
Are Urethral Pressure Profile Measurements Effective in Diagnosing Urodynamic Stress Incontinence in Women Presenting with Stress or Mixed Urinary Incontinence? Results from a Cross-Sectional Study

 , , , , ,
, , , , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int. Urogynecol. J. 2010, 21, 5–26. [Google Scholar] [CrossRef] [PubMed]
- Ebbesen, M.H.; Hunskaar, S.; Rortveit, G.; Hannestad, Y.S. Prevalence, incidence and remission of urinary incontinence in women: Longitudinal data from the Norwegian HUNT study (EPINCONT). BMC Urol. 2013, 13, 27. [Google Scholar] [CrossRef] [PubMed]
- Falah-Hassani, K.; Reeves, J.; Shiri, R.; Hickling, D.; McLean, L. The pathophysiology of stress urinary incontinence: A systematic review and meta-analysis. Int. Urogynecol. J. 2021, 32, 501–552. [Google Scholar] [CrossRef] [PubMed]
- Ptaszkowski, K.; Paprocka-Borowicz, M.; Slupska, L.; Bartnicki, J.; Dymarek, R.; Rosinczuk, J.; Heimrath, J.; Dembowski, J.; Zdrojowy, R. Assessment of bioelectrical activity of synergistic muscles during pelvic floor muscles activation in postmenopausal women with and without stress urinary incontinence: A preliminary observational study. Clin. Interv. Aging 2015, 10, 1521–1528. [Google Scholar] [CrossRef] [PubMed]
- Petros, P.E.; Ulmsten, U.I. An integral theory of female urinary incontinence. Experimental and clinical considerations. Acta Obstet. Gynecol. Scand. Suppl. 1990, 153, 7–31. [Google Scholar] [CrossRef] [PubMed]
- Bergström, B.S. Urethral Hanging Theory. Neurourol. Urodyn. 2017, 36, 826–827. [Google Scholar] [CrossRef] [PubMed]
- DeLancey, J.O. Structural support of the urethra as it relates to stress urinary incontinence: The hammock hypothesis. Am. J. Obstet. Gynecol. 1994, 170, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- DeLancey, J.O.; Trowbridge, E.R.; Miller, J.M.; Morgan, D.M.; Guire, K.; Fenner, D.E.; Weadock, W.J.; Ashton-Miller, J.A. Stress urinary incontinence: Relative importance of urethral support and urethral closure pressure. J. Urol. 2008, 179, 2286–2290. [Google Scholar] [CrossRef] [PubMed]
- Kelly, H.A.; Burnam, C.F. Diseases of Kidneys, Ureters and Bladder; D. Appleton and Company: New York, NY, USA; London, UK, 1922; Volume 2v. [Google Scholar]
- Cardozo, L.; Rovner, E.; Wagg, A.; Wein, A.; Abrams, P. (Eds.) Incontinence 7th Edition, Committee 5; ICI-ICS. International Continence Society: Bristol, UK, 2023; ISBN 978-0-9569607-4-0. [Google Scholar]
- Avery, K.; Donovan, J.; Peters, T.J.; Shaw, C.; Gotoh, M.; Abrams, P. ICIQ: A brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol. Urodyn. 2004, 23, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, S.; Grigoriadis, T.; Kyriakidou, N.; Giannoulis, G.; Antsaklis, A. The validation of international consultation on incontinence questionnaires in the Greek language. Neurourol. Urodyn. 2012, 31, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Bump, R.C.; Mattiasson, A.; Bø, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; Shull, B.L.; Smith, A.R. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Rosier, P.F.W.M.; Schaefer, W.; Lose, G.; Goldman, H.B.; Guralnick, M.; Eustice, S.; Dickinson, T.; Hashim, H. International Continence Society Good Urodynamic Practices and Terms 2016: Urodynamics, Uroflowmetry, Cystometry, and Pressure-Flow Study. Neurourol. Urodyn. 2017, 36, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Grigoriadis, T.; Giannoulis, G.; Zacharakis, D.; Protopapas, A.; Cardozo, L.; Athanasiou, S. The “1-3-5 cough test”: Comparing the severity of urodynamic stress incontinence with severity measures of subjective perception of stress urinary incontinence. Int. Urogynecol. J. 2016, 27, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Guralnick, L.; Fritel, X.; Tarcan, T.; Espuna-Pons, M.; Rosier, P.F.W.M. ICS Educational Module: Cough stress test in the evaluation of female urinary incontinence: Introducing the ICS-Uniform Cough Stress Test. Neurourol. Urodyn. 2018, 37, 1849–1855. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Cardozo, L.; Wagg, A.; Wein, A. (Eds.) Incontinence 6th Edition, Committee 5; ICI-ICS. International Continence Society: Bristol, UK, 2017; ISBN 978-0956960733. [Google Scholar]
- Hill, B.J.; Fletcher, S.; Blume, J.; Adam, R.; Ward, R. Variables affecting maximum urethral closure pressure (MUCP) and abdominal leak point pressure (ALPP) measurements. Int. Urogynecol. J. 2017, 28, 1651–1656. [Google Scholar] [CrossRef] [PubMed]
- Park, K.K.; Kim, S.D.; Huh, J.-S.; Kim, Y.-J. A Study of Clinical Predictors Associated with Intrinsic Sphincter Defciency in Women with Stress Urinary Incontinence. Int. Neurourol. J. 2017, 21, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Arribillaga, L.; Ledesma, M.; Montedoro, A.; Grutadauria, G.; Oulton, G.; Bengió, R.G. Clinical score predictive of abdominal leak point pressure (ALPP) < 60 cm H2O in the urodynamics study of women with stress urinary incontinence. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 237, 13–17. [Google Scholar] [PubMed]
- Kapoor, D.S.; Housami, F.; White, P.; Swithinbank, L.; Drake, M. Maximum urethral closure pressure in women: Normative data and evaluation as a diagnostic test. Int. Urogynecol. J. 2012, 23, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Constantinou, C.E. Resting and stress urethral pressures as a clinical guide to the mechanism of continence in the female patient. Urol. Clin. N. Am. 1985, 12, 247–258. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Exclusion Criteria | Inclusion Criteria |
|---|---|
| Prolapse stage higher than POP-Q Stage 1 | Stress urinary incontinence |
| Previous incontinence surgery | Mixed urinary incontinence |
| Active OAB treatment |
| Group 1 (no USI) | Group 2 (USI) | |||||
|---|---|---|---|---|---|---|
| n = 29 | n = 28 | |||||
| Mean | SD | Mean | SD | p | 95% CI | |
| Age | 59.69 | 8.95 | 61.85 | 9.72 | 0.385 | - |
| ICI-Q SF score | 15.27 | 4.12 | 16.4 | 4.11 | 0.344 | - |
| Uroflow | ||||||
| Qave (mL/s) | 7.24 | 6.51 | 8.44 | 6.65 | 0.522 | - |
| Qmax (mL/s) | 20.37 | 21.03 | 19.72 | 15.97 | 0.901 | - |
| Vol (mL) | 217.18 | 165.6 | 188.63 | 164.67 | 0.528 | - |
| PVR (mL) | 53.1 | 97.49 | 32.64 | 74.79 | 0.379 | - |
| CMG | ||||||
| First desire (mL) | 250.59 | 111.57 | 276.07 | 108.54 | 0.056 | - |
| Normal desire (mL) | 403.16 | 100.62 | 397.16 | 123.54 | 0.851 | - |
| UDS capacity (mL) | 559.31 | 132.77 | 552.15 | 66.87 | 0.802 | - |
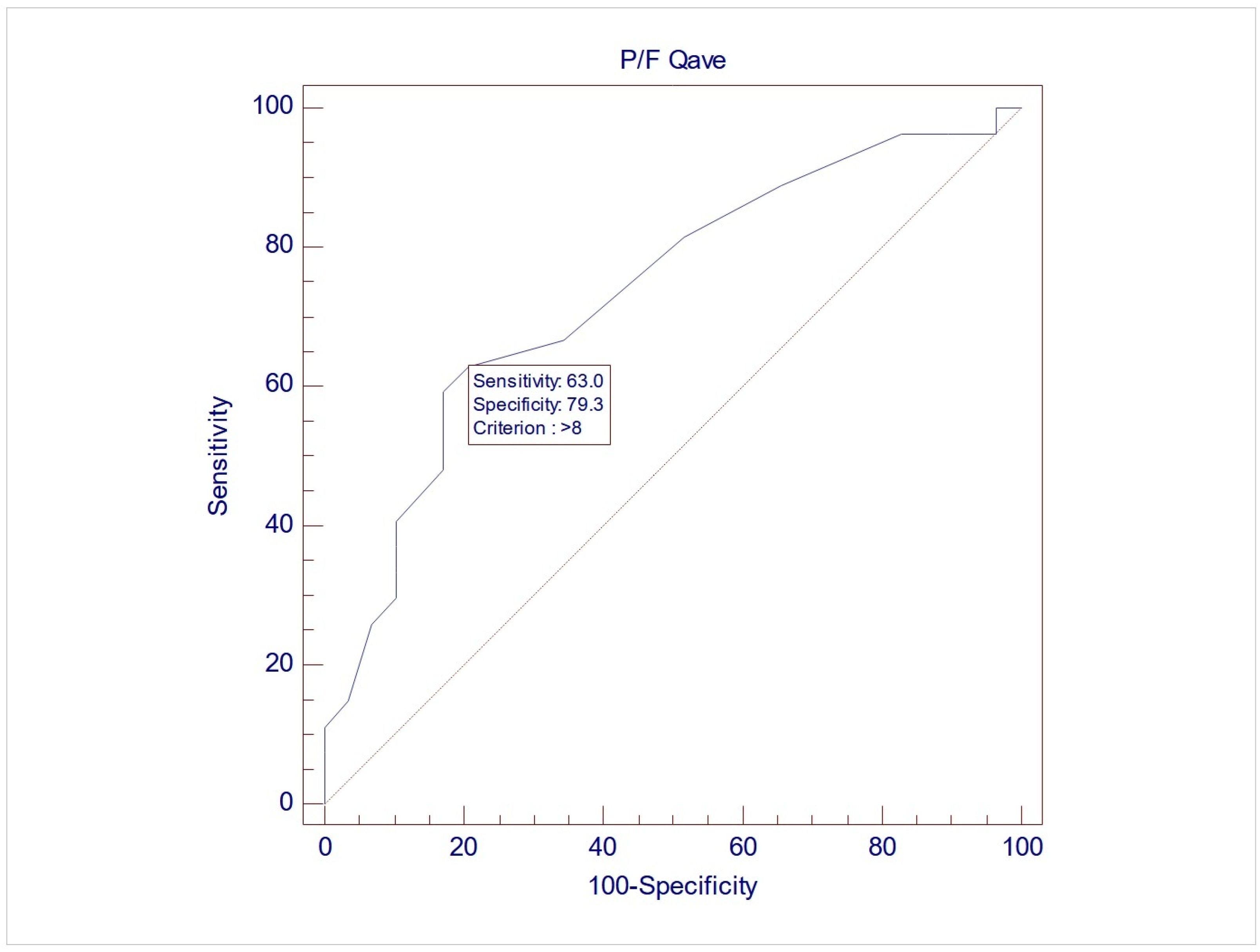
| Pressure flow | ||||||
| Qave (mL/s) | 7.24 | 3.75 | 11.56 | 5.98 | 0.0019 * | 1.66–6.97 |
| Qmax (mL/s) | 19.45 | 10.65 | 23.68 | 11.41 | 0.1533 | - |
| PVR (mL) | 87.93 | 95.33 | 42.14 | 69.46 | 0.0435 * | −90.19–−1.38 |
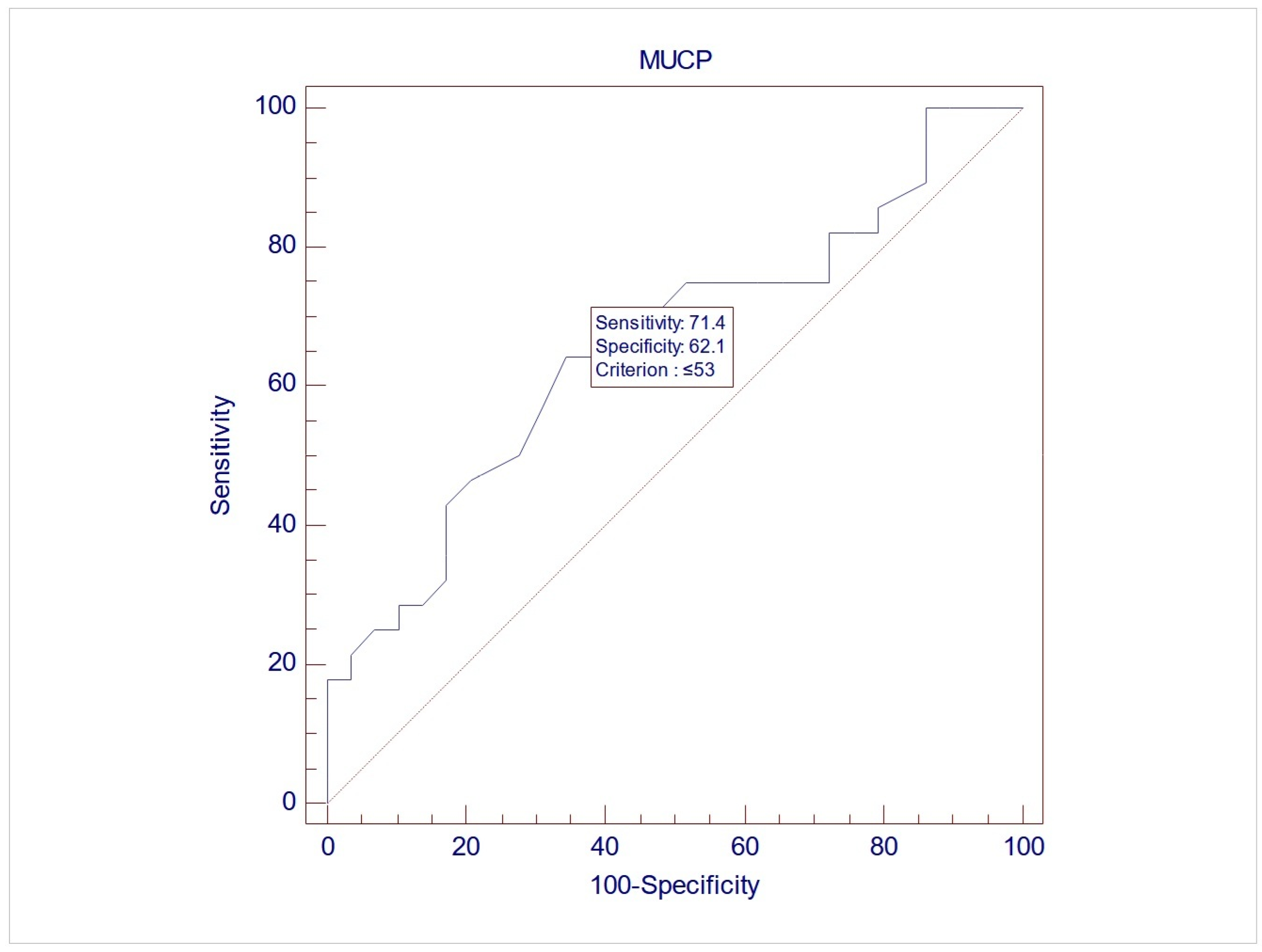
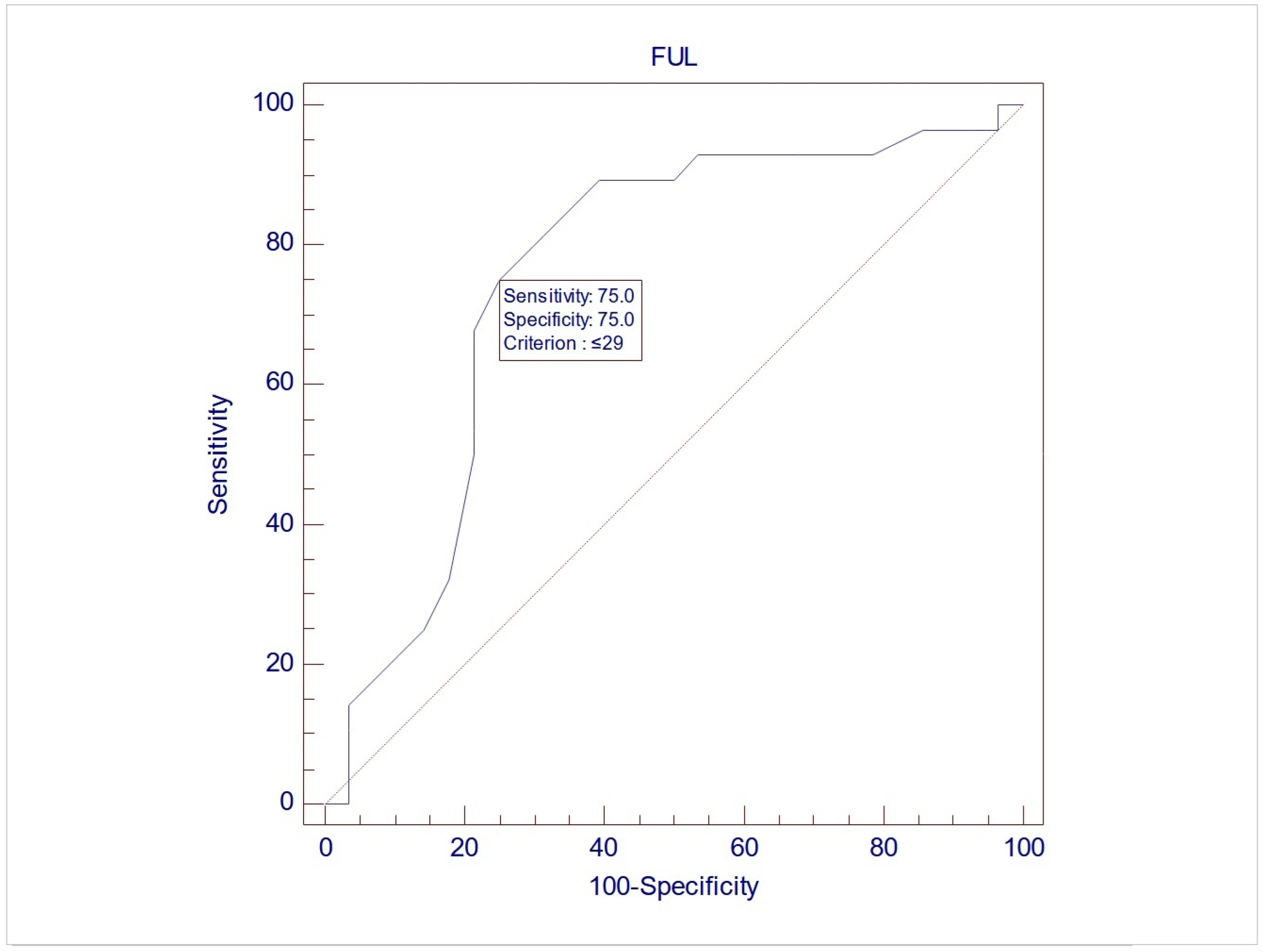
| UPP | ||||||
| MUCP (cmH2O) | 68.58 | 36.03 | 51.5 | 23.1 | 0.0383 * | −33.22–−0.95 |
| FUL (cm) | 30.89 | 5.36 | 26.88 | 4.51 | 0.0037 * | −6.66–−1.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantazis, K.; Mikos, T.; Tsiapakidou, S.; Theodoulidis, I.; Petousis, S.; Dinas, K.; Schiattarella, A.; Laganà, A.S.; Athanasiadis, A.P. Are Urethral Pressure Profile Measurements Effective in Diagnosing Urodynamic Stress Incontinence in Women Presenting with Stress or Mixed Urinary Incontinence? Results from a Cross-Sectional Study. Medicina 2025, 61, 1206. https://doi.org/10.3390/medicina61071206
Pantazis K, Mikos T, Tsiapakidou S, Theodoulidis I, Petousis S, Dinas K, Schiattarella A, Laganà AS, Athanasiadis AP. Are Urethral Pressure Profile Measurements Effective in Diagnosing Urodynamic Stress Incontinence in Women Presenting with Stress or Mixed Urinary Incontinence? Results from a Cross-Sectional Study. Medicina. 2025; 61(7):1206. https://doi.org/10.3390/medicina61071206
Chicago/Turabian StylePantazis, Konstantinos, Themistoklis Mikos, Sofia Tsiapakidou, Iakovos Theodoulidis, Stamatios Petousis, Konstantinos Dinas, Antonio Schiattarella, Antonio Simone Laganà, and Apostolos P. Athanasiadis. 2025. "Are Urethral Pressure Profile Measurements Effective in Diagnosing Urodynamic Stress Incontinence in Women Presenting with Stress or Mixed Urinary Incontinence? Results from a Cross-Sectional Study" Medicina 61, no. 7: 1206. https://doi.org/10.3390/medicina61071206
APA StylePantazis, K., Mikos, T., Tsiapakidou, S., Theodoulidis, I., Petousis, S., Dinas, K., Schiattarella, A., Laganà, A. S., & Athanasiadis, A. P. (2025). Are Urethral Pressure Profile Measurements Effective in Diagnosing Urodynamic Stress Incontinence in Women Presenting with Stress or Mixed Urinary Incontinence? Results from a Cross-Sectional Study. Medicina, 61(7), 1206. https://doi.org/10.3390/medicina61071206