan, D.; Geneves, M.; Caviezel, B.; Gourgon, R. Prolonged Kinetics of Recovery of Oxygen Consumption After Maximal Graded Exercise in Patients with Chronic Heart Failure. Circulation 1995, 91, 2924–2932. [Google Scholar] [CrossRef]
- Healy, R.D.; Smith, C.; Woessner, M.N.; Levinger, I. Relationship between VO2peak, VO2 Recovery Kinetics, and Muscle Function in Older Adults. Gerontology 2023, 69, 1278–1283. [Google Scholar] [CrossRef]
- Hunter, S.K. Performance Fatigability: Mechanisms and Task Specificity. Cold Spring Harb. Perspect. Med. 2018, 8, a029728. [Google Scholar] [CrossRef]
- Ouergui, I.; Franchini, E.; Selmi, O.; Levitt, D.E.; Chtourou, H.; Bouhlel, E.; Ardigò, L.P. Relationship between Perceived Training Load, Well-Being Indices, Recovery State and Physical Enjoyment during Judo-Specific Training. Int. J. Environ. Res. Public Health 2020, 17, 7400. [Google Scholar] [CrossRef]
- Aldhafiri, A.; Almutairi, N.; Alharbi, M.; Aloufi, A.; Hakeem, A.; Kattan, A.; Alzahrani, F. Evaluation of Sleep Behavior and the Use of Sleep Aids among Adults Living in Saudi Arabia: A Cross-Sectional Study. Clocks Sleep 2023, 5, 536–551. [Google Scholar] [CrossRef]
- Salem, V.; AlHusseini, N.; Abdul Razack, H.I.; Naoum, A.; Sims, O.T.; Alqahtani, S.A. Prevalence, Risk Factors, and Interventions for Obesity in Saudi Arabia: A Systematic Review. Obes. Rev. 2022, 23, e13448. [Google Scholar] [CrossRef]
- Michels, N.; Clays, E.; De Buyzere, M.; Vanaelst, B.; De Henauw, S.; Sioen, I. Children’s Sleep and Autonomic Function: Low Sleep Quality Has an Impact on Heart Rate Variability. Sleep 2013, 36, 1939–1946. [Google Scholar] [CrossRef]
- Qvisth, V.; Hagström-Toft, E.; Enoksson, S.; Bolinder, J. Catecholamine Regulation of Local Lactate Production in Vivo in Skeletal Muscle and Adipose Tissue: Role of β-Adrenoreceptor Subtypes. J. Clin. Endocrinol. Metab. 2008, 93, 240–246. [Google Scholar] [CrossRef]
- Matsuo, T.; Ohkawara, K.; Seino, S.; Shimojo, N.; Yamada, S.; Ohshima, H.; Tanaka, K.; Mukai, C. Cardiorespiratory Fitness Level Correlates Inversely with Excess Post-Exercise Oxygen Consumption after Aerobic-Type Interval Training. BMC Res. Notes 2012, 5, 646. [Google Scholar] [CrossRef]
- Habib, S.S. Body Mass Index and Body Fat Percentage in Assessment of Obesity Prevalence in Saudi Adults. Biomed. Environ. Sci. 2013, 26, 94–99. [Google Scholar] [CrossRef]
- Ramania, N.S.; Apriantono, T.; Winata, B. The Effects of Differences in Sleep Quality and Quantity on VO2max Levels. Adv. Rehabil. 2020, 34, 11–17. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Pariser, G. Cardiorespiratory Fitness Levels and Its Correlates Among Adults with Diabetes. Cardiopulm. Phys. Ther. J. 2013, 24, 27–34. [Google Scholar] [CrossRef]
- Kaze, A.D.; Agoons, D.D.; Santhanam, P.; Erqou, S.; Ahima, R.S.; Echouffo-Tcheugui, J.B. Correlates of Cardiorespiratory Fitness among Overweight or Obese Individuals with Type 2 Diabetes. BMJ Open Diabetes Res. Care 2022, 10, e002446. [Google Scholar] [CrossRef] [PubMed]
- Pokar, K.; Thoriya, R.; Parmar, D.; Chauhan, A.; Nakarani, K.; Tank, N.; Sharma, D. A Study to Correlate between Bmi and Cardiorespiratory Fitness among Collegiate Students: A Correlational Study. Int. Res. Conf. Innov. Startup Invest. 2022, 48–59. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Warburton, D.E.; Jamnik, V.; Bredin, S.S.; Shephard, R.J.; Gledhill, N. The 2019 Physical Activity Readiness Questionnaire for Everyone (PAR-Q+) and Electronic Physical Activity Readiness Medical Examination (ePARmed-X+). Health Fit. J. Can. 2018, 11, 80–83. [Google Scholar]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy Percentage Body Fat Ranges: An Approach for Developing Guidelines Based on Body Mass Index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Popiolek-Kalisz, J.; Szczygiel, K. Bioelectrical Impedance Analysis and Body Composition in Cardiovascular Diseases. Curr. Probl. Cardiol. 2023, 48, 101911. [Google Scholar] [CrossRef]
- Al Maqbali, M.; Hughes, C.; Gracey, J.; Rankin, J.; Dunwoody, L.; Hacker, E. Validation of the Pittsburgh Sleep Quality Index (PSQI) with Arabic Cancer Patients. Sleep Biol. Rhythm 2020, 18, 217–223. [Google Scholar] [CrossRef]
- Suleiman, K.H.; Yates, B.C.; Berger, A.M.; Pozehl, B.; Meza, J. Translating the Pittsburgh Sleep Quality Index into Arabic. West. J. Nurs. Res. 2010, 32, 250–268. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–Retest Reliability and Validity of the Pittsburgh Sleep Quality Index in Primary Insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Schnelle, J.F.; Buchowski, M.S.; Ikizler, T.A.; Durkin, D.W.; Beuscher, L.; Simmons, S.F. Evaluation of Two Fatigability Severity Measures in Elderly Adults. J. Am. Geriatr. Soc. 2012, 60, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Myers, J.; Williams, M.A.; Gulati, M.; Kligfield, P.; Balady, G.J.; Collins, E.; Fletcher, G. Assessment of Functional Capacity in Clinical and Research Settings. Circulation 2007, 116, 329–343. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018; ISBN 978-1-4963-3906-5. [Google Scholar]
- Myers, J.; Bellin, D. Ramp Exercise Protocols for Clinical and Cardiopulmonary Exercise Testing. Sports Med. 2000, 30, 23–29. [Google Scholar] [CrossRef]
- Hansen, J.E.; Sue, D.Y.; Wasserman, K. Predicted Values for Clinical Exercise Testing. Am. Rev. Respir. Dis. 1984, 129, S49-55. [Google Scholar] [CrossRef] [PubMed]
- Mondal, H.; Mishra, S.P. Effect of BMI, Body Fat Percentage and Fat Free Mass on Maximal Oxygen Consumption in Healthy Young Adults. J. Clin. Diagn. Res. 2017, 11, CC17. [Google Scholar] [CrossRef]
- Carneiro-Barrera, A.; Amaro-Gahete, F.J.; Acosta, F.M.; Ruiz, J.R. Body Composition Impact on Sleep in Young Adults: The Mediating Role of Sedentariness, Physical Activity, and Diet. J. Clin. Med. 2020, 9, 1560. [Google Scholar] [CrossRef]
- Wong, T.; Harber, V. Lower Excess Postexercise Oxygen Consumption and Altered Growth Hormone and Cortisol Responses to Exercise in Obese Men. J. Clin. Endocrinol. Metab. 2006, 91, 678–686. [Google Scholar] [CrossRef]
- Goyal, G.L.; Sharma, R.; Joshi, S.; Bhardwaj, A. Effect of Sleep Deprivation on Heart Rate Recovery after Treadmill Testing in Otherwise Healthy Young Adults. Natl. J. Physiol. Pharm. Pharmacol. 2019, 9, 19–22. [Google Scholar] [CrossRef]
- Laforgia, J.; Withers, R.T.; Gore, C.J. Effects of Exercise Intensity and Duration on the Excess Post-Exercise Oxygen Consumption. J. Sports Sci. 2006, 24, 1247–1264. [Google Scholar] [CrossRef] [PubMed]
- Simmons, R. The Effects of Fitness Level and Sex on EPOC Following High Intensity Interval and Moderate Intensity Aerobic Exercise. Human Movement Studies & Special Education Theses & Dissertations, Old Dominion University, Norfolk, VA, USA, 2016. [Google Scholar] [CrossRef]
- Hopker, J.G.; Caporaso, G.; Azzalin, A.; Carpenter, R.; Marcora, S.M. Locomotor Muscle Fatigue Does Not Alter Oxygen Uptake Kinetics during High-Intensity Exercise. Front. Physiol. 2016, 7, 463. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | All n = 80 Mean ± SD | Fat Percentage | p-Value | |
|---|---|---|---|---|
| Normal n = 40 Mean ± SD | High n = 40 Mean ± SD | |||
| Age (years) | 24.53 ± 5.78 | 24.67 ± 5.73 | 24.4 ± 5.91 | 0.8 |
| Weight (kg) | 68.24 ± 16.53 | 60.61 ± 9.83 | 75.87 ± 18.38 | <0.001 * |
| Height (cm) | 164 ± 8.1 | 165 ± 8.3 | 163 ± 7.9 | 0.29 |
| BMI (kg/m2) | 25 ± 5.1 | 21.97 ± 2.56 | 28.03 ± 5.23 | <0.001 * |
| Fat-free mass (kg) | 46.90 ± 10.16 | 46.56 ± 9.41 | 47.2 ± 10.96 | 0.76 |
| Skeletal muscle mass (kg) | 21.64 ± 5.81 | 21.45 ± 5.45 | 21.84 ± 6.21 | <0.001 * |
| Absolute fat (kg) | 21.34 ± 10.23 | 14.05 ± 4.22 | 28.623 ± 9.25 | <0.001 * |
| Fat percentage | 30.17 ± 9.47 | 22.86 ± 7.02 | 37.47 ± 4.81 | <0.001 * |
| Male gender, n (%) | 32(40) | 19 (47.50) | 13 (32.50) | 9.17 |
| Educational level, n (%) | ||||
| Bachelor’s degree | 78 (97.5) | 40 (100) | 38 (95) | 0.4 |
| Post-graduate degree | 2 (2.5) | 0 | 2 (5) | |
| Baseline VO2 (mL/kg/min) | 3.5 ± 0.2 | 4 ± 0.4 | 3.5 ± 0.3 | 0.8 |
| Variables | Correlation Coefficient | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| VO2 recovery T1 half-time (T1) | 1 | |||||||
| VO2 recovery T2 half-time (T2) | 0.97 * | 1 | ||||||
| Age | −0.07 | −0.04 | 1 | |||||
| Fat % | −0.62 ** | -0.62 ** | 0.06 | 1 | ||||
| Peak VO2 (mL/kg/min) | 0.98 ** | 0.98 ** | −0.07 | −0.64 ** | 1 | |||
| PFI | −0.31 ** | −0.31 ** | −0.07 | 0.22 * | −0.31 ** | 1 | ||
| Perceived Fatigability Index | −0.161 | −0.15 | −0.14 | 0.12 | −0.16 | 0.22 * | 1 | |
| PSQI | −0.08 | −0.11 | 0.09 | 0.33 ** | −0.10 | 0.05 | 0.11 | 1 |
| Model | Predictors a | Coefficients | R2 | VIF | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| β | B | SE | T | p-Value | 95% CI | |||||
| Lower | Upper | |||||||||
| Model * | (Constant) | - | 27.93 | 3.47 | 8.04 | <0.001 | 21.01 | 34.86 | 0.72 | - |
| Fat % | −0.36 | −0.27 | 0.08 | −3.33 | 0.001 | −0.44 | −0.11 | 1.08 | ||
| Peak VO2 (mL/kg/min) | 0.08 | 5.85 | 0.68 | 8.53 | <0.001 | 4.48 | 7.21 | 1.14 | ||
| PFI | −0.60 | −41.24 | 17.88 | −2.31 | 0.025 | −76.84 | −5.63 | 0.8 | ||
| Sleep quality | −1.42 | 0.13 | 0.16 | 0.83 | 0.40 | −0.18 | 0.45 | 0.9 | ||
| F | F (5, 74) = 39.58 | |||||||||
| F-value | <0.001 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldhahi, M.I.; Alahmed, R.I.; Almutairi, R.H.; Alqahtani, H.A.; Alawad, H.M.; Alkabeer, R.S.; Alqhtani, L.K.; Aljubairi, M.S. Multifactorial Influences on Oxygen Consumption Recovery Post-High-Intensity Exercise in Adults: A Case-Control Study. Medicina 2025, 61, 1213. https://doi.org/10.3390/medicina61071213
Aldhahi MI, Alahmed RI, Almutairi RH, Alqahtani HA, Alawad HM, Alkabeer RS, Alqhtani LK, Aljubairi MS. Multifactorial Influences on Oxygen Consumption Recovery Post-High-Intensity Exercise in Adults: A Case-Control Study. Medicina. 2025; 61(7):1213. https://doi.org/10.3390/medicina61071213
Chicago/Turabian StyleAldhahi, Monira I., Rawan I. Alahmed, Reem H. Almutairi, Haya A. Alqahtani, Hatoon M. Alawad, Rania S. Alkabeer, Leena K. Alqhtani, and Mohanad S. Aljubairi. 2025. "Multifactorial Influences on Oxygen Consumption Recovery Post-High-Intensity Exercise in Adults: A Case-Control Study" Medicina 61, no. 7: 1213. https://doi.org/10.3390/medicina61071213
APA StyleAldhahi, M. I., Alahmed, R. I., Almutairi, R. H., Alqahtani, H. A., Alawad, H. M., Alkabeer, R. S., Alqhtani, L. K., & Aljubairi, M. S. (2025). Multifactorial Influences on Oxygen Consumption Recovery Post-High-Intensity Exercise in Adults: A Case-Control Study. Medicina, 61(7), 1213. https://doi.org/10.3390/medicina61071213