

Mindfulness Reduces Adolescent Depression Through Stress Appraisal and Cognitive Reactivity: Evidence from a Four-Wave Longitudinal Study


Abstract
1. Introduction
1.1. Stressful Life Events and Depression
1.2. The Role of Mindfulness
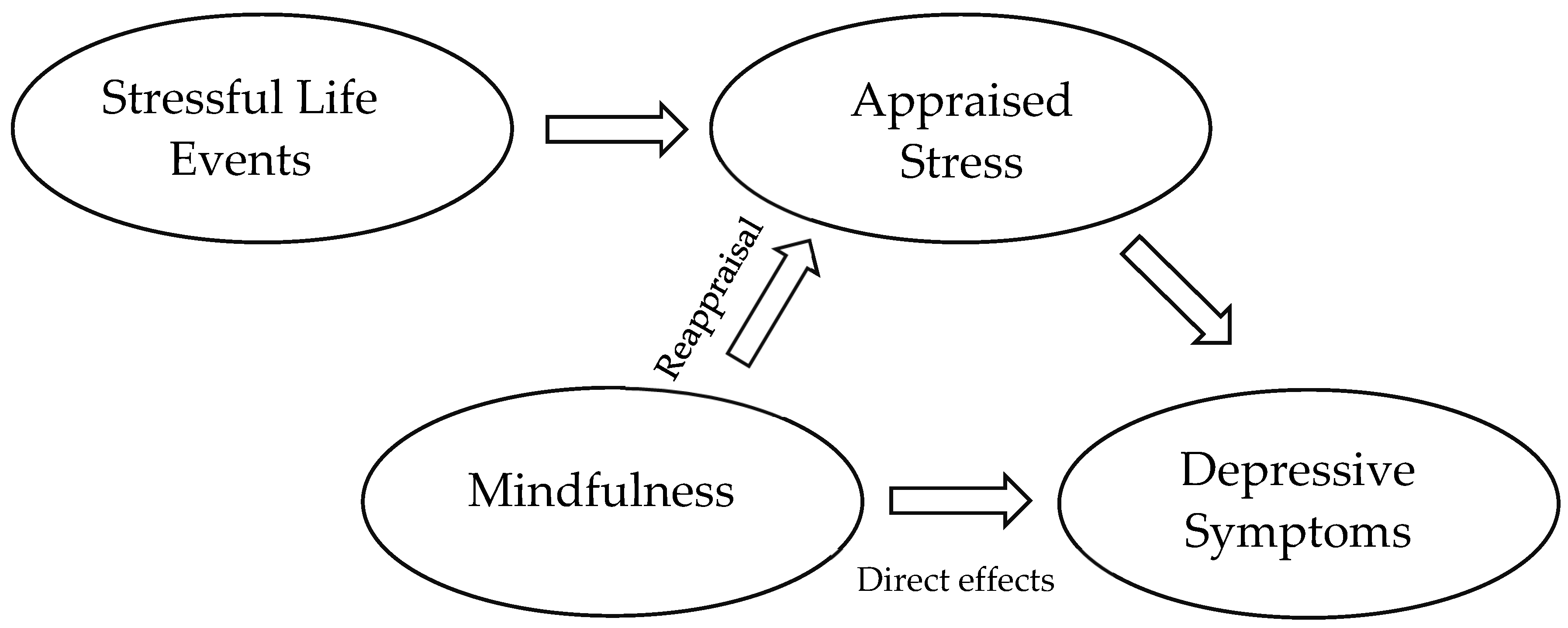
1.3. Mechanisms and Pathways of Mindfulness in Coping with Stress
1.4. The Current Study
- Indirectly, through the reappraisal of stressful events, thereby diminishing their perceived threat;
- Directly, through the modulation of cognitive processes such as rumination and emotional reactivity.
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Stressful Life Events
2.2.2. Reliability Considerations
2.2.3. Mindfulness
2.2.4. MAASA
2.2.5. CAMM
2.2.6. Depression
2.2.7. Analytic Strategy
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnett, J.J. Adolescent Storm and Stress, Reconsidered. Am. Psychol. 1999, 54, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Adolescence and Emerging Adulthood, 5th ed.; Pearson: Boston, MA, USA, 2012; p. 504. [Google Scholar] [CrossRef]
- Blakemore, S.J. Adolescence and Mental Health. Lancet 2019, 393, 2030–2031. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in Adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef] [PubMed]
- Clayborne, Z.M.; Varin, M.; Colman, I. Systematic Review and Meta-Analysis: Adolescent Depression and Long-Term Psychosocial Outcomes. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 72–79. [Google Scholar] [CrossRef]
- Aalto-Setälä, T.; Marttunen, M.; Tuulio-Henriksson, A.; Poikolainen, K.; Lönnqvist, J. Depressive Symptoms in Adolescence as Predictors of Early Adulthood Depressive Disorders and Maladjustment. Am. J. Psychiatry 2002, 159, 1235–1237. [Google Scholar] [CrossRef]
- Pine, D.S.; Cohen, E.; Cohen, P.; Brook, J. Adolescent Depressive Symptoms as Predictors of Adult Depression: Moodiness or Mood Disorder? Am. J. Psychiatry 1999, 156, 133–135. [Google Scholar] [CrossRef]
- Copeland, W.E.; Alaie, I.; Jonsson, U.; Shanahan, L. Associations of Childhood and Adolescent Depression With Adult Psychiatric and Functional Outcomes. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 604–611. [Google Scholar] [CrossRef]
- Shorey, S.; Ng, E.D.; Wong, C.H.J. Global Prevalence of Depression and Elevated Depressive Symptoms among Adolescents: A Systematic Review and Meta-Analysis. Br. J. Clin. Psychol. 2022, 61, 287–305. [Google Scholar] [CrossRef]
- Cohen, S.; Murphy, M.L.M.; Prather, A.A. Ten Surprising Facts About Stressful Life Events and Disease Risk. Annu. Rev. Psychol. 2019, 70, 577–597. [Google Scholar] [CrossRef]
- Holmes, T.H.; Rahe, R.H. The Social Readjustment Rating Scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Hammen, C. Stress and Depression. Annu. Rev. Clin. Psychol. 2005, 1, 293–319. [Google Scholar] [CrossRef] [PubMed]
- Hammen, C.; Kim, E.Y.; Eberhart, N.K.; Brennan, P.A. Chronic and Acute Stress and the Prediction of Major Depression in Women. Depress. Anxiety 2009, 26, 718–723. [Google Scholar] [CrossRef]
- Kendler, K.S.; Gardner, C.O. Dependent Stressful Life Events and Prior Depressive Episodes in the Prediction of Major Depression: The Problem of Causal Inference in Psychiatric Epidemiology. Arch. Gen. Psychiatry 2010, 67, 1120–1127. [Google Scholar] [CrossRef]
- Slavich, G.M. Life Stress and Health: A Review of Conceptual Issues and Recent Findings. Teach. Psychol. 2016, 43, 346–355. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging Adulthood: A Theory of Development from the Late Teens through the Twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The Age of Adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef]
- Crone, E.A.; Dahl, R.E. Understanding Adolescence as a Period of Social-Affective Engagement and Goal Flexibility. Nat. Rev. Neurosci. 2012, 13, 636–650. [Google Scholar] [CrossRef]
- Hollenstein, T.; Lougheed, J.P. Beyond Storm and Stress: Typicality, Transactions, Timing, and Temperament to Account for Adolescent Change. Am. Psychol. 2013, 68, 444–454. [Google Scholar] [CrossRef]
- Patalay, P.; Gage, S.H. Changes in Millennial Adolescent Mental Health and Health-Related Behaviours over 10 Years: A Population Cohort Comparison Study. Int. J. Epidemiol. 2019, 48, 1650–1664. [Google Scholar] [CrossRef]
- Silva, S.A.; Silva, S.U.; Ronca, D.B.; Gonçalves, V.S.S.; Dutra, E.S.; Carvalho, K.M.B. Common Mental Disorders Prevalence in Adolescents: A Systematic Review and Metaanalyses. PLoS ONE 2020, 15, e0232007. [Google Scholar] [CrossRef] [PubMed]
- Milas, G.; Ribar, M.; Ćavar, F. Why Are Adolescent Girls More Prone to Stress-induced Depression? Testing Moderation, Mediation, and Reciprocal Causality in a Three-wave Longitudinal Study. J. Res. Adolesc. 2025, 35, e70015. [Google Scholar] [CrossRef] [PubMed]
- Dunning, D.L.; Griffiths, K.; Kuyken, W.; Crane, C.; Foulkes, L.; Parker, J.; Dalgleish, T. Research Review: The Effects of Mindfulness-Based Interventions on Cognition and Mental Health in Children and Adolescents—A Meta-Analysis of Randomized Controlled Trials. J. Child Psychol. Psychiatry 2019, 60, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Kallapiran, K.; Koo, S.; Kirubakaran, R.; Hancock, K. Review: Effectiveness of Mindfulness in Improving Mental Health Symptoms of Children and Adolescents: A Meta-Analysis. Child Adolesc. Ment. Health 2015, 20, 182–194. [Google Scholar] [CrossRef]
- Fulambarkar, N.; Seo, B.; Testerman, A.; Rees, M.; Bausback, K.; Bunge, E. Review: Meta-Analysis on Mindfulness-Based Interventions for Adolescents’ Stress, Depression, and Anxiety in School Settings: A Cautionary Tale. Child Adolesc. Ment. Health 2023, 28, 307–317. [Google Scholar] [CrossRef]
- Royuela-Colomer, E.; Fernández-González, L.; Orue, I. Longitudinal Associations between Internalizing Symptoms, Dispositional Mindfulness, Rumination and Impulsivity in Adolescents. J. Youth Adolesc. 2021, 50, 2067–2078. [Google Scholar] [CrossRef]
- Zhang, B.; Yan, X.; Zhao, F.; Yuan, F. The Relationship Between Perceived Stress and Adolescent Depression: The Roles of Social Support and Gender. Soc. Indic. Res. 2015, 123, 501–518. [Google Scholar] [CrossRef]
- Broderick, P.C.; Metz, S. Learning to BREATHE: A Pilot Trial of a Mindfulness Curriculum for Adolescents. Adv. Sch. Ment. Health Promot. 2009, 2, 35–46. [Google Scholar] [CrossRef]
- Ćavar, F.; Mihić, J.; Milas, G. Exploring the Effects of Mindfulness on Adolescent Depression—Findings from a Longitudinal Study. Healthcare 2025, 13, 906. [Google Scholar] [CrossRef]
- Garland, E.L.; Hanley, A.; Farb, N.A.; Froeliger, B. State Mindfulness During Meditation Predicts Enhanced Cognitive Reappraisal. Mindfulness 2015, 6, 234–242. [Google Scholar] [CrossRef]
- Garland, E.L.; Gaylord, S.A.; Fredrickson, B.L. Positive Reappraisal Mediates the Stress-Reductive Effects of Mindfulness: An Upward Spiral Process. Mindfulness 2011, 2, 59–67. [Google Scholar] [CrossRef]
- Milas, G.; Ćavar, F.; Ribar, M. How Much Stressful Life Events Really Matter? Conceptual and Methodological Difficulties in Assessing the Impact of Self-Reported Events on Adolescents’ Subjective Stress. Stress Health 2024, 40, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Moya-Higueras, J.; Cuevas, A.; Marques-Feixa, L.; Mezquita, L.; Mayoral, M.; Fañanás, L.; Ortet, G.; Ibáñez, M.I. Recent Stressful Life Events (SLE) and Adolescent Mental Health: Initial Validation of the LEIA, a New Checklist for SLE Assessment According to Their Severity, Interpersonal, and Dependent Nature. Assessment 2020, 27, 1777–1795. [Google Scholar] [CrossRef]
- Newcomb, M.D.; Huba, G.J.; Bentler, P.M. A Multidimensional Assessment of Stressful Life Events among Adolescents: Derivation and Correlates. J. Health Soc. Behav. 1981, 22, 400–415. [Google Scholar] [CrossRef]
- Stikkelbroek, Y.; Bodden, D.H.M.; Kleinjan, M.; Reijnders, M.; Van Baar, A.L. Adolescent Depression and Negative Life Events, the Mediating Role of Cognitive Emotion Regulation. PLoS ONE 2016, 11, e0161062. [Google Scholar] [CrossRef]
- Brown, K.W.; West, A.M.; Loverich, T.M.; Biegel, G.M. Assessing Adolescent Mindfulness: Validation of an Adapted Mindful Attention Awareness Scale in Adolescent Normative and Psychiatric Populations. Psychol. Assess. 2011, 23, 1023–1033. [Google Scholar] [CrossRef]
- Greco, L.A.; Baer, R.A.; Smith, G.T. Assessing Mindfulness in Children and Adolescents: Development and Validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychol. Assess. 2011, 23, 606–614. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Little, R.J.A. A Test of Missing Completely at Random for Multivariate Data with Missing Values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Raykov, T.; Marcoulides, G.A. Identifying Useful Auxiliary Variables for Incomplete Data Analyses: A Note on a Group Difference Examination Approach. Educ. Psychol. Meas. 2014, 74, 537–550. [Google Scholar] [CrossRef]
- Enders, C.K. Missing Data: An Update on the State of the Art. Psychol. Methods 2023, 30, 322–339. [Google Scholar] [CrossRef] [PubMed]
- Putnick, D.L.; Bornstein, M.H. Measurement Invariance Conventions and Reporting: The State of the Art and Future Directions for Psychological Research. Dev. Rev. 2016, 41, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, J.L. AMOS 27 User’s Guide, AMOS 27; IBM SPSS: Chicago, IL, USA, 2020. [Google Scholar]
- Arbuckle, J.L. AMOS 4.0 User’s Guide; SPSS Inc. & Small Waters Corporation: Chicago, IL, USA, 1999; 470p, ISBN 978-1568272641. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Sivo, S.a.; Fan, X.; Witta, E.L.; Willse, J.T. The Search for “Optimal” Cutoff Properties: Fit Index Criteria in Structural Equation Modeling. J. Exp. Educ. 2006, 74, 267–288. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Knight, R.C.; Dunning, D.L.; Cotton, J.; Franckel, G.; Ahmed, S.P.; Blakemore, S.J.; Ford, T.; Kuyken, W.; Dalgleish, T.; Bennett, M.P. Investigation of the Mental Health and Cognitive Correlates of Psychological Decentering in Adolescence. Cogn. Emot. 2024, 39, 465–475. [Google Scholar] [CrossRef]
- De Vibe, M.; Solhaug, I.; Rosenvinge, J.H.; Tyssen, R.; Hanley, A.; Garland, E. Six-Year Positive Effects of a Mindfulness-Based Intervention on Mindfulness, Coping and Well-Being in Medical and Psychology Students; Results from a Randomized Controlled Trial. PLoS ONE 2018, 13, e0196053. [Google Scholar] [CrossRef]
- Carreres-Ponsoda, F.; Escartí, A.; Llopis-Goig, R.; Cortell-Tormo, J.M. The Effect of an Out-of-School Mindfulness Program on Adolescents’ Stress Reduction and Emotional Wellbeing. Cuad. Psicol. Deporte 2017, 17, 35–44. [Google Scholar]
- Tan, L.B.G.; Martin, G. Mind Full or Mindful: A Report on Mindfulness and Psychological Health in Healthy Adolescents. Int. J. Adolesc. Youth 2016, 21, 64–74. [Google Scholar] [CrossRef]
- Bluth, K.; Campo, R.A.; Pruteanu-Malinici, S.; Reams, A.; Mullarkey, M.; Broderick, P.C. A School-Based Mindfulness Pilot Study for Ethnically Diverse At-Risk Adolescents. Mindfulness 2016, 7, 90–104. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| N | Biological Sex | Age | School Type | ||||
|---|---|---|---|---|---|---|---|
| % Males | % Females | M | SD | % Vocational | % Gymnasium | ||
| Time 1 | 2486 | 48.83 | 51.17 | 15.91 | 0.74 | 60.12 | 39.88 |
| Time 2 | 1794 | 45.54 | 54.46 | 16.41 | 0.71 | 62.97 | 37.03 |
| Time 3 | 2319 | 45.75 | 54.25 | 16.80 | 0.76 | 54.91 | 45.09 |
| Time 4 | 1575 | 46.48 | 53.52 | 17.38 | 0.72 | 53.10 | 46.90 |
| M | SD | Min. | Max. | Reliability (Alpha) | |||
|---|---|---|---|---|---|---|---|
| Occurrence-based SLEs first wave | Health problems | 0.27 | 0.24 | 0.00 | 1.00 | 0.64 | |
| Bullying, harassment, and abuse | 0.33 | 0.29 | 0.00 | 1.00 | 0.66 | ||
| Problems at school | 0.26 | 0.18 | 0.00 | 1.00 | 0.56 | ||
| Relationship problems | 0.41 | 0.28 | 0.00 | 1.00 | 0.71 | ||
| Loss of loved ones | 0.22 | 0.20 | 0.00 | 1.00 | 0.45 | ||
| Health problems of close people | 0.33 | 0.30 | 0.00 | 1.00 | 0.66 | ||
| Family situation | 0.17 | 0.18 | 0.00 | 1.00 | 0.72 | ||
| TOTAL | 0.27 | 0.16 | 0.00 | 1.00 | 0.87 | ||
| Severity-based SLEs first wave | Health problems | 0.73 | 0.77 | 0.00 | 4.86 | 0.67 | |
| Bullying, harassment, and abuse | 0.76 | 0.89 | 0.00 | 5.00 | 0.72 | ||
| Problems at school | 0.62 | 0.52 | 0.00 | 5.00 | 0.56 | ||
| Relationship problems | 1.20 | 1.03 | 0.00 | 5.00 | 0.76 | ||
| Loss of loved ones | 0.74 | 0.80 | 0.00 | 5.00 | 0.50 | ||
| Health problems of close people | 0.98 | 1.06 | 0.00 | 5.00 | 0.72 | ||
| Family situation | 0.46 | 0.58 | 0.00 | 5.00 | 0.76 | ||
| TOTAL | 0.74 | 0.55 | 0.00 | 4.98 | 0.89 | ||
| Occurrence-based SLEs third wave | Health problems | 0.26 | 0.25 | 0.00 | 1.00 | 0.68 | |
| Bullying, harassment, and abuse | 0.30 | 0.30 | 0.00 | 1.00 | 0.70 | ||
| Problems at school | 0.25 | 0.19 | 0.00 | 1.00 | 0.63 | ||
| Relationship problems | 0.37 | 0.28 | 0.00 | 1.00 | 0.73 | ||
| Loss of loved ones | 0.19 | 0.21 | 0.00 | 1.00 | 0.52 | ||
| Health problems of close people | 0.27 | 0.30 | 0.00 | 1.00 | 0.70 | ||
| Family situation | 0.14 | 0.18 | 0.00 | 1.00 | 0.78 | ||
| TOTAL | 0.24 | 0.17 | 0.00 | 1.00 | 0.78 | ||
| Severity-based SLEs third wave | Health problems | 0.72 | 0.80 | 0.00 | 5.00 | 0.71 | |
| Bullying, harassment, and abuse | 0.71 | 0.89 | 0.00 | 5.00 | 0.73 | ||
| Problems at school | 0.58 | 0.55 | 0.00 | 5.00 | 0.66 | ||
| Relationship problems | 1.09 | 1.00 | 0.00 | 5.00 | 0.77 | ||
| Loss of loved ones | 0.62 | 0.77 | 0.00 | 5.00 | 0.54 | ||
| Health problems of close people | 0.79 | 0.99 | 0.00 | 5.00 | 0.73 | ||
| Family situation | 0.38 | 0.58 | 0.00 | 5.00 | 0.81 | ||
| TOTAL | 0.66 | 0.56 | 0.00 | 5.00 | 0.91 | ||
| Mindfulness | MAAS-A wave1 | 3.69 | 1.00 | 1.00 | 6.00 | 0.90 | |
| MAAS-A wave3 | 3.70 | 0.97 | 1.00 | 6.00 | 0.90 | ||
| CAMM wave1 | 2.24 | 0.84 | 0.00 | 4.00 | 0.87 | ||
| CAMM wave3 | 2.24 | 0.83 | 0.00 | 4.00 | 0.88 | ||
| PHQ-9 depression wave2 | 9.19 | 6.31 | 0.00 | 27.00 | 0.88 | ||
| PHQ-9 depression wave4 | 8.70 | 5.93 | 0.00 | 27.00 | 0.88 | ||
| MAASA Wave1 | MAASA Wave3 | CAMM Wave1 | CAMM Wave3 | PHQ-9 Wave2 | PHQ-9 Wave4 | ||
|---|---|---|---|---|---|---|---|
| Occurrence-based SLEs first wave | Health problems | −0.360 ** | −0.311 ** | −0.385 ** | −0.339 ** | 0.454 ** | 0.361 ** |
| Bullying, harassment, and abuse | −0.224 ** | −0.251 ** | −0.306 ** | −0.273 ** | 0.297 ** | 0.248 ** | |
| Problems at school | −0.126 ** | −0.211 ** | −0.141 ** | −0.154 ** | 0.212 ** | 0.202 ** | |
| Relationship problems | −0.230 ** | −0.192 ** | −0.282 ** | −0.199 ** | 0.261 ** | 0.252 ** | |
| Loss of loved ones | 0.001 | −0.114 | −0.025 | −0.012 | 0.115 ** | 0.064 | |
| Health problems of close people | −0.169 ** | −0.134 * | −0.261 ** | −0.176 ** | 0.208 ** | 0.232 ** | |
| Family situation | −0.247 ** | −0.167 ** | −0.281 ** | −0.223 ** | 0.289 ** | 0.244 ** | |
| TOTAL | −0.308 ** | −0.297 ** | −0.377 ** | −0.311 ** | 0.395 ** | 0.352 ** | |
| Severity-based SLEs first wave | Health problems | −0.414 ** | −0.359 ** | −0.499 ** | −0.411 ** | 0.549 ** | 0.426 ** |
| Bullying, harassment, and abuse | −0.311 ** | −0.258 ** | −0.394 ** | −0.341 ** | 0.383 ** | 0.332 ** | |
| Problems at school | −0.276 ** | −0.263 ** | −0.339 ** | −0.294 ** | 0.378 ** | 0.373 ** | |
| Relationship problems | −0.329 ** | −0.220 ** | −0.438 ** | −0.330 ** | 0.394 ** | 0.320 ** | |
| Loss of loved ones | −0.084 * | −0.142 * | −0.125 ** | −0.095 ** | 0.188 ** | 0.130 ** | |
| Health problems of close people | −0.230 ** | −0.146 * | −0.338 ** | −0.238 ** | 0.273 ** | 0.287 ** | |
| Family situation | −0.291 ** | −0.200 ** | −0.360 ** | −0.299 ** | 0.339 ** | 0.314 ** | |
| TOTAL | −0.407 ** | −0.324 ** | −0.517 ** | −0.419 ** | 0.502 ** | 0.440 ** | |
| Occurrence-based SLEs third wave | Health problems | −0.278 ** | −0.329 ** | −0.264 ** | −0.355 ** | 0.426 ** | 0.439 ** |
| Bullying, harassment, and abuse | −0.196 ** | −0.278 ** | −0.204 ** | −0.307 ** | 0.399 ** | 0.325 ** | |
| Problems at school | −0.121 ** | −0.145 ** | −0.077 * | −0.130 ** | 0.201 ** | 0.211 ** | |
| Relationship problems | −0.265 ** | −0.217 ** | −0.223 ** | −0.272 ** | 0.286 ** | 0.287 ** | |
| Loss of loved ones | −0.037 | −0.085 * | 0.046 | −0.024 | 0.137 ** | 0.045 | |
| Health problems of close people | −0.146 ** | −0.203 ** | −0.131 ** | −0.207 ** | 0.249 ** | 0.207 ** | |
| Family situation | −0.189 ** | −0.226 ** | −0.196 ** | −0.266 ** | 0.322 ** | 0.280 ** | |
| TOTAL | −0.259 ** | −0.322 ** | −0.232 ** | −0.336 ** | 0.419 ** | 0.390 ** | |
| Severity-based SLEs third wave | Health problems | −0.329 ** | −0.393 ** | −0.345 ** | −0.436 ** | 0.530 ** | 0.524 ** |
| Bullying, harassment, and abuse | −0.252 ** | −0.297 ** | −0.287 ** | −0.380 ** | 0.471 ** | 0.391 ** | |
| Problems at school | −0.176 ** | −0.240 ** | −0.170 ** | −0.274 ** | 0.344 ** | 0.323 ** | |
| Relationship problems | −0.342 ** | −0.294 ** | −0.314 ** | −0.408 ** | 0.413 ** | 0.408 ** | |
| Loss of loved ones | −0.056 | −0.150 ** | −0.003 | −0.113 ** | 0.199 ** | 0.122 ** | |
| Health problems of close people | −0.159 ** | −0.236 ** | −0.168 ** | −0.263 ** | 0.293 ** | 0.246 ** | |
| Family situation | −0.204 ** | −0.249 ** | −0.222 ** | −0.341 ** | 0.385 ** | 0.337 ** | |
| TOTAL | −0.303 ** | −0.388 ** | −0.309 ** | −0.451 ** | 0.516 ** | 0.481 ** | |
| Mindfulness | MAASA wave1 | - | |||||
| MAASA wave3 | 0.559 ** | - | |||||
| CAMM wave1 | 0.682 ** | 0.561 ** | - | ||||
| CAMM wave3 | 0.461 ** | 0.630 ** | 0.582 ** | - | |||
| PHQ-9 depression wave2 | −0.544 ** | −0.547 ** | −0.531 ** | −0.560 ** | - | ||
| PHQ-9 depression wave4 | −0.388 ** | −0.531 ** | −0.457 ** | −0.537 ** | 0.663 ** | - |
| χ2 | df | p | TLI | CFI | RMSEA | 90% CI | M → SLEs | M → Dep Direct | M → Dep Indirect | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 → SLE1 | M3 → SLE3 | M1 → Dep2 | M3 → Dep4 | M1 → Dep2 | M3 → Dep4 | ||||||||
| SLEtot | 713.997 | 69 | <0.001 | 0.930 | 0.954 | 0.049 | 0.046–0.052 | −0.259 *** | −0.215 *** | −0.635 *** | −0.621 *** | −0.169 *** | −0.122 *** |
| SLEhealth | 736.994 | 69 | <0.001 | 0.927 | 0.952 | 0.050 | 0.047–0.053 | −0.223 *** | −0.182 *** | −0.625 *** | −0.598 *** | −0.175 *** | −0.124 *** |
| SLEabuse | 552.503 | 69 | <0.001 | 0.939 | 0.960 | 0.042 | 0.039–0.046 | −0.177 *** | −0.168 *** | −0.701 *** | −0.657 *** | −0.075 *** | −0.062 *** |
| SLEschool | 272.490 | 69 | <0.001 | 0.972 | 0.982 | 0.028 | 0.024–0.031 | −0.278 *** | −0.205 *** | −0.705 *** | −0.679 *** | −0.041 *** | −0.030 *** |
| SLErelations | 471.399 | 69 | <0.001 | 0.952 | 0.969 | 0.039 | 0.035–0.042 | −0.252 *** | −0.231 *** | −0.687 *** | −0.656 *** | −0.037 *** | −0.030 *** |
| SLEloss | 171.525 | 69 | <0.001 | 0.988 | 0.992 | 0.020 | 0.016–0.023 | −0.124 *** | −0.107 *** | −0.739 *** | −0.702 *** | −0.022 | −0.018 |
| SLEhealth-close | 375.590 | 69 | <0.001 | 0.965 | 0.977 | 0.034 | 0.030–0.037 | −0.131 *** | −0.098 *** | −0.734 *** | −0.690 *** | −0.008 | −0.009 |
| SLEfamily | 480.769 | 69 | <0.001 | 0.953 | 0.969 | 0.039 | 0.036–0.042 | −0.140 *** | −0.126 *** | −0.708 *** | −0.672 *** | −0.019 *** | −0.016 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ćavar Mišković, F.; Milas, G. Mindfulness Reduces Adolescent Depression Through Stress Appraisal and Cognitive Reactivity: Evidence from a Four-Wave Longitudinal Study. Medicina 2025, 61, 1154. https://doi.org/10.3390/medicina61071154
Ćavar Mišković F, Milas G. Mindfulness Reduces Adolescent Depression Through Stress Appraisal and Cognitive Reactivity: Evidence from a Four-Wave Longitudinal Study. Medicina. 2025; 61(7):1154. https://doi.org/10.3390/medicina61071154
Chicago/Turabian StyleĆavar Mišković, Filipa, and Goran Milas. 2025. "Mindfulness Reduces Adolescent Depression Through Stress Appraisal and Cognitive Reactivity: Evidence from a Four-Wave Longitudinal Study" Medicina 61, no. 7: 1154. https://doi.org/10.3390/medicina61071154
APA StyleĆavar Mišković, F., & Milas, G. (2025). Mindfulness Reduces Adolescent Depression Through Stress Appraisal and Cognitive Reactivity: Evidence from a Four-Wave Longitudinal Study. Medicina, 61(7), 1154. https://doi.org/10.3390/medicina61071154