
Development of the GDF-TRACK-AKI Score for Predicting Acute Kidney Injury in Patients with Rhabdomyolysis Due to Excessive Exercise or Trauma

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
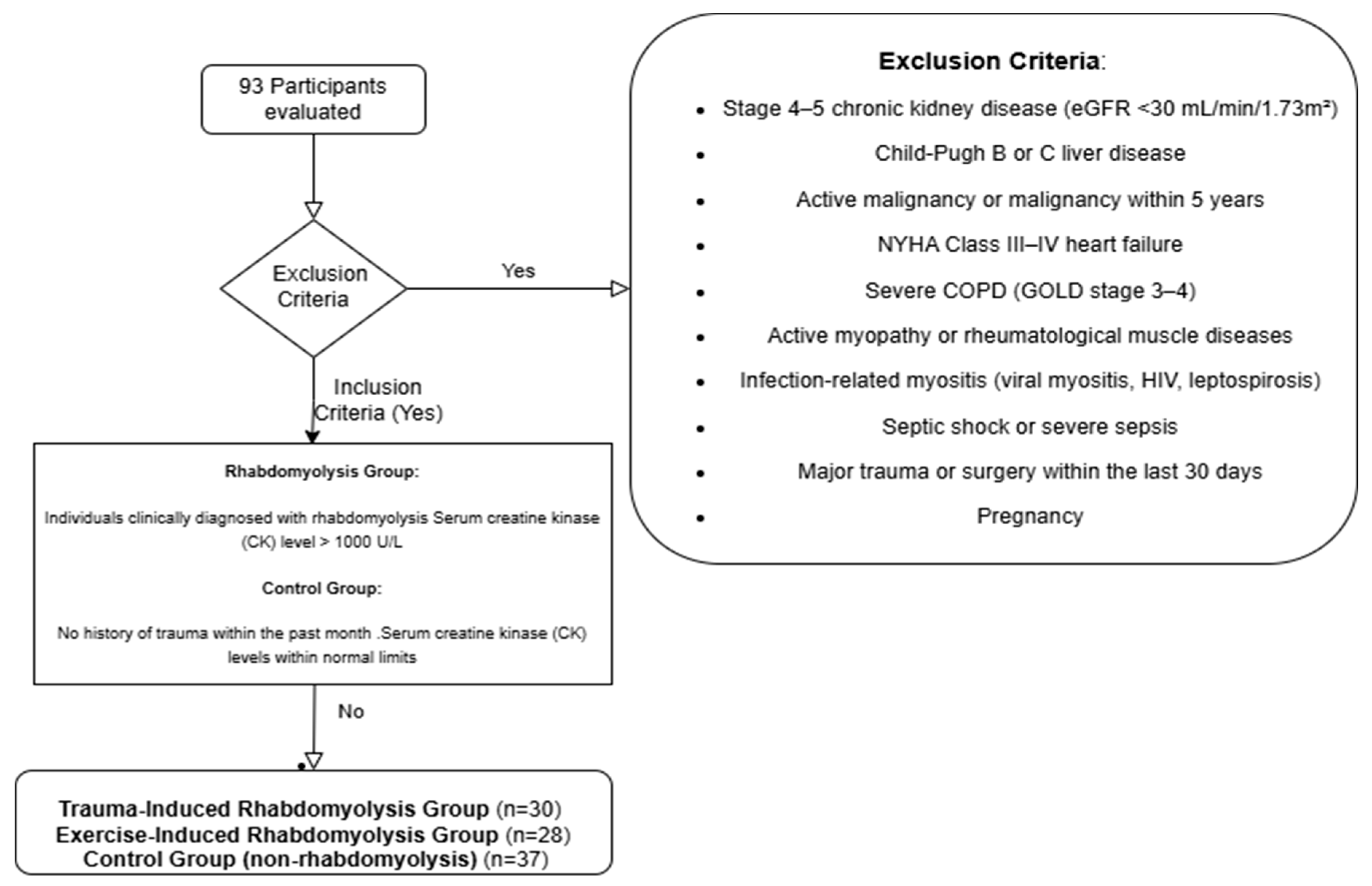
2.2. Study Population and Participant Selection
2.3. Sample Size Calculation
2.4. Data Collection
2.5. Clinical Definitions
2.6. Development of the GDF-TRACK-AKI Score
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AKI | Acute Kidney Injury |
| ALT | Alanine Aminotransferase |
| ANOVA | Analysis of Variance |
| AST | Aspartate Aminotransferase |
| ATP | Adenosine Triphosphate |
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| CK | Creatine Kinase |
| COPD | Chronic Obstructive Pulmonary Disease |
| CPK | Creatine Phosphokinase |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| GDF-15 | Growth Differentiation Factor-15 |
| GDF-TRACK-AKI | Growth Differentiation Factor-15, Trauma, Creatine Kinase Acute Kidney Injury Score |
| GFR | Glomerular Filtration Rate |
| GGT | Gamma-Glutamyl Transferase |
| GOLD | Global Initiative for Chronic Obstructive Lung Disease |
| HIV | Human Immunodeficiency Virus |
| KDIGO | Kidney Disease Improving Global Outcomes |
| LDH | Lactate Dehydrogenase |
| NPV | Negative Predictive Value |
| NYHA | New York Heart Association |
| OR | Odds Ratio |
| PPV | Positive Predictive Value |
| ROC | Receiver Operating Characteristic |
| RRT | Renal Replacement Therapy |
| SD | Standard Deviation |
| SPSS | Statistical Package for the Social Sciences |
| WBC | White Blood Cell |
References
- Baeza-Trinidad, R. Rhabdomyolysis: A syndrome to be considered. Med. Clin. 2022, 158, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Bosch, X.; Poch, E.; Grau, J.M. Rhabdomyolysis and acute kidney injury. N. Engl. J. Med. 2009, 361, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Dall’Aglio, A.; Kissling, S.; Vollenweider, P.; Jaccard, E. Rhabdomyolysis: Early management. Rev. Med. Suisse 2020, 16, 2272–2278. [Google Scholar] [PubMed]
- Harmelink, M. Uncommon Causes of Rhabdomyolysis. Crit. Care Clin. 2022, 38, 271–285. [Google Scholar] [CrossRef]
- Lubbe, C.; Meyer, L.C.R.; Kohn, T.A.; Harvey, B.H.; Wolmarans, D.W. The pathophysiology of rhabdomyolysis in ungulates and rats: Towards the development of a rodent model of capture myopathy. Vet. Res. Commun. 2023, 47, 361–371. [Google Scholar] [CrossRef]
- Petejova, N.; Martinek, A. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: A critical review. Crit. Care 2014, 18, 224. [Google Scholar] [CrossRef]
- Ahmad, S.; Anees, M.; Elahi, I.; Fazal, E.M. Rhabdomyolysis Leading to Acute Kidney Injury. J. Coll. Physicians Surg. Pak. 2021, 31, 235–237. [Google Scholar]
- Zhu, D.C.; Li, W.Y.; Zhang, J.W.; Tong, J.S.; Xie, W.Y.; Qin, X.L.; Zhang, X. Rhabdomyolysis-associated acute kidney injury: Clinical characteristics and intensive care unit transfer analysis. Intern. Med. J. 2022, 52, 1251–1257. [Google Scholar] [CrossRef]
- Torr, L.; Mortimore, G. The management and diagnosis of rhabdomyolysis-induced acute kidney injury: A case study. Br. J. Nurs. 2022, 31, 844–852. [Google Scholar] [CrossRef]
- Cabral, B.M.I.; Edding, S.N.; Portocarrero, J.P.; Lerma, E.V. Rhabdomyolysis. Dis. Mon. 2020, 66, 101015. [Google Scholar] [CrossRef]
- Gupta, A.; Thorson, P.; Penmatsa, K.R.; Gupta, P. Rhabdomyolysis: Revisited. Ulster Med. J. 2021, 90, 61–69. [Google Scholar] [PubMed]
- Fredrickson, K.A.; Carver, T.W. Trauma-related electrolyte disturbances: From resuscitation to rhabdomyolysis. Nutr. Clin. Pract. 2022, 37, 1004–1014. [Google Scholar] [CrossRef]
- Reinertson, R. Suspension trauma and rhabdomyolysis. Wilderness Environ. Med. 2011, 22, 286–287. [Google Scholar] [CrossRef]
- Long, B.; Liang, S.Y.; Gottlieb, M. Crush injury and syndrome: A review for emergency clinicians. Am. J. Emerg. Med. 2023, 69, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Stahl, K.; Rastelli, E.; Schoser, B. A systematic review on the definition of rhabdomyolysis. J. Neurol. 2020, 267, 877–882. [Google Scholar] [CrossRef]
- Hadzalic, H.; Herzog, A.; Keller, D.I. Elevated Creatine Kinase as a Diagnostic Parameter of Rhabdomyolysis. Praxis 2021, 110, 2–8. [Google Scholar] [CrossRef]
- Marson, J.W.; Baldwin, H.E. The creatine kinase conundrum: A reappraisal of the association of isotretinoin, creatine kinase, and rhabdomyolysis. Int. J. Dermatol. 2020, 59, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, J.L.; Shen, M.C. Rhabdomyolysis. Chest 2013, 144, 1058–1065. [Google Scholar] [CrossRef]
- Sawasawa, T.; Lin, J.D.; Wang, Y.H.; Chen, K.J.; Yang, Y.M.; Hu, S.W.; Cheng, C.W. Elevated serum GDF15 level as an early indicator of proximal tubular cell injury in acute kidney injury. Life Sci. 2024, 357, 123093. [Google Scholar] [CrossRef]
- Valiño-Rivas, L.; Cuarental, L.; Ceballos, M.I.; Pintor-Chocano, A.; Perez-Gomez, M.V.; Sanz, A.B.; Ortiz, A.; Sanchez-Niño, M.D. Growth differentiation factor-15 preserves Klotho expression in acute kidney injury and kidney fibrosis. Kidney Int. 2022, 101, 1200–1215. [Google Scholar] [CrossRef]
- Lasaad, S.; Crambert, G. GDF15, an Emerging Player in Renal Physiology and Pathophysiology. Int. J. Mol. Sci. 2024, 25, 5956. [Google Scholar] [CrossRef]
- Perez-Gomez, M.V.; Pizarro-Sanchez, S.; Gracia-Iguacel, C.; Cano, S.; Cannata-Ortiz, P.; Sanchez-Rodriguez, J.; Sanz, A.B.; Sanchez-Niño, M.D.; Ortiz, A. Urinary Growth Differentiation Factor-15 (GDF15) levels as a biomarker of adverse outcomes and biopsy findings in chronic kidney disease. J. Nephrol. 2021, 34, 1819–1832. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Kumar, S.; Heinzel, A.; Gao, M.; Guo, J.; Alvarado, G.F.; Reindl-Schwaighofer, R.; Krautzberger, A.M.; Cippà, P.E.; McMahon, J.; et al. Renoprotective and Immunomodulatory Effects of GDF15 following AKI Invoked by Ischemia-Reperfusion Injury. J. Am. Soc. Nephrol. 2020, 31, 701–715. [Google Scholar] [CrossRef] [PubMed]
- Durand, F.; Valla, D. Assessment of the prognosis of cirrhosis: Child-Pugh versus MELD. J. Hepatol. 2005, 42 (Suppl. S1), S100–S107. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421, Erratum in J. Am. Coll. Cardiol. 2023, 81, 1551. [Google Scholar]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; Montes de Oca, M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur. Respir. J. 2023, 61, 2300239. [Google Scholar] [CrossRef]
- McMahon, G.M.; Zeng, X.; Waikar, S.S. A risk prediction score for kidney failure or mortality in rhabdomyolysis. JAMA Intern. Med. 2013, 173, 1821–1827. [Google Scholar] [CrossRef]
- Huerta-Alardín, A.L.; Varon, J.; Marik, P.E. Bench-to-bedside review: Rhabdomyolysis—An overview for clinicians. Crit. Care. 2004, 9, 158. [Google Scholar] [CrossRef]
- Kaya, B.; Balal, M.; Seyrek, N.; Mete, B.; Karayaylali, I. Hemodialysis Experience After Kahramanmaraş Earthquake. J. Clin. Med. 2024, 13, 6610. [Google Scholar] [CrossRef]
- Khan, F.Y. Rhabdomyolysis: A review of the literature. Neth. J. Med. 2009, 67, 272–283. [Google Scholar]
- Seo, J.S.; Yeo, I.; Kim, C.; Kim, D.; Lim, J.H.; Park, K.; Jeong, J.; Kwon, H.; Cho, Y.; Park, S. Factors Associated with Acute Kidney Injury Occurrence and Prognosis in Rhabdomyolysis at the Emergency Department. Medicina 2024, 60, 105. [Google Scholar] [CrossRef]
- Chandel, A.; Brusher, K.; Hall, V.; Howard, R.S.; Clark, P.A. Diagnosis and Management of Rhabdomyolysis in the Absence of Creatine Phosphokinase: A Medical Record Review. Mil. Med. 2019, 184, 820–825. [Google Scholar] [CrossRef]
- Luo, Y.; Liu, C.; Li, D.; Yang, B.; Shi, J.; Guo, X.; Fan, H.; Lv, Q. Progress in the Diagnostic and Predictive Evaluation of Crush Syndrome. Diagnostics 2023, 13, 3034. [Google Scholar] [CrossRef]
- Siddiqui, J.A.; Pothuraju, R.; Khan, P.; Sharma, G.; Muniyan, S.; Seshacharyulu, P.; Jain, M.; Nasser, M.W.; Batra, S.K. Pathophysiological role of growth differentiation factor 15 (GDF15) in obesity, cancer, and cachexia. Cytokine Growth Factor Rev. 2022, 64, 71–83. [Google Scholar] [CrossRef]
- Johann, K.; Kleinert, M.; Klaus, S. The Role of GDF15 as a Myomitokine. Cells 2021, 10, 2990. [Google Scholar] [CrossRef]
- Duvvuri, B.; Gonzalez-Chapa, J.A.; Pachman, L.M.; Morgan, G.A.; Naik, N.; Shenoi, S.; Lood, C. The emerging role of growth differentiation factor 15 as a potential disease biomarker in juvenile dermatomyositis. Rheumatology 2025, 64, 805–809. [Google Scholar] [CrossRef]
- Kümpers, P.; Lukasz, A.; David, S.; Horn, R.; Hafer, C.; Faulhaber-Walter, R.; Fliser, D.; Haller, H.; Kielstein, J.T. Excess Circulating Angiopoietin-2 Is a Strong Predictor of Mortality in Critically Ill Medical Patients. Crit. Care 2008, 12, R147. [Google Scholar] [CrossRef]
- Parikh, S.M.; Mammoto, T.; Schultz, A.; Yuan, H.T.; Christiani, D.; Karumanchi, S.A.; Sukhatme, V.P. Excess Circulating Angiopoietin-2 May Contribute to Pulmonary Vascular Leak in Sepsis in Humans. PLoS Med. 2006, 3, e46. [Google Scholar] [CrossRef]
- Huang, W.; Tang, Y.; Li, L.; Du, Y.; Zhang, S.; Lv, Y.; Dong, L.; Liu, H. Angiopoietin-2 Is Associated with Severity of Disease and Mortality in Patients with Acute Pancreatitis. Pancreas 2016, 45, 556–560. [Google Scholar]
- Ong, S.G.; Hausenloy, D.J. Hypoxia-Inducible Factor as a Therapeutic Target for Cardioprotection. Pharmacol. Ther. 2012, 136, 69–81. [Google Scholar] [CrossRef]
- Zhang, Z.; Lu, B.; Sheng, X.; Jin, N.; Chen, Y.; Yuan, Y. Diagnostic Value of Plasma NGAL for Early Prediction of Acute Kidney Injury in Critically Ill Patients: A Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 452. [Google Scholar]
- Sabbisetti, V.S.; Waikar, S.S.; Antoine, D.J.; Smiles, A.; Wang, C.; Ravisankar, A.; Ito, K.; Sharma, S.; Ramadesikan, S.; Lee, M. Blood Kidney Injury Molecule-1 (KIM-1) as a Biomarker of Acute and Chronic Kidney Injury in Humans. J. Am. Soc. Nephrol. 2014, 25, 2177–2186. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Koyfman, A.; Gottlieb, M. An evidence-based narrative review of the emergency department evaluation and management of rhabdomyolysis. Am. J. Emerg. Med. 2019, 37, 518–523. [Google Scholar] [CrossRef]
- Fernandes, P.F.C.B.C.; Paiva, J.H.H.G.L. Motor Vehicle Injury and Kidney Damage: Trauma, Rhabdomyolysis, Acute Kidney Injury and Beyond. In Nephrology and Public Health Worldwide; Karger Publisher: Basel, Switzerland, 2021; p. 122. [Google Scholar]

{kind=link}
{kind=link}
| Parameter | 1 Point | 2 Points | 3 Points |
|---|---|---|---|
| Bilirubin (mg/dL) | <2 | 2–3 | >3 |
| Albumin (g/dL) | >3.5 | 2.8–3.5 | <2.8 |
| INR | <1.7 | 1.7–2.3 | >2.3 |
| Ascites | None | Mild | Moderate to Severe |
| Hepatic Encephalopathy | None | Grade I–II | Grade III–IV |
| Class | Description |
|---|---|
| I | No limitation of physical activity. Ordinary activities do not cause symptoms. |
| II | Slight limitation of physical activity. Ordinary activity results in symptoms. |
| III | Marked limitation. Symptoms occur with less than ordinary activity. |
| IV | Symptoms are present even at rest. Any physical activity leads to discomfort. |
| Stage | FEV₁ (% Predicted) | Description |
|---|---|---|
| GOLD 1 | ≥80% | Mild COPD |
| GOLD 2 | 50–79% | Moderate COPD |
| GOLD 3 | 30–49% | Severe COPD |
| GOLD 4 | <30% | Very Severe COPD |
| Variable | Category | Group | p | |||||
|---|---|---|---|---|---|---|---|---|
| Rhabdomyolysis After Trauma | Control | Rhabdomyolysis After Excessive Exercise | ||||||
| n | % | n | % | n | % | |||
| Sex | Female | 12 | 40.00 | 19 | 51.35 | 6 | 21.43 | 0.046 * |
| Male | 18 | 60.00 | 18 | 48.65 | 22 | 78.57 | ||
| Renal Replacement Therapy | Absent | 5 | 16.67 | 37 | 100.00 | 28 | 100.00 | 0.001 * |
| Present | 25 | 83.33 | 0 | 0.00 | 0 | 0.00 | ||
| Mortality | Absent | 29 | 96.67 | 37 | 100.00 | 28 | 100.00 | 0.335 |
| Present | 1 | 3.33 | 0 | 0.00 | 0 | 0.00 | ||
| Acute Kidney Injury | Absent | 5 | 16.67 | 37 | 100.00 | 26 | 92.86 | 0.001 * |
| Present | 25 | 83.33 | 0 | 0.00 | 2 | 7.14 | ||
| Variable | Median ± IQR | Min.- Maks. | Median ± IQR | Min. -Maks. | Median ± IQR | Min.- Maks. | p | |
| Age | 33.00 ± 14.25 | 18 85 | 75.00 ± 19.00 | 22 87 | 22.50 ± 14.25 | 18 65 | 0.001 * | |
| GDF-15 Level (pg/mL) | 5741.50 ± 2830.50 | 2200 7494 | 2378.00 ± 1314.00 | 1211 4722 | 2958.50 ± 1386.00 | 1467 5056 | 0.001 * | |
| Variable | Correlation Coefficient (r) | p-Value |
|---|---|---|
| Creatine Kinase (U/L) | 0.517 | 0.001 * |
| Creatinine (mg/dL) | 0.517 | 0.001 * |
| Urea (mg/dL) | 0.649 | 0.001 * |
| Glomerular Filtration Rate (mL/min/1.73 m2) | −0.568 | 0.001 * |
| Uric Acid (mg/dL) | −0.026 | 0.799 |
| Aspartate Aminotransferase (U/L) | −0.01 | 0.927 |
| Alanine Aminotransferase (U/L) | 0.082 | 0.43 |
| Alkaline Phosphatase (U/L) | 0.281 | 0.006 * |
| Gamma-Glutamyl Transferase (U/L) | 0.057 | 0.582 |
| Lactate Dehydrogenase (U/L) | 0.175 | 0.09 |
| Total Bilirubin (mg/dL) | 0.27 | 0.008 * |
| Direct Bilirubin (mg/dL) | −0.043 | 0.682 |
| Sodium (mmol/L) | −0.409 | 0.001 * |
| Potassium (mmol/L) | 0.228 | 0.026 * |
| Calcium (mg/dL) | 0.207 | 0.044 |
| Hemoglobin (g/dL) | 0.008 | 0.804 |
| Platelet (×103/µL) | −0.025 | 0.81 |
| White Blood Cell Count (×103/µL) | 0.597 | 0.001 * |
| Category | Subgroup | GDF-15 Median | IQR | Test Value (t) | p-Value |
|---|---|---|---|---|---|
| Sex | Female | 3267.00 | 2222.00 | −0.530 | 0.596 |
| Male | 2991.50 | 2471.00 | |||
| Renal Replacement Therapy | Absent | 2639.00 | 1276.75 | −6.233 | 0.001 * |
| Present | 5794.00 | 2125.50 | |||
| Acute Kidney Disease | Absent | 2608.50 | 1251.75 | −6.514 | 0.001 * |
| Present | 5756.00 | 2006.00 | |||
| Rhabdomyolysis Etiology | Trauma | 5741.50 | 2830.50 | −4.808 | 0.001 * |
| Excessive exercise | 2958.50 | 1386.00 | |||
| Group Comparison (Rhabdomyolysis vs. Control) | Rhabdomyolysis | 3580.50 | 3108.50 | −4.759 | 0.001 * |
| Control | 2378.00 | 1314.00 |
| Variable | Acute Kidney Injury | Mann–Whitney U Test | ||||
|---|---|---|---|---|---|---|
| Absent | Present | |||||
| Median | IQR | Median | IQR | z | p | |
| GDF-TRACK-AKI score | 0.00 | 0.00 | 3.00 | 2.00 | −8.079 | 0.001 * |
| Creatine Kinase (U/L) | 174.00 | 13,966.75 | 33,976.00 | 79,574.00 | −5.875 | 0.001 * |
| Creatinine (mg/dL) | 0.84 | 0.25 | 5.29 | 2.92 | −7.576 | 0.001 * |
| Urea (mg/dL) | 28.00 | 15.75 | 92.00 | 65.00 | −5.434 | 0.001 * |
| Glomerular Filtration Rate (mL/min/1.73 m2) | 101.50 | 38.75 | 20.00 | 43.00 | −5.496 | 0.001 * |
| Uric Acid (mg/dL) | 4.70 | 1.98 | 5.50 | 3.40 | −1.250 | 0.211 |
| Aspartate Aminotransferase (U/L) | 39.00 | 9.00 | 24.00 | 8.00 | −6.296 | 0.001 * |
| Alanine Aminotransferase (U/L) | 39.00 | 93.00 | 68.00 | 60.00 | −2.009 | 0.044 * |
| Alkaline Phosphatase (U/L) | 36.50 | 76.75 | 67.00 | 64.00 | −1.787 | 0.074 |
| Gamma-Glutamyl Transferase (U/L) | 26.00 | 40.00 | 48.00 | 59.00 | −1.585 | 0.113 |
| Lactate Dehydrogenase (U/L) | 260.50 | 197.00 | 480.00 | 326.00 | −2.695 | 0.007 * |
| Total Bilirubin (mg/dL) | 0.50 | 0.38 | 0.60 | 0.90 | −4.464 | 0.001 * |
| Direct Bilirubin (mg/dL) | 0.20 | 0.20 | 0.20 | 0.40 | −0.896 | 0.370 |
| Sodium (mmol/L) | 139.00 | 3.75 | 135.00 | 9.00 | −1.770 | 0.077 |
| Potassium (mmol/L) | 4.25 | 0.050 | 59.382 | 0.90 | −3.445 | 0.001 * |
| Calcium (mg/dL) | 9.00 | 0.70 | 8.50 | 0.50 | −0.116 | 0.908 |
| Hemoglobin (g/dL) | 12.65 | 3.67 | 8.80 | 1.70 | −3.854 | 0.001 * |
| Platelet (×103/µL) | 266.50 | 151.25 | 249.00 | 195.00 | −4.869 | 0.001 * |
| White Blood Cell Count (×103/µL) | 8.13 | 3.80 | 13.77 | 5.56 | −0.153 | 0.879 |
| Variable | Acute Kidney Injury | Mann–Whitney U Test | ||||
|---|---|---|---|---|---|---|
| Absent | Present | |||||
| Median | IQR | Median | IQR | t | p | |
| GDF Track AKI score | 0.00 | 0.00 | 3.00 | 2.00 | −8.079 | 0.001 * |
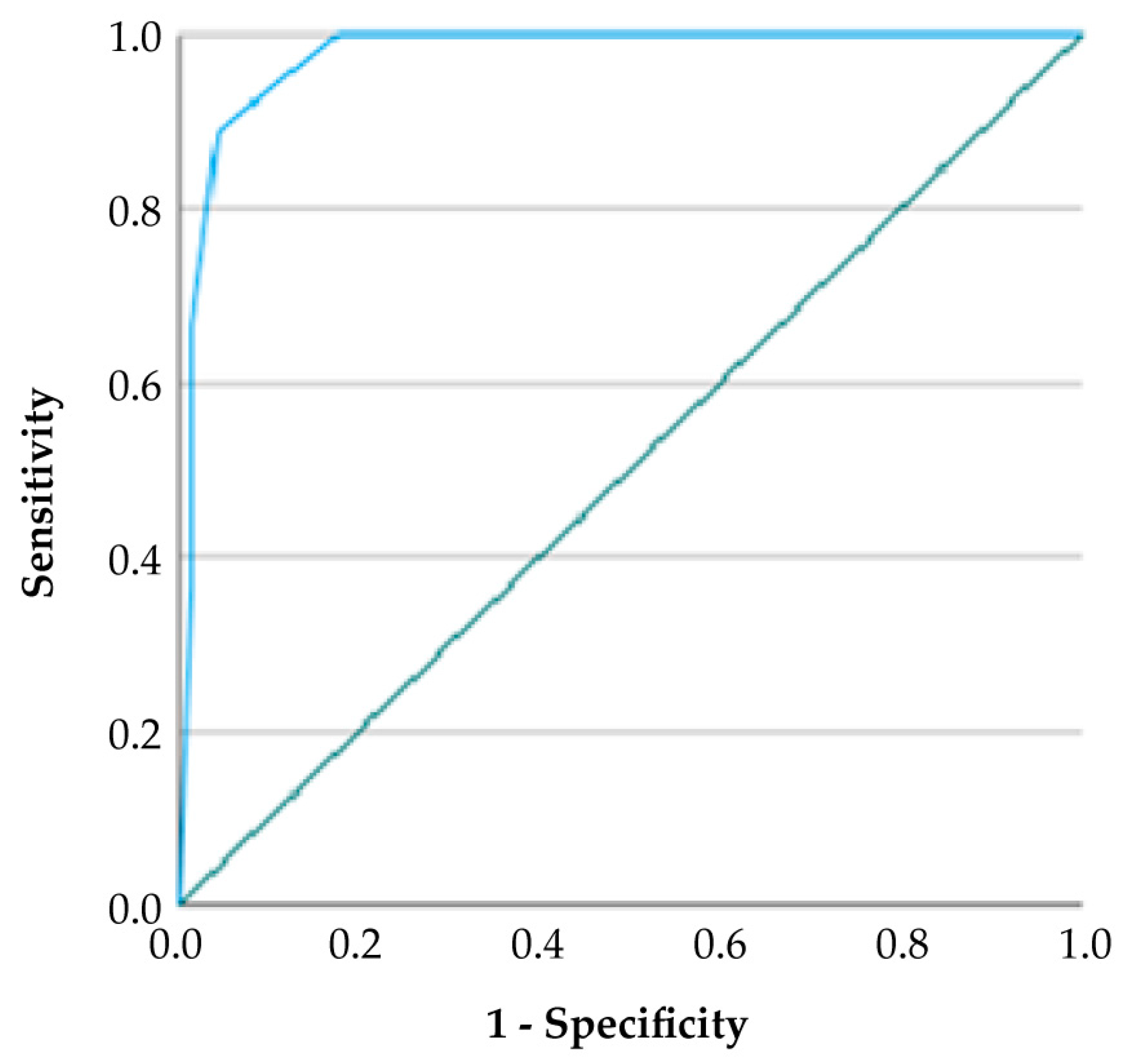
| Variable | Cut-off Value | AUC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Youden Index |
|---|---|---|---|---|---|---|---|
| Acute Kidney Injury | 2.5 | 0.918 (0.857–0.979) | 67.0% | 98.0% | 94.4% | 81.4% | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zengin, O.; Göre, B.; Yakut, M.; Yaylalı, M.; Göv, M.; Dönmez, S.; Çelik, G.K.; Günaydın, G.P.; Uzdoğan, E.A.; Asfuroğlu Kalkan, E.; et al. Development of the GDF-TRACK-AKI Score for Predicting Acute Kidney Injury in Patients with Rhabdomyolysis Due to Excessive Exercise or Trauma. Medicina 2025, 61, 1116. https://doi.org/10.3390/medicina61071116
Zengin O, Göre B, Yakut M, Yaylalı M, Göv M, Dönmez S, Çelik GK, Günaydın GP, Uzdoğan EA, Asfuroğlu Kalkan E, et al. Development of the GDF-TRACK-AKI Score for Predicting Acute Kidney Injury in Patients with Rhabdomyolysis Due to Excessive Exercise or Trauma. Medicina. 2025; 61(7):1116. https://doi.org/10.3390/medicina61071116
Chicago/Turabian StyleZengin, Oğuzhan, Burak Göre, Melike Yakut, Mustafa Yaylalı, Muhammet Göv, Safa Dönmez, Gülhan Kurtoğlu Çelik, Gül Pamukçu Günaydın, Esma Andaç Uzdoğan, Emra Asfuroğlu Kalkan, and et al. 2025. "Development of the GDF-TRACK-AKI Score for Predicting Acute Kidney Injury in Patients with Rhabdomyolysis Due to Excessive Exercise or Trauma" Medicina 61, no. 7: 1116. https://doi.org/10.3390/medicina61071116
APA StyleZengin, O., Göre, B., Yakut, M., Yaylalı, M., Göv, M., Dönmez, S., Çelik, G. K., Günaydın, G. P., Uzdoğan, E. A., Asfuroğlu Kalkan, E., & Ateş, İ. (2025). Development of the GDF-TRACK-AKI Score for Predicting Acute Kidney Injury in Patients with Rhabdomyolysis Due to Excessive Exercise or Trauma. Medicina, 61(7), 1116. https://doi.org/10.3390/medicina61071116