
Sutureless Dehydrated Amniotic Membrane (Omnigen) Application Using a Specialised Bandage Contact Lens (OmniLenz) for the Treatment of Dry Eye Disease: A 6-Month Randomised Control Trial



Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Selection
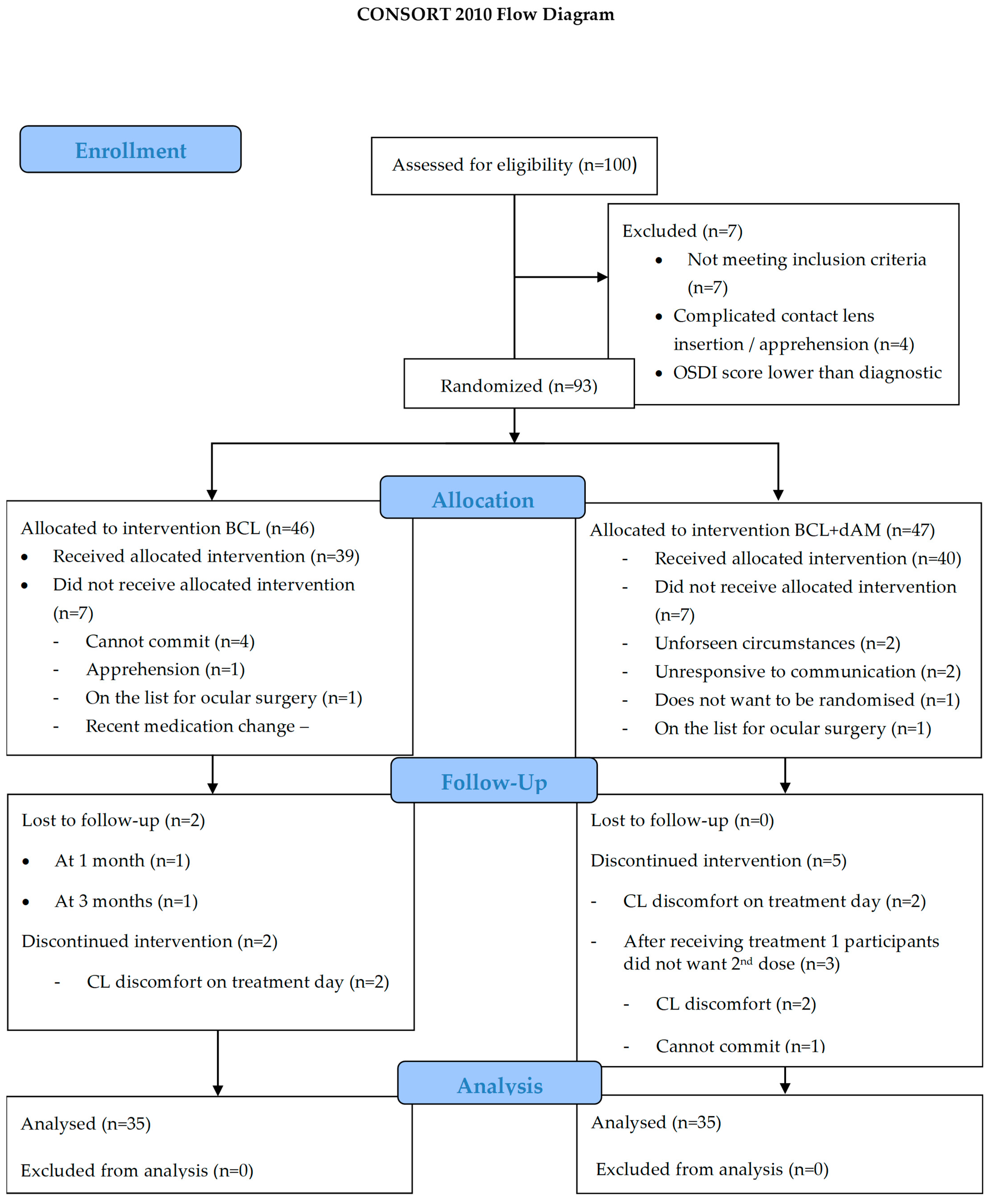
2.2. Study Design
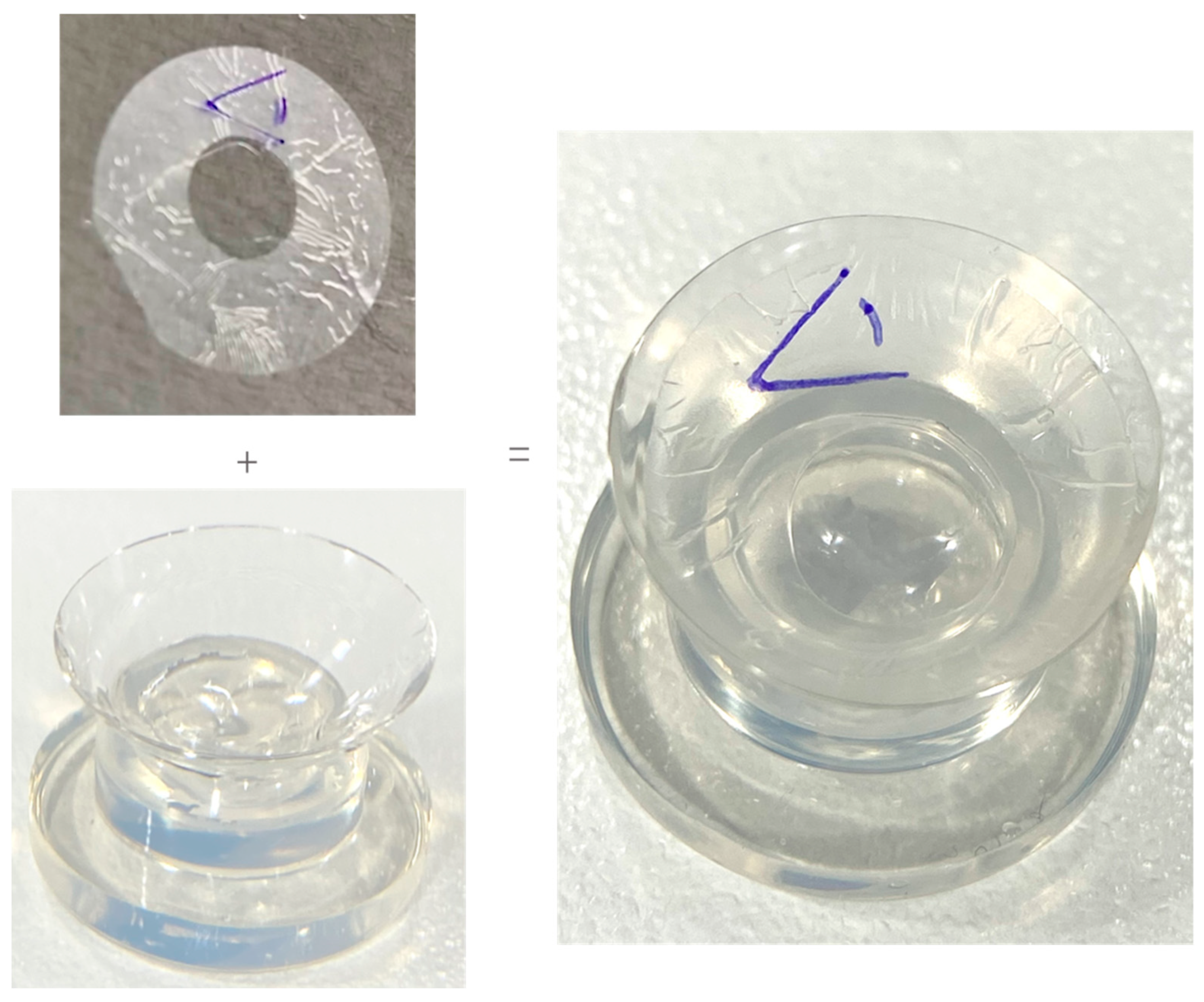
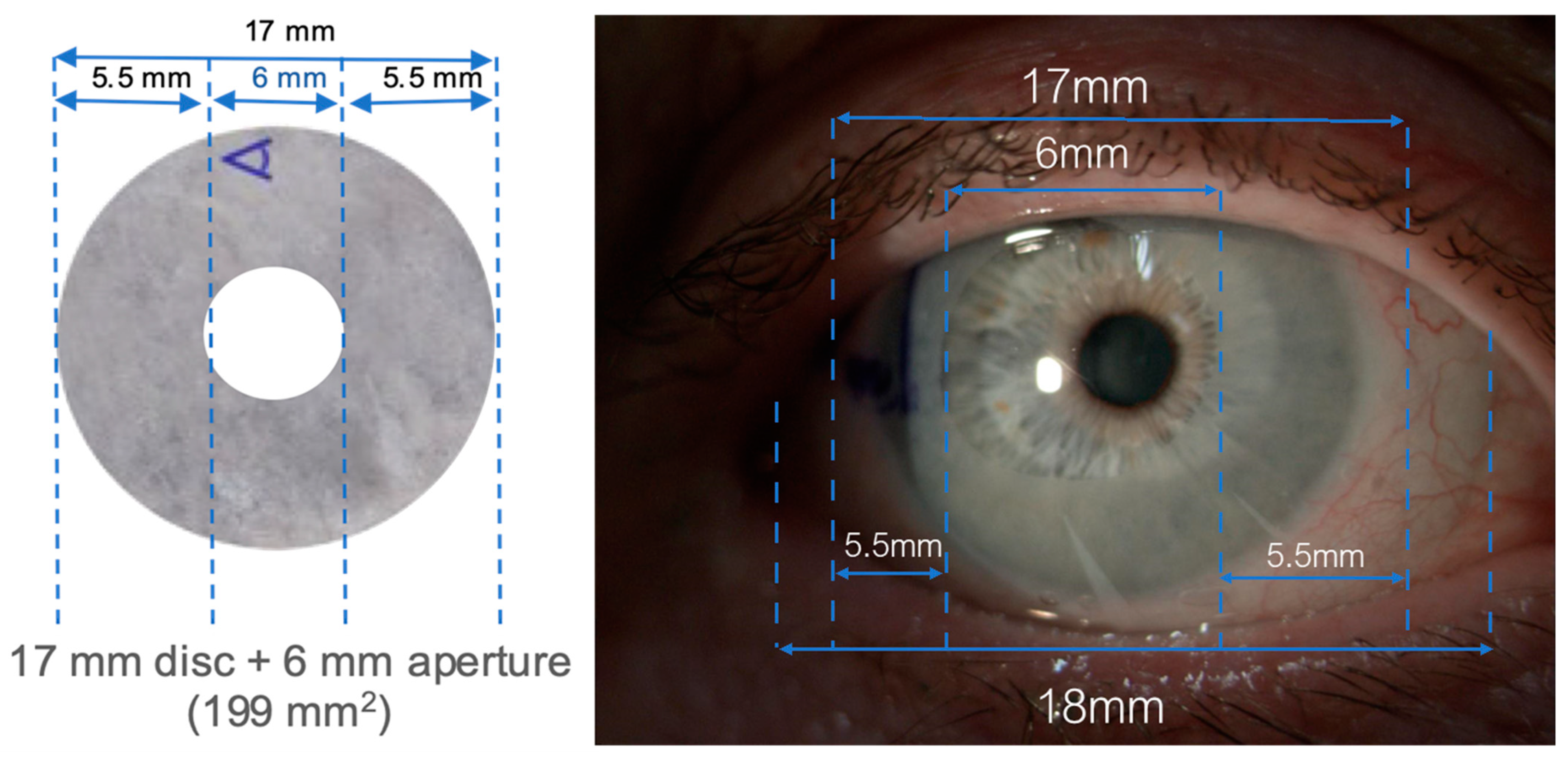
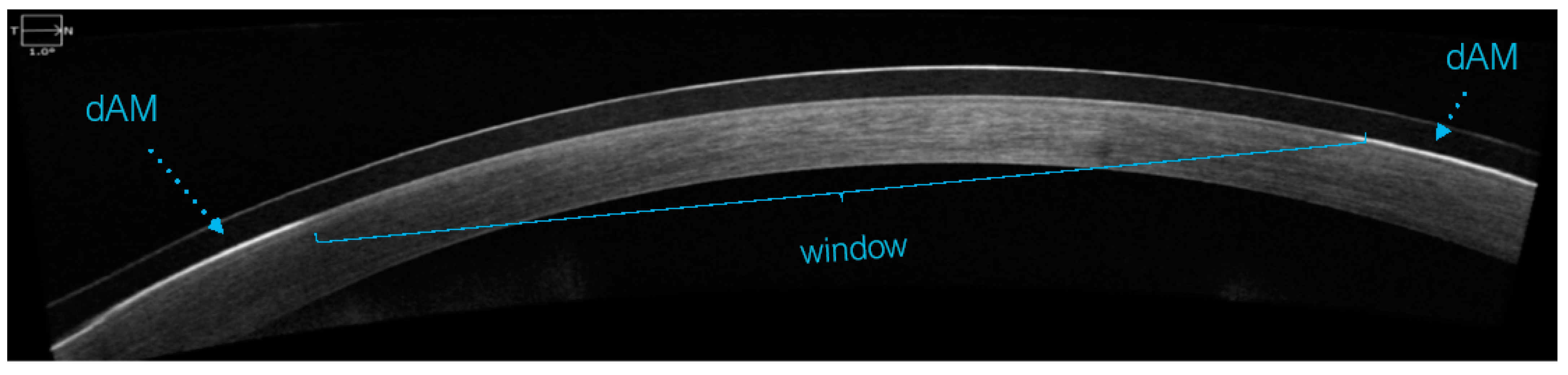
2.3. Intervention
2.4. Measurements
2.5. Responder Analysis
2.6. Statistical Analysis
3. Results
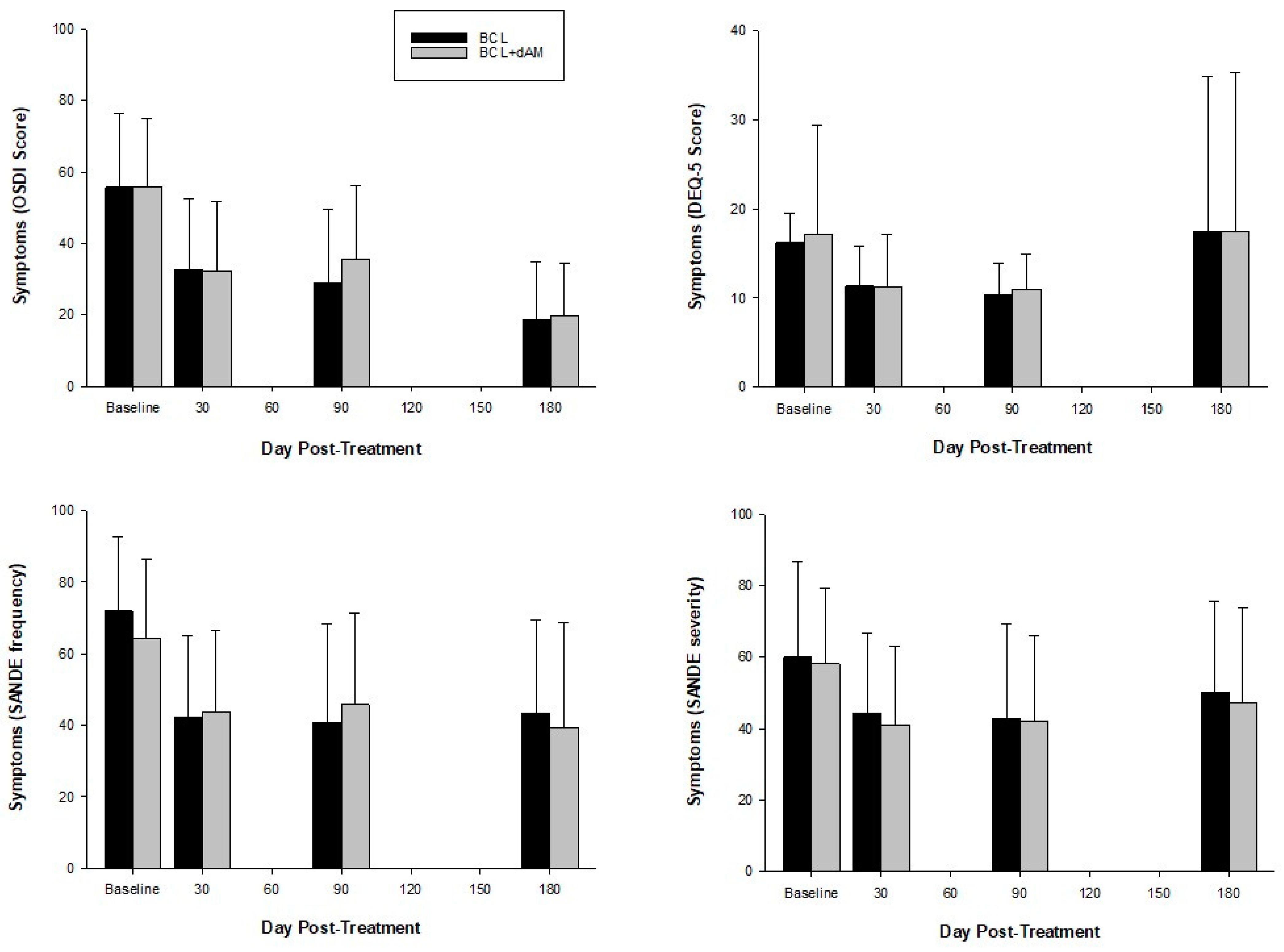
3.1. Symptomatology
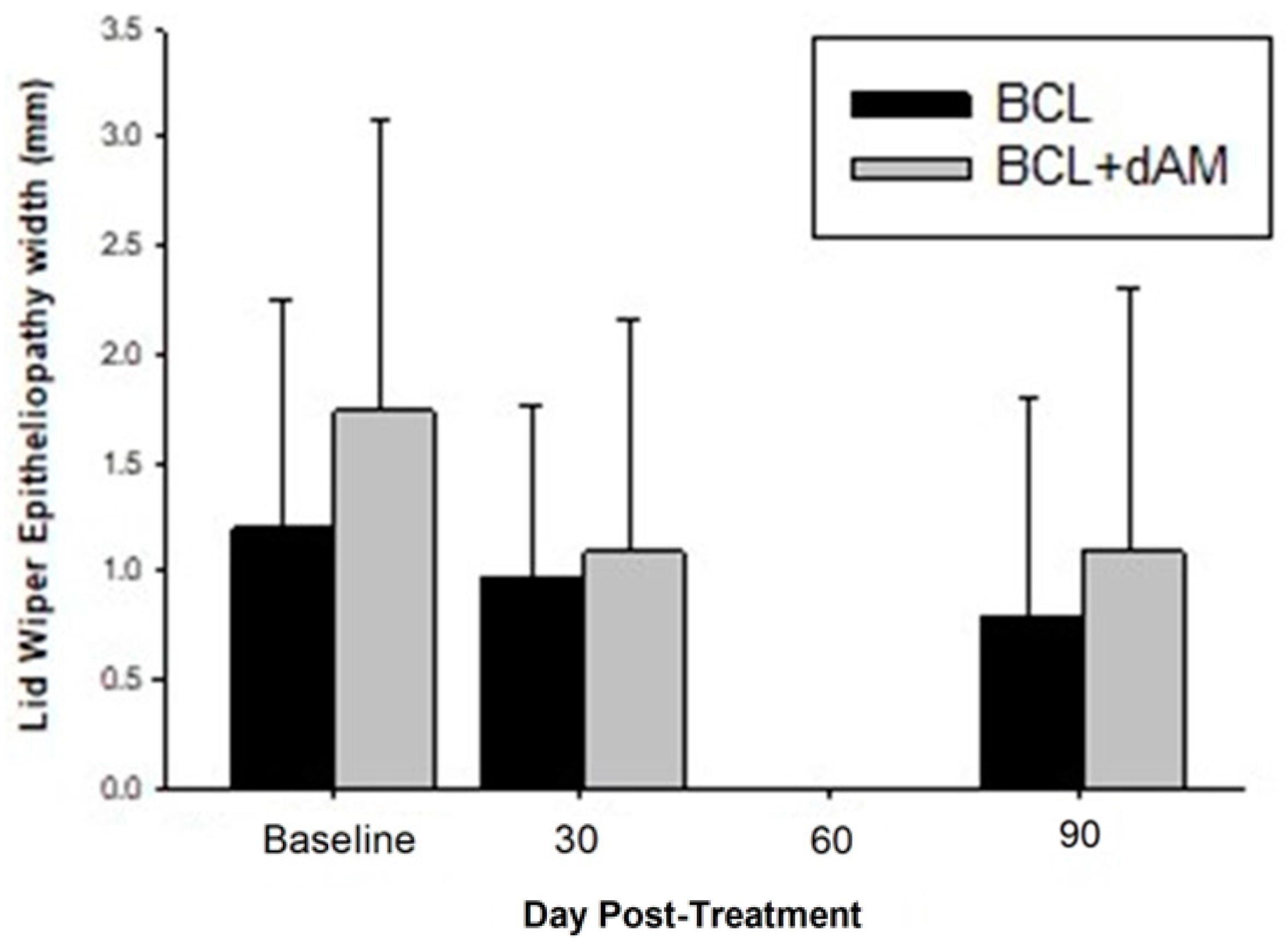
3.2. Signs
3.3. In Vivo Corneal Microscopy (IVCM) Analyses
3.3.1. Corneal Nerves
3.3.2. Corneal Dendritic Cells (CDCs)
Mature CDCs
Immature CDC
3.4. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.G.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Rohr, M.; Craig, J.P.; Davies, L.N.; Wolffsohn, J.S. The epidemiology of dry eye disease in the UK: The Aston dry eye study. Contact Lens Anterior Eye 2023, 46, 101837. [Google Scholar] [CrossRef] [PubMed]
- García-Marqués, J.V.; Talens-Estarelles, C.; García-Lázaro, S.; Wolffsohn, J.S.; Cerviño, A. Systemic, environmental and lifestyle risk factors for dry eye disease in a mediterranean caucasian population. Contact Lens Anterior Eye 2022, 45, 101539. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.T.M.; Vidal-Rohr, M.; Muntz, A.; Diprose, W.K.; Ormonde, S.E.; Wolffsohn, J.S.; Craig, J.P. Systemic risk factors of dry eye disease subtypes: A New Zealand cross-sectional study. Ocul. Surf. 2020, 18, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Wei, J.; Zhou, J.; Zou, W. Prevalence and Incidence of Dry Eye Disease in Asia: A Systematic Review and Meta-Analysis. Ophthalmic Res. 2022, 65, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Dana, R.; Bradley, J.L.; Guerin, A.; Pivneva, I.; Stillman, I.Ö.; Evans, A.M.; Schaumberg, D.A. Estimated Prevalence and Incidence of Dry Eye Disease Based on Coding Analysis of a Large, All-age United States Health Care System. Am. J. Ophthalmol. 2019, 202, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II pathophysiology report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef] [PubMed]
- De Paiva, C.S.; Corrales, R.M.; Villarreal, A.L.; Farley, W.J.; Li, D.Q.; Stern, M.E.; Pfiugfelder, S.C. Corticosteroid and doxycycline suppress MMP-9 and inflammatory cytokine expression, MAPK activation in the corneal epithelium in experimental dry eye. Exp. Eye Res. 2006, 83, 526–535. [Google Scholar] [CrossRef]
- Belmonte, C.; Nichols, J.J.; Cox, S.M.; Brock, J.A.; Begley, C.G.; Bereiter, D.A.; Dartt, D.A.; Galor, A.; Hamrah, P.; Ivanusic, J.J.; et al. TFOS DEWS II pain and sensation report. Ocul. Surf. 2017, 15, 404–437. [Google Scholar] [CrossRef]
- Shetty, R.; Sethu, S.; Deshmukh, R.; Deshpande, K.; Ghosh, A.; Agrawal, A.; Shroff, R. Corneal Dendritic Cell Density Is Associated with Subbasal Nerve Plexus Features, Ocular Surface Disease Index, and Serum Vitamin D in Evaporative Dry Eye Disease. BioMed Res. Int. 2016, 2016, 4369750. [Google Scholar] [CrossRef] [PubMed]
- Hossain, P.; Siffel, C.; Joseph, C.; Meunier, J.; Markowitz, J.T.; Dana, R. Patient-reported burden of dry eye disease in the UK: A cross-sectional web-based survey. BMJ Open 2021, 11, e039209. [Google Scholar] [CrossRef] [PubMed]
- Gayton, J.L. Etiology, prevalence, and treatment of dry eye disease. Clin. Ophthalmol. 2009, 3, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.L.; Özer Stillman, I.; Pivneva, I.; Guerin, A.; Evans, A.M.; Dana, R. Dry eye disease ranking among common reasons for seeking eye care in a large US claims database. Clin. Ophthalmol. 2019, 13, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Farrand, K.F.; Fridman, M.; Stillman, I.; Schaumberg, D.A. Prevalence of Diagnosed Dry Eye Disease in the United States Among Adults Aged 18 Years and Older. Am. J. Ophthalmol. 2017, 182, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Vehof, J.; Kozareva, D.; Hysi, P.; Fahy, S.; Direk, K.; Spector, T.; Hammond, C. Prevalence and Determinants of Dry Eye Disease in a British Female Cohort. Investig. Ophthalmol. Vis. Sci. 2013, 54, 2665. [Google Scholar]
- Yu, J.; Asche, C.V.; Fairchild, C.J. The economic burden of dry eye disease in the United States: A decision tree analysis. Cornea 2011, 30, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef] [PubMed]
- Sabeti, S.; Kheirkhah, A.; Yin, J.; Dana, R. Management of meibomian gland dysfunction: A review. Surv. Ophthalmol. 2020, 65, 205–217. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Trave Huarte, S.; Jones, L.; Craig, J.P.; Wang, M.T.M.; Ambassadors, T. Clinical practice patterns in the management of dry eye disease: A TFOS international survey. Ocul. Surf. 2021, 21, 78–86. [Google Scholar] [CrossRef]
- The management of dry eye. BMJ 2016, 353, i2333. [CrossRef]
- Hopkinson, A.; Britchford, E.R.; Sidney, L.E. Preparation of Dried Amniotic Membrane for Corneal Repair. In Corneal Regeneration. Methods and Protocols; Ahearne, M., Ed.; Springer Protocols: Methods in Molecular Biology (MIMB); Humana: New York, NY, USA, 2020; Volume 2145, pp. 143–157. [Google Scholar]
- Dua, H.S.; Gomes, J.A.P.; King, A.J.; Maharajan, V.S. The amniotic membrane in ophthalmology. Surv. Ophthalmol. 2004, 49, 51–77. [Google Scholar] [CrossRef]
- Hao, Y.X.; Ma, D.H.K.; Hwang, D.G.; Kim, W.S.; Zhang, F. Identification of antiangiogenic and antiinflammatory proteins in human amniotic membrane. Cornea 2000, 19, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, A.; McIntosh, R.S.; Shanmuganathan, V.; Tighe, P.J.; Dua, H.S. Proteomic analysis of amniotic membrane prepared for human transplantation: Characterization of proteins and clinical implications. J. Proteome Res. 2006, 5, 2226–2235. [Google Scholar] [CrossRef] [PubMed]
- Tseng, S.C.G.; Li, D.Q.; Ma, X. Suppression of transforming growth factor-beta isoforms, TGF-beta receptor type II, and myofibroblast differentiation in cultured human corneal and limbal fibroblasts by amniotic membrane matrix. J. Cell. Physiol. 1999, 179, 325–335. [Google Scholar] [CrossRef]
- Walkden, A. Amniotic Membrane Transplantation in Ophthalmology: An Updated Perspective. Clin. Ophthalmol. 2020, 14, 2057–2072. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.; Janik, S.B.; Bowden, F.W.; Chokshi, A.; Singer, M.A.; Tighe, S.; Mead, O.G.; Nanda, S.; Qazi, M.A.; Dierker, D.; et al. Association of Treatment Duration and Clinical Outcomes in Dry Eye Treatment with Sutureless Cryopreserved Amniotic Membrane. Clin. Ophthalmol. 2023, 17, 2697–2703. [Google Scholar] [CrossRef] [PubMed]
- Maqsood, S.; Elsawah, K.; Dhillon, N.; Soliman, S.; Laginaf, M.; Lodhia, V.; Lake, D.; Hamada, S.; Elalfy, M. Management of Persistent Corneal Epithelial Defects with Human Amniotic Membrane-derived Dry Matrix. Clin. Ophthalmol. 2021, 15, 2231–2238. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.K.; Holland, L.; Elhaddad, O. Treating Corneal Epithelial Defects Using Dehydrated Human Amniotic Membrane-Derived Material: A Prospective Study. Eye 2023. [Google Scholar] [CrossRef]
- Lotfy, N.M.; Al Rashidi, S.; Hagras, S.M. Clinical outcomes of vacuum-dehydrated amniotic membrane (Omnigen) mounted on contact lens (Omnilenz) in eyes with acute chemical eye injuries. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 3541–3547. [Google Scholar] [CrossRef]
- Mehta, A.; Pradhan, S.; Figueiredo, F. Low temperature vacuum-dehydrated amnion membrane (Omnigen)—Case series for the treatment of ocular surface burn and related complications at a tertiary eye unit in the UK. Investig. Ophthalmol. Vis. Sci. 2021, 62, 1258. [Google Scholar]
- Travé-Huarte, S.; Wolffsohn, J.S. Bilateral Sutureless Application of Human Dehydrated Amniotic Membrane with a Specialized Bandage Contact Lens for Moderate-to-Severe Dry Eye Disease: A Prospective Study with 1-Month Follow-Up. Clin. Ophthalmol. 2024, 18, 1329–1339. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Grp, C. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomized Trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.A.P.; Azar, D.T.; Baudouin, C.; Bitton, E.; Chen, W.; Hafezi, F.; Hamrah, P.; Hogg, R.E.; Horwath-Winter, J.; Kontadakis, G.A.; et al. TFOS Lifestyle: Impact of elective medications and procedures on the ocular surface. Ocul. Surf. 2023, 29, 331–385. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.L.; Walt, J.G.; Mink, D.R.; Satram-Hoang, S.; Wilson, S.E.; Perry, H.D.; Asbell, P.A.; Pflugfelder, S.C. Minimal Clinically Important Difference for the Ocular Surface Disease Index. Arch. Ophthalmol. 2010, 128, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Kheirkhah, A.; Johnson, D.A.; Paranjpe, D.R.; Raju, V.K.; Casas, V.; Tseng, S.C.G. Temporary sutureless amniotic membrane patch for acute alkaline burns. Arch. Ophthalmol. 2008, 126, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.L.; Clare, G.; Stewart, E.A.; Branch, M.J.; McIntosh, O.D.; Dadhwal, M.; Dua, H.S.; Hopkinson, A. Augmented Dried versus Cryopreserved Amniotic Membrane as an Ocular Surface Dressing. PLoS ONE 2013, 8, e78441. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhai, H.L.; Xu, Y.Y.; Dong, Y.L.; Sun, Y.J.; Zang, X.J.; Zhao, J. Amniotic membrane traps and induces apoptosis of inflammatory cells in ocular surface chemical burn. Mol. Vis. 2012, 18, 2137–2146. [Google Scholar] [PubMed]
- Kim, J.S.; Kim, J.C.; Na, B.K.; Jeong, J.M.; Song, C.Y. Amniotic membrane patching promotes healing and inhibits proteinase activity on wound healing following acute corneal alkali burn. Exp. Eye Res. 2000, 70, 329–337. [Google Scholar] [CrossRef]
- Teson, M.; Lopez-Miguel, A.; Neves, H.; Calonge, M.; Gonzalez-Garcia, M.J.; Gonzalez-Meijome, J.M. Influence of Climate on Clinical Diagnostic Dry Eye Tests: Pilot Study. Optom. Vision Sci. 2015, 92, E284–E289. [Google Scholar] [CrossRef]
- Schaumberg, D.A.; Gulati, A.; Mathers, W.D.; Clinch, T.; Lemp, M.A.; Nelson, J.D.; Foulks, G.N.; Dana, R. Development and validation of a short global dry eye symptom index. Ocul. Surf. 2007, 5, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, R.L.; Begley, C.G.; Caffery, B. Validation of the 5-Item Dry Eye Questionnaire (DEQ-5): Discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Contact Lens Anterior Eye 2010, 33, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Guillon, J.P. Use of the tearscope plus and attachments in the routine examination of the marginal dry eye contact lens patient. In Lacrimal Gland, Tear Film, and Dry Eye Syndromes 2: Basic Science and Clinical Relevance; Springer: New York, NY, USA, 1998; Volume 438, pp. 859–867. [Google Scholar]
- Wu, S.Q.; Hong, J.X.; Tian, L.J.; Cui, X.H.; Sun, X.H.; Xu, J.J. Assessment of Bulbar Redness with a Newly Developed Keratograph. Optom. Vision Sci. 2015, 92, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Peterson, R.C.; Wolffsohn, J.S.; Fowler, C.W. Optimization of anterior eye fluorescein viewing. Am. J. Ophthalmol. 2006, 142, 572–575. [Google Scholar] [CrossRef]
- Bron, A.J.; Evans, V.E.; Smith, J.A. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea 2003, 22, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Korb, D.R.; Herman, J.P.; Finnemore, V.M.; Greiner, J.V.; Olson, M.C.; Scaffidi, R.C. Lid wiper epitheliopathy and associated dry eye symptoms. Investig. Ophthalmol. Vis. Sci. 2004, 45, U123. [Google Scholar]
- Tavakoli, M.; Malik, R.A. Corneal confocal microscopy: A novel non-invasive technique to quantify small fibre pathology in peripheral neuropathies. J. Vis. Exp. JoVE 2011, 47, e2194. [Google Scholar] [CrossRef] [PubMed]
- Dabbah, M.A.; Graham, J.; Petropoulos, I.; Tavakoli, M.; Malik, R.A. Dual-model automatic detection of nerve-fibres in corneal confocal microscopy images. Med. Image Comput. Comput. Assist. Interv. 2010, 13, 300–307. [Google Scholar] [CrossRef]
- Tavakoli, M.; Ferdousi, M.; Petropoulos, I.N.; Morris, J.; Pritchard, N.; Zhivov, A.; Ziegler, D.; Pacaud, D.; Romanchuk, K.; Perkins, B.A.; et al. Normative Values for Corneal NerveMorphology Assessed Using Corneal Confocal Microscopy: A Multinational Normative Data Set. Diabetes Care 2015, 38, 838–843. [Google Scholar] [CrossRef]
- Mobeen, R.; Stapleton, F.; Chao, C.; Madigan, M.C.; Briggs, N.; Golebiowski, B. Corneal epithelial dendritic cell density in the healthy human cornea: A meta-analysis of in-vivo confocal microscopy data. Ocul. Surf. 2019, 17, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, Y.; Pritchard, N.; Efron, N. Changes in corneal Langerhans cell density during the first few hours of contact lens wear. Contact Lens Anterior Eye 2016, 39, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.M.S.; Zhao, D.; Chen, R.; Yin, H.Y.; Tighe, S.; Sheha, H.; Casas, V.; Tseng, S.C.G. Accelerated Restoration of Ocular Surface Health in Dry Eye Disease by Self-Retained Cryopreserved Amniotic Membrane. Ocul. Surf. 2016, 14, 56–63. [Google Scholar] [CrossRef] [PubMed]
- John, T.; Tighe, S.; Sheha, H.; Hamrah, P.; Salem, Z.M.; Cheng, A.M.S.; Wang, M.X.; Rock, N.D. Corneal Nerve Regeneration after Self-Retained Cryopreserved Amniotic Membrane in Dry Eye Disease. J. Ophthalmol. 2017, 2017, 6404918. [Google Scholar] [CrossRef]
- McDonald, M.B.; Sheha, H.; Tighe, S.; Janik, S.B.; Bowden, F.W.; Chokshi, A.R.; Singer, M.A.; Nanda, S.; Qazi, M.A.; Dierker, D.; et al. Treatment outcomes in the DRy Eye Amniotic Membrane (DREAM) study. Clin. Ophthalmol. 2018, 12, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Muntz, A.; Wang, M.T.M.; Luensmann, D.; Tan, J.; Huarte, S.T.; Xue, A.L.; Jones, L.; Willcox, M.D.P.; Wolffsohn, J.S. Developing evidence-based guidance for the treatment of dry eye disease with artificial tear supplements: A six-month multicentre, double-masked randomised controlled trial. Ocul. Surf. 2021, 20, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.D.; Ma, Y.J.; Chen, X.; He, S.H.; Lin, X.Q.; Yu, X.W.; Chen, W.J.; Luo, C.Q.; Xu, W. Efficacy of bandage contact lens for the management of dry eye disease after cataract surgery. Int. Ophthalmol. 2021, 41, 1403–1413. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.S.; Carrasquillo, K.G.; Cottrell, P.D.; Fernandez-Velazquez, F.J.; Gil-Cazorla, R.; Jalbert, I.; Pucker, A.D.; Riccobono, K.; Robertson, D.M.; Szczotka-Flynn, L.; et al. CLEAR–Medical use of contact lenses. Contact Lens Anterior Eye 2021, 44, 289–329. [Google Scholar] [CrossRef] [PubMed]
- Colorado, L.H.; Pritchard, N.; Alzahrani, Y.; Edwards, K.; Efron, N. Association between conjunctival goblet cells and corneal resident dendritic cell density changes in new contact lens wearers. Clin. Exp. Optom. 2020, 103, 787–791. [Google Scholar] [CrossRef]
- Auran, J.D.; Koester, C.J.; Kleiman, N.J.; Rapaport, R.; Bomann, J.S.; Wirotsko, B.M.; Florakis, G.J.; Koniarek, J.P. Scanning Slit Confocal Microscopic Observation of Cell Morphology and Movement within the Normal Human Anterior Cornea. Ophthalmology 1995, 102, 33–41. [Google Scholar] [CrossRef]
- Mastropasqua, L.; Nubile, M.; Lanzini, M.; Carpineto, P.; Ciancaglini, M.; Pannellini, T.; Di Nicola, M.; Dua, H.S. Epithelial dendritic cell distribution in normal and inflamed human cornea: In vivo confocal microscopy study. Am. J. Ophthalmol. 2006, 142, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Narumi, M.; Kashiwagi, Y.; Namba, H.; Ohe, R.; Yamakawa, M.; Yamashita, H. Contribution of Corneal Neovascularization to Dendritic Cell Migration into the Central Area during Human Corneal Infection. PLoS ONE 2014, 9, e109859. [Google Scholar] [CrossRef] [PubMed]
- Zhivov, A. In vivo confocal microscopic evaluation of langerhans cell density and distribution in the corneal epithelium of healthy volunteers and contact lens wearers. Cornea 2007, 26, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Sindt, C.W.; Grout, T.K.; Critser, D.B.; Kern, J.R.; Meadows, D.L. Dendritic immune cell densities in the central cornea associated with soft contact lens types and lens care solution types: A pilot study. Clin. Ophthalmol. 2012, 6, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Qazi, Y.; Kheirkhah, A.; Blackie, C.; Cruzat, A.; Trinidad, M.; Williams, C.; Korb, D.R.; Hamrah, P. In vivo detection of clinically non-apparent ocular surface inflammation in patients with meibomian gland dysfunction-associated refractory dry eye symptoms: A pilot study. Eye 2015, 29, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Steinman, R.M. The Dendritic Cell System and Its Role in Immunogenicity. Annu. Rev. Immunol. 1991, 9, 271–296. [Google Scholar] [CrossRef] [PubMed]
- Austyn, J.M. New insights into the mobilization and phagocytic activity of dendritic cells. J. Exp. Med. 1996, 183, 1287–1292. [Google Scholar] [CrossRef] [PubMed]
- Sheha, Y.H.H.; Tseng, S. Self-retained Amniotic Membrane for Recurrent Corneal Erosion. J. Clin. Exp. Ophthalmol. 2013, 4, 272. [Google Scholar] [CrossRef]
- Mimouni, M.; Trinh, T.; Sorkin, N.; Cohen, E.; Santaella, G.; Rootman, D.S.; Slomovic, A.R.; Chan, C.C. Sutureless dehydrated amniotic membrane for persistent epithelial defects. Eur. J. Ophthalmol. 2022, 32, 875–879. [Google Scholar] [CrossRef]
- Gris, O.; del Campo, Z.; Wolley-Dod, C.; Güell, J.L.; Bruix, A.; Calatayud, M.; Adán, A. Amniotic membrane implantation as a therapeutic contact lens for the treatment of epithelial disorders. Cornea 2002, 21, 22–27. [Google Scholar] [CrossRef]
- Sheha, H.; Liang, L.Y.; Li, J.J.; Tseng, S.C.G. Sutureless Amniotic Membrane Transplantation for Severe Bacterial Keratitis. Cornea 2009, 28, 1118–1123. [Google Scholar] [CrossRef] [PubMed]
- Mead, O.G.; Tighe, S.; Tseng, S.C.G. Amniotic membrane transplantation for managing dry eye and neurotrophic keratitis. Taiwan J. Ophthalmol. 2020, 10, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, M.; Naderan, M. Management Strategies of Ocular Chemical Burns: Current Perspectives. Clin. Ophthalmol. 2020, 14, 2687–2699. [Google Scholar] [CrossRef] [PubMed]
- Kheirkhah, A.; Casas, V.; Raju, V.K.; Tseng, S.C.G. Sutureless amniotic membrane transplantation for partial limbal stem cell deficiency. Am. J. Ophthalmol. 2008, 145, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.X.; Kruse, F.; Gomes, J.A.P.; Chan, C.C.; Daya, S.; Dana, R.; Figueiredo, F.C.; Kinoshita, S.; Rama, P.; Sangwan, V.; et al. Global Consensus on the Management of Limbal Stem Cell Deficiency. Cornea 2020, 39, 1291–1302. [Google Scholar] [CrossRef] [PubMed]
- Morkin, M.I.; Hamrah, P. Efficacy of self-retained cryopreserved amniotic membrane for treatment of neuropathic corneal pain. Ocul. Surf. 2018, 16, 132–138. [Google Scholar] [CrossRef]
- Singh, P.; Raj, A.; Gupta, A.; Pradhan, S.; Aftab, N.; Biswas, S. Role of amniotic membrane transplantation in treating acute ocular manifestations in Steven-Johnson syndrome and its long-term impact. Indian J. Ophthalmol. 2022, 70, 4470–4471. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | BCL-Alone | dAM+sBCL | p Value |
|---|---|---|---|
| Age | 50.820 ± 19.14 | 49.76 ± 17.0 | 0.813 |
| Gender | 8 males, 27 females | 11 males, 21 females | 0.373 |
| OSDI | 55.71 ± 20.67 | 56.71 ± 18.53 | 0.831 |
| DEQ-5 | 16.24 ± 3.32 | 14.81 ± 2.58 | 0.123 |
| SANDE Frequency | 71.92 ± 20.85 | 65.04 ± 22.68 | 0.312 |
| SANDE severity | 59.96 ± 26.66 | 59.67 ± 19.77 | 0.959 |
| VA (LogMAR) | 0.08 ± 0.17 | 0.12 ± 0.15 | 0.473 |
| TMH (mm) | 0.30 ± 0.13 | 0.26 ± 0.09 | 0.125 |
| Hyperaemia Bulbar temporal (grade) | 1.16 ± 0.53 | 1.11 ± 0.45 | 0.629 |
| Hyperaemia Bulbar nasal (grade) | 0.95 ± 0.46 | 1.09 ± 0.51 | 0.242 |
| Hyperaemia Limbal temporal (grade) | 0.82 ± 0.41 | 0.79 ± 0.36 | 0.772 |
| Hyperaemia Limbal nasal(grade) | 0.74 ± 0.42 | 0.79 ± 0.40 | 0.545 |
| NIKBUT (seconds) | 8.33 ± 5.91 | 7.84 ± 4.66 | 0.710 |
| LLT (grade) | 3.20 ± 1.61 | 4.14 ± 1.14 | 0.007 * |
| CornS (grade) | 1.14 ± 1.35 | 1.37 ± 1.21 | 0.469 |
| ConjS (grade) | 1.63 ± 0.94 | 1.80 ± 1.28 | 0.841 |
| LWE Length (grade) | 1.51 ± 1.48 | 1.97 ± 1.40 | 0.133 |
| LWE Width (grade) | 1.20 ± 1.05 | 1.74 ± 1.34 | 0.060 |
| CNFD (no./mm2) | 20.36 ± 10.88 | 23.16 ± 11.36 | 0.252 |
| CNBD (no./mm2) | 26.47 ± 25.24 | 33.64 ± 37.02 | 0.363 |
| CNFL (mm/mm2) | 13.63 ± 4.17 | 13.79 ± 5.82 | 0.659 |
| CTBD (mm/mm2) | 49.26 ± 35.74 | 54.78 ± 61.39 | 0.638 |
| CDC Activated (no./mm2) | 6.96 ± 9.55 | 11.78 ± 10.03 | 0.005 * |
| CDC Inactivated (no./mm2) | 24.82 ± 30.75 | 22.32 ± 20.97 | 0.672 |
| Feature (Units) | With Treatment (Over Time) | Between Treatments |
|---|---|---|
| CNFD no./mm2 | F = 1.072, p = 0.363 | F = 2.005, p = 0.163 |
| CNBD no./mm2 | F = 0.178, p = 0.837 | F = 1.810, p = 0.184 |
| CNFL mm/mm2 | F = 2.162, p = 0.120 | F = 1.43-, p = 0.237 |
| CTBD mm/mm2 | F = 0.035, p = 0.966 | F = 1.098, p = 0.299 |
| CDCs activated no./mm2 | F = 0.779, p = 0.461 | F = 0.138, p = 0.711 |
| CDCs deactivated no./mm2 | F = 5.355, p = 0.006 * | F = 1.261, p = 0.266 |
| Parameter | Baseline | Change— 1 Month | p Value | Change— 3 Months | p Value |
|---|---|---|---|---|---|
| CNFL | |||||
| sBCL-alone | 14.52 ± 3.72 | −0.8% (−0.11) | 0.908 | 10% (+1.45) | 0.013 * |
| dAM+sBCL | 14.3 ± 3.43 | 9.7% (+1.4) | 0.170 | 6.7% (0.82) | 0.359 |
| p value | 0.927 | 0.379 | 0.466 | ||
| CNFD | |||||
| sBCL-alone | 22.46 ± 5.11 | −5.2% (−1.17) | 0.526 | 12.2% (+2.7) | 0.232 |
| dAM+sBCL | 19.17 ± 4.82 | 15.2% (+2.92) | 0.070 | 10.9% (+2.1)) | 0.231 |
| p value | 0.253 | 0.791 | 0.190 | ||
| CNBD | |||||
| sBCL-alone | 29.43 ± 4.12 | −8.9% (−2.62) | 0.554 | 14.4% (+4.23) | 0.448 |
| dAM+sBCL | 32.71 ± 4.32 | 15.9% (+5.21) | 0.501 | −3.2% (−1.04) | 0.869 |
| p value | 0.687 | 0.114 | 0.774 | ||
| CTBD | |||||
| sBCL-alone | 47.26 ± 6.12 | −3.3% (−1.56) | 0.797 | 9.9% (+4.69) | 0.504 |
| dAM+sBCL | 53.88 ± 6.32 | 12.4% (+6.68) | 0.599 | −7.6% (−4.09) | 0.681 |
| p value | 0.620 | 0.043 * | 0.817 |
| 1-Month 100% Participants (n = 35) | 3-Month 100% Participants (n = 35) | |||||
|---|---|---|---|---|---|---|
| Combined Nerves | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone |
| Responders | 74% (26) | 29% (10) | <0.001 * | 74% (26) | 74% (25) | 0.870 |
| Negative responders | 14% (5) | 65% (22) | <0.001 * | 11% (4) | 21% (7) | 0.245 |
| p value | <0.001 * | 0.037 * | <0.001 * | <0.001 * | ||
| CNFL | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM-sBCL | sBCL-alone | dAM-sBC Lv sBCL-alone |
| Positive responders | 34% (11) | 15% (5) | 0.072 * | 41% (13) | 18% (6) | 0.424 |
| Negative responders | 9% (3) | 9% (3) | 0.658 | 13% (4) | 6% (2) | 0.610 |
| p value | 0.011 * | 0.317 | 0.001 * | 0.046 * | ||
| CNFD | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone |
| Positive responders | 35% (11) | 15% (5) | 0.142 | 47% (15) | 26% (9) | 0.430 |
| Negative responders | 13% (4) | 24% (8) | 0.320 | 19% (6) | 15% (6) | 0.950 |
| p value | 0.006 * | 0.239 | 0.011 * | 0.131 | ||
| CNBD | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone |
| Positive responders | 56% (18) | 33% (11) | 0.018 * | 42% (13) | 45% (15) | 0.610 |
| Negative responders | 34% (11) | 42% (14) | 0.675 | 32% (10) | 27% (9) | 0.290 |
| p value | 0.066 | 0.228 | 0.376 | 0.058 | ||
| CTBD | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM-sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone |
| Positive responders | 59% (19) | 33% (11) | 0.004 * | 42% (13) | 45% (15) | 0.76 |
| Negative responders | 34% (11) | 42% (14) | 0.867 | 39% (12) | 27% (9) | 0.59 |
| p value | 0.039 * | 0.206 | 0.777 | 0.564 | ||
| Treatment | % Change: 1 Month (Units) | p Value | % Change: 3 Month (Units) | p Value | Effect over Time |
|---|---|---|---|---|---|
| Mature CDCs | |||||
| sBCL-alone | −12.82% (−0.15) | 0.922 | 7.69% (0.09) | 0.563 | 0.740 |
| dAM+sBCL | −22.22% (−0.44) | 0.056 | −30.16% (−0.59) | 0.025 * | 0.070 |
| variance | −9.4% (−0.29) | −37.85% (−0.68) | |||
| p value | 0.184 | 0.068 | |||
| Immature CDCs | |||||
| sBCL-alone | 41% (1.63) | 0.248 | −4% (−0.17) | 0.656 | −0.073 |
| dAM+sBCL | 54.6% (1.97) | 0.009 * | 34.5% (1.24) | 0.153 | 0.079 |
| variance | 13% (0.34) | 38.5% (1.41) | |||
| p value | 0.375 | 0.108 |
| 1-Month 100% Participants (n = 70) | 3-Month 100% Participants (n = 70) | |||||
|---|---|---|---|---|---|---|
| Mature CDCs | dAM+sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM+sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone |
| Positive responders | 31% (10) | 25% (8) | 0.929 | 47% (15) | 16% (5) | 0.384 |
| Negative responders | 25% (8) | 50% (16) | 25% (8) | 56% (18) | ||
| p value | 0.083 | 0.447 | 0.055 * | 0.792 | ||
| Immature CDCs | dAM+sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone | dAM+sBCL | sBCL-alone | dAM-sBCL vs. sBCL-alone |
| Positive responders | 18% (6) | 23% (8) | 0.634 | 25% (8) | 40% (14) | 0.165 |
| Negative responders | 55% (18) | 51% (18) | 52% (17) | 23% (8) | ||
| p value | <0.002 * | 0.013 * | 0.022 * | 0.122 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Travé-Huarte, S.; Wolffsohn, J.S. Sutureless Dehydrated Amniotic Membrane (Omnigen) Application Using a Specialised Bandage Contact Lens (OmniLenz) for the Treatment of Dry Eye Disease: A 6-Month Randomised Control Trial. Medicina 2024, 60, 985. https://doi.org/10.3390/medicina60060985
Travé-Huarte S, Wolffsohn JS. Sutureless Dehydrated Amniotic Membrane (Omnigen) Application Using a Specialised Bandage Contact Lens (OmniLenz) for the Treatment of Dry Eye Disease: A 6-Month Randomised Control Trial. Medicina. 2024; 60(6):985. https://doi.org/10.3390/medicina60060985
Chicago/Turabian StyleTravé-Huarte, Sònia, and James S. Wolffsohn. 2024. "Sutureless Dehydrated Amniotic Membrane (Omnigen) Application Using a Specialised Bandage Contact Lens (OmniLenz) for the Treatment of Dry Eye Disease: A 6-Month Randomised Control Trial" Medicina 60, no. 6: 985. https://doi.org/10.3390/medicina60060985
APA StyleTravé-Huarte, S., & Wolffsohn, J. S. (2024). Sutureless Dehydrated Amniotic Membrane (Omnigen) Application Using a Specialised Bandage Contact Lens (OmniLenz) for the Treatment of Dry Eye Disease: A 6-Month Randomised Control Trial. Medicina, 60(6), 985. https://doi.org/10.3390/medicina60060985