

ACE I/D Genotype and Risk of Non-Contact Injury in Moroccan Elite Athletes: A Pilot Study

 ,
,  , ,
, ,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design and Participants
2.3. Injury Collection
2.4. Genotyping
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (Soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Delecroix, B.; McCall, A.; Dawson, B.; Berthoin, S.; Dupont, G. Workload and Non-Contact Injury Incidence in Elite Football Players Competing in European Leagues. Eur. J. Sport Sci. 2018, 18, 1280–1287. [Google Scholar] [CrossRef]
- McCall, A.; Dupont, G.; Ekstrand, J. Internal Workload and Non-Contact Injury: A One-Season Study of Five Teams from the UEFA Elite Club Injury Study. Br. J. Sports Med. 2018, 52, 1517–1522. [Google Scholar] [CrossRef] [PubMed]
- Chia, L.; De Oliveira Silva, D.; Whalan, M.; McKay, M.J.; Sullivan, J.; Fuller, C.W.; Pappas, E. Non-Contact Anterior Cruciate Ligament Injury Epidemiology in Team-Ball Sports: A Systematic Review with Meta-Analysis by Sex, Age, Sport, Participation Level, and Exposure Type. Sports Med. 2022, 52, 2447–2467. [Google Scholar] [CrossRef] [PubMed]
- Sonkodi, B.; Bardoni, R.; Poór, G. Osteoporosis in Light of a New Mechanism Theory of Delayed Onset Muscle Soreness and Non-Contact Anterior Cruciate Ligament Injury. Int. J. Mol. Sci. 2022, 23, 9046. [Google Scholar] [CrossRef]
- Khoshnoodi, P.; Tehranzadeh, A.D.; Dunn, J.M.; Tehranzadeh, J. Semimembranosus Tendon Avulsion Fracture of the Posteromedial Tibial Plateau Associated with Posterior Cruciate Ligament Tear and Capsular Rupture. Skelet. Radiol. 2014, 43, 239–242. [Google Scholar] [CrossRef]
- Prien, A.; Feddermann-Demont, N.; Verhagen, E.; Twisk, J.; Junge, A. Neurocognitive Performance and Mental Health of Retired Female Football Players Compared to Non-Contact Sport Athletes. BMJ Open Sport Exerc. Med. 2020, 6, e000952. [Google Scholar] [CrossRef]
- Bezuglov, E.; Talibov, O.; Butovskiy, M.; Lyubushkina, A.; Khaitin, V.; Lazarev, A.; Achkasov, E.; Waśkiewicz, Z.; Rosemann, T.; Nikolaidis, P.T.; et al. The Prevalence of Non-Contact Muscle Injuries of the Lower Limb in Professional Soccer Players Who Perform Salah Regularly: A Retrospective Cohort Study. J. Orthop. Surg. Res. 2020, 15, 440. [Google Scholar] [CrossRef]
- Edouard, P.; Navarro, L.; Branco, P.; Gremeaux, V.; Timpka, T.; Junge, A. Injury Frequency and Characteristics (Location, Type, Cause and Severity) Differed Significantly among Athletics (‘track and Field’) Disciplines during 14 International Championships (2007–2018): Implications for Medical Service Planning. Br. J. Sports Med. 2020, 54, 159–167. [Google Scholar] [CrossRef]
- Myerson, S.; Hemingway, H.; Budget, R.; Martin, J.; Humphries, S.; Montgomery, H. Human Angiotensin I-Converting Enzyme Gene and Endurance Performance. J. Appl. Physiol. 1999, 87, 1313–1316. [Google Scholar] [CrossRef]
- Lindpaintner, K.; Pfeffer, M.A.; Kreutz, R.; Stampfer, M.J.; Grodstein, F.; LaMotte, F.; Buring, J.; Hennekens, C.H. A Prospective Evaluation of an Angiotensin-Converting-Enzyme Gene Polymorphism and the Risk of Ischemic Heart Disease. N. Engl. J. Med. 1995, 332, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.; Kiely, J.; Suraci, B.; Collins, D.J.; de Lorenzo, D.; Pickering, C.; Grimaldi, K.A. A Genetic-Based Algorithm for Personalized Resistance Training. Biol. Sport 2016, 33, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Ahmetov, I.I.; Hall, E.C.R.; Semenova, E.A.; Pranckevičienė, E.; Ginevičienė, V. Chapter Five—Advances in Sports Genomics. In Advances in Clinical Chemistry; Makowski, G.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2022; Volume 107, pp. 215–263. [Google Scholar] [CrossRef]
- McCall, A.; Carling, C.; Nedelec, M.; Davison, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Risk Factors, Testing and Preventative Strategies for Non-Contact Injuries in Professional Football: Current Perceptions and Practices of 44 Teams from Various Premier Leagues. Br. J. Sports Med. 2014, 48, 1352–1357. [Google Scholar] [CrossRef] [PubMed]
- Coelho, D.B.; Pimenta, E.M.; Rosse, I.C.; Veneroso, C.; Pussieldi, G.D.A.; Becker, L.K.; Oliveira, E.C.; Carvalho, M.R.S.; Silami-Garcia, E. Alpha-Actinin-3 R577x Polymorphism Influences Muscle Damage and Hormonal Responses After a Soccer Game. J. Strength Cond. Res. 2019, 33, 2655–2664. [Google Scholar] [CrossRef]
- Massidda, M.; Bachis, V.; Corrias, L.; Piras, F.; Scorcu, M.; Culigioni, C.; Masala, D.; Calò, C.M. ACTN3 R577X Polymorphism Is Not Associated with Team Sport Athletic Status in Italians. Sports Med. Open 2015, 1, 6. [Google Scholar] [CrossRef]
- Massidda, M.; Myamoto-Mikami, E.; Kumagai, H.; Ikeda, H.; Shimasaki, Y.; Yoshimura, M.; Cugia, P.; Piras, F.; Scorcu, M.; Kikuchi, N.; et al. Association between the ACE I/D Polymorphism and Muscle Injuries in Italian and Japanese Elite Football Players. J. Sports Sci. 2020, 38, 2423–2429. [Google Scholar] [CrossRef]
- Kumagai, H.; Miyamoto-Mikami, E.; Hirata, K.; Kikuchi, N.; Kamiya, N.; Hoshikawa, S.; Zempo, H.; Naito, H.; Miyamoto, N.; Fuku, N. ESR1 Rs2234693 Polymorphism Is Associated with Muscle Injury and Muscle Stiffness. Med. Sci. Sports Exerc. 2019, 51, 19–26. [Google Scholar] [CrossRef]
- Montgomery, H.E.; Clarkson, P.; Dollery, C.M.; Prasad, K.; Losi, M.A.; Hemingway, H.; Statters, D.; Jubb, M.; Girvain, M.; Varnava, A.; et al. Association of Angiotensin-Converting Enzyme Gene I/D Polymorphism with Change in Left Ventricular Mass in Response to Physical Training. Circulation 1997, 96, 741–747. [Google Scholar] [CrossRef]
- Juffer, P.; Furrer, R.; González-Freire, M.; Santiago, C.; Verde, Z.; Serratosa, L.; Morate, F.J.; Rubio, J.C.; Martin, M.A.; Ruiz, J.R.; et al. Genotype Distributions in Top-Level Soccer Players: A Role for ACE? Int. J. Sports Med. 2009, 30, 387–392. [Google Scholar] [CrossRef]
- Chen, Y.J.; Li, L.J.; Tang, W.L.; Song, J.Y.; Qiu, R.; Li, Q.; Xue, H.; Wright, J.M. First-Line Drugs Inhibiting the Renin Angiotensin System versus Other First-Line Antihypertensive Drug Classes for Hypertension. Cochrane Database Syst. Rev. 2018, 11, CD008170. [Google Scholar] [CrossRef]
- Simonyte, S.; Kuciene, R.; Medzioniene, J.; Dulskiene, V.; Lesauskaite, V. Renin-Angiotensin System Gene Polymorphisms and High Blood Pressure in Lithuanian Children and Adolescents. BMC Med. Genet. 2017, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Danser, A.H.; Schalekamp, M.A.; Bax, W.A.; van den Brink, A.M.; Saxena, P.R.; Riegger, G.A.; Schunkert, H. Angiotensin-Converting Enzyme in the Human Heart. Eff. Deletion Inser. Polymorphism. Circ. 1995, 92, 1387–1388. [Google Scholar] [CrossRef] [PubMed]
- Rigat, B.; Hubert, C.; Alhenc-Gelas, F.; Cambien, F.; Corvol, P.; Soubrier, F. An Insertion/Deletion Polymorphism in the Angiotensin I-Converting Enzyme Gene Accounting for Half the Variance of Serum Enzyme Levels. J. Clin. Investig. 1990, 86, 1343–1346. [Google Scholar] [CrossRef] [PubMed]
- Sayed-Tabatabaei, F.A.; Oostra, B.A.; Isaacs, A.; van Duijn, C.M.; Witteman, J.C.M. ACE Polymorphisms. Circ. Res. 2006, 98, 1123–1133. [Google Scholar] [CrossRef]
- Jones, A.; Woods, D.R. Skeletal Muscle RAS and Exercise Performance. Int. J. Biochem. Cell Biol. 2003, 35, 855–866. [Google Scholar] [CrossRef]
- Zhang, B.; Tanaka, H.; Shono, N.; Miura, S.; Kiyonaga, A.; Shindo, M.; Saku, K. The I Allele of the Angiotensin-Converting Enzyme Gene Is Associated with an Increased Percentage of Slow-Twitch Type I Fibers in Human Skeletal Muscle. Clin. Genet. 2003, 63, 139–144. [Google Scholar] [CrossRef]
- Ma, F.; Yang, Y.; Li, X.; Zhou, F.; Gao, C.; Li, M.; Gao, L. The Association of Sport Performance with ACE and ACTN3 Genetic Polymorphisms: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e54685. [Google Scholar] [CrossRef]
- Fluck, M.; Kramer, M.; Fitze, D.; Kasper, S.; Franchi, M.; Valdivieso, P. Cellular Aspects of Muscle Specialization Demonstrate Genotype—Phenotype Interaction Effects in Athletes. Front. Physiol. 2019, 10, 526. [Google Scholar] [CrossRef]
- Vaughan, D.; Brogioli, M.; Maier, T.; White, A.; Waldron, S.; Rittweger, J.; Toigo, M.; Wettstein, J.; Laczko, E.; Flück, M. The Angiotensin Converting Enzyme Insertion/Deletion Polymorphism Modifies Exercise-Induced Muscle Metabolism. PLoS ONE 2016, 11, e0149046. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Kostek, M.A.; Gordish-Dressman, H.; Thompson, P.D.; Seip, R.L.; Price, T.B.; Angelopoulos, T.J.; Clarkson, P.M.; Gordon, P.M.; Moyna, N.M.; et al. ACE ID Genotype and the Muscle Strength and Size Response to Unilateral Resistance Training. Med. Sci. Sports Exerc. 2006, 38, 1074–1081. [Google Scholar] [CrossRef]
- Charbonneau, D.E.; Hanson, E.D.; Ludlow, A.T.; Delmonico, M.J.; Hurley, B.F.; Roth, S.M. ACE Genotype and the Muscle Hypertrophic and Strength Responses to Strength Training. Med. Sci. Sports Exerc. 2008, 40, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-J.; Kim, C.-H.; Park, D.-S.; Choi, S.-Y.; Lee, D.-H.; Nam, H.-S.; Hur, J.-G.; Woo, J.-H. The Impacts of ACE Activity According to ACE I/D Polymorphisms on Muscular Functions of People Aged 65. Ann. Rehabil. Med. 2012, 36, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Baumert, P.; Lake, M.J.; Stewart, C.E.; Drust, B.; Erskine, R.M. Genetic Variation and Exercise-Induced Muscle Damage: Implications for Athletic Performance, Injury and Ageing. Eur. J. Appl. Physiol. 2016, 116, 1595–1625. [Google Scholar] [CrossRef] [PubMed]
- Yamin, C.; Amir, O.; Sagiv, M.; Attias, E.; Meckel, Y.; Eynon, N.; Sagiv, M.; Amir, R.E. ACE ID Genotype Affects Blood Creatine Kinase Response to Eccentric Exercise. J. Appl. Physiol. 2007, 103, 2057–2061. [Google Scholar] [CrossRef]
- Del Coso, J.; Salinero, J.J.; Lara, B.; Gallo-Salazar, C.; Areces, F.; Herrero, D.; Puente, C. Polygenic Profile and Exercise-Induced Muscle Damage by a Competitive Half-Ironman. J. Strength Cond. Res. 2020, 34, 1400. [Google Scholar] [CrossRef]
- Del Coso, J.; Valero, M.; Salinero, J.J.; Lara, B.; Gallo-Salazar, C.; Areces, F. Optimum Polygenic Profile to Resist Exertional Rhabdomyolysis during a Marathon. PLoS ONE 2017, 12, e0172965. [Google Scholar] [CrossRef]
- Sierra, A.P.R.; Lima, G.H.O.; da Silva, E.D.; de Souza Maciel, J.F.; Benetti, M.P.; de Oliveira, R.A.; de Oliveira Martins, P.F.; Kiss, M.A.P.; Ghorayeb, N.; Newsholme, P.; et al. Angiotensin-Converting Enzyme Related-Polymorphisms on Inflammation, Muscle and Myocardial Damage After a Marathon Race. Front. Genet. 2019, 10, 984. [Google Scholar] [CrossRef]
- Tanisawa, K.; Wang, G.; Seto, J.; Verdouka, I.; Twycross-Lewis, R.; Karanikolou, A.; Tanaka, M.; Borjesson, M.; Di Luigi, L.; Dohi, M.; et al. Sport and Exercise Genomics: The FIMS 2019 Consensus Statement Update. Br. J. Sports Med. 2020, 54, 969–975. [Google Scholar] [CrossRef]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee Consensus Statement: Methods for Recording and Reporting of Epidemiological Data on Injury and Illness in Sport 2020 (Including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef]
- Clarsen, B.; Pluim, B.M.; Moreno-Pérez, V.; Bigard, X.; Blauwet, C.; Del Coso, J.; Courel-Ibáñez, J.; Grimm, K.; Jones, N.; Kolman, N.; et al. Methods for Epidemiological Studies in Competitive Cycling: An Extension of the IOC Consensus Statement on Methods for Recording and Reporting of Epidemiological Data on Injury and Illness in Sport 2020. Br. J. Sports Med. 2021, 55, 1262–1269. [Google Scholar] [CrossRef]
- Chiu, Y.-H.; Lai, J.-I.; Tseng, C.-Y.; Wang, S.-H.; Li, L.-H.; Kao, W.-F.; How, C.-K.; Chang, W.-H.; Hsieh, C.-Y. Impact of Angiotension I Converting Enzyme Gene I/D Polymorphism on Running Performance, Lipid, and Biochemical Parameters in Ultra-Marathoners. Medicine 2019, 98, e16476. [Google Scholar] [CrossRef] [PubMed]
- Rigat, B.; Hubert, C.; Corvol, P.; Soubrier, R. PCR Detection of the Insertion/Deletion Polymorphism of the Human Angiotensin Converting Enzyme Gene (DCP1) (Dipeptidyl Carboxypeptidase 1). Nucleic Acids Res. 1992, 20, 1433. [Google Scholar] [CrossRef] [PubMed]
- Lim, T.; Santiago, C.; Pareja-Galeano, H.; Iturriaga, T.; Sosa-Pedreschi, A.; Fuku, N.; Pérez-Ruiz, M.; Yvert, T. Genetic Variations Associated with Non-Contact Muscle Injuries in Sport: A Systematic Review. Scand. J. Med. Sci. Sports 2021, 31, 2014–2032. [Google Scholar] [CrossRef]
- Larruskain, J.; Celorrio, D.; Barrio, I.; Odriozola, A.; Gil, S.M.; Fernandez-Lopez, J.R.; Nozal, R.; Ortuzar, I.; Lekue, J.A.; Aznar, J.M. Genetic Variants and Hamstring Injury in Soccer: An Association and Validation Study. Med. Sci. Sports Exerc. 2018, 50, 361–368. [Google Scholar] [CrossRef]
- Varillas-Delgado, D.; Gutierrez-Hellín, J.; Maestro, A. Genetic Profile in Genes Associated with Sports Injuries in Elite Endurance Athletes. Int. J. Sports Med. 2023, 44, 64–71. [Google Scholar] [CrossRef]
- Onori, M.E.; Pasqualetti, M.; Moretti, G.; Canu, G.; De Paolis, G.; Baroni, S.; Minucci, A.; Galvani, C.; Urbani, A. Genetics and Sport Injuries: New Perspectives for Athletic Excellence in an Italian Court of Rugby Union Players. Genes 2022, 13, 995. [Google Scholar] [CrossRef]
- de Almeida, K.Y.; Cetolin, T.; Marrero, A.R.; Aguiar Junior, A.S.; Mohr, P.; Kikuchi, N. A Pilot Study on the Prediction of Non-Contact Muscle Injuries Based on ACTN3 R577X and ACE I/D Polymorphisms in Professional Soccer Athletes. Genes 2022, 13, 2009. [Google Scholar] [CrossRef]
- Moreno-Perez, V.; Campos-Vazquez, M.A.; Toscano, J.; Sotos-Martinez, V.J.; López-Del Campo, R.; Resta, R.; Del Coso, J. Influence of the Weekly and Match-Play Load on Muscle Injury in Professional Football Players. Int. J. Sports Med. 2022, 43, 783–790. [Google Scholar] [CrossRef]
- Tanabe, Y.; Fujii, N.; Suzuki, K. Dietary Supplementation for Attenuating Exercise-Induced Muscle Damage and Delayed-Onset Muscle Soreness in Humans. Nutrients 2021, 14, 70. [Google Scholar] [CrossRef]
- Massidda, M.; Scorcu, M.; Calo, C. New Genetic Model for Predicting Phenotype Traits in Sports. Int. J. Sports Physiol. Perform. 2014, 9, 554–560. [Google Scholar] [CrossRef]
- Hughes, D.C.; Day, S.H.; Ahmetov, I.I.; Williams, A.G. Genetics of Muscle Strength and Power: Polygenic Profile Similarity Limits Skeletal Muscle Performance. J. Sports Sci. 2011, 29, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.G.; Folland, J.P. Similarity of Polygenic Profiles Limits the Potential for Elite Human Physical Performance. J. Physiol. 2008, 586, 113–121. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| All Athletes | Injury | No Injury | p-Value | |
|---|---|---|---|---|
| Age (yr) | 20 (18–23) | 21.83 ± 3.86 | 20 (18–23) | 0.80 |
| Weight (kg) | 64.30 ± 6.23 | 65.83 ± 4.59 | 64 (60–67) | 0.22 |
| Height (m) | 1.77 ± 0.05 | 1.78 ± 0.04 | 1.76 ± 0.05 | 0.65 |
| BMI (kg/m2) | 20.64 ± 1.93 | 20.87 ± 1.43 | 20.55 ± 2.11 | 0.89 |
| N (%) | Dominant (DD + ID vs. II) | Recessive (DD vs. ID + II) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Groups | Genotype | Injury | Non-Injury | χ2 | df | p-Value | OR [95% CI] | p-Value | OR [95% CI] | p-Value |
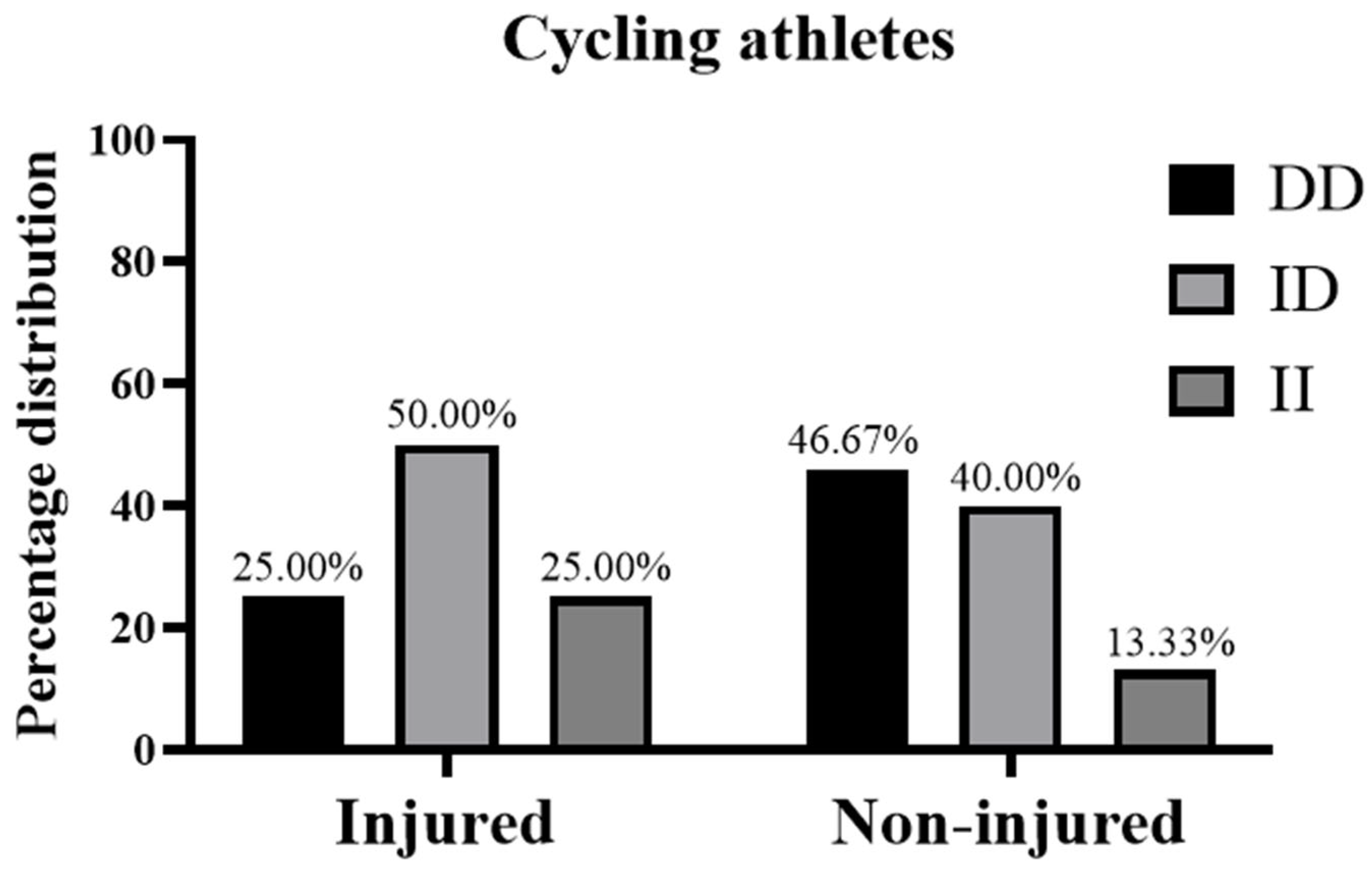
| Cyclists | DD | 1 (25.00%) | 7 (46.67%) | 0.69 | 2 | 0.7 | 0.46 [0.04–8.74] | 0.57 | 2.62 [0.30–38.34] | 0.43 |
| ID | 2 (50.00%) | 6 (40.00%) | ||||||||
| II | 1 (25.00%) | 2 (13.33%) | ||||||||
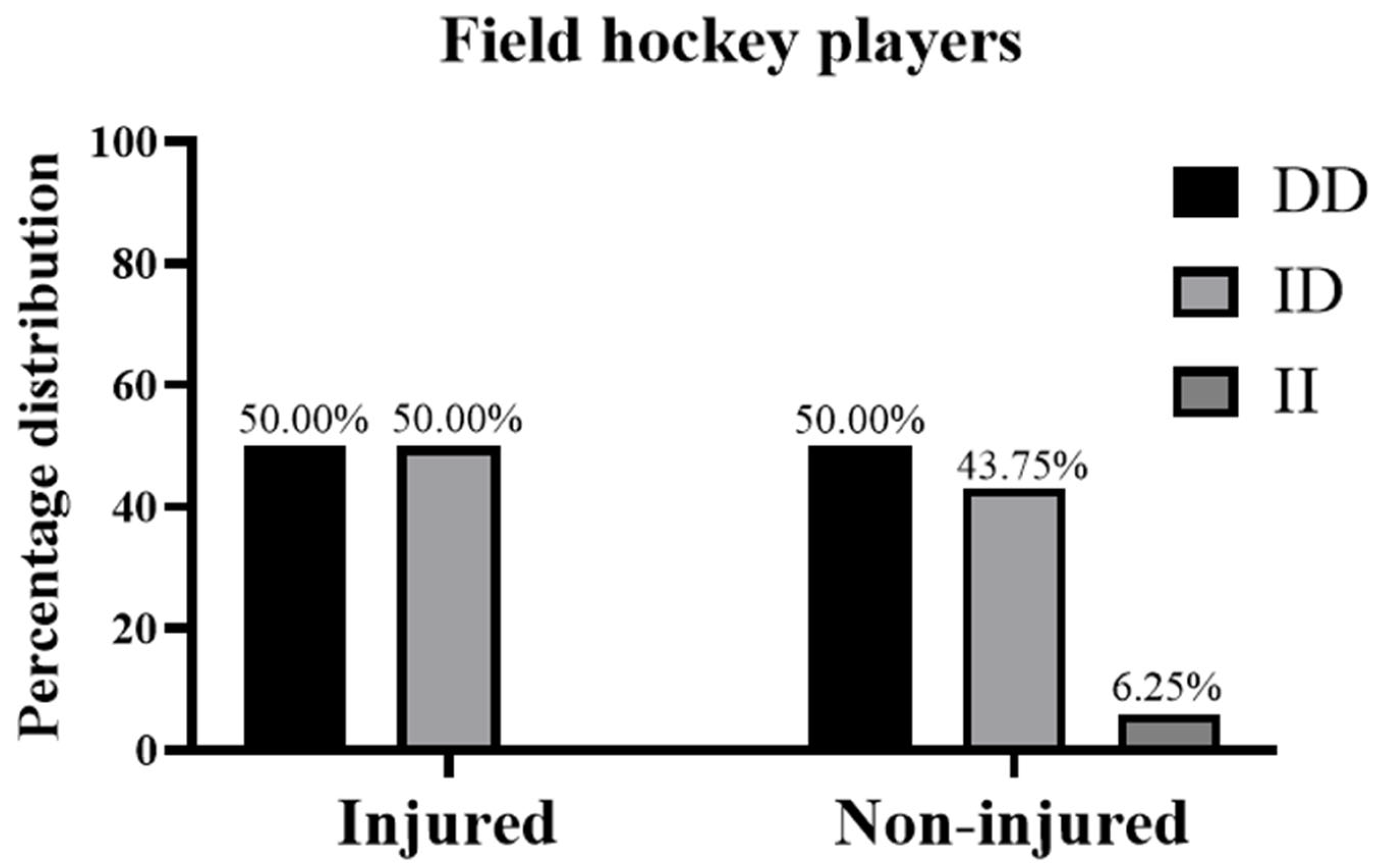
| Field hockey players | DD | 4 (50.00%) | 8 (50.00%) | 0.54 | 2 | 0.76 | Infinity [0.05–infinity] | 0.47 | 1.00 [0.21–4.71] | >0.999 |
| ID | 4 (50.00%) | 7 (43.75%) | ||||||||
| II | 0 (0%) | 1 (6.25%) | ||||||||
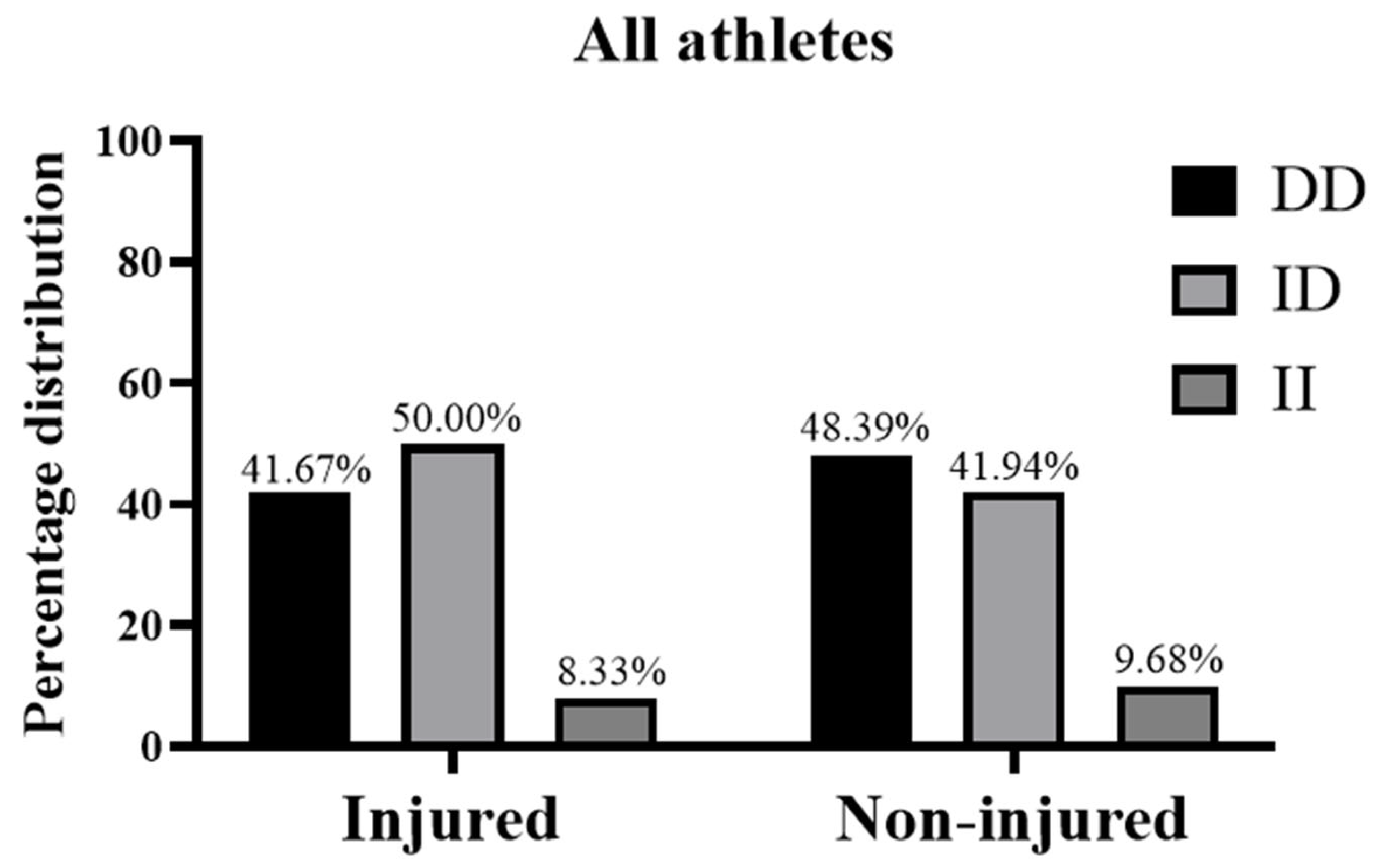
| All athletes | DD | 5 (41.67%) | 15 (48.39%) | 0.22 | 2 | 0.89 | 1.17 [0.15–16.56] | 0.89 | 1.31 [1.31–4.89] | 0.69 |
| ID | 6 (50.00%) | 13 (41.94%) | ||||||||
| II | 1 (8.33%) | 3 (9.68%) | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Ouali, E.M.; Kartibou, J.; Del Coso, J.; Supriya, R.; Laher, I.; El Kettani, Z.; Ghazal, H.; Al Idrissi, N.; Saeidi, A.; Mesfioui, A.; et al. ACE I/D Genotype and Risk of Non-Contact Injury in Moroccan Elite Athletes: A Pilot Study. Medicina 2025, 61, 98. https://doi.org/10.3390/medicina61010098
El Ouali EM, Kartibou J, Del Coso J, Supriya R, Laher I, El Kettani Z, Ghazal H, Al Idrissi N, Saeidi A, Mesfioui A, et al. ACE I/D Genotype and Risk of Non-Contact Injury in Moroccan Elite Athletes: A Pilot Study. Medicina. 2025; 61(1):98. https://doi.org/10.3390/medicina61010098
Chicago/Turabian StyleEl Ouali, El Mokhtar, Jihan Kartibou, Juan Del Coso, Rashmi Supriya, Ismail Laher, Zineb El Kettani, Hassan Ghazal, Najib Al Idrissi, Ayoub Saeidi, Abdelhalem Mesfioui, and et al. 2025. "ACE I/D Genotype and Risk of Non-Contact Injury in Moroccan Elite Athletes: A Pilot Study" Medicina 61, no. 1: 98. https://doi.org/10.3390/medicina61010098
APA StyleEl Ouali, E. M., Kartibou, J., Del Coso, J., Supriya, R., Laher, I., El Kettani, Z., Ghazal, H., Al Idrissi, N., Saeidi, A., Mesfioui, A., & Zouhal, H. (2025). ACE I/D Genotype and Risk of Non-Contact Injury in Moroccan Elite Athletes: A Pilot Study. Medicina, 61(1), 98. https://doi.org/10.3390/medicina61010098