
Prognostic Role of Inflammatory and Nutritional Indices in NSCLC Patients Treated with Immune Checkpoint Inhibitors: Retrospective, Multicenter, Turkish Oncology Group Study of Overall and Elderly Populations
 , , , , , , , , ,
, , , , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Methods
Patients
2.2. Prognostic Nutritional Index (PNI) and Geriatric Nutritional Index (GNRI)
Inflammatory-Based Indices
- Neutrophil–Lymphocyte Ratio (NLR): Neutrophil count/lymphocyte count
- Platelet–Lymphocyte Ratio (PLR): Platelet count/lymphocyte count
- Inflammatory Burden Index (IBI): CRP (mg/L) × neutrophil-to-lymphocyte ratio
2.3. Statistical Analysis
2.4. Optimal Cut-Off Values for Prognostic Markers for Overall Survival
3. Results
3.1. Demographic and Clinicopathologic Characteristics of Patients
3.2. Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index. |
| CRP | C-Reactive Protein. |
| ECOG PS | Eastern Cooperative Oncology Group Performance Status. |
| GNRI | Geriatric Nutritional Risk Index. |
| HR | Hazard Ratio. |
| IBI | Inflammatory Burden Index. |
| ICIs | Immune Checkpoint Inhibitors. |
| NLR | Neutrophil-to-Lymphocyte Ratio. |
| NOS | Not Otherwise Specified |
| NSCLC | Non-Small-Cell Lung Cancer. |
| OS | Overall Survival. |
| PD-1 | Programmed Death-1. |
| PD-L1 | Programmed Death Ligand-1. |
| PFS | Progression-Free Survival. |
| PLR | Platelet-to-Lymphocyte Ratio. |
| PNI | Prognostic Nutritional Index. |
| ROC | Receiver Operating Characteristic. |
| TNM | Tumor Node Metastasis. |
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meyer, M.L.; Fitzgerald, B.G.; Paz-Ares, L.; Cappuzzo, F.; Jänne, P.A.; Peters, S.; Hirsch, F.R. New promises and challenges in the treatment of advanced non-small-cell lung cancer. Lancet 2024, 404, 803–822. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, C.; Yang, R.; Jin, J.; Liu, D.; Li, W. Prognostic Value of the Geriatric Nutritional Risk Index in Non-Small Cell Lung Cancer Patients: A Systematic Review and Meta-Analysis. Front Oncol. 2022, 11, 794862. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Y.; Chen, Y.; Guo, C.; Li, S.; Huang, C. Systemic immune-inflammation index as a predictor of survival in non-small cell lung cancer patients undergoing immune checkpoint inhibition: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2025, 210, 104669. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Chen, S.W.; Chiang, Y.S. Prognostic role of geriatric nutritional risk index (GNRI) and controlling nutritional status (CONUT) on outcomes in patients with head and neck cancer: A systematic review and meta-analysis. BMC Cancer 2025, 25, 242. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peterson, C.M.; Thomas, D.M.; Blackburn, G.L.; Heymsfield, S.B. Universal equation for estimating ideal body weight and body weight at any BMI. Am. J. Clin. Nutr. 2016, 103, 1197–1203, Erratum in Am. J. Clin. Nutr. 2017, 105, 772. https://doi.org/10.3945/ajcn.116.151985. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, W.; Li, M.; Lian, S.; Hou, X.; Ling, Y. Geriatric nutritional risk index as a predictor for postoperative complications in patients with solid cancers: A meta-analysis. Front. Oncol. 2024, 14, 1266291. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Chen, J.-H.; Iskandar, E.A.; Cai, S.I.; Chen, C.-Q.; Wu, H.; Xu, J.-B.; He, Y.-L. Significance of Onodera’s prognostic nutritional index in patients with colorectal cancer: A large cohort study in a single Chinese institution. Tumour. Biol. 2016, 37, 3277–3283. [Google Scholar] [CrossRef]
- Ida, N.; Nakamura, K.; Saijo, M.; Kusumoto, T.; Masuyama, H. Prognostic nutritional index as a predictor of survival in patients with recurrent cervical cancer. Mol. Clin. Oncol. 2018, 8, 257–263. [Google Scholar] [CrossRef]
- Demir, A.; Alan, O.; Koca, S.; Surmeli, H. The relationship between the prognostic nutritional index and overall survival in elderly patients with epithelial ovarian cancer. ejmi 2020, 4, 269–273. [Google Scholar] [CrossRef]
- Alan, O.; Telli, T.A.; Basoğlu, T.; Arikan, R.; Demircan, N.C.; Ercelep, O.; Sakar, M.; Bozkurt, S.; Atasoy, B.M.; Dane, F.; et al. Impact of prognostic nutritional index on survival in recurrent glioblastoma. Neurocir. (Engl. Ed.) 2022, 33, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.; Curtis, A. Current insights in nutrition assessment and intervention for malnutrition or muscle loss in people with lung cancer: A narrative review. Adv. Nutr. 2022, 13, 2420–2432. [Google Scholar] [CrossRef]
- Zhang, Q.; Bao, J.; Zhu, Z.Y.; Jin, M.X. Prognostic nutritional index as a prognostic factor in lung cancer patients receiving chemotherapy: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5636–5652. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, Y.; Yang, P.; Xu, L.; Liu, S.; Zhang, S.; Weng, X. Correlation of the controlling nutritional status score and the prognostic nutritional index with the prognosis of patients treated with radiotherapy for small-cell lung cancer. Ann. Palliat. Med. 2021, 10, 11635–11642. [Google Scholar] [CrossRef]
- Matsubara, T.; Takamori, S.; Haratake, N.; Toyozawa, R.; Miura, N.; Shimokawa, M.; Yamaguchi, M.; Seto, T.; Takenoyama, M. The impact of immune-inflammation-nutritional parameters on the prognosis of non-small cell lung cancer patients treated with atezolizumab. J. Thorac. Dis. 2020, 12, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Fang, Q.; Yu, J.; Li, W.; Luo, J.; Deng, Q.; Chen, B.; He, Y.; Zhang, J.; Zhou, C. Prognostic value of inflammatory and nutritional indexes among advanced NSCLC patients receiving PD-1 inhibitor therapy. Clin. Exp. Pharmacol. Physiol. 2023, 50, 178–190. [Google Scholar] [CrossRef]
- Yan, X.; Wang, J.; Mao, J.; Wang, Y.; Wang, X.; Yang, M.; Qiao, H. Identification of prognostic nutritional index as a reliable prognostic indicator for advanced lung cancer patients receiving immune checkpoint inhibitors. Front. Nutr. 2023, 10, 1213255. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Qi, W.X.; Xiang, Y.; Zhao, S.; Chen, J. Assessment of systematic inflammatory and nutritional indexes in extensive-stage small-cell lung cancer treated with firstline chemotherapy and atezolizumab. Cancer Immunol. Immunother. 2021, 70, 3199–3206. [Google Scholar] [CrossRef]
- Shijubou, N.; Sumi, T.; Yamada, Y.; Nakata, H.; Mori, Y.; Chiba, H. Immunological and nutritional predictive factors in patients receiving pembrolizumab for the first-line treatment of non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2022, 148, 1893–1901. [Google Scholar] [CrossRef]
- Stares, M.; Ding, T.E.; Stratton, C.; Thomson, F.; Baxter, M.; Cagney, H.; Cumming, K.; Swan, A.; Ross, F.; Barrie, C.; et al. Biomarkers of systemic inflammation predict survival with first-line immune checkpoint inhibitors in non-small-cell lung cancer. ESMO Open 2022, 7, 100445. [Google Scholar] [CrossRef] [PubMed]
- Zaitsu, J.; Yamashita, Y.; Ishikawa, A.; Saito, A.; Kagimoto, A.; Mimura, T.; Hirakawa, T.; Mito, M.; Fukuhara, K.; Senoo, T.; et al. Systemic inflammatory score predicts response and prognosis in patients with lung cancer treated with immunotherapy. Anticancer Res. 2021, 41, 3673–3682. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Wang, Y.; Liu, F.; Qiu, X.; Zhang, X.; Fang, C.; Qian, X.; Li, Y. Peripheral blood markers predictive of outcome and immune-related adverse events in advanced non-small cell lung cancer treated with PD-1 inhibitors. Cancer Immunol. Immunother. 2020, 69, 1813–1822. [Google Scholar] [CrossRef]
- Shoji, F.; Takeoka, H.; Kozuma, Y.; Toyokawa, G.; Yamazaki, K.; Ichiki, M.; Takeo, S. Pretreatment prognostic nutritional index as a novel biomarker in non-small cell lung cancer patients treated with immune checkpoint inhibitors. Lung Cancer 2019, 136, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Yang, M.; Liu, Z.; Li, G.; Li, B.; Li, C.; Xiao, L.; Zhou, J. Geriatric Nutritional Risk Index as a prognostic factor of patients with non-small cell lung cancer: A meta-analysis. Horm. Metab. Res. 2022, 54, 604–612. [Google Scholar] [CrossRef]
- Karayama, M.; Inoue, Y.; Yasui, H.; Hozumi, H.; Suzuki, Y.; Furuhashi, K.; Fujisawa, T.; Enomoto, N.; Nakamura, Y.; Inui, N.; et al. Association of the Geriatric Nutritional Risk Index with the survival of patients with non-small-cell lung cancer after platinum-based chemotherapy. BMC Pulm. Med. 2021, 21, 409. [Google Scholar] [CrossRef]
- Sonehara, K.; Tateishi, K.; Araki, T.; Komatsu, M.; Yamamoto, H.; Hanaoka, M. Prognostic value of the geriatric nutritional risk index among patients with previously treated advanced non-small cell lung cancer who subsequently underwent immunotherapy. Thorac. Cancer 2021, 12, 1366–1372. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jiang, S.; Yang, A.; Yang, F.; Zhu, X.; Chen, X.; Li, Z.; Yao, Y.; Xu, S.; Yang, Z.; Mo, N.; et al. The Geriatric Nutritional Risk Index as a prognostic factor in patients treated with immune checkpoint inhibitors with non-small-cell lung cancer. J. Thorac. Dis. 2024, 16, 5222–5237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karayama, M.; Inoue, Y.; Yoshimura, K.; Hozumi, H.; Suzuki, Y.; Furuhashi, K.; Fujisawa, T.; Enomoto, N.; Nakamura, Y.; Inui, N.; et al. Association of the Geriatric Nutritional Risk Index with the Survival of Patients with Non-Small Cell Lung Cancer After Nivolumab Therapy. J. Immunother. 2022, 45, 125–131. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shimizu, A.; Fukasawa, M.; Mitani, K.; Goto, K.; Wakamoto, A.; Hatsuyama, T.; Hoshi, T.; Hasegawa, I.; Sato, H. Association of Geriatric Nutritional Risk Index with Immune Checkpoint Inhibitor Treatment Duration and Adverse Events in Lung Cancer. In Vivo 2024, 38, 418–424. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hirabayashi, T.; Sonehara, K.; Ozawa, R.; Hachiya, T.; Nozawa, S.; Agatsuma, T.; Yamamoto, H.; Kato, A.; Matsuo, A.; Araki, T.; et al. Prognostic Value of the Geriatric Nutritional Risk Index in Previously Untreated Patients with Advanced Non-Small Cell Lung Cancer Treated with a Combination Therapy of Anti-PD-1/-PD-L1 Antibodies and Platinum-Based Chemotherapy: A Multicenter Retrospective Study. Oncology 2024, 102, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Karadoğan, D.; Telatar, T.G.; Kaya, İ.; Atlı, S.; Kabil, N.K.; Marım, F.; Şenel, M.Y.; Yüksel, A.; Yalçın, B.; Gültekin, Ö.; et al. Immediately scheduled for an appointment to smoking cessation clinics: Key to quitting smoking in chronic airway disease—A multicenter randomized study. Tob. Induc. Dis. 2025, 23, 76. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 196 (%) | |
|---|---|---|
| Age (years) | Median (range) | 65 (23–88) |
| ≥65 | 101 (51.5) | |
| Gender | Female | 29 (14.8) |
| Male | 167 (85.2) | |
| Smoking | Never a smoker | 30 (15.3) |
| Ex-smoker | 114 (58.2) | |
| Active smoker | 52 (26.5) | |
| Smoking duration (pack/years) (median) (range) | 40 (10–120) | |
| ECOG PS | PS 0 | 53 (27) |
| PS 1 | 130 (66.3) | |
| PS ≥ 2 | 13 (6.7) | |
| Body mass index (kg/m2) (median) (range) | 24.4 (14.8–37.04) | |
| Histopathology | Adenocarcinoma | 101 (51.5) |
| Squamous cell carcinoma | 82 (41.8) | |
| NOS | 13 (6.6) | |
| Stage at diagnosis | Stage 1 | 10 (5.1%) |
| Stage 2 | 35 (17.9%) | |
| Stage 3 | 52 (26.5%) | |
| Stage 4 | 99 (50.5%) | |
| PD-L1 status | PD-L1 < 1% | 67 (34.6) |
| PD-L1 ≥ 1% | 69 (35.2) | |
| Unknown | 60 (30.6) | |
| PD-L1 level (median %) (range) | 35 (1–95) | |
| Prognostic Nutritional Index (PNI) (median) (range) | 45.2 (23.0–73.9) | |
| Geriatric Nutritional Index (GNR) (median) (range) | 103.8 (64.6–139.31) | |
| Inflammatory Burden Index (IBI) (median) (range) | 60.2 (0.17–2362.5) | |
| Neutrophil/Lymphocyte Ratio (NLR) (median) (range) | 3.7 (0.9–21.5) | |
| Platelet/Lymphocyte Ratio (PLR) (median) (range) | 196.8 (26.6–1970) | |
| Status | Exitus | 74 (37.8) |
| Alive | 122 (62.2) | |
| Overall survival | Median (months) | 12.4 (95% CI: 8.4–16.4) |
| 1 years (%) | 53 | |
| 2 years (%) | 25 | |
| Variables | Median OS (Months) (95% CI) | Univariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p | |||
| Age | ≥65 | 12.1 (8.7–15.5) | 1.2(0.7–1.9) | 0.37 |
| <65 | 14.2 (6.5–21.9) | |||
| Gender | Female | 9.7 (not calculated) | 0.8 (0.4–1.5) | 0.55 |
| Male | 14.2 (8.8–19.6) | |||
| BMI | <25 | 11.9 (8.0–15.8) | 0.97 (0.92–1.0) | 0.41 |
| ≥25 | 17.8 (6.1–29.6) | |||
| Smoking | Never a smoker | 7.2 (6.1–8.3) | 0.6 (0.1–1.1) | 0.21 |
| Active-ex | 14.2 (9.1–19.3) | |||
| ECOG PS | PS 0–1 | 14.2 (8.8–19.6) | 4.2 (2.1–8.4) | <0.01 |
| PS ≥ 2 | 5.1 (0.84–9.4) | |||
| PD-L1 | PD-L1 < 1% | 10.6 (6.7–14.5) | 1.02 (0.59–1.7) | 0.93 |
| PD-L1 ≥ 1% | 12.1 (6.8–17.4) | |||
| PD-L1 < 50% | 10.6 (7.8–13.4) | 0.9 (0.5–1.8) | 0.90 | |
| PD-L1 ≥ 50% | 14.6 (3.5–25.7) | |||
| NLR | <3.3 | 17.8 (10.6–25.1) | 2.5 (1.5–4.2) | <0.01 |
| ≥3.3 | 8.03 (4.7–11.3) | |||
| PLR | <196.8 | 17.8 (10.5–25.2) | 1.7 (1.1–2.8) | 0.01 |
| ≥196.8 | 9.7 (4.6–14.9) | |||
| PNI | <45.2 | 7.1 (1.5–12.8) | 0.5 (0.3–0.8) | 0.004 |
| ≥45.2 | 17.8 (11.7–24.03) | |||
| IBI | <60.2 | 11.9 (3.4–20.3) | 1.4 (0.8–2.3) | 0.13 |
| ≥60.2 | 12.1 (5.9–18.3) | |||
| GNRI | <98.0 | 5.1 (2.3–7.8) | 0.4 (0.24–0.8) | 0.01 |
| ≥98.0 | Not reached | |||
| Variables | Median OS (Months) (95% CI) | Univariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p | |||
| Gender | Female | Not reached | 1.5 (0.5–4.2) | 0.43 |
| Male | 12.1 (9.3–14.9) | |||
| BMI | <25 | 14.6 (8.4–20.7) | 1.07 (0.56–2.0) | 0.82 |
| ≥25 | 9.8 (6.6–13.0) | |||
| Smoking | Never a smoker | Not reached | 1.1 (0.3–3.7) | 0.82 |
| Active–ex | 12.1 (8.6–15.6) | |||
| ECOG PS | PS 0–1 | 12.4 (9.7–15.7) | 3.04 (1.0–8.6) | 0.03 |
| PS ≥ 2 | 5,1 (1.0–11.4) | |||
| PD-L1 | PD-L1 < 1% | 10.1 (5.6–14.5) | 0.8 (0.4–1.7) | 0.67 |
| PD-L1 ≥ 1% | 14.6 (9.1–20.1) | |||
| PD-L1 < 50% | 12.4 (9.1–15.1) | 0.4 (0.1–1.5) | 0.22 | |
| PD-L1 ≥ 50% | 14.6 (1.0–30.9) | |||
| NLR | <3.3 | Not reached | 1.6 (0.8–3.2) | 0.12 |
| ≥3.3 | 12.1 (4.9–19.3) | |||
| PLR | <196.8 | 12.1 (9.6–14.6) | 1.5 (0.8–2.8) | 0.17 |
| ≥196.8 | 14.6 (0.65–28.6) | |||
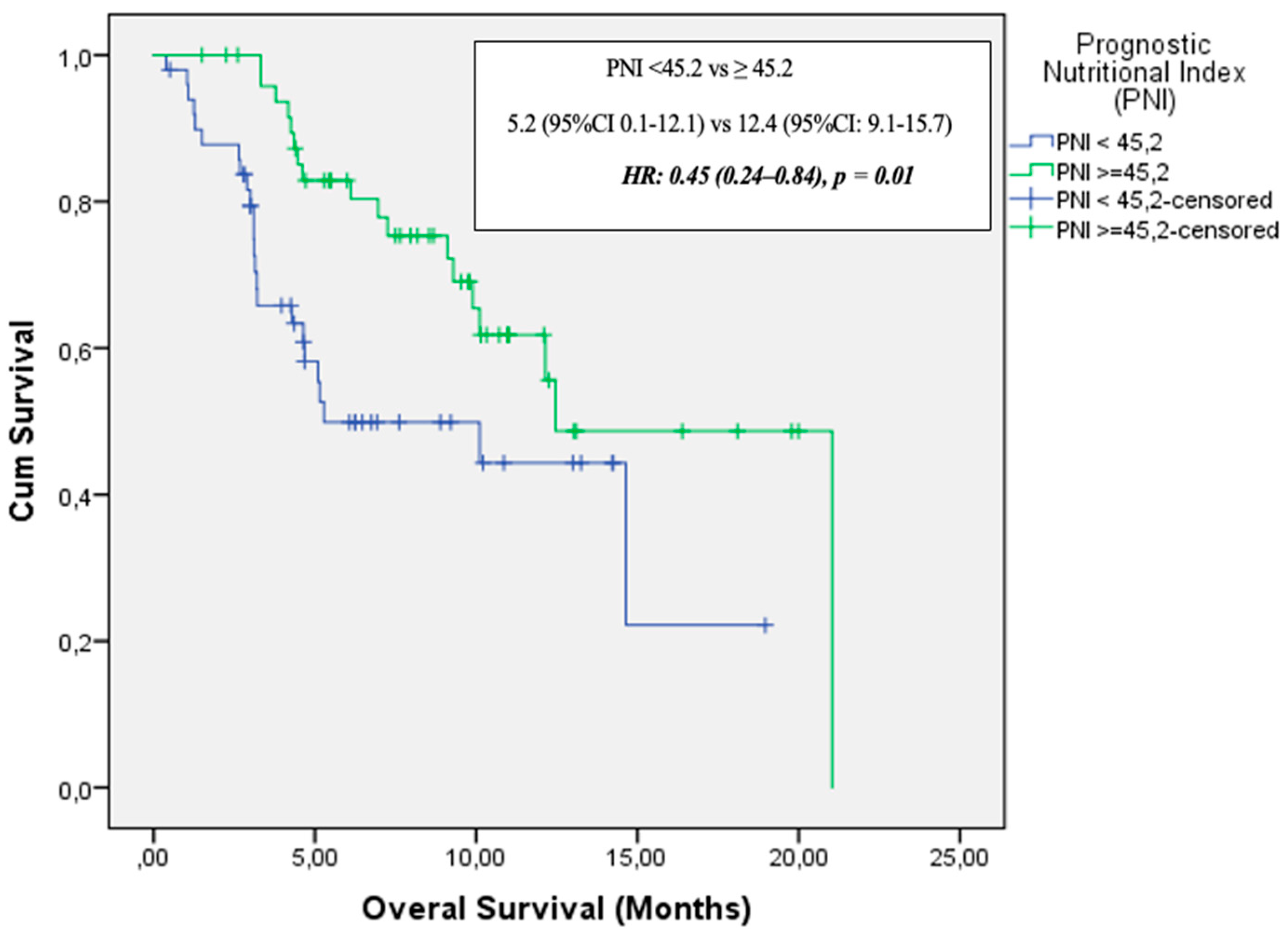
| PNI | <45.2 | 5.2 (0.1–12.1) | 0.4 (0.2–1.1) | 0.01 |
| ≥45.2 | 12.4 (9.1–15.7) | |||
| IBI | <60.2 | 10.1 (6.1–14.08) | 1.4 (0.7–2.7) | 0.28 |
| ≥60.2 | 12.1 (5.7–18.5) | |||
| GNRI | <98.0 | 5.1 (2.3–7.8) | 0.4 (0.24–0.8) | 0.01 |
| ≥98.0 | Not reached | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alan, O.; Telli, T.A.; Akbas, S.; Isik, S.; Çavdar, E.; Karaboyun, K.; Merc Cetinkaya, A.; Ekinci, F.; Erdoğan, A.P.; Büyükşimsek, M.; et al. Prognostic Role of Inflammatory and Nutritional Indices in NSCLC Patients Treated with Immune Checkpoint Inhibitors: Retrospective, Multicenter, Turkish Oncology Group Study of Overall and Elderly Populations. Medicina 2025, 61, 1160. https://doi.org/10.3390/medicina61071160
Alan O, Telli TA, Akbas S, Isik S, Çavdar E, Karaboyun K, Merc Cetinkaya A, Ekinci F, Erdoğan AP, Büyükşimsek M, et al. Prognostic Role of Inflammatory and Nutritional Indices in NSCLC Patients Treated with Immune Checkpoint Inhibitors: Retrospective, Multicenter, Turkish Oncology Group Study of Overall and Elderly Populations. Medicina. 2025; 61(7):1160. https://doi.org/10.3390/medicina61071160
Chicago/Turabian StyleAlan, Ozkan, Tugba Akın Telli, Sinem Akbas, Selver Isik, Eyyüb Çavdar, Kubilay Karaboyun, Aysegül Merc Cetinkaya, Ferhat Ekinci, Atike Pınar Erdoğan, Mahmut Büyükşimsek, and et al. 2025. "Prognostic Role of Inflammatory and Nutritional Indices in NSCLC Patients Treated with Immune Checkpoint Inhibitors: Retrospective, Multicenter, Turkish Oncology Group Study of Overall and Elderly Populations" Medicina 61, no. 7: 1160. https://doi.org/10.3390/medicina61071160
APA StyleAlan, O., Telli, T. A., Akbas, S., Isik, S., Çavdar, E., Karaboyun, K., Merc Cetinkaya, A., Ekinci, F., Erdoğan, A. P., Büyükşimsek, M., Er, M. M., Karakurt Eryilmaz, M., Güçlü Kantar, T., Gököz Doğu, G., Sakalar, T., Bayram, E., Inal, A., Akdağ Kahvecioğlu, F., Hacibekiroğlu, İ., ... Yumuk, P. F. (2025). Prognostic Role of Inflammatory and Nutritional Indices in NSCLC Patients Treated with Immune Checkpoint Inhibitors: Retrospective, Multicenter, Turkish Oncology Group Study of Overall and Elderly Populations. Medicina, 61(7), 1160. https://doi.org/10.3390/medicina61071160