
A Novel Hybrid Approach to Manage Mycotic Pseudoaneurysm Post-Renal Transplantation: Successful Graft Preservation

 , ,
, ,  , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Case Report
3. Discussion
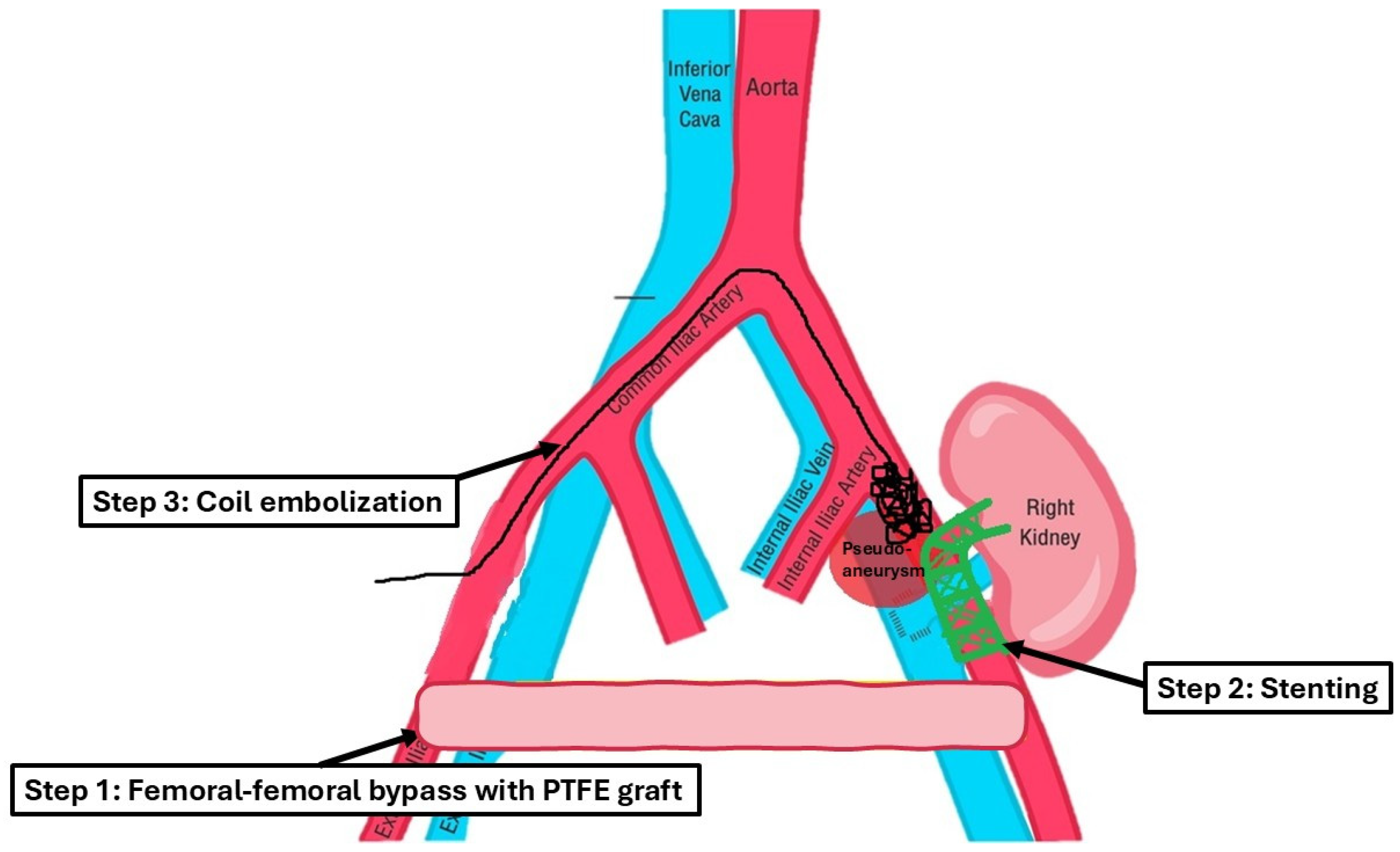
- Bypass grafting ensured continuous perfusion to the lower limb, mitigating the risk of ischemic complications;
- Endovascular stenting minimized surgical trauma while effectively excluding the pseudoaneurysm;
- Coil embolization provided an additional layer of pseudoaneurysm isolation, further enhancing treatment efficacy.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dimitroulis, D.; Bokos, J.; Zavos, G.; Nikiteas, N.; Karidis, N.P.; Katsaronis, P.; Kostakis, A. Vascular complications in renal transplantation: A single-center experience in 1367 renal transplantations and review of the literature. Transplant. Proc. 2009, 41, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Asztalos, L.; Olvasztó, S.; Fedor, R.; Szabó, L.; Balázs, G.; Lukács, G. Renal artery aneurysm at the anastomosis after kidney transplantation. Transplant. Proc. 2006, 38, 2915–2918. [Google Scholar] [CrossRef] [PubMed]
- Patrono, D.; Verhelst, R.; Buemi, A.; Darius, T.; Godefroid, N.; Mourad, M. Presentation and management of mycotic pseudoaneurysm after kidney transplantation. Transpl. Infect. Dis. 2015, 17, 129–136. [Google Scholar] [CrossRef]
- Anders, L.; Stephens, R.; Laub, M.; Amarath-Madav, R.; Mirza, A.; Saeed, M.I. Management of Transplant Renal Artery Pseudoaneurysm and Literature Review. Case Rep. Transplant. 2022, 2022, 6232586. [Google Scholar] [CrossRef]
- Peel, R.K.; Patel, J.; Woodrow, G. Iliac artery false aneurysm following renal allograft: Presentation with non-specific inflammatory response and treatment by endovascular stent graft. Nephrol. Dial. Transplant. 2003, 18, 1939–1940. [Google Scholar] [CrossRef]
- Bracale, U.M.; Santangelo, M.; Carbone, F.; Del Guercio, L.; Maurea, S.; Porcellini, M.; Bracale, G. Anastomotic pseudoaneurysm complicating renal transplantation: Treatment options. Eur. J. Vasc. Endovasc. Surg. 2010, 39, 565–568. [Google Scholar] [CrossRef]
- Cao, P.; Verzini, F.; Parlani, G.; Romano, L.; De Rango, P.; Pagliuca, V.; Iacono, G. Clinical effect of abdominal aortic aneurysm endografting: 7-year concurrent comparison with open repair. J. Vasc. Surg. 2004, 40, 841–848. [Google Scholar] [CrossRef]
- Zavos, G.; Pappas, P.; Kakisis, J.D.; Leonardou, P.; Manoli, E.; Bokos, J.; Kostakis, A. Endovascular repair as first-choice treatment of iliac pseudoaneurysms following renal transplantation. Transplant. Proc. 2005, 37, 4300–4302. [Google Scholar] [CrossRef]
- Kyriakides, G.K.; Simmons, R.L.; Najarian, J.S. Mycotic aneurysms in transplant patients. Arch. Surg. 1976, 111, 472–476. [Google Scholar] [CrossRef]
- Koo, C.K.; Rodger, S.; Baxter, G.M. Extra-renal pseudoaneurysm: An uncommon complication following renal transplantation. Clin. Radiol. 1999, 54, 755–758. [Google Scholar] [CrossRef]
- Battaglia, M.; Ditonno, P.; Fiore, T.; De Ceglie, G.; Regina, G.; Selvaggi, F.P. True mycotic arteritis by Candida albicans in 2 kidney transplant recipients from the same donor. J. Urol. 2000, 163, 1236–1237. [Google Scholar] [CrossRef] [PubMed]
- Garrido, J.; Lerma, J.L.; Heras, M.; Labrador, P.J.; García, P.; Bondía, A.; Corbacho, L.; Tabernero, J.M. Pseudoaneurysm of the iliac artery secondary to Aspergillus infection in two recipients of kidney transplants from the same donor. Am. J. Kidney Dis. 2003, 41, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Laouad, I.; Buchler, M.; Noel, C.; Sadek, T.; Maazouz, H.; Westeel, P.F.; Lebranchu, Y. Renal artery aneurysm secondary to Candida albicans in four kidney allograft recipients. Transplant. Proc. 2005, 37, 2834–2836. [Google Scholar] [CrossRef] [PubMed]
- Saidi, R.F.; Fasola, C.; El-Ghoroury, M.; Oh, H. Arterial anastomosis disrupton in two kidney recipients of contaminated grafts from a donor with Gorham’s syndrome. Transplant. Proc. 2004, 36, 1392–1394. [Google Scholar] [CrossRef]
- Eng, M.M.; Power, R.E.; Hickey, D.P.; Little, D.M. Vascular complications of allograft nephrectomy. Eur. J. Vasc. Endovasc. Surg. 2006, 32, 212–216. [Google Scholar] [CrossRef]
- Nguan, C.Y.; Luke, P.P. Renal artery pseudoaneurysm of infectious etiology: A life-threatening complication after renal transplantation. Urology 2006, 68, 668–669. [Google Scholar] [CrossRef]
- Orlando, G.; Di Cocco, P.; Gravante, G.; D’Angelo, M.; Famulari, A.; Pisani, F. Fatal hemorrhage in two renal graft recipients with multi-drug resistant Pseudomonas aeruginosa infection. Transpl. Infect. Dis. 2009, 11, 442–447. [Google Scholar] [CrossRef]
- Gravante, G.; Pisani, F.; D’Angelo, M.; Iaria, G.; Orlando, G. Renal artery aneurysms in kidney grafts. Am. J. Surg. 2008, 196, e46–e47. [Google Scholar] [CrossRef]
- Liu, K.Y.; Tsai, P.J.; King, K.L.; Chen, T.H.; Shyr, Y.M.; Su, C.H. Pseudoaneurysm of the iliac artery secondary to Aspergillus infection after kidney transplantation. J. Chin. Med. Assoc. 2009, 72, 654–656. [Google Scholar] [CrossRef]
- Osmán, I.; Barrero, R.; León, E.; Medina, R.; Torrubia, F. Mycotic pseudoaneurysm following a kidney transplant: A case report and review of the literature. Pediatr. Transplant. 2009, 13, 615–619. [Google Scholar] [CrossRef]
- Wang, R.; Wu, J.; Wang, Y.; Huang, H.; He, Q.; Chen, J. Aspergillus infection limited to the anastomosed artery following renal transplantation: A report of 4 cases. Transpl. Infect. Dis. 2009, 11, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Berglund, D.; Bergqvist, D.; Lundqvist, E.; Magnusson, A.; Sedigh, A.; Bäckman, L.; Biglarnia, A.R. Vascular reconstruction using allogeneic homografts in a renal transplant patient with pseudoaneurysm and infected vascular prosthesis. Transplantation 2012, 93, e15–e16. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.Z.; Jones, A.; Sideso, E.; Sinha, S.; Vaidya, A.; Darby, C. Management of a ruptured mycotic pseudo-aneurysm following pancreas-kidney transplantation. Ann. Transplant. 2011, 16, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Kao, Y.C.; Chan, W.P. Pseudoaneurysm with candidal infection after renal transplantation. Intern. Med. 2011, 50, 2679–2680. [Google Scholar] [CrossRef]
- Minz, M.; Sharma, A.; Kumar, S.; Singh, S.; Shivaprakash, M.R.; Bag, S. Use of autogenous internal iliac artery for bridging the external iliac artery after excision of Aspergillus mycotic aneurysm in renal transplant recipients. J. Vasc. Surg. 2011, 53, 802–804. [Google Scholar] [CrossRef]
- Polat, K.Y.; Aydinli, B.; Keles, M.; Uyanik, A.; Ozturk, G.; Ceviz, M.; Gundogdu, C.; Kantarci, M. Spontaneous mycotic external iliac artery aneurysm rupture after perforated acute appendicitis in a renal allograft recipient. Exp. Clin. Transplant. 2011, 9, 211–213. [Google Scholar]
- Kountidou, C.S.; Stier, K.; Niehues, S.M.; Lingnau, A.; Schostak, M.; Fuller, T.F.; Lützenberg, R. Successful repair of post-transplant mycotic aneurysm of iliac artery with renal graft preservation: A case report. Urology 2012, 80, 1151–1153. [Google Scholar] [CrossRef]
- Leonardou, P.; Gioldasi, S.; Zavos, G.; Pappas, P. Mycotic pseudoaneurysms complicating renal transplantation: A case series and review of literature. J. Med. Case Rep. 2012, 6, 59. [Google Scholar] [CrossRef]
- Santangelo, M.L.; Bracale, U.M.; Carlomagno, N.; De Rosa, D.; Spiezia, S.; Scotti, A.; Tammaro, V.; Porcellini, M.; Renda, A. Kidney transplantation and large anastomotic pseudoaneurysm. Transplant management considerations. Ann. Ital. Chir. 2013, 84, 275–279. [Google Scholar]
- Chandak, P.; Kessaris, N.; Uwechue, R.U.; Abboudi, H.; Hossain, M.; Harris, F.; Jones, K.; Fronek, J. Successful excision of a suspected mycotic transplant renal artery patch aneurysm with renal allograft autotransplantation. Transplantation 2014, 97, e25–e26. [Google Scholar] [CrossRef]
- Dębska-Ślizień, A.; Chrobak, Ł.; Bzoma, B.; Perkowska, A.; Zadrożny, D.; Chamienia, A.; Kostro, J.; Milecka, A.; Bronk, M.; Śledziński, Z.; et al. Candida arteritis in kidney transplant recipients: Case report and review of the literature. Transpl. Infect. Dis. 2015, 17, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Madhav, D.; Kumar, P.; Mohan, C.; Mahesh, U. Candida-associated pseudo-aneurysm of the transplant renal artery presenting as malignant hypertension and managed successfully without nephrectomy. Saudi J. Kidney Dis. Transpl. 2015, 26, 1000–1005. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.D.; Huang, Z.Y.; Hong, L.Q.; Liao, T.; Tang, Y.E.; Na, N.; Li, H.; Miao, B.; Hua, X.F.; Sun, Q.Q. Massive hemorrhage caused by fungal infections after donation-after-cardiac-death kidney transplantation: Clinical features, prevention and treatment experience. Zhonghua Yi Xue Za Zhi 2016, 96, 1570–1572. [Google Scholar] [PubMed]
- Fananapazir, G.; Hannsun, G.; Wright, L.A.; Corwin, M.T.; Troppmann, C. Diagnosis and Management of Transplanted Kidney Extrarenal Pseudoaneurysms: A Series of Four Cases and a Review of the Literature. Cardiovasc. Interv. Radiol. 2016, 39, 1649–1653. [Google Scholar] [CrossRef]
- Berger, M.F.; Badell, I.R. Single Donor-Derived Pseudomonas aeruginosa Pseudoaneurysms in Two Kidney Transplant Recipients: A Case Report of Dichotomous Allograft Outcomes. Transplant. Proc. 2017, 49, 2357–2361. [Google Scholar] [CrossRef]
- Chung, M.M.; Chan, Y.C.; Law, Y.; Cheng, S.W. Infectious anastomotic pseudoaneurysm complicating renal allograft: Case report and review of literature. Int. J. Nephrol. Renov. Dis. 2017, 10, 55–60. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Liao, C.-H.; Jiang, B.-J.; Chen, T.-H. Early renal arterial rupture and arterial pseudoaneurysm in graft kidneys from the same deceased donor. Tzu Chi Med. J. 2018, 30, 250–254. [Google Scholar]
- Ministro, A.; Ferreira, T.; Batista, L.; Santana, A.; Alves, N.; Guerra, J.; Fernandes, E.F.J. Mycotic Pseudoaneurysm After Kidney Transplantation: Two Case Reports. Transplant. Proc. 2017, 49, 906–912. [Google Scholar] [CrossRef]
- Liu, G.; Wang, X.; Wu, J.; Peng, W.; Wang, R.; Huang, H.; Chen, J. Successful repair of kidney graft artery rupture secondary to infection using a preprocessed homologous “Y”-shaped iliac artery. Clin. Transplant. 2019, 33, e13493. [Google Scholar] [CrossRef]
- Liu, X.L.; Zu, Q.Q.; Wang, B.; Zhou, C.G.; Zhao, L.B.; Xia, J.G.; Gu, M.; Shi, H.B.; Liu, S. Minimally invasive salvage therapy for transplanted renal allografts. Ren. Fail. 2015, 37, 1470–1475. [Google Scholar] [CrossRef]
- Khalil, M.A.M.; Sadagah, N.M.; Alqurashi, M.M.; Basha, A.A.; Sakran, H.I.M.; Assiri, I.M.N.; Aboalsamh, G.A.; Al-Qurashi, S.H. A Rare Case of Gas Forming Enterobacter cloacae Leading to Bleeding Mycotic Pseudoaneurysm of Transplant Renal Artery Culminating in Graft Nephrectomy. J. Med. Cases 2024, 15, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Horn, A.; Summers, K.L.; Fuell, W.; Vijay, A.; Jeon, H.; Donovan, M.; Tulla, K.; Paramesh, A. Salvage of a kidney transplant with a mycotic extrarenal pseudoaneursym using donor vessels. Ann. Vasc. Surg.-Brief Rep. Innov. 2024, 4, 100314. [Google Scholar] [CrossRef]
- Poels, J.A.; Riley, P.L. Extrarenal transplant artery pseudoaneurysm: A combined therapeutic approach. Cardiovasc. Interv. Radiol. 2008, 31, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Che, H.; Men, C.; Yang, M.; Zhang, J.; Chen, P.; Yong, J. Endovascular repair of a transplant renal artery anastomotic pseudoaneurysm using the snorkel technique. J. Vasc. Surg. 2014, 60, 1052–1055. [Google Scholar] [CrossRef]
- Patil, V.V.; Roytman, M.; Ames, S.; Beckerman, W.; Lookstein, R.A. Endovascular Repair of Renal Artery Anastomotic Pseudoaneurysm Following Living Donor Kidney Transplant. Cardiovasc. Interv. Radiol. 2015, 38, 1640–1644. [Google Scholar] [CrossRef]
- Hassanein, W.; Schweitzer, E.; Toursavadkohi, S.; Nagarsheth, K. Totally percutaneous endovascular renal allograft salvage for common iliac artery pseudoaneurysm. J. Vasc. Surg. Cases Innov. Tech. 2024, 10, 101485. [Google Scholar] [CrossRef]
- Yeh, C.C.; Khan, A.; Muo, C.H.; Yang, H.R.; Li, P.C.; Chang, C.H.; Chen, T.L.; Jeng, L.B.; Liao, C.C. De Novo Malignancy After Heart, Kidney, and Liver Transplant: A Nationwide Study in Taiwan. Exp. Clin. Transplant. 2020, 18, 224–233. [Google Scholar] [CrossRef]
- Malik, M.S.; Akoh, J.A.; Houlberg, K.; Barwell, J.; Powell, R. Iliofemoral Polytetrafluoroethylene Graft Interposition: A Rescue Procedure in External Iliac Artery Dissection to Restore Lower Limb Revascularization and Salvage Kidney Transplant. Exp. Clin. Transplant. 2023, 21, 467–470. [Google Scholar] [CrossRef]
- Verloh, N.; Doppler, M.; Hagar, M.T.; Kulka, C.; von Krüchten, R.; Neubauer, J.; Weiß, J.; Röthele, E.; Schneider, J.; Jänigen, B.; et al. Interventional Management of Vascular Complications after Renal Transplantation. Rofo 2023, 195, 495–504. [Google Scholar] [CrossRef]
- Buimer, M.G.; van Hamersvelt, H.W.; Adam van der Vliet, J. Anastomotic pseudoaneurysm after renal transplantation; a new hybrid approach with graft salvage. Transpl. Int. 2012, 25, e86–e88. [Google Scholar] [CrossRef]
- Kaabak, M.; Babenko, N.; Zokoev, A.; Morozova, M.; Platova, E.; Zverev, D.; Dzhamanchin, D.; Novozhilova, T.; Kozlov, S. Successful repair of kidney graft artery rupture using external stenting. Transplantation 2013, 95, e48–e49. [Google Scholar] [CrossRef] [PubMed]
- Kwon Koo, B.; Shim, W.H.; Yoon, Y.S.; Kwon Lee, B.; Choi, D.; Jang, Y.; Lee, D.Y.; Chang, B.C. Endovascular therapy combined with immunosuppressive treatment for pseudoaneurysms in patients with Behçet’s disease. J. Endovasc. Ther. 2003, 10, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Sanada, J.; Matsui, O.; Arakawa, F.; Tawara, M.; Endo, T.; Ito, H.; Ushijima, S.; Endo, M.; Ikeda, M.; Miyazu, K. Endovascular stent-grafting for infected iliac artery pseudoaneurysms. Cardiovasc. Interv. Radiol. 2005, 28, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Berchtold, C.; Eibl, C.; Seelig, M.H.; Jakob, P.; Schönleben, K. Endovascular treatment and complete regression of an infected abdominal aortic aneurysm. J. Endovasc. Ther. 2002, 9, 543–548. [Google Scholar] [CrossRef]
- Ting, A.C.W.; Cheng, S.W.K.; Ho, P.; Poon, J.T.C. Endovascular stent graft repair for infected thoracic aortic pseudoaneurysms—A durable option? J. Vasc. Surg. 2006, 44, 701–705. [Google Scholar] [CrossRef]
- Keeling, A.N.; Naughton, P.A.; McGrath, F.P.; Conlon, P.J.; Lee, M.J. Successful endovascular treatment of a hemodialysis graft pseudoaneurysm by covered stent and direct percutaneous thrombin injection. Semin. Dial. 2008, 21, 553–556. [Google Scholar] [CrossRef]
- Ting, A.C.W.; Cheng, S.W.K.; Ho, P.; Poon, J.T.C.; Tsu, J.H.L. Surgical treatment of infected aneurysms and pseudoaneurysms of the thoracic and abdominal aorta. Am. J. Surg. 2005, 189, 150–154. [Google Scholar] [CrossRef]
- Kim, W.H.; Choi, D.; Kim, J.S.; Ko, Y.G.; Jang, Y.; Shim, W.H. Effectiveness and safety of endovascular aneurysm treatment in patients with vasculo-Behçet disease. J. Endovasc. Ther. 2009, 16, 631–636. [Google Scholar] [CrossRef]
- Kim, S.H.; Kwon, O.K.; Jung, C.K.; Kang, H.S.; Oh, C.W.; Han, M.H.; Kim, Y.S.; Baik, S.K. Endovascular treatment of ruptured aneurysms or pseudoaneurysms on the collateral vessels in patients with moyamoya disease. Neurosurgery 2009, 65, 1000–1004; discussion 1004. [Google Scholar] [CrossRef]
- Granata, A.; Clementi, S.; Londrino, F.; Romano, G.; Veroux, M.; Fiorini, F.; Fatuzzo, P. Renal transplant vascular complications: The role of Doppler ultrasound. J. Ultrasound 2015, 18, 101–107. [Google Scholar] [CrossRef]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed Graft Function in the Kidney Transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | Author | Year | Number/Treatment | Outcome |
|---|---|---|---|---|
| Open surgery (Including transplantectomy) | Kyriakides [9] | 1976 | 8/Tx 1/SR | 2/death 6/graft loss |
| Koo [10] | 1999 | 1/Tx | 1/graft loss | |
| Battaglia [11] | 2000 | 2/Tx | 2/graft loss | |
| Garrido [12,13] | 2003 | 2/Tx | 1/death 1/graft loss | |
| Saidi [14] | 2004 | 2/Tx | 2/graft loss | |
| Laouad [10,13] | 2005 | 4/Tx | 1/death 3/graft loss | |
| Zavos [8] | 2005 | 2/Tx | 2/graft loss | |
| Eng [14,15] | 2006 | 4/Tx | 4/graft loss 2/death | |
| Nguan [15,16] | 2006 | 1/Tx | 1/graft loss | |
| Orlando [17,18] | 2009 | 2/Tx | 2/death | |
| Liu [19] | 2009 | 1/Tx | 1/graft loss | |
| Osman [20] | 2009 | 1/EVS and Tx | 1/graft loss | |
| Wang [21] | 2009 | 4/Tx | 4/graft loss | |
| Bracale [6] | 2009 | 8/Tx 3/EVS and Tx 1/SR and replantation | 8/graft loss 3/death after OP 1/graft preserved | |
| Bozkurt | 2010 | 2/Tx | 2/graft loss | |
| Berglund [22] | 2011 | 1/SR | 1/graft preserved | |
| Akhtar [23] | 2011 | 1/Tx | 1/graft loss | |
| Lee [24] | 2011 | 1/Tx | 1/graft loss | |
| Minz [25] | 2011 | 2/Tx | 1/death 1/graft loss | |
| Polat [26] | 2011 | 1/Tx | 1/graft loss | |
| Kountidou [27] | 2012 | 1/SR | 1/graft preserved | |
| Leonardou [28] | 2012 | 4/EVS and Tx | 4 graft loss | |
| Santangelo [29] | 2013 | 1/SR and replantation 4/Tx 1/EVS and Tx | 5/graft loss 1/graft preserved | |
| Chandak [30] | 2014 | 1/SR | 1/graft preserved | |
| Debska-Slizien [31] | 2015 | 2/Tx | 2/death after OP | |
| Madhav [32] | 2015 | 1/SR | 1/graft preserved | |
| Patrono [3] | 2015 | 2/Tx 1/SR | 2/graft loss 1/graft preserved | |
| Zhao [33] | 2016 | 2/EVS and Tx | 2/graft loss | |
| Fananapazir [34] | 2016 | 3/Tx | 3/graft loss | |
| Berger [35] | 2017 | 1/Tx | 1/graft loss | |
| Chung [36] | 2017 | 1/Tx | 1/graft loss | |
| Lin [37] | 2017 | 1/Tx 1/SR | 1/graft loss 1/graft preserved | |
| Ministro [38] | 2017 | 2/SR | 2/graft preserved | |
| Liu [39,40] | 2018 | 5/SR | 5/graft preserved | |
| Khalil [41] | 2024 | 1/Tx | 1/graft loss | |
| Horn [42] | 2024 | 1/SR | 1/graft preserved | |
| Endovascular repair | Koo [10] | 1999 | 1/EVC | 1/graft preserved |
| Peel [5] | 2003 | 1/EVC | 1/graft preserved | |
| Poels [43] | 2007 | 1/EVS + thrombin | 1/graft preserved | |
| Berger [35] | 2017 | 1/EVS | 1/graft preserved | |
| Che [44] | 2014 | 1/EVS | 1/graft preserved | |
| Patil [45] | 2015 | 1/EVS | 1/graft preserved | |
| Fananapazir [34] | 2016 | 1/EVC | 1/graft preserved | |
| Hassanein [46] | 2024 | 1/EVS | 1/graft preserved |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Lin, Y.-C.; Kao, C.-C.; Chiang, P.-J.; Chou, M.-H.; Ting, H.-K.; Jhuo, Y.-C.; Yang, M.-H.; Tsao, C.-W.; Meng, E.; et al. A Novel Hybrid Approach to Manage Mycotic Pseudoaneurysm Post-Renal Transplantation: Successful Graft Preservation. Medicina 2025, 61, 521. https://doi.org/10.3390/medicina61030521
Li H, Lin Y-C, Kao C-C, Chiang P-J, Chou M-H, Ting H-K, Jhuo Y-C, Yang M-H, Tsao C-W, Meng E, et al. A Novel Hybrid Approach to Manage Mycotic Pseudoaneurysm Post-Renal Transplantation: Successful Graft Preservation. Medicina. 2025; 61(3):521. https://doi.org/10.3390/medicina61030521
Chicago/Turabian StyleLi, Ho, Yi-Chang Lin, Chien-Chang Kao, Pei-Jhang Chiang, Meng-Han Chou, Hui-Kung Ting, Yu-Cing Jhuo, Ming-Hsin Yang, Chih-Wei Tsao, En Meng, and et al. 2025. "A Novel Hybrid Approach to Manage Mycotic Pseudoaneurysm Post-Renal Transplantation: Successful Graft Preservation" Medicina 61, no. 3: 521. https://doi.org/10.3390/medicina61030521
APA StyleLi, H., Lin, Y.-C., Kao, C.-C., Chiang, P.-J., Chou, M.-H., Ting, H.-K., Jhuo, Y.-C., Yang, M.-H., Tsao, C.-W., Meng, E., Sun, G.-H., Yu, D.-S., Chang, S.-Y., Chen, C.-L., & Wu, S.-T. (2025). A Novel Hybrid Approach to Manage Mycotic Pseudoaneurysm Post-Renal Transplantation: Successful Graft Preservation. Medicina, 61(3), 521. https://doi.org/10.3390/medicina61030521