
Is Percutaneous Endoscopic Gastrostomy an Innocent Procedure? A Retrospective Single-Center Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Application Technique
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PEG | Percutaneous endoscopic gastrostomy |
| PD | Parkinson’s disease |
| CP | Cerebral palsy |
| ALS | Amyothrophic lateral sclerosis |
| MS | Multiple sclerosis |
References
- Arvanitakis, M.; Gkolfakis, P.; Despott, E.J.; Ballarin, A.; Beyna, T.; Boeykens, K.; Elbe, P.; Gisbertz, I.; Hoyois, A.; Mosteanu, O.; et al. Endoscopic Management of Enteral Tubes in Adult Patients—Part 1: Definitions and Indications. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 81–92. [Google Scholar] [CrossRef]
- Piñar-Gutiérrez, A.; González-Gracia, L.; Vázquez Gutiérrez, R.; García-Rey, S.; Jiménez-Sánchez, A.; González-Navarro, I.; Tatay-Domínguez, D.; Garrancho-Domínguez, P.; Remón-Ruiz, P.J.; Martínez-Ortega, A.J.; et al. Percutaneous Gastrostomies: Associated Complications in PUSH vs. PULL Techniques over 12 Years in a Referral Centre. J. Clin. Med. 2024, 13, 1836. [Google Scholar] [CrossRef]
- Akıcı, M.; Erşen, O.; Çelik, G.; Çilekar, M. Experiences with Percutaneous Endoscopic Gastrostomy in a General Surgery Clinic. Med. J. Süleyman Demirel Univ. 2019, 26, 234–238. [Google Scholar] [CrossRef]
- Turan, U.F.; Katar, M.K. Evaluation of 644 Percutaneous Endoscopic Gastrostomy Patients in a Single Center. Cureus 2023, 15, e38324. [Google Scholar] [CrossRef]
- Casas Deza, D.; Monzón Baez, R.M.; Lamuela Calvo, L.J.; Betoré Glaria, E.; Montil Miguel, E.; Julián Gomara, B.; Vicente Lidón, R. Complications and Survival Following Percutaneous Endoscopic Gastrostomy Tube Placement. Rev. Española Enfermedades Dig. 2024, 116, 526–531. [Google Scholar] [CrossRef]
- Wei, M.; Ho, E.; Hegde, P. An Overview of Percutaneous Endoscopic Gastrostomy Tube Placement in the Intensive Care Unit. J. Thorac. Dis. 2021, 13, 5277–5296. [Google Scholar] [CrossRef] [PubMed]
- Gauderer, M.W.; Ponsky, J.L.; Izant, R.J., Jr. Gastrostomy without Laparotomy: A Percutaneous Endoscopic Technique. J. Pediatr. Surg. 1980, 15, 872–875. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.R.; Brotman, M.; Norris, F. Percutaneous Gastrostomy: A New Simplified and Cost-Effective Technique. Am. J. Surg. 1984, 148, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Rahnemai-Azar, A.A.; Rahnemaiazar, A.A.; Naghshizadian, R.; Kurtz, A.; Farkas, D.T. Percutaneous Endoscopic Gastrostomy: Indications, Technique, Complications and Management. World J. Gastroenterol. WJG 2014, 20, 7739. [Google Scholar] [CrossRef]
- Park, J.W.; Kim, T.G.; Cho, K.B.; Kim, J.S.; Cho, J.W.; Jeon, J.W.; Lim, S.G.; Kim, C.G.; Park, H.J.; Kim, T.J.; et al. A Multicenter Survey of Percutaneous Endoscopic Gastrostomy in 2019 at Korean Medical Institutions. Gut Liver 2024, 18, 77–84. [Google Scholar] [CrossRef]
- Doğu, C.; Yılmaz, P.Ö. Percutaneous Endoscopic Gastrostomy Experience in a Tertiary Intensive Care Unit. Meandros Med. Dent. J. 2021, 22, 28. [Google Scholar] [CrossRef]
- Gkolfakis, P.; Arvanitakis, M.; Despott, E.J.; Ballarin, A.; Beyna, T.; Boeykens, K.; Elbe, P.; Gisbertz, I.; Hoyois, A.; Mosteanu, O.; et al. Endoscopic Management of Enteral Tubes in Adult Patients—Part 2: Peri- and Post-Procedural Management. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 178–195. [Google Scholar] [CrossRef]
- Peveling-Oberhag, J.; Osman, I.; Walter, D.; Filmann, N.; Stratmann, K.; Hausmann, J.; Knop, V.; Waidmann, O.; Vermehren, J.; Herrmann, E.; et al. Risk Factors for Early and Late Procedure-related Adverse Events in Percutaneous Endoscopic Gastrostomy: A Single Center, Retrospective Study. J. Gastroenterol. Hepatol. 2019, 34, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Vujasinovic, M.; Ingre, C.; Baldaque Silva, F.; Frederiksen, F.; Yu, J.; Elbe, P. Complications and Outcome of Percutaneous Endoscopic Gastrostomy in a High-Volume Centre. Scand. J. Gastroenterol. 2019, 54, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Im, J.P.; Kim, J.W.; Kim, S.-E.; Ryu, D.Y.; Cha, J.M.; Kim, E.Y.; Kim, E.R.; Chang, D.K. Risk Factors for Complications and Mortality of Percutaneous Endoscopic Gastrostomy: A Multicenter, Retrospective Study. Surg. Endosc. 2013, 27, 3806–3815. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.S.; Schettler, A.; Markowski, A.; Luettig, B.; Kaufmann, B.; Klamt, S.; Lenzen, H.; Momma, M.; Seipt, C.; Lankisch, T.; et al. Complication and Mortality Rate after Percutaneous Endoscopic Gastrostomy Are Low and Indication-Dependent*. Scand. J. Gastroenterol. 2014, 49, 891–898. [Google Scholar] [CrossRef]
- Ley, D.; Austin, K.; Wilson, K.A.; Saha, S. Tutorial on Adult Enteral Tube Feeding: Indications, Placement, Removal, Complications, and Ethics. J. Parenter. Enter. Nutr. 2023, 47, 677–685. [Google Scholar] [CrossRef]
- Limpias Kamiya, K.J.L.; Hosoe, N.; Takabayashi, K.; Hayashi, Y.; Fukuhara, S.; Mutaguchi, M.; Nakamura, R.; Kawakubo, H.; Kitagawa, Y.; Ogata, H.; et al. Factors Predicting Major Complications, Mortality, and Recovery in Percutaneous Endoscopic Gastrostomy. JGH Open 2021, 5, 590–598. [Google Scholar] [CrossRef]
- Stenberg, K.; Eriksson, A.; Odensten, C.; Darehed, D. Mortality and Complications after Percutaneous Endoscopic Gastrostomy: A Retrospective Multicentre Study. BMC Gastroenterol. 2022, 22, 361. [Google Scholar] [CrossRef]
- Boylan, C.; Barrett, D.; Li, V.; Merrick, S.; Steed, H. Longitudinal Complications Associated with PEG: Rate and Severity of 30-Day and 1-Year Complications Experienced by Patients after Primary PEG Insertion. Clin. Nutr. ESPEN 2021, 43, 514–521. [Google Scholar] [CrossRef]
- Pih, G.Y.; Na, H.K.; Ahn, J.Y.; Jung, K.W.; Kim, D.H.; Lee, J.H.; Choi, K.D.; Song, H.J.; Lee, G.H.; Jung, H.-Y. Risk Factors for Complications and Mortality of Percutaneous Endoscopic Gastrostomy Insertion. BMC Gastroenterol. 2018, 18, 101. [Google Scholar] [CrossRef] [PubMed]
- Szlagatys-Sidorkiewicz, A.; Borkowska, A.; Popińska, K.; Toporowska-Kowalska, E.; Grzybowska-Chlebowczyk, U.; Wernicka, A.; Hapyn, E.; Sibilska, M.; Gębora-Kowalska, B.; Więcek, S.; et al. Complications of PEG Are Not Related to Age—The Result of 10-Year Multicenter Survey. Adv. Med. Sci. 2016, 61, 1–5. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Characteristics | Count | % | |
|---|---|---|---|
| Gender | Male | 218 | 42.4 |
| Female | 297 | 57.6 | |
| Age | Mean ± SD. (Min.–Max.) | 68.7 ± 15.2 (12–103) |
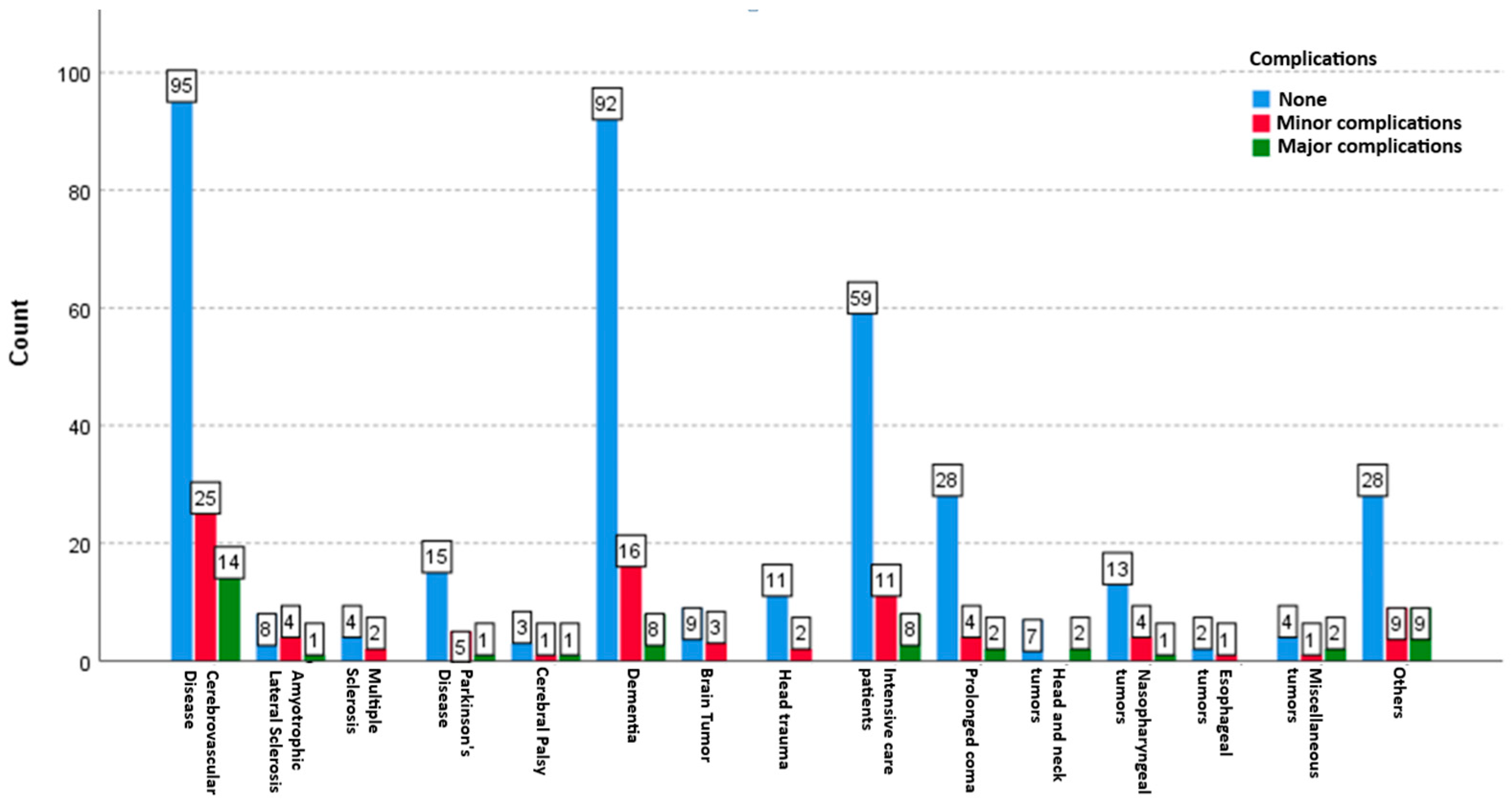
| General Disease Group | Diseases | Complications | Minor Complications | Major Complications | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| None | Minor Complications | Major Complications | Peristomal Infection | PEG Site Leakage | PEG Edge Bleeding | Tube Dislodgement | Pneumoperitoneum | Bleeding | Aspiration Pneumonia | Internal Organ Injury | Buried Bumper Syndrome | Necrotizing Fasciitis | |||||||
| n | Count | % | Count | % | Count | % | p | n | n | n | n | n | n | n | n | n | n | ||
| Neurological diseases | Cerebrovascular disease | 134 | 95 | 70.90 | 25 | 18.70 | 14 | 10.40 | 0.000 ** | 7 | 4 | 6 | 4 | 4 | 2 | 4 | 1 | 6 | 1 |
| Amyotrophic lateral sclerosis | 13 | 8 | 61.50 | 4 | 30.80 | 1 | 7.70 | 0.058 | 2 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |
| Multiple sclerosis | 6 | 4 | 66.70 | 2 | 33.30 | 0 | 0.00 | 0.414 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Parkinson’s disease | 21 | 15 | 71.40 | 5 | 23.80 | 1 | 4.80 | 0.001 ** | 2 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | |
| Cerebral palsy | 5 | 3 | 60.00 | 1 | 20.00 | 1 | 20.00 | 0.449 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | |
| Dementia | 116 | 92 | 79.30 | 16 | 13.80 | 8 | 6.90 | 0.000 ** | 6 | 2 | 3 | 2 | 3 | 1 | 1 | 2 | 4 | 0 | |
| Brain tumour | 12 | 9 | 75.00 | 3 | 25.00 | 0 | 0.00 | 0.083 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Reduced level of consciousness | Head trauma | 13 | 11 | 84.60 | 2 | 15.40 | 0 | 0.00 | 0.013 * | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Intensive care patients | 78 | 59 | 75.60 | 11 | 14.10 | 8 | 10.30 | 0.000 ** | 3 | 3 | 2 | 1 | 2 | 3 | 1 | 0 | 3 | 1 | |
| Prolonged coma | 34 | 28 | 82.40 | 4 | 11.80 | 2 | 5.90 | 0.000 ** | 2 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | |
| Malignancy | Head and neck tumours | 9 | 7 | 77.80 | 0 | 0.00 | 2 | 22.20 | 0.096 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Nasopharyngeal tumours | 18 | 13 | 72.20 | 4 | 22.20 | 1 | 5.60 | 0.002 ** | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | |
| Oesophageal cancer | 3 | 2 | 66.70 | 1 | 33.30 | 0 | 0.00 | 0.564 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Miscellaneous | 7 | 4 | 57.10 | 1 | 14.30 | 2 | 28.60 | 0.368 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | |
| Others | Unclassified | 46 | 28 | 60.90 | 9 | 19.60 | 9 | 19.60 | 0.000 ** | 1 | 2 | 3 | 2 | 1 | 2 | 3 | 0 | 4 | 0 |
| Total | 515 | 378 | 88 | 49 | 1.42 | 27 | 17 | 20 | 13 | 11 | 9 | 12 | 5 | 20 | 3 | ||||
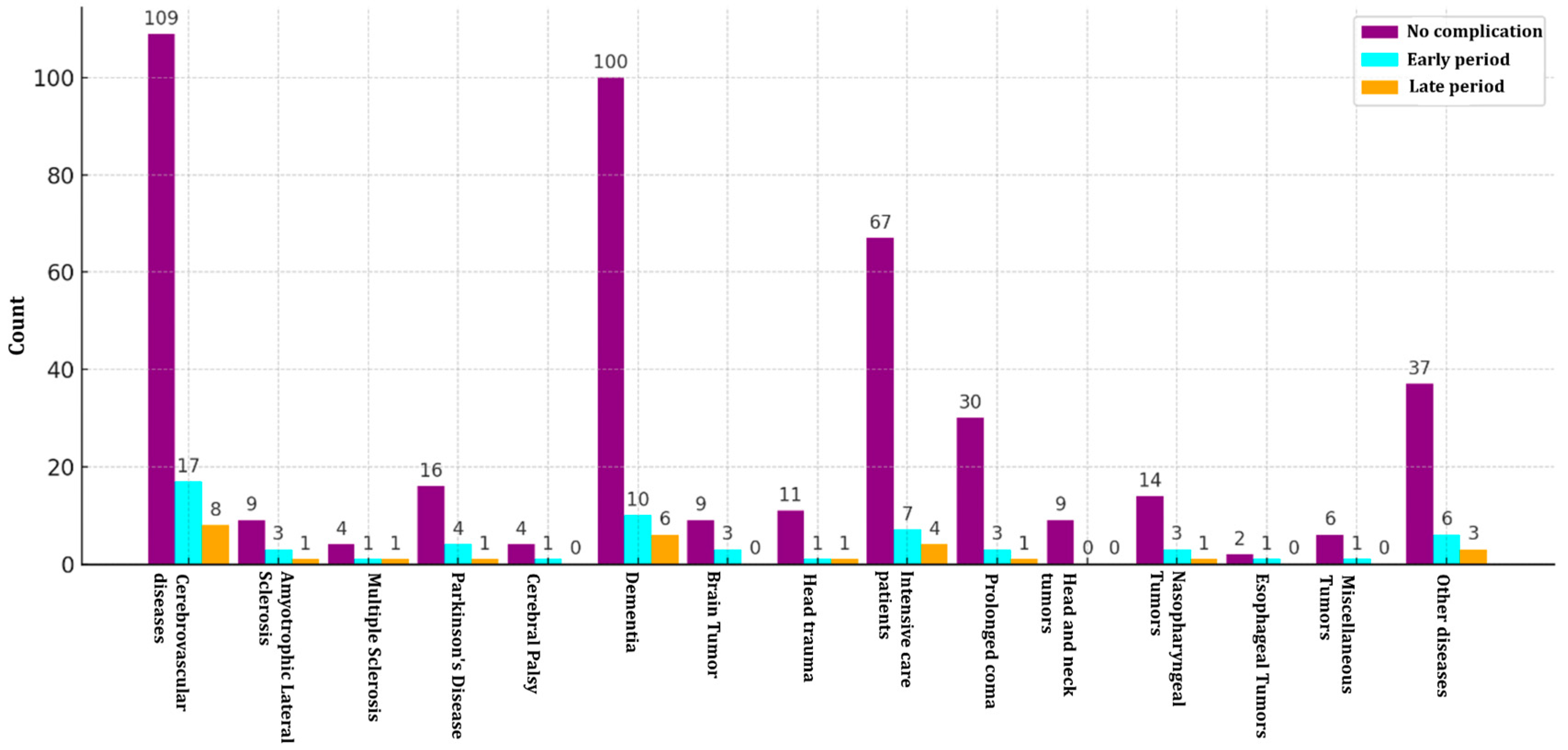
| General Disease Group | Diseases | n | Complications | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Early Period | Late Period | |||||||
| Count | % | Count | % | Count | % | p | |||
| Neurological diseases | Cerebrovascular Disease | 134 | 109 | 81.3 | 17 | 12.7 | 8 | 6 | 1.000 |
| Amyotrophic Lateral Sclerosis | 13 | 9 | 69.2 | 3 | 23.1 | 1 | 7.7 | 1.000 | |
| Multiple Sclerosis—MS | 6 | 4 | 66.8 | 1 | 16.6 | 1 | 16.6 | 0.521 | |
| Parkinson’s Disease | 21 | 16 | 76.2 | 4 | 19.0 | 1 | 4.7 | 1.000 | |
| Cerebral Palsy | 5 | 4 | 80.0 | 1 | 20.0 | 0 | 0.0 | 1.000 | |
| Dementia | 116 | 100 | 86.2 | 10 | 8.6 | 6 | 5.2 | 0.555 | |
| Brain Tumour | 12 | 9 | 75.0 | 3 | 25.0 | 0 | 0.0 | 0.540 | |
| Reduced level of consciousness | Head Trauma | 13 | 11 | 84.6 | 1 | 7.7 | 1 | 7.7 | 0.521 |
| Intensive Care Patients | 78 | 67 | 85.9 | 7 | 9.0 | 4 | 5.1 | 0.730 | |
| Prolonged Coma | 34 | 30 | 88.2 | 3 | 8.9 | 1 | 2.9 | 1.000 | |
| Malignancy | Head and Neck Tumours | 9 | 9 | 100.0 | 0 | 0.0 | 0 | 0.0 | 1.000 |
| Nasopharyngeal Tumours | 18 | 14 | 77.8 | 3 | 16.7 | 1 | 5.5 | 1.000 | |
| Oesophageal Cancer | 3 | 2 | 66.7 | 1 | 33.0 | 0 | 0.0 | 1.000 | |
| Miscellaneous | 7 | 6 | 85.7 | 1 | 14.3 | 0 | 0.0 | 1.000 | |
| Others | Unclassified | 46 | 37 | 80.4 | 6 | 13.1 | 3 | 6.5 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arslan, R.S.; Koca, Y.S.; Sahin, S.T.; Beyoglu, R. Is Percutaneous Endoscopic Gastrostomy an Innocent Procedure? A Retrospective Single-Center Study. Medicina 2025, 61, 802. https://doi.org/10.3390/medicina61050802
Arslan RS, Koca YS, Sahin ST, Beyoglu R. Is Percutaneous Endoscopic Gastrostomy an Innocent Procedure? A Retrospective Single-Center Study. Medicina. 2025; 61(5):802. https://doi.org/10.3390/medicina61050802
Chicago/Turabian StyleArslan, Ramazan Serdar, Yavuz Savas Koca, Semra Tutcu Sahin, and Resad Beyoglu. 2025. "Is Percutaneous Endoscopic Gastrostomy an Innocent Procedure? A Retrospective Single-Center Study" Medicina 61, no. 5: 802. https://doi.org/10.3390/medicina61050802
APA StyleArslan, R. S., Koca, Y. S., Sahin, S. T., & Beyoglu, R. (2025). Is Percutaneous Endoscopic Gastrostomy an Innocent Procedure? A Retrospective Single-Center Study. Medicina, 61(5), 802. https://doi.org/10.3390/medicina61050802