

Association Between Cardiometabolic Index and Mortality Among Patients with Atherosclerotic Cardiovascular Disease: Evidence from NHANES 1999–2018

Abstract
1. Introduction
2. Materials and Methods
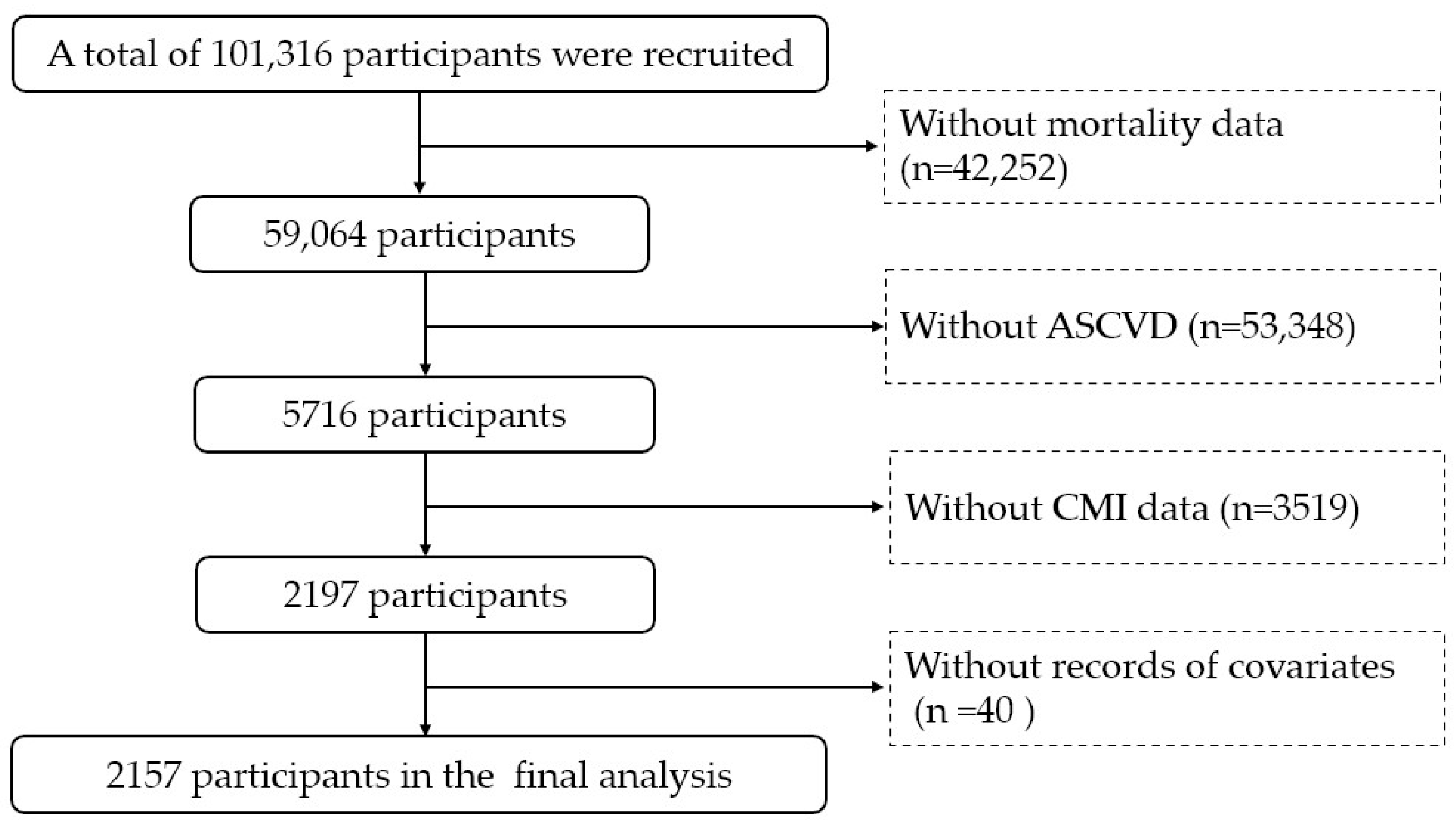
2.1. Study Design and Population
2.2. Assessment of CMI
2.3. Assessment of Mortality
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
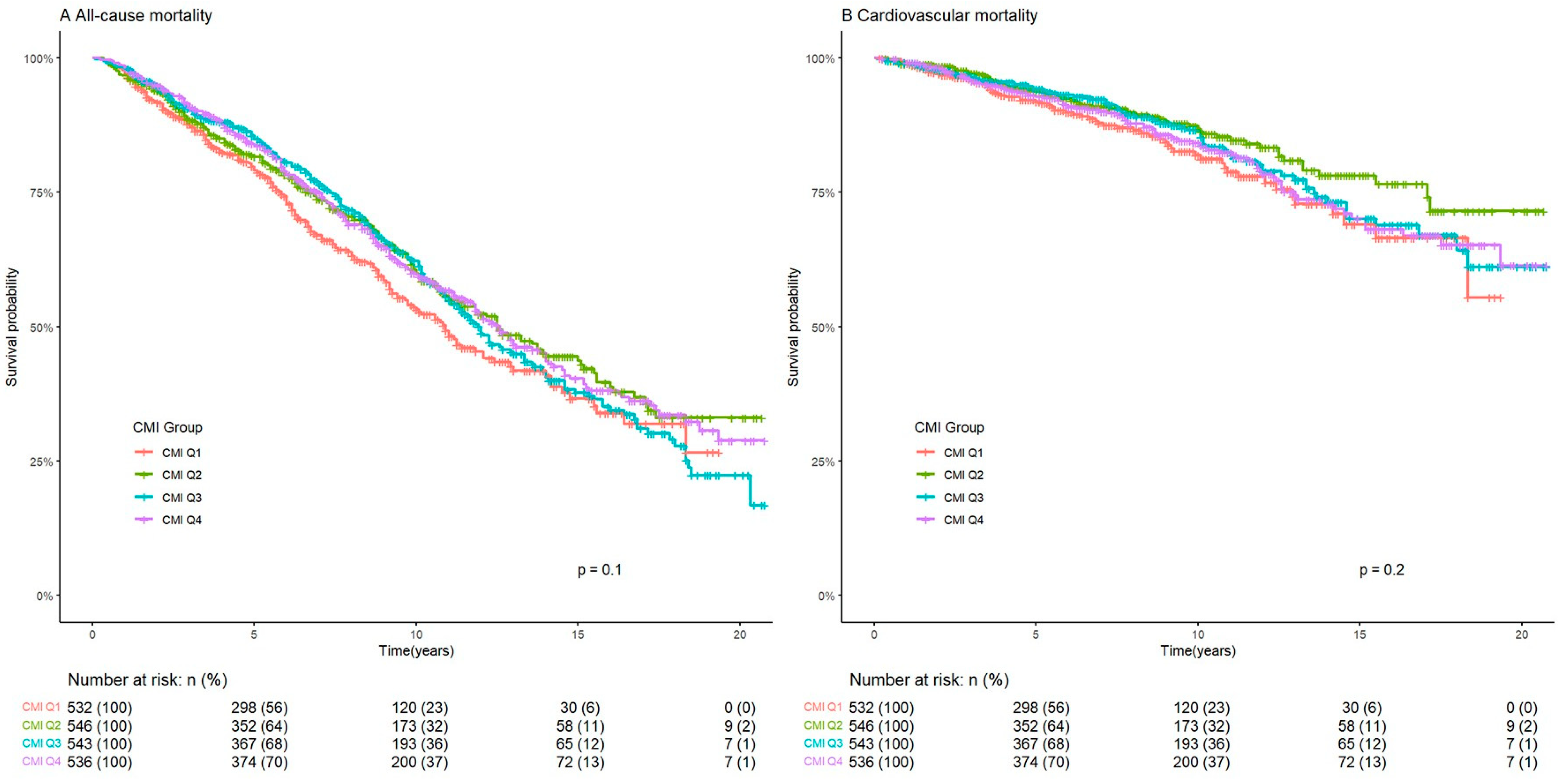
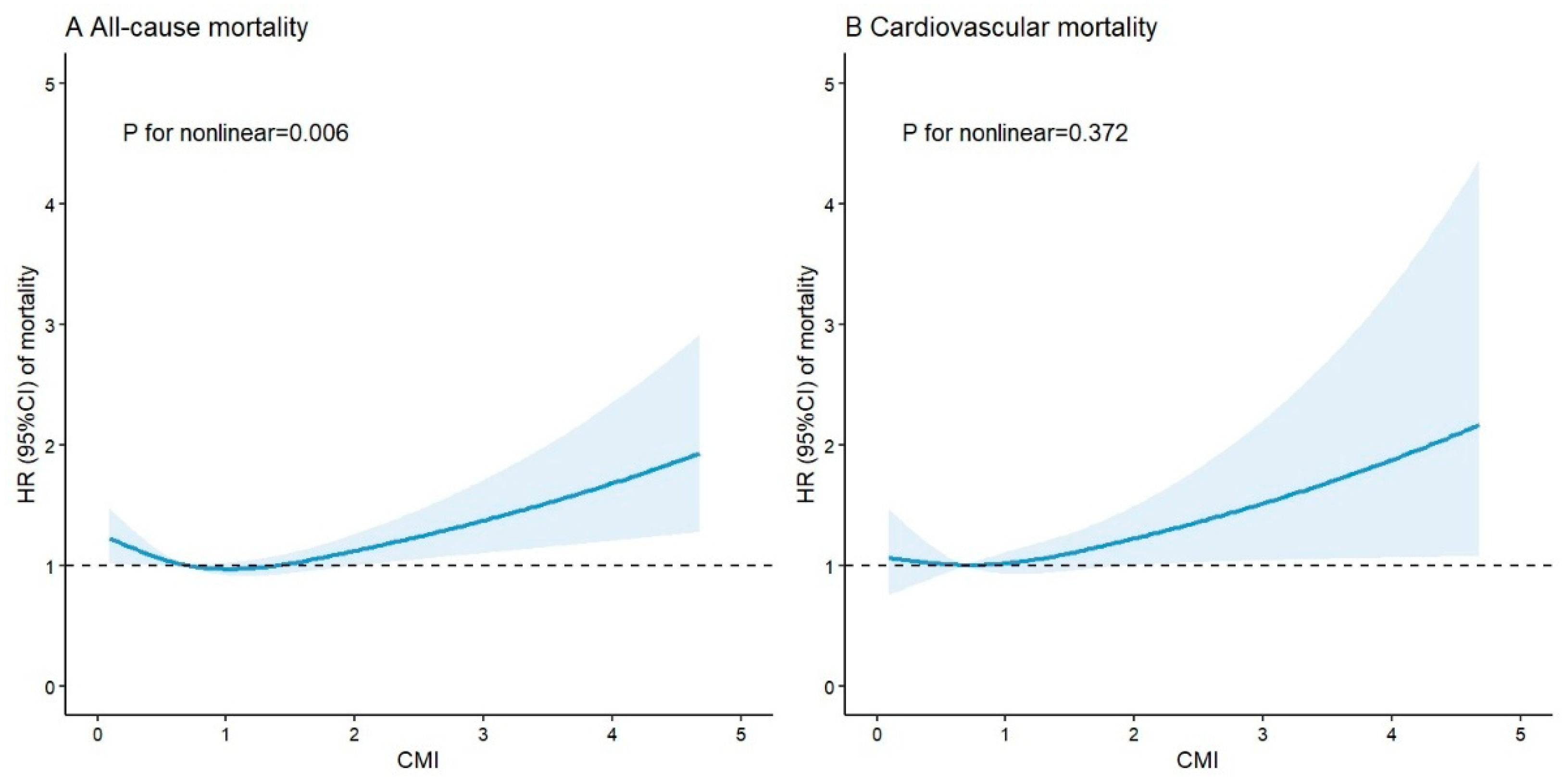
3.2. Association Between CMI and Mortality
3.3. Subgroup Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASCVD | atherosclerotic cardiovascular disease |
| CMI | cardiometabolic index |
| NHANES | National Health and Nutrition Examination Survey |
| MetS | metabolic syndrome |
| WHtR | waist-to-height ratio |
| TG | triglycerides |
| HDL-C | high-density lipoprotein cholesterol |
| NCHS | National Center for Health Statistics |
| CDC | Centers for Disease Control and Prevention |
| WC | waist circumference |
| ICD | International Classification of Diseases |
| PIR | poverty income ratio |
| BMI | body mass index |
| TC | total cholesterol |
| MVPA | moderate-to-vigorous physical activity |
| SD | standard deviation |
| IQR | interquartile range |
| ANOVA | one-way analysis of variance |
| HR | hazard ratio |
| CI | confidence interval |
| MESA | Multi-Ethnic Study of Atherosclerosis |
References
- Mensah, G.A.; Fuster, V.; Murray, C.J.L.; Roth, G.A. Global Burden of Cardiovascular Diseases and Risks, 1990–2022. J. Am. Coll. Cardiol. 2023, 82, 2350–2473. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, I.; Daimon, T. The “cardiometabolic index” as a new marker determined by adiposity and blood lipids for discrimination of diabetes mellitus. Clin. Chim. Acta 2015, 438, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, Y.; Sun, G.; Jia, P.; Qian, H.; Sun, Y. Validity of cardiometabolic index, lipid accumulation product, and body adiposity index in predicting the risk of hypertension in Chinese population. Postgrad. Med. 2018, 130, 325–333. [Google Scholar] [CrossRef]
- Zha, F.; Cao, C.; Hong, M.; Hou, H.; Zhang, Q.; Tang, B.; Hu, H.; Han, Y.; Zan, Y.; Wang, Y.; et al. The nonlinear correlation between the cardiometabolic index and the risk of diabetes: A retrospective Japanese cohort study. Front. Endocrinol. 2023, 14, 1120277. [Google Scholar] [CrossRef]
- Tamini, S.; Bondesan, A.; Caroli, D.; Sartorio, A. The Lipid Accumulation Product Index (LAP) and the Cardiometabolic Index (CMI) Are Useful for Predicting the Presence and Severity of Metabolic Syndrome in Adult Patients with Obesity. J. Clin. Med. 2024, 13, 2843. [Google Scholar] [CrossRef]
- Lazzer, S.; D’Alleva, M.; Isola, M.; De Martino, M.; Caroli, D.; Bondesan, A.; Marra, A.; Sartorio, A. Cardiometabolic Index (CMI) and Visceral Adiposity Index (VAI) Highlight a Higher Risk of Metabolic Syndrome in Women with Severe Obesity. J. Clin. Med. 2023, 12, 3055. [Google Scholar] [CrossRef]
- Li, F.E.; Luo, Y.; Zhang, F.L.; Zhang, P.; Liu, D.; Ta, S.; Yu, Y.; Guo, Z.-N.; Yang, Y. Association Between Cardiometabolic Index and Stroke: A Population- based Cross-sectional Study. Curr. Neurovasc. Res. 2021, 18, 324–332. [Google Scholar] [CrossRef]
- Xu, B.; Wu, Q.; La, R.; Lu, L.; Abdu, F.A.; Yin, G.; Zhang, W.; Ding, W.; Ling, Y.; He, Z.; et al. Is systemic inflammation a missing link between cardiometabolic index with mortality? Evidence from a large population-based study. Cardiovasc. Diabetol. 2024, 23, 212. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wu, Q.; Yan, G.; Duan, J.; Chen, Z.; Yang, P.; Bragazzi, N.L.; Lu, Y.; Yuan, H. Cardiometabolic index: A new tool for screening the metabolically obese normal weight phenotype. J. Endocrinol. Investig. 2021, 44, 1253–1261. [Google Scholar] [CrossRef]
- Desquilbet, L.; Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Song, J.; Li, Y.; Zhu, J.; Liang, J.; Xue, S.; Zhu, Z. Non-linear associations of cardiometabolic index with insulin resistance, impaired fasting glucose, and type 2 diabetes among US adults: A cross-sectional study. Front. Endocrinol. 2024, 15, 1341828. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, L.; Lai, M.; Wan, L.; Zhang, X.; Chen, R. Cardiometabolic index and the risk of new-onset chronic diseases: Results of a national prospective longitudinal study. Front. Endocrinol. 2024, 15, 1446276. [Google Scholar] [CrossRef]
- Merkin, S.S.; Karlamangla, A.; Elashoff, D.; Grogan, T.; Seeman, T. Change in cardiometabolic score and incidence of cardiovascular disease: The multi-ethnic study of atherosclerosis. Ann. Epidemiol. 2015, 25, 912–917.e911. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, I.; Sotoda, Y.; Hirooka, S.; Orita, H. Association between cardiometabolic index and atherosclerotic progression in patients with peripheral arterial disease. Clin. Chim. Acta 2015, 446, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Pang, T.; Dang, C.; Liang, H.; Wu, J.; Shen, X.; Wang, L.; Lou, R.; Lan, H.; Zhang, P. Correlation between the cardiometabolic index and arteriosclerosis in patients with type 2 diabetes mellitus. BMC Cardiovasc. Disord. 2024, 24, 186. [Google Scholar] [CrossRef]
- Zhu, M.; Jin, H.; Yin, Y.; Xu, Y.; Zhu, Y. Association of cardiometabolic index with all-cause and cardiovascular mortality among middle-aged and elderly populations. Sci. Rep. 2025, 15, 681. [Google Scholar]
- Wang, J.; Xiao, L.; Li, Z. Cardiometabolic index and mortality risks: Elevated cancer and reduced cardiovascular mortality risk in a large cohort. Lipids Health Dis. 2024, 23, 427. [Google Scholar] [CrossRef]
- Liu, M.; Wang, C.; Liu, R.; Wang, Y.; Wei, B. Association between cardiometabolic index and all-cause and cause-specific mortality among the general population: NHANES 1999–2018. Lipids Health Dis. 2024, 23, 425. [Google Scholar] [CrossRef]
- Söderström, L.; Rosenblad, A. Long-term association between malnutrition and all-cause mortality among older adults: A 10-years follow-up study. Clin. Nutr. 2023, 42, 2554–2561. [Google Scholar] [CrossRef]
- Sun, D.L.; Wang, J.H.; Jiang, B.; Li, L.S.; Li, L.S.; Wu, L.; Wu, H.Y.; He, Y. Metabolic syndrome vs. its components for prediction of cardiovascular mortality: A cohort study in Chinese elderly adults. J. Geriatr. Cardiol. 2012, 9, 123–129. [Google Scholar]
- Vigna, L.; Tirelli, A.S.; Gaggini, M.; Di Piazza, S.; Tomaino, L.; Turolo, S.; Moroncini, G.; Chatzianagnostou, K.; Bamonti, F.; Vassalle, C. Insulin resistance and cardiometabolic indexes: Comparison of concordance in working-age subjects with overweight and obesity. Endocrine 2022, 77, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Camargo-Ramos, C.M.; Correa-Bautista, J.E.; Correa-Rodríguez, M.; Ramírez-Vélez, R. Dietary Inflammatory Index and Cardiometabolic Risk Parameters in Overweight and Sedentary Subjects. Int. J. Environ. Res. Public Health 2017, 14, 1104. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.A.; Yang, Y.; Zhang, L.; Sun, Z.; Jia, G.; Parrish, A.R.; Sowers, J.R. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism 2021, 119, 154766. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; I Gonzalez-Requero, A.; I Perez-Caballero, A.; Yubero-Serrano, E.M.; et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): A randomised controlled trial. Lancet 2022, 399, 1876–1885. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Tucker, W.J.; Fegers-Wustrow, I.; Halle, M.; Haykowsky, M.J.; Chung, E.H.; Kovacic, J.C. Exercise for Primary and Secondary Prevention of Cardiovascular Disease: JACC Focus Seminar 1/4. J. Am. Coll. Cardiol. 2022, 80, 1091–1106. [Google Scholar] [CrossRef] [PubMed]
- Walli-Attaei, M.; Rosengren, A.; Rangarajan, S.; Breet, Y.; Abdul-Razak, S.; Sharief, W.A.; Alhabib, K.F.; Avezum, A.; Chifamba, J.; Diaz, R.; et al. Metabolic, behavioural, and psychosocial risk factors and cardiovascular disease in women compared with men in 21 high-income, middle-income, and low-income countries: An analysis of the PURE study. Lancet 2022, 400, 811–821. [Google Scholar] [CrossRef]
- Thomson, B.; Emberson, J.; Lacey, B.; Lewington, S.; Peto, R.; Jemal, A.; Islami, F. Association Between Smoking, Smoking Cessation, and Mortality by Race, Ethnicity, and Sex Among US Adults. JAMA Netw. Open 2022, 5, e2231480. [Google Scholar] [CrossRef]
- Jeong, S.H.; Joo, H.J.; Kwon, J.; Park, E.C. Association Between Smoking Behavior and Insulin Resistance Using Triglyceride-Glucose Index Among South Korean Adults. J. Clin. Endocrinol. Metab. 2021, 106, e4531–e4541. [Google Scholar] [CrossRef]
- Caliri, A.W.; Tommasi, S.; Besaratinia, A. Relationships among smoking, oxidative stress, inflammation, macromolecular damage, and cancer. Mutat. Res. Rev. Mutat. Res. 2021, 787, 108365. [Google Scholar] [CrossRef]
- Xu, B.; Wu, Q.; Yin, G.; Lu, L.; La, R.; Zhang, Y.; Alifu, J.; Zhang, W.; Guo, F.; Ji, B.; et al. Associations of cardiometabolic index with diabetic statuses and insulin resistance: The mediating role of inflammation-related indicators. BMC Public Health 2024, 24, 2736. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.B.; Lin, Y.X.; Meng, T.T.; Tian, P.; Chen, J.L.; Zhang, X.H.; Xu, W.-H.; Zhang, Y.; Zhang, D.; Zheng, Y.; et al. Associations of the cardiometabolic index with insulin resistance, prediabetes, and diabetes in U.S. adults: A cross-sectional study. BMC Endocr. Disord. 2024, 24, 217. [Google Scholar] [CrossRef]
- Di Pino, A.; DeFronzo, R.A. Insulin Resistance and Atherosclerosis: Implications for Insulin-Sensitizing Agents. Endocr. Rev. 2019, 40, 1447–1467. [Google Scholar] [CrossRef] [PubMed]
- Bornfeldt, K.E.; Tabas, I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011, 14, 575–585. [Google Scholar] [CrossRef]
- Libby, P.; Loscalzo, J.; Ridker, P.M.; Farkouh, M.E.; Hsue, P.Y.; Fuster, V.; Hasan, A.A.; Amar, S. Inflammation, Immunity, and Infection in Atherothrombosis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2018, 72, 2071–2081. [Google Scholar] [CrossRef] [PubMed]
- Kaptoge, S.; Seshasai, S.R.; Gao, P.; Freitag, D.F.; Butterworth, A.S.; Borglykke, A.; Di Angelantonio, E.; Gudnason, V.; Rumley, A.; Lowe, G.D.; et al. Inflammatory cytokines and risk of coronary heart disease: New prospective study and updated meta-analysis. Eur. Heart J. 2014, 35, 578–589. [Google Scholar] [CrossRef]
- Wang, X.; He, B. Endothelial dysfunction: Molecular mechanisms and clinical implications. MedComm 2024, 5, e651. [Google Scholar] [CrossRef]
- Senoner, T.; Dichtl, W. Oxidative Stress in Cardiovascular Diseases: Still a Therapeutic Target? Nutrients 2019, 11, 2090. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total (n = 2157) | Q1 (n = 532) | Q2 (n = 546) | Q3 (n = 543) | Q4 (n = 536) | p | |
|---|---|---|---|---|---|---|
| Age, years | 66.4 ± 12.6 | 66.8 ± 13.5 | 67.5 ± 12.1 | 67.1 ± 11.5 | 64.3 ± 12.9 | <0.001 |
| Gender | <0.001 | |||||
| Male | 1244 (57.7) | 269 (50.6) | 304 (55.7) | 326 (60.0) | 345 (64.4) | |
| Female | 913 (42.3) | 263 (49.4) | 242 (44.3) | 217 (40.0) | 191 (35.6) | |
| Race | <0.001 | |||||
| Mexican American | 248 (11.5) | 33 (6.2) | 55 (10.0) | 76 (14.0) | 84 (15.7) | |
| Other Hispanic | 151 (7.0) | 35 (6.6) | 37 (6.8) | 40 (7.4) | 39 (7.3) | |
| Non-Hispanic White | 1205 (55.9) | 263 (49.4) | 302 (55.3) | 303 (55.8) | 337 (62.9) | |
| Non-Hispanic Black | 425 (19.7) | 165 (31.0) | 120 (22.0) | 89 (16.4) | 51 (9.5) | |
| Other Race | 128 (5.9) | 36 (6.8) | 32 (5.9) | 35 (6.5) | 25 (4.7) | |
| Educational level | 0.002 | |||||
| Below high school | 377 (17.5) | 80 (15.0) | 86 (15.8) | 106 (19.5) | 105 (19.6) | |
| High school | 909 (42.1) | 204 (38.4) | 235 (43.0) | 221 (40.7) | 249 (46.5) | |
| Above high school | 871 (40.4) | 248 (46.6) | 225 (41.2) | 216 (39.8) | 182 (34.0) | |
| Marital status | <0.001 | |||||
| Never married | 124 (5.8) | 45 (8.5) | 24 (4.4) | 22 (4.0) | 33 (6.2) | |
| Married/living with partner | 1284 (59.5) | 285 (53.6) | 315 (57.7) | 342 (63.0) | 342 (63.8) | |
| Divorced, separated, or widowed | 749 (34.7) | 202 (38.0) | 207 (37.9) | 179 (33.0) | 161 (30.0) | |
| Family PIR | 0.028 | |||||
| <1.3 | 886 (41.1) | 205 (38.5) | 208 (38.1) | 217 (40.0) | 256 (47.8) | |
| 1.3–3.5 | 812 (37.6) | 207 (38.9) | 213 (39.0) | 208 (38.3) | 184 (34.3) | |
| >3.5 | 459 (21.3) | 120 (22.6) | 125 (22.9) | 118 (21.7) | 96 (17.9) | |
| Smoking | <0.001 | |||||
| Never | 819 (38.0) | 225 (42.3) | 234 (42.9) | 196 (36.1) | 164 (30.6) | |
| Former | 874 (40.5) | 192 (36.1) | 200 (36.6) | 239 (44.0) | 243 (45.3) | |
| Current | 464 (21.5) | 115 (21.6) | 112 (20.5) | 108 (19.9) | 129 (24.1) | |
| Alcohol consumption | 0.494 | |||||
| <12 drinks/year | 1054 (48.9) | 261 (49.1) | 275 (50.4) | 271 (49.9) | 247 (46.1) | |
| ≥12 drinks/year | 1103 (51.1) | 271 (50.9) | 271 (49.6) | 272 (50.1) | 289 (53.9) | |
| MVPA | 844 (39.1) | 214 (40.2) | 214 (39.2) | 206 (37.9) | 210 (39.2) | 0.898 |
| BMI, kg/m2 | 29.9 ± 6.6 | 26.7 ± 6.0 | 29.2 ± 6.0 | 31.1 ± 6.4 | 32.4 ± 6.7 | <0.001 |
| TC, mmol/L | 4.8 ± 1.2 | 4.7 ± 1.1 | 4.6 ± 1.1 | 4.7 ± 1.2 | 5.1 ± 1.3 | <0.001 |
| Hypertension | 1532 (71.0) | 370 (69.6) | 371 (68.0) | 394 (72.6) | 397 (74.1) | 0.152 |
| Diabetes | 651 (30.2) | 97 (18.2) | 165 (30.2) | 174 (32.0) | 215 (40.1) | <0.001 |
| Antihypertensive medication | 1446 (67.0) | 342 (64.3) | 346 (63.4) | 374 (68.9) | 384 (71.6) | 0.011 |
| Antidiabetic medication | 308 (14.3) | 45 (8.5) | 73 (13.4) | 77 (14.2) | 113 (21.1) | <0.001 |
| Cardiovascular medication | 1485 (68.9) | 347 (65.2) | 355 (65.0) | 388 (71.5) | 395 (73.7) | 0.002 |
| Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|
| Death, (%) | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| All-cause mortality | |||||||
| CMI | 887 (41.1) | 0.974 (0.973, 0.975) | <0.001 | 1.135 (1.133, 1.136) | <0.001 | 1.113 (1.112, 1.115) | <0.001 |
| Q1 | 204 (38.4) | 1.318 (1.315, 1.322) | <0.001 | 1.350 (1.346, 1.353) | <0.001 | 1.426 (1.423, 1.430) | <0.001 |
| Q2 | 214 (39.2) | Ref. | Ref. | Ref. | |||
| Q3 | 236 (43.5) | 1.183 (1.180, 1.186) | <0.001 | 1.278 (1.274, 1.281) | <0.001 | 1.332 (1.328, 1.335) | <0.001 |
| Q4 | 233 (43.5) | 1.109 (1.106, 1.111) | <0.001 | 1.475 (1.471, 1.479) | <0.001 | 1.426 (1.422, 1.430) | <0.001 |
| Cardiovascular mortality | |||||||
| CMI | 300 (13.9) | 1.056 (1.054, 1.057) | <0.001 | 1.134 (1.132, 1.135) | <0.001 | 1.064 (1.062, 1.065) | <0.001 |
| Q1 | 70 (13.2) | 1.658 (1.650, 1.665) | <0.001 | 1.671 (1.664, 1.679) | <0.001 | 1.678 (1.670, 1.686) | <0.001 |
| Q2 | 63 (11.5) | Ref. | Ref. | Ref. | |||
| Q3 | 79 (14.6) | 1.333 (1.327, 1.339) | <0.001 | 1.386 (1.380, 1.393) | <0.001 | 1.397 (1.391, 1.404) | <0.001 |
| Q4 | 88 (16.4) | 1.714 (1.706, 1.721) | <0.001 | 1.983 (1.974, 1.991) | <0.001 | 1.826 (1.818, 1.835) | <0.001 |
| All-Cause Mortality | Cardiovascular Mortality | |||||||
|---|---|---|---|---|---|---|---|---|
| Death, (%) | HR (95% CI) | p | p for Interaction | Death, (%) | HR (95% CI) | p | p for Interaction | |
| Gender | <0.001 | <0.001 | ||||||
| Male | 560 (45.0) | 1.065 (1.063, 1.066) | <0.001 | 201 (16.2) | 1.167 (1.164, 1.169) | <0.001 | ||
| Female | 327 (35.8) | 1.201 (1.199, 1.203) | <0.001 | 99 (10.8) | 0.903 (0.900, 0.905) | <0.001 | ||
| Educational level | <0.001 | <0.001 | ||||||
| Below high school | 189 (50.1) | 1.330 (1.326, 1.333) | <0.001 | 57 (15.1) | 1.491 (1.483, 1.500) | <0.001 | ||
| High school | 390 (42.9) | 1.107 (1.105, 1.109) | <0.001 | 119 (13.1) | 0.800 (0.798, 0.803) | <0.001 | ||
| Above high school | 308 (35.4) | 1.054 (1.052, 1.056) | <0.001 | 124 (14.2) | 1.219 (1.217, 1.222) | <0.001 | ||
| Marital status | <0.001 | <0.001 | ||||||
| Never married | 36 (29.0) | 0.363 (0.359, 0.367) | <0.001 | 16 (12.9) | 0.163 (0.156, 1.170) | <0.001 | ||
| Married/living with partner | 483 (37.6) | 1.142 (1.140, 1.143) | <0.001 | 162 (12.6) | 1.057 (1.054, 1.059) | <0.001 | ||
| Divorced, separated, or widowed | 368 (49.1) | 1.030 (1.028, 1.032) | <0.001 | 122 (16.3) | 1.073 (1.069, 1.076) | <0.001 | ||
| Family PIR | <0.001 | <0.001 | ||||||
| <1.3 | 371 (41.9) | 0.995 (0.993, 0.998) | <0.001 | 120 (13.5) | 0.877 (0.874, 0.880) | <0.001 | ||
| 1.3–3.5 | 362 (44.6) | 1.255 (1.253, 1.257) | <0.001 | 121 (14.9) | 1.230 (1.226, 1.233) | <0.001 | ||
| >3.5 | 154 (33.6) | 1.003 (1.000, 1.006) | 0.061 | 59 (12.9) | 1.127 (1.122, 1.131) | <0.001 | ||
| Smoking status | <0.001 | <0.001 | ||||||
| Never | 304 (37.1) | 1.062 (1.060, 1.065) | <0.001 | 107 (13.1) | 0.914 (0.910, 0.918) | <0.001 | ||
| Former | 408 (46.7) | 1.137 (1.135, 1.139) | <0.001 | 141 (16.1) | 1.167 (1.164, 1.171) | <0.001 | ||
| Current | 175 (37.7) | 1.005 (1.002, 1.008) | 0.002 | 52 (11.2) | 0.947 (0.943, 0.951) | <0.001 | ||
| Alcohol consumption | <0.001 | <0.001 | ||||||
| <12 drinks/year | 408 (38.7) | 1.246 (1.244, 1.248) | <0.001 | 149 (14.1) | 1.107 (1.105, 1.110) | <0.001 | ||
| ≥12 drinks/year | 479 (43.4) | 0.968 (0.966, 0.970) | <0.001 | 151 (13.7) | 1.005 (1.002, 1.008) | 0.001 | ||
| MVPA | <0.001 | <0.001 | ||||||
| No | 577 (44.0) | 1.091 (1.090, 1.093) | <0.001 | 205 (15.6) | 1.007 (1.004, 1.009) | <0.001 | ||
| Yes | 310 (36.7) | 1.149 (1.147, 1.151) | <0.001 | 95 (11.3) | 1.142 (1.139, 1.146) | <0.001 | ||
| Hypertension | <0.001 | <0.001 | ||||||
| No | 249 (39.8) | 1.083 (1.081, 1.086) | <0.001 | 79 (12.6) | 1.021 (1.016, 1.027) | <0.001 | ||
| Yes | 638 (41.6) | 1.091 (1.089, 1.092) | <0.001 | 221 (14.3) | 1.071 (1.069, 1.073) | <0.001 | ||
| Diabetes | <0.001 | <0.001 | ||||||
| No | 610 (40.5) | 1.078 (1.076, 1.080) | <0.001 | 197 (13.1) | 1.030 (1.027, 1.033) | <0.001 | ||
| Yes | 277 (42.6) | 1.129 (1.128, 1.131) | <0.001 | 103 (15.8) | 1.072 (1.069, 1.075) | <0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, D.; Li, W.; Luo, W.; Yang, Y.; Yi, J.; Li, C.; Gao, H.; Zhao, X. Association Between Cardiometabolic Index and Mortality Among Patients with Atherosclerotic Cardiovascular Disease: Evidence from NHANES 1999–2018. Medicina 2025, 61, 1064. https://doi.org/10.3390/medicina61061064
Yang D, Li W, Luo W, Yang Y, Yi J, Li C, Gao H, Zhao X. Association Between Cardiometabolic Index and Mortality Among Patients with Atherosclerotic Cardiovascular Disease: Evidence from NHANES 1999–2018. Medicina. 2025; 61(6):1064. https://doi.org/10.3390/medicina61061064
Chicago/Turabian StyleYang, Duo, Wei Li, Wei Luo, Yunxiao Yang, Jiayi Yi, Chen Li, Hai Gao, and Xuedong Zhao. 2025. "Association Between Cardiometabolic Index and Mortality Among Patients with Atherosclerotic Cardiovascular Disease: Evidence from NHANES 1999–2018" Medicina 61, no. 6: 1064. https://doi.org/10.3390/medicina61061064
APA StyleYang, D., Li, W., Luo, W., Yang, Y., Yi, J., Li, C., Gao, H., & Zhao, X. (2025). Association Between Cardiometabolic Index and Mortality Among Patients with Atherosclerotic Cardiovascular Disease: Evidence from NHANES 1999–2018. Medicina, 61(6), 1064. https://doi.org/10.3390/medicina61061064