

Antiretroviral Therapy Switch in HIV-Infected Adults from a Regional HIV/AIDS Center in NE Romania

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Database Description
2.2. Ethical Approval
2.3. Study Design
2.4. Study Setting and Data Collection
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
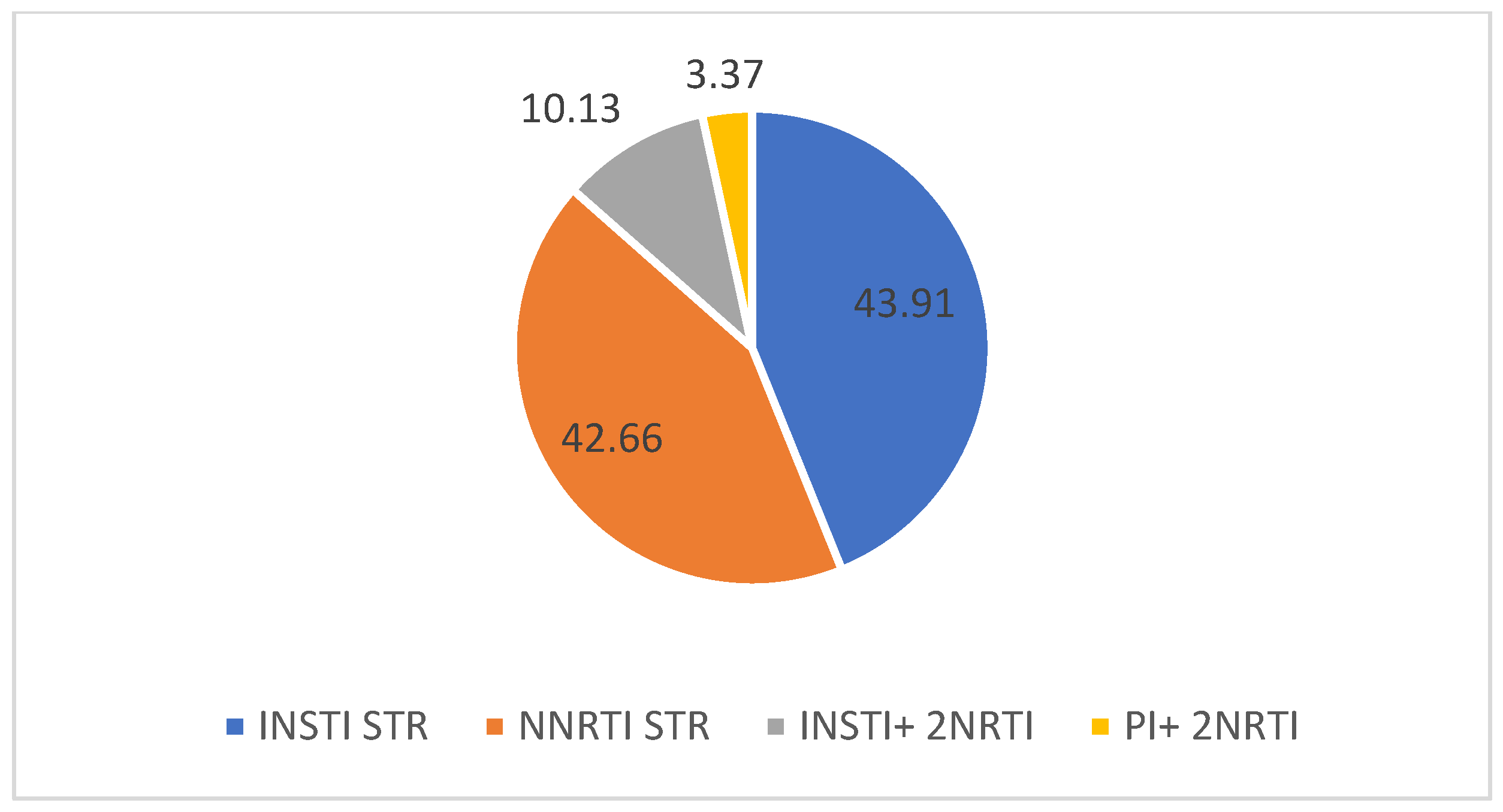
3.2. Antiretroviral Regimens
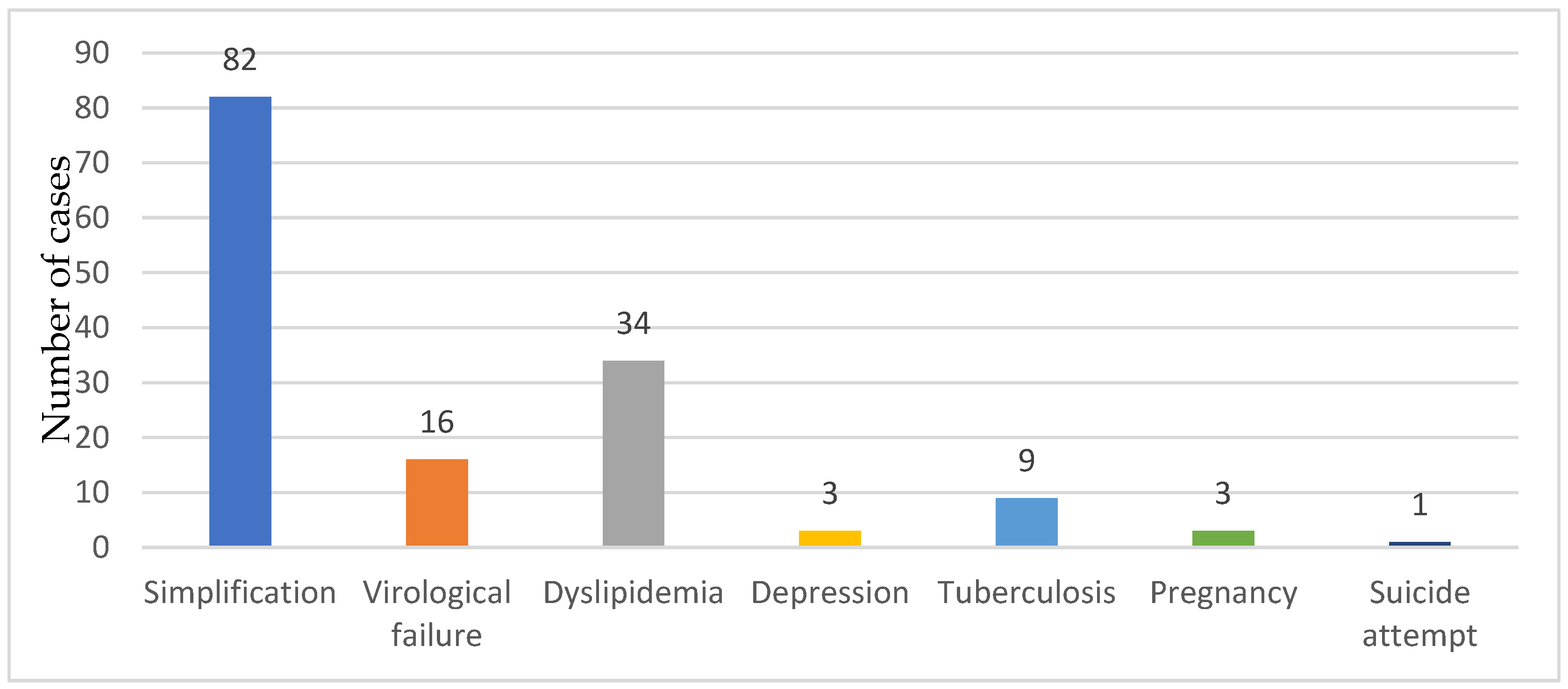
3.3. Switching Antiretroviral Therapy Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The ART-LINC of IeDEA Study Group. Switching to second-line antiretroviral therapy in resource-limited settings: Comparison of programmes with and without viral load monitoring. AIDS 2009, 23, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Wandel, S.; Colebunders, R.; Attia, S.; Furrer, H.; Egger, M.; IeDEA Southern and Central Africa. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: A systematic review and meta-analysis. Lancet Infect Dis. 2010, 10, 251–261. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Naito, T.; Mori, H.; Fujibayashi, K.; Fukushima, S.; Yuda, M.; Fukui, N.; Tsukamoto, S.; Suzuki, M.; Goto-Hirano, K.; Kuwatsuru, R. Analysis of antiretroviral therapy switch rate and switching pattern for people living with HIV from a national database in Japan. Sci. Rep. 2022, 12, 1732. [Google Scholar] [CrossRef] [PubMed]
- Kabarambi, A.; Balinda, S.; Abaasa, A.; Cogill, D.; Orrell, C. Determinants and reasons for switching anti-retroviral regimen among HIV-infected youth in a large township of South Africa (2002–2019). AIDS Res. Ther. 2022, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Chastain, D.; Badowski, M.; Huesgen, E.; Pandit, N.S.; Pallotta, A.; Michienzi, S. Optimizing Antiretroviral Therapy in Treatment-Experienced Patients Living with HIV: A Critical Review of Switch and Simplification Strategies. An Opinion of the HIV Practice and Research Network of the American College of Clinical Pharmacy. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2019, 18, 2325958219867325. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ruzicka, D.J.; Kuroishi, N.; Oshima, N.; Sakuma, R.; Naito, T. Switch rates, time-to-switch, and switch patterns of antiretroviral therapy in people living with human immunodeficiency virus in Japan, in a hospital-claim database. BMC Infect. Dis. 2019, 19, 505. [Google Scholar] [CrossRef] [PubMed]
- Nachega, J.B.; Uthman, O.A.; Anderson, J.; Peltzer, K.; Wampold, S.; Cotton, M.F.; Mills, E.J.; Ho, Y.-S.; Stringer, J.S.; McIntyre, J.A.; et al. Adherence to antiretroviral therapy during and after pregnancy in low-income, middle-income, and high-income countries: A systematic review and meta-analysis. AIDS 2012, 26, 2039–2052. [Google Scholar] [CrossRef]
- Lester, R.T.; Ritvo, P.; Mills, E.J.; Kariri, A.; Karanja, S.; Chung, M.H.; Jack, W.; Habyarimana, J.; Sadatsafavi, M.; Najafzadeh, M.; et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): A randomised trial. Lancet 2010, 376, 1838–1845. [Google Scholar] [CrossRef] [PubMed]
- Papot, E.; Kaplan, R.; Vitoria, M.; Polizzotto, M.N. Optimizing switching strategies to simplify antiretroviral therapy: The future of second-line from a public health perspective. AIDS 2021, 35 (Suppl. S2), S153–S163. [Google Scholar] [CrossRef]
- Watt, M.H.; Maman, S.; Golin, C.E.; Earp, J.A.; Eng, E.; Bangdiwala, S.I.; Jacobson, M. Factors associated with self-reported adherence to antiretroviral therapy in a Tanzanian setting. AIDS Care 2010, 22, 381–389. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, Y.; Wang, Q.; Liang, S.; Feng, C.; Yang, H.; Yu, H.; Yuan, D.; Yang, S. Effect of Switching Antiretroviral Treatment Regimen in Patients With Drug-Resistant HIV-1 Infection: Retrospective Observational Cohort Study. JMIR Public Health Surveill. 2022, 8, e33429. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Initiative for Paediatric HIV Education and Research (CIPHER) Global Cohort Collaboration. Incidence of switching to second-line antiretroviral therapy and associated factors in children with HIV: An international cohort collaboration. Lancet HIV 2019, 6, e105–e115, Erratum in Lancet HIV 2020, 7, e803. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alemu, K.D.; Moges, N.A.; Boneya, D.J.; Asrade, A.A.; Tsega, T.D.; Tewachew, A.S. Time to Switch to Second-Line Anti-Retroviral Treatment and Its Predictors Among HIV Infected Adults with Virological Failure in Northwest Ethiopia: A Retrospective Follow-Up Study. HIV/AIDS-Res. Palliat. Care 2022, 14, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Panel on Clinical Practices for Treatment of HIV Infection. Guidelines for the use of antiretroviral agents in HIV-infected adults and adolescents. Ann. Intern. Med. 1998, 128 Pt 2, 1079–1100. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.T.; Bedimo, R.; Hoy, J.F.; Landovitz, R.J.; Smith, D.M.; Eaton, E.F.; Lehmann, C.; Springer, S.A.; Sax, P.E.; Thompson, M.A.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society–USA Panel. JAMA-J. Am. Med. Assoc. 2023, 329, 63–84. [Google Scholar] [CrossRef]
- Rizzardini, G.; Overton, E.T.; Orkin, C.; Swindells, S.; Arasteh, K.; Górgolas Hernández-Mora, M.; Pokrovsky, V.; Girard, P.M.; Oka, S.; Andrade-Villanueva, J.F.; et al. Long-Acting Injectable Cabotegravir + Rilpivirine for HIV Maintenance Therapy: Week 48 Pooled Analysis of Phase 3 ATLAS and FLAIR Trials. J. Acquir. Immune Defic. Syndr. 2020, 85, 498–506. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Margolis, D.A.; Gonzalez-Garcia, J.; Stellbrink, H.-J.; Eron, J.J.; Yazdanpanah, Y.; Podzamczer, D.; Lutz, T.; Angel, J.B.; Richmond, G.J.; Clotet, B.; et al. Long-acting intramuscular cabotegravir and rilpivirine in adults with HIV-1 infection (LATTE-2): 96-week results of a randomised, open-label, phase 2b, non-inferiority trial. Lancet 2017, 390, 1499–1510. [Google Scholar] [CrossRef] [PubMed]
- Achhra, A.C.; Mwasakifwa, G.; Amin, J.; Boyd, M.A. Efficacy and safety of contemporary dual-drug antiretroviral regimens as first-line treatment or as a simplification strategy: A systematic review and meta-analysis. Lancet HIV 2016, 3, e351–e360. [Google Scholar] [CrossRef] [PubMed]
- Plum, P.E.; Maes, N.; Sauvage, A.S.; Frippiat, F.; Meuris, C.; Uurlings, F.; Lecomte, M.; Léonard, P.; Paquot, N.; Fombellida, K.; et al. Impact of switch from tenofovir disoproxil fumarate-based regimens to tenofovir alafenamide-based regimens on lipid profile, weight gain and cardiovascular risk score in people living with HIV. BMC Infect. Dis. 2021, 21, 910. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cohen, C. Low-level viremia in HIV-1 infection: Consequences and implications for switching to a new regimen. HIV Clin. Trials 2009, 10, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Baril, J.G.; Angel, J.B.; Gill, M.J.; Gathe, J.; Cahn, P.; van Wyk, J.; Walmsley, S. Dual Therapy Treatment Strategies for the Management of Patients Infected with HIV: A Systematic Review of Current Evidence in ARV-Naive or ARV-Experienced, Virologically Suppressed Patients. PLoS ONE 2016, 11, e0148231. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bronkhorst, E.; Hattingh, S.; Poka, M. Antiretroviral stewardship in a tertiary academic hospital: The need for a clinical pharmacist. Health SA 2023, 28, 2135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tuot, S.; Sim, J.W.; Nagashima-Hayashi, M.; Chhoun, P.; Teo, A.K.J.; Prem, K.; Yi, S. What are the determinants of antiretroviral therapy adherence among stable people living with HIV? A cross-sectional study in Cambodia. AIDS Res. Ther. 2023, 20, 47. [Google Scholar] [CrossRef] [PubMed]
- Lodi, S.; Günthard, H.F.; Gill, J.; Phillips, A.N.; Dunn, D.; Vu, Q.; Siemieniuk, R.; Garcia, F.; Logan, R.; Jose, S.; et al. Effectiveness of Transmitted Drug Resistance Testing Before Initiation of Antiretroviral Therapy in HIV-Positive Individuals. J. Acquir. Immune Defic. Syndr. 2019, 82, 314–320. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Iannone, V.; Passerotto, R.A.; Lamanna, F.; Steiner, R.J.; Lombardi, F.; Salvo, P.F.; Dusina, A.; Farinacci, D.; Borghetti, A.; Di Giambenedetto, S.; et al. Changes in Metabolic Profile in PLWHIV Switching to Doravirine-Based Regimen. Viruses 2023, 15, 1046. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. 2015. Available online: http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf (accessed on 1 April 2024).
- World Health Organization HIV/AIDS Programme. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Collins, S.E.; Grant, P.M.; Shafer, R.W. Modifying Antiretroviral Therapy in Virologically Suppressed HIV-1-Infected Patients. Drugs 2015, 76, 75–98. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Y.; Xiao, J.; Zhang, W.; Han, N.; Yang, D.; Liu, W.; Zeng, H.; Han, J.; Zhao, H. Cumulative effects of hypertriglyceridemia in HIV-infected patients switching from NNRTIs to PI-based antiretroviral therapy. J. Infect. Dev. Ctries. 2022, 16, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, S.S.; Locascio, J.J.; Misra, V.; Lorenz, D.R.; Holman, A.; Dutta, A.; Penugonda, S.; Wolinsky, S.M.; Gabuzda, D. Lipid profiles and APOE4 allele impact midlife cognitive decline in HIV-infected men on antiretroviral therapy. Clin. Infect. Dis. 2016, 63, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Esser, S.; Eisele, L.; Schwarz, B.; Schulze, C.; Holzendorf, V.; Brockmeyer, N.H.; Hower, M.; Kwirant, F.; Rudolph, R.; Neumann, T.; et al. Rates of cardiovascular events and deaths are associated with advanced stages of HIV-infection: Results of the HIV HEART study 7, 5-year follow-up. J. Int. AIDS Soc. 2014, 17, 19542. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With Switch | Without Switch | p | |||
| Age (Years) | n (148) | % | n (1562) | % | |
| 20–29 | 20 | 13.5 | 260 | 16.6 | p < 0.00001 |
| 30–39 | 85 | 57.4 | 473 | 30.3 | |
| 40–49 | 19 | 12.8 | 387 | 24.8 | |
| 50–59 | 17 | 11.5 | 344 | 22.0 | |
| Over 60 | 7 | 4.8 | 98 | 6.3 | |
| Laboratory Marker | Value | Before Switch | After Switch | |||
|---|---|---|---|---|---|---|
| N (148) | % | N (148) | % | p | ||
| ALT | normal | 113 | 76.4 | 135 | 91.2 | 0.0005 |
| elevated | 35 | 23.6 | 13 | 8.8 | ||
| AST | normal | 113 | 76.4 | 135 | 91.2 | 0.0005 |
| elevated | 35 | 23.6 | 13 | 8.8 | ||
| GGT | normal | 117 | 79.1 | 131 | 88.5 | 0.028 |
| elevated | 31 | 20.9 | 17 | 11.5 | ||
| Total cholesterol | normal | 94 | 63.5 | 112 | 75.7 | 0.023 |
| elevated | 54 | 36.5 | 36 | 24.3 | ||
| HDL-col | normal | 101 | 68.24 | 112 | 75.67 | 0.15 |
| elevated | 47 | 31.75 | 36 | 24.32 | ||
| LDL-col | normal | 99 | 66.89 | 112 | 75.67 | 0.095 |
| elevated | 49 | 33.10 | 36 | 24.32 | ||
| Triglycerides | normal | 97 | 65.5 | 121 | 81.75 | 0.001 |
| elevated | 51 | 34.5 | 27 | 18.24 | ||
| ART Regimen | N (148) | % |
|---|---|---|
| Protease inhibitors + 2 NRTI (more than one pill) | 84 | 56.7 |
| Non-nucleoside reverse transcriptase inhibitor + 2 NRTI (more than one pill) | 37 | 25 |
| Integrase inhibitors + 2 NRTI (more than one pill) | 13 | 8.7 |
| Other | 14 | 9.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loghin, I.I.; Rusu, Ș.A.; Vâţă, A.; Cobaschi, M.; Cecan, I.; Manciuc, C.; Dorobăţ, C.M. Antiretroviral Therapy Switch in HIV-Infected Adults from a Regional HIV/AIDS Center in NE Romania. Medicina 2024, 60, 854. https://doi.org/10.3390/medicina60060854
Loghin II, Rusu ȘA, Vâţă A, Cobaschi M, Cecan I, Manciuc C, Dorobăţ CM. Antiretroviral Therapy Switch in HIV-Infected Adults from a Regional HIV/AIDS Center in NE Romania. Medicina. 2024; 60(6):854. https://doi.org/10.3390/medicina60060854
Chicago/Turabian StyleLoghin, Isabela Ioana, Șerban Alin Rusu, Andrei Vâţă, Mihaela Cobaschi, Ion Cecan, Carmen Manciuc, and Carmen Mihaela Dorobăţ. 2024. "Antiretroviral Therapy Switch in HIV-Infected Adults from a Regional HIV/AIDS Center in NE Romania" Medicina 60, no. 6: 854. https://doi.org/10.3390/medicina60060854
APA StyleLoghin, I. I., Rusu, Ș. A., Vâţă, A., Cobaschi, M., Cecan, I., Manciuc, C., & Dorobăţ, C. M. (2024). Antiretroviral Therapy Switch in HIV-Infected Adults from a Regional HIV/AIDS Center in NE Romania. Medicina, 60(6), 854. https://doi.org/10.3390/medicina60060854