
Comparing the Outcomes of Cast Immobilization with and Without K-Wire Fixation for Displaced Distal Radius Fractures in the Pediatric Population: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Study Selection and Data Extraction
2.3. Risk of Bias
2.4. Parameters Evaluated
2.5. Statistical Analysis
3. Results
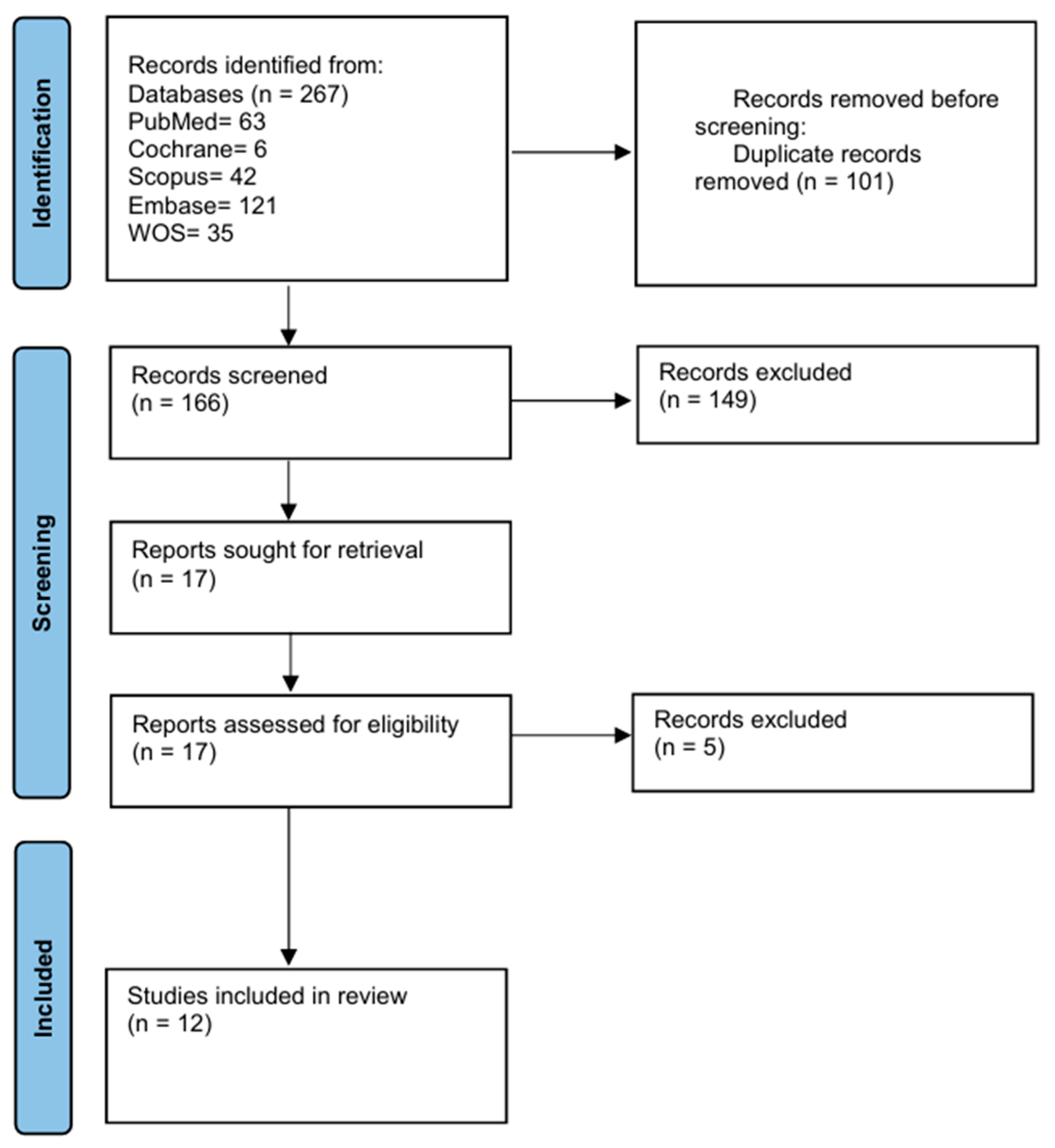
3.1. Study Selection and Characteristics
3.2. Patient Demographics and Baseline Characteristics
3.3. Clinical and Functional Outcomes by Meta-Analysis
3.3.1. Intervention Details
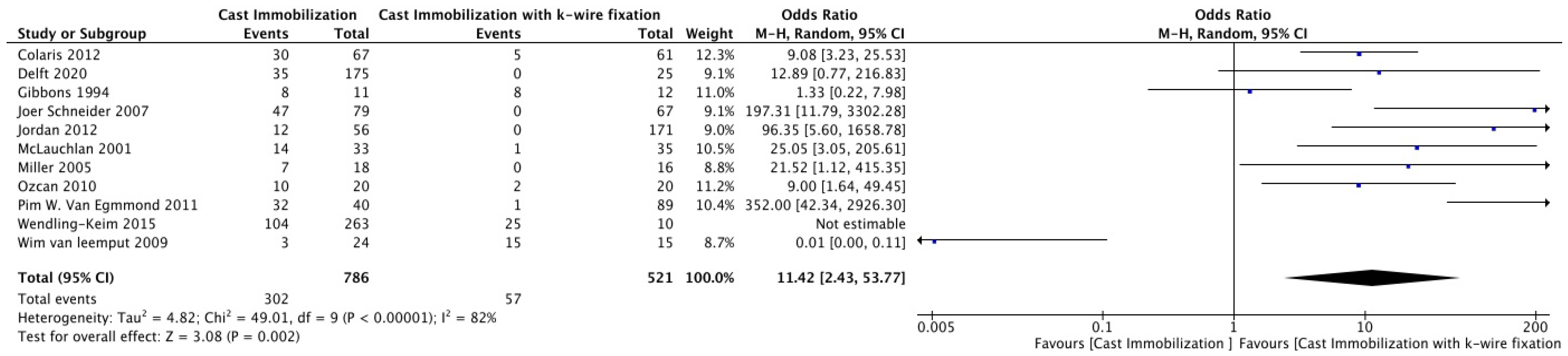
3.3.2. Re-Displacement
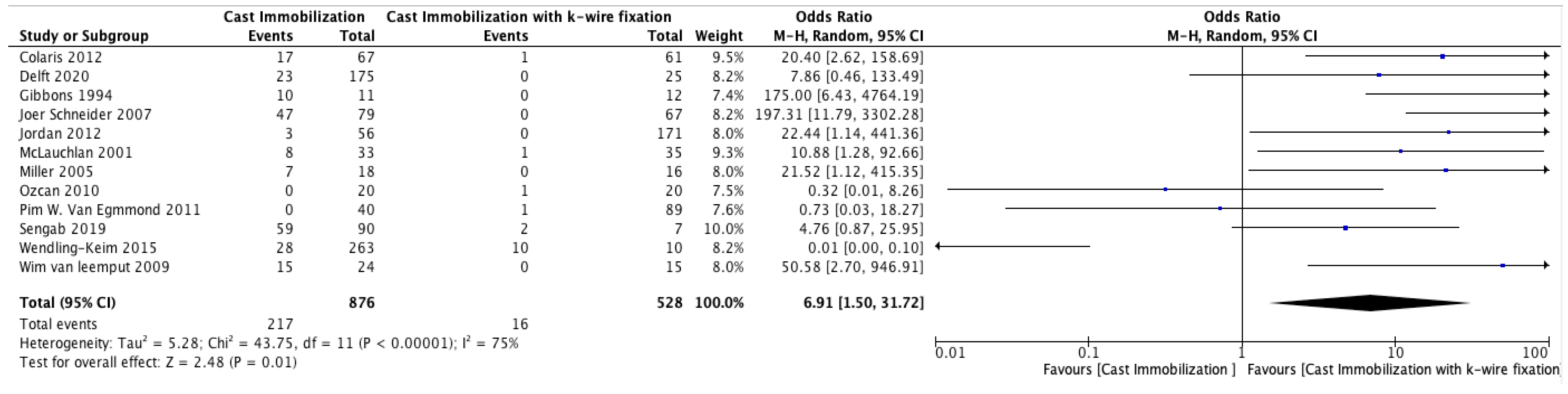
3.3.3. Secondary Interventions
3.3.4. Complications
3.4. Systematic Review
3.4.1. Radiological Outcomes
3.4.2. Range of Motion (ROM) Outcomes
3.4.3. Angulation Outcomes
3.5. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DDRFs | displaced distal radius fractures. |
| MINORS | Methodological Index for Non-Randomized Studies |
| RCT | Randomized controlled study |
| CI | Confidence interval |
References
- Sengab, A.; Krijnen, P.; Schipper, I.B. Displaced distal radius fractures in children, cast alone vs additional K-wire fixation: A meta-analysis. Eur. J. Trauma Emerg. Surg. 2019, 45, 1003–1011. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Joeris, A.; Lutz, N.; Blumenthal, A.; Slongo, T.; Audigé, L.; The, A.O. Pediatric Comprehensive Classification of Long Bone Fractures (PCCF) part I: Location and morphology of 2,292 upper extremity fractures in children and adolescents. Acta Orthop. 2017, 88, 129–132. [Google Scholar] [CrossRef]
- Cheng, J.C.; Shen, W.Y. Limb fracture pattern in diferent pediatric age groups: A study of 3,350 children. J. Orthop. Trauma 1993, 7, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Worlock, P.; Stower, M. Fracture patterns in Nottingham children. J. Pediatr. Orthop. 1986, 6, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Rennie, L.; Court-Brown, C.M.; Mok, J.Y.; Beattie, T.F. The epidemiology of fractures in children. Injury 2007, 38, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Landin, L.A. Epidemiology of children’s fractures. J. Pediatr. Orthop. B 1997, 6, 79–83. [Google Scholar] [CrossRef]
- Voto, S.J.; Weiner, D.S.; Leighley, B.L. Redisplacement after closed reduction of forearm fractures in children. J. Pediatr. Orthop. 1990, 10, 79–84. [Google Scholar] [CrossRef]
- Proctor, M.T.; Moore, D.J.; Paterson, J.M.H. Redisplacement after manipulation of distal radial fractures in children. J. Bone Jt. Surg. 1993, 75-B, 453–454. [Google Scholar] [CrossRef]
- Davis, D.R.; Green, D.P. Forearm fractures in children: Pitfalls and complications. Clin. Orthop. 1976, 120, 172–183. [Google Scholar] [CrossRef]
- Wong, K.K.; Chan, K.W. Percutaneous pinning for distal radius fractures: A review of techniques and outcomes. J. Orthop. Surg. 2010, 18, 330–333. [Google Scholar]
- Grewal, R.; MacDermid, J.C. The risk of adverse outcomes in extra-articular distal radius fractures is increased with malalignment in patients of all ages but mitigated in older patients. J. Hand Surg. 2007, 32, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Mah, E.T.; Atkinson, R.N. Percutaneous Kirschner wire stabilisation following closed reduction of Colles’ fractures. J. Hand Surg. 1992, 17, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Schneider, J.; Staubli, G.; Kubat, S. Treating Displaced Distal Forearm Fractures in Children. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2007, 33, 619–625. [Google Scholar] [CrossRef]
- Van Leemput, W.; De Ridder, K. Distal metaphyseal radius fractures in children: Reduction with or without pinning. Acta Orthop. Belg. 2009, 75, 306–309. [Google Scholar] [PubMed]
- van Egmond, P.W.; Schipper, I.B.; van Luijt, P.A. Displaced distal forearm fractures in children with an indication for reduction under general anesthesia should be percutaneously fixated. Eur. J. Orthop. Surg. Traumatol. 2012, 22, 201–207. [Google Scholar] [CrossRef]
- Miller, B.S.; Taylor, B.; Widmann, R.F.; Bae, D.S.; Snyder, B.D.; Waters, P.M. Cast Immobilization Versus Percutaneous Pin Fixation of Displaced Distal Radius Fractures in Children. J. Pediatr. Orthop. 2005, 25, 490–494. [Google Scholar] [CrossRef]
- Gibbons, C.L.M.H.; Woods, D.A.; Pailthorpe, C.; Carr, A.J.; Worlock, P. The Management of Isolated Distal Radius Fractures in Children. J. Pediatr. Orthop. 1994, 14, 207–210. [Google Scholar] [CrossRef]
- Colaris, J.W.; Allema, J.H.; Biter, L.U.; de Vries, M.R.; van de Ven, C.P.; Bloem, R.M.; Kerver, A.J.; Reijman, M.; Verhaar, J.A. Re-displacement of stable distal both-bone forearm fractures in children: A randomised controlled multicentre trial. Injury 2013, 44, 498–503. [Google Scholar] [CrossRef]
- van Delft, E.A.K.; Vermeulen, J.; Schep, N.W.L.; van Stralen, K.J.; van der Bij, G.J. Prevention of secondary displacement and reoperation of distal metaphyseal forearm fractures in children. J. Clin. Orthop. Trauma 2020, 11, S817–S822. [Google Scholar] [CrossRef]
- Ozcan, M.; Memisoglu, S.; Copuroglu, C.; Saridogan, K. Percutaneous Kirschner Wire fixation in distal radius metaphyseal fractures in children: Does it change the overall outcome? Hippokratia 2010, 14, 265–270. [Google Scholar]
- McLauchlan, G.J.; Cowan, B.; Annan, I.H.; Robb, J.E. Management of completely displaced metaphyseal fractures of the distal radius in children: A prospective, randomised controlled trial. J. Bone Jt. Surg. 2002, 84, 413–417. [Google Scholar] [CrossRef]
- Diederix, L.W.; Roth, K.C.; Edomskis, P.P.; Musters, L.; Allema, J.H.; Kraan, G.A.; Reijman, M.; Colaris, J.W. Do We Need to Stabilize All Reduced Metaphyseal Both-bone Forearm Fractures in Children with K-wires? Clin. Orthop. Relat. Res. 2022, 480, 395–404. [Google Scholar] [CrossRef]
- Jordan, R.W.; Westacott, D.J. Displaced paediatric distal radius fractures—When should we use percutaneous wires? Injury 2012, 43, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Wendling-Keim, D.S.; Wieser, B.; Dietz, H.-G. Closed reduction and immobilization of displaced distal radial fractures. Method of choice for the treatment of children? Eur. J. Trauma Emerg. Surg. 2015, 41, 421–428. [Google Scholar] [CrossRef]
- Handoll, H.H.; Madhok, R. Percutaneous pinning for treating distal radial fractures in adults. Cochrane Database Syst. Rev. 2003. [Google Scholar] [CrossRef]
- Nakashian, M.N.; Pointer, L.; Owens, B.D.; Wolf, J.M. Incidence of loss of fixation of distal radius fractures after percutaneous K-wire fixation. J. Hand Surg. 2012, 37, 330–335. [Google Scholar]
- Leung, F.; Tu, Y.K.; Chew, W.Y.C.; Chow, S.P. Comparison of external and percutaneous pin fixation with plate fixation for intra-articular distal radial fractures. J. Bone Jt. Surg. 2000, 82, 659–665. [Google Scholar] [CrossRef]
- Chung, K.C.; Watt, A.J.; Kotsis, S.V.; Margaliot, Z.; Haase, S.C.; Kim, H.M. Treatment of unstable distal radial fractures with the volar locking plating system. J. Bone Jt. Surg. 2006, 88, 2687–2694. [Google Scholar] [CrossRef]
- Rozental, T.D.; Blazar, P.E. Functional outcome and complications after volar plating for dorsally displaced, unstable fractures of the distal radius. J. Hand Surg. 2006, 31, 359–365. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Year | Study Design | Country | Total Patients | Group 1 (Cast) | Group 2 (K-Wire) | Age Range (Years) | Males (n) | Females (n) |
|---|---|---|---|---|---|---|---|---|---|
| Wendling‚ ÄêKeim, 2015 [25] | 2015 | Retrospective | Germany | 293 | 263 | 30 | 0–18 | ||
| Jordan, 2012 [24] | 2012 | Retrospective | United Kingdom | 227 | 56 | 171 | 2–15 | 63 | 20 |
| Diederix, 2021 [23] | 2021 | RCT | Netherlands | 128 | 67 | 61 | 3–9 | ||
| McLauchlan, 2001 [22] | 2001 | RCT | Scotland | 68 | 33 | 35 | 4–14 | 42 | 26 |
| Ozcan, 2010 [21] | 2010 | Retrospective | Turkey | 40 | 20 | 20 | 5–15 (K-wire), 6–14 (Cast) | ||
| Delft, 2020 [20] | 2020 | Retrospective | Netherlands | 200 | 175 | 25 | 8–14 | 118 | 82 |
| Colaris, 2013 [19] | 2012 | RCT | Netherlands | 128 | 67 | 61 | <16 | 83 | 45 |
| Gibbons, 1994 [18] | 1994 | Retrospective randomized | England | 23 | 11 | 12 | 5–14 | 15 | 8 |
| Miller, 2005 [17] | 2005 | Prospective randomized | United States | 34 | 18 | 16 | 10–14 | 31 | 3 |
| Pim W. Van Egmond, 2011 [16] | 2011 | Retrospective cohort | Netherlands | 129 | 40 | 89 | 3–17 | 134 | 74 |
| Wim van leemput, 2009 [15] | 2009 | Retrospective | Belgium | 39 | 24 | 15 | 8–13 | 27 | 12 |
| Joreg Schneider, 2007 [14] | 2007 | Retrospective | Switzerland | 146 | 79 | 67 | 3–16 | 150 | 75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alotaibi, M.N.; Aldaraani, L.G.A.; Altala, A.S.; Alqurashi, A.A.; Alateeq, I.S.; Alkhamisi, A.A.; Allehaimeed, I.S.; Jad, A.Y.; Alosaimi, H.; Alharbi, B.H.; et al. Comparing the Outcomes of Cast Immobilization with and Without K-Wire Fixation for Displaced Distal Radius Fractures in the Pediatric Population: A Systematic Review and Meta-Analysis. Medicina 2025, 61, 852. https://doi.org/10.3390/medicina61050852
Alotaibi MN, Aldaraani LGA, Altala AS, Alqurashi AA, Alateeq IS, Alkhamisi AA, Allehaimeed IS, Jad AY, Alosaimi H, Alharbi BH, et al. Comparing the Outcomes of Cast Immobilization with and Without K-Wire Fixation for Displaced Distal Radius Fractures in the Pediatric Population: A Systematic Review and Meta-Analysis. Medicina. 2025; 61(5):852. https://doi.org/10.3390/medicina61050852
Chicago/Turabian StyleAlotaibi, Muteb N., Lamya Ghanim A. Aldaraani, Abdulaziz S. Altala, Aseel A. Alqurashi, Ismail S. Alateeq, Abdulkarim Abdullatif Alkhamisi, Ibrahim Saleh Allehaimeed, Ammar Yasser Jad, Hamed Alosaimi, Bassam H. Alharbi, and et al. 2025. "Comparing the Outcomes of Cast Immobilization with and Without K-Wire Fixation for Displaced Distal Radius Fractures in the Pediatric Population: A Systematic Review and Meta-Analysis" Medicina 61, no. 5: 852. https://doi.org/10.3390/medicina61050852
APA StyleAlotaibi, M. N., Aldaraani, L. G. A., Altala, A. S., Alqurashi, A. A., Alateeq, I. S., Alkhamisi, A. A., Allehaimeed, I. S., Jad, A. Y., Alosaimi, H., Alharbi, B. H., Alenezi, A., Almutairi, A. Z., Alroudhan, F. K., & Alqarni, M. M. (2025). Comparing the Outcomes of Cast Immobilization with and Without K-Wire Fixation for Displaced Distal Radius Fractures in the Pediatric Population: A Systematic Review and Meta-Analysis. Medicina, 61(5), 852. https://doi.org/10.3390/medicina61050852