
Comparison of Integrase Strand Transfer Inhibitors (INSTIs) and Protease-Boosted Inhibitors (PIs) on the Reduction in Chronic Immune Activation in a Virally Suppressed, Mainly Male Population Living with HIV (PLWH)

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Study Time Points and Data Collection
2.4. Outcomes
2.5. Methods for Determining the Measured Plasma Biomarkers
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Included Participants (PLWH), which Were Collected from Their Medical Records (during the Recruitment Visit)
3.2. Primary Analysis/Outcome of Interest
3.3. Secondary Analyses
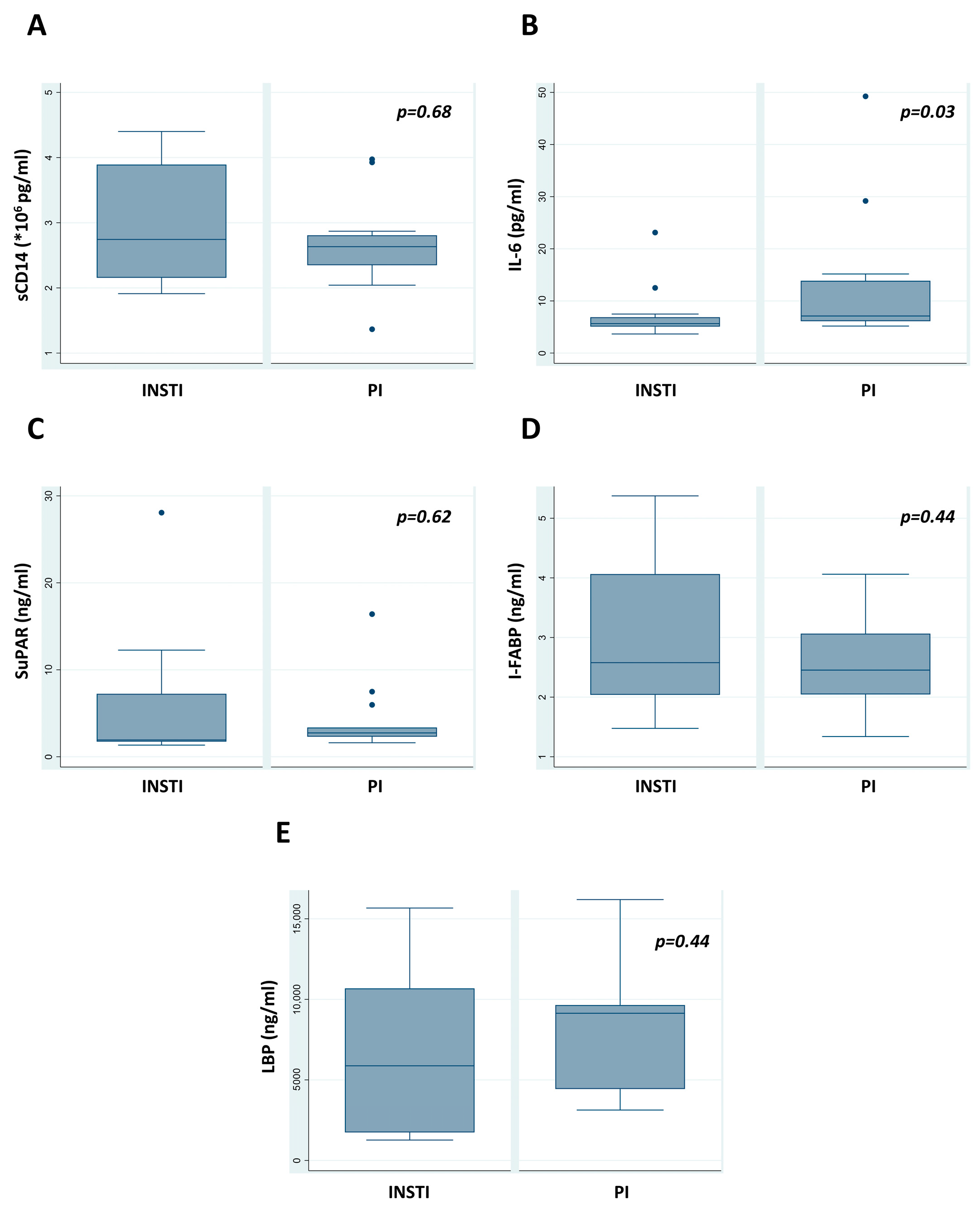
3.3.1. Comparison of Resting Immune Parameters during the Recruitment Visit
3.3.2. Comparison of Metabolic Parameters during the Recruitment Visit
3.3.3. Comparison of Longitudinal Laboratory Immune Parameters
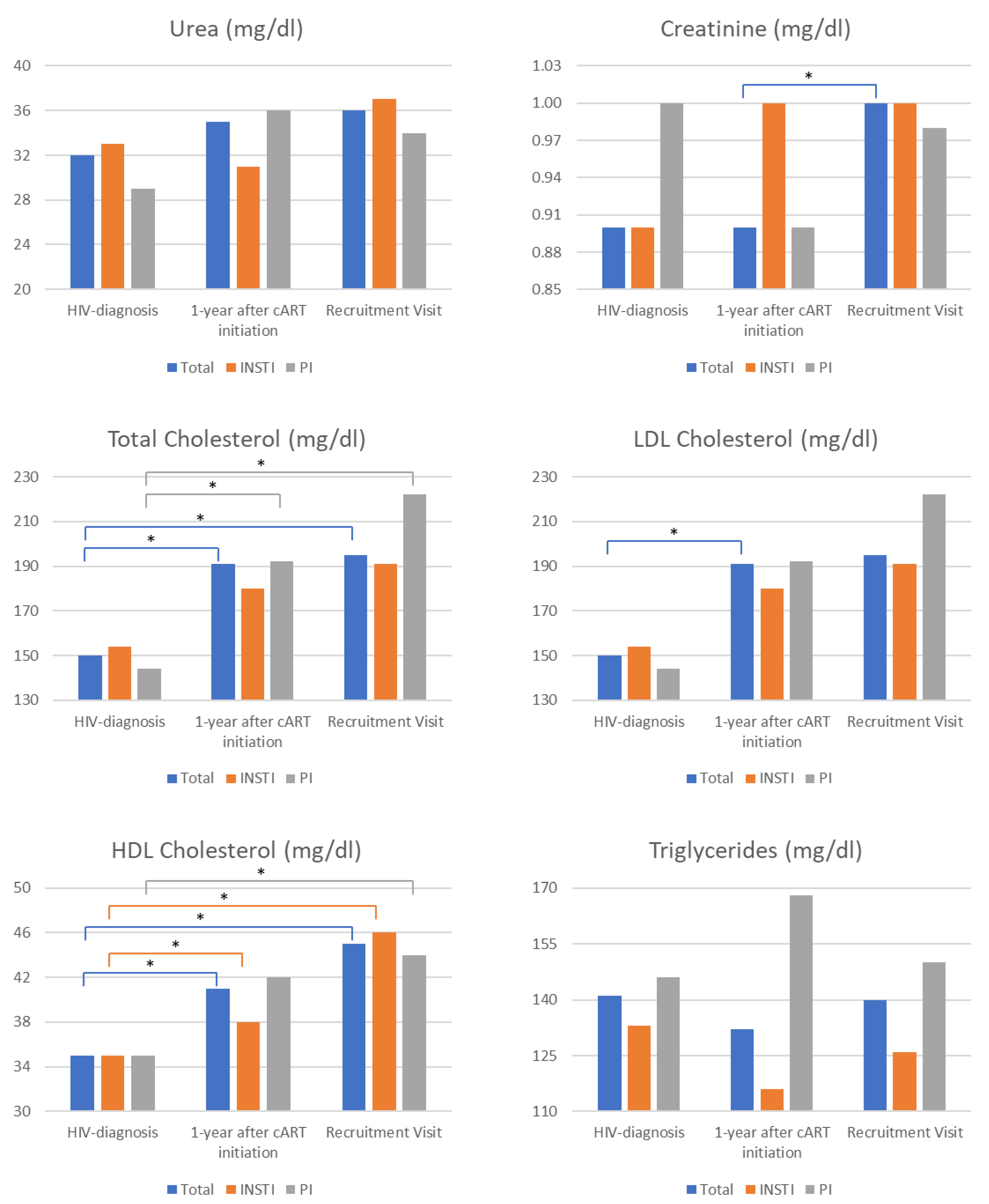
3.3.4. Comparison of Longitudinal Laboratory Metabolic Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Assimakopoulos, S.F.; Dimitropoulou, D.; Marangos, M.; Gogos, C.A. Intestinal barrier dysfunction in HIV infection: Pathophysiology, clinical implications and potential therapies. Infection 2014, 42, 951–959. [Google Scholar] [CrossRef]
- Hileman, C.O.; Funderburg, N.T. Inflammation, Immune Activation, and Antiretroviral Therapy in HIV. Curr. HIV/AIDS Rep. 2017, 14, 93–100. [Google Scholar] [CrossRef]
- McGettrick, P.; Tinago, W.; O’Brien, J.; Miles, S.; Lawler, L.; Garcia-Leon, A.; Mahon, N.; Lambert, J.; Sheehan, G.; Landay, A.; et al. Distinct Inflammatory Phenotypes are associated with subclinical and clinical Cardiovascular disease in People living with HIV. J. Infect. Dis. 2024, jiae007. [Google Scholar] [CrossRef]
- Ghosh, S.S.; Wang, J.; Yannie, P.J.; Ghosh, S. Intestinal Barrier Dysfunction, LPS Translocation, and Disease Development. J. Endocr. Soc. 2020, 4, bvz039. [Google Scholar] [CrossRef]
- Hoenigl, M.; Moser, C.B.; Funderburg, N.; Bosch, R.; Kantor, A.; Zhang, Y.; Eugen-Olsen, J.; Finkelman, M.; Reiser, J.; Landay, A.; et al. Soluble Urokinase Plasminogen Activator Receptor Is Predictive of Non-AIDS Events During Antiretroviral Therapy-mediated Viral Suppression. Clin. Infect. Dis. 2019, 69, 676–686. [Google Scholar] [CrossRef]
- Nakagawa, F.; May, M.; Phillips, A. Life expectancy living with HIV: Recent estimates and future implications. Curr. Opin. Infect. Dis. 2013, 26, 17–25. [Google Scholar] [CrossRef]
- McGettrick, P.; Mallon, P.W.G. Biomarkers to predict cardiovascular disease in people living with HIV. Curr. Opin. Infect. Dis. 2022, 35, 15–20. [Google Scholar] [CrossRef]
- Sukumaran, L.; Kunisaki, K.M.; Bakewell, N.; Winston, A.; Mallon, P.W.G.; Doyle, N.; Anderson, J.; Boffito, M.; Haddow, L.; Post, F.A.; et al. Association between inflammatory biomarker profiles and cardiovascular risk in individuals with and without HIV. AIDS 2023, 37, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Hope, T.J.; Richman, D.D.; Stevenson, M. Encyclopedia of AIDS; Springer: New York, NY, USA, 2018. [Google Scholar]
- Jaworowski, A.; Hearps, A.C.; Angelovich, T.A.; Hoy, J.F. How Monocytes Contribute to Increased Risk of Atherosclerosis in Virologically-Suppressed HIV-Positive Individuals Receiving Combination Antiretroviral Therapy. Front. Immunol. 2019, 10, 1378. [Google Scholar] [CrossRef]
- Lederman, M.M.; Funderburg, N.T.; Sekaly, R.P.; Klatt, N.R.; Hunt, P.W. Residual immune dysregulation syndrome in treated HIV infection. Adv. Immunol. 2013, 119, 51–83. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.W.; Sereti, I. Residual immune dysfunction under antiretroviral therapy. Semin. Immunol. 2021, 51, 101471. [Google Scholar] [CrossRef]
- Michelini, Z.; Baroncelli, S.; Fantauzzi, A.; Pasquale, C.; Galluzzo, C.M.; Sanchez, M.; Gatto, M.; Amici, R.; Franco, M.; d’Ettorre, G.; et al. Reduced Plasma Levels of sCD14 and I-FABP in HIV-infected Patients with Mesalazine-treated Ulcerative Colitis. HIV Clin. Trials 2016, 17, 49–54. [Google Scholar] [CrossRef]
- Kelesidis, T.; Tran, T.T.; Stein, J.H.; Brown, T.T.; Moser, C.; Ribaudo, H.J.; Dube, M.P.; Murphy, R.; Yang, O.O.; Currier, J.S.; et al. Changes in Inflammation and Immune Activation With Atazanavir-, Raltegravir-, Darunavir-Based Initial Antiviral Therapy: ACTG 5260s. Clin Infect. Dis. 2015, 61, 651–660. [Google Scholar] [CrossRef]
- Hellmuth, J.; Slike, B.M.; Sacdalan, C.; Best, J.; Kroon, E.; Phanuphak, N.; Fletcher, J.L.K.; Prueksakaew, P.; Jagodzinski, L.L.; Valcour, V.; et al. Very Early Initiation of Antiretroviral Therapy During Acute HIV Infection Is Associated With Normalized Levels of Immune Activation Markers in Cerebrospinal Fluid but Not in Plasma. J. Infect. Dis. 2019, 220, 1885–1891. [Google Scholar] [CrossRef]
- Neff, C.P.; Krueger, O.; Xiong, K.; Arif, S.; Nusbacher, N.; Schneider, J.M.; Cunningham, A.W.; Armstrong, A.; Li, S.; McCarter, M.D.; et al. Fecal Microbiota Composition Drives Immune Activation in HIV-infected Individuals. eBioMedicine 2018, 30, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Uciechowski, P.; Dempke, W.C.M. Interleukin-6: A Masterplayer in the Cytokine Network. Oncology 2020, 98, 131–137. [Google Scholar] [CrossRef]
- Ward, A.R.; Mota, T.M.; Jones, R.B. Immunological approaches to HIV cure. Semin. Immunol. 2021, 51, 101412. [Google Scholar] [CrossRef]
- Velissaris, D.; Dimopoulos, G.; Parissis, J.; Alexiou, Z.; Antonakos, N.; Babalis, D.; Gerakari, S.; Kaldis, V.; Koutoukas, P.; Lada, M.; et al. Prognostic Role of Soluble Urokinase Plasminogen Activator Receptor at the Emergency Department: A Position Paper by the Hellenic Sepsis Study Group. Infect. Dis. Ther. 2020, 9, 407–416. [Google Scholar] [CrossRef] [PubMed]
- de Vos, W.M.; Tilg, H.; Van Hul, M.; Cani, P.D. Gut microbiome and health: Mechanistic insights. Gut 2022, 71, 1020–1032. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Takeuchi, S.; Kubota, K.; Kobayashi, Y.; Kozakai, S.; Ukai, I.; Shichiku, A.; Okubo, M.; Numasaki, M.; Kanemitsu, Y.; et al. Lipopolysaccharide (LPS)-binding protein stimulates CD14-dependent Toll-like receptor 4 internalization and LPS-induced TBK1-IKKϵ-IRF3 axis activation. J. Biol. Chem. 2018, 293, 10186–10201. [Google Scholar] [CrossRef]
- Monnig, M.A.; Cohen, R.; Ramratnam, B.; McAdams, M.; Tashima, K.; Monti, P.M. HIV Infection, HCV Coinfection, and Alcohol Use: Associations with Microbial Translocation and Immune Activation. Alcohol. Clin. Exp. Res. 2019, 43, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.K.; Kim, S.J.; Rah, S.H.; Kang, J.I.; Jung, H.E.; Lee, D.; Lee, H.K.; Lee, J.O.; Park, B.S.; Yoon, T.Y.; et al. Reconstruction of LPS Transfer Cascade Reveals Structural Determinants within LBP, CD14, and TLR4-MD2 for Efficient LPS Recognition and Transfer. Immunity 2017, 46, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Mehraj, V.; Vyboh, K.; Cao, W.; Li, T.; Routy, J.P. CD4:CD8 ratio as a frontier marker for clinical outcome, immune dysfunction and viral reservoir size in virologically suppressed HIV-positive patients. J. Int. AIDS Soc. 2015, 18, 20052. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Assessment | HIV Diagnosis | Recruitment Visit |
|---|---|---|
| Selection Criteria | ✓ | |
| Medical History | ✓ | |
| Clinical Examination | ✓ |
| HIV Diagnosis | Recruitment Visit | |
|---|---|---|
| CD4+ | ✓ | ✓ |
| CD8+ | ✓ | ✓ |
| CD4+/CD8+ | ✓ | ✓ |
| NK cells | ✓ | ✓ |
| HIV RNA copies/ml | ✓ | ✓ |
| Glucose | ✓ | ✓ |
| Urea/creatinine | ✓ | ✓ |
| Cholesterol | ✓ | ✓ |
| Liver function | ✓ | ✓ |
| Uric acid | ✓ | ✓ |
| sCD14 | ✓ | |
| IL-6 | ✓ | |
| SuPAR | ✓ | |
| I-FABP | ✓ | |
| LBP | ✓ |
| Assessment | Overall | INSTIs | PIs | p-Value |
|---|---|---|---|---|
| n | 28 | 15 | 13 | - |
| Males | 26 (93) | 15 (100) | 11 (85) | 0.21 |
| Age | 52 (32–70) | 52 (32–67) | 53 (33–70) | 0.47 |
| BMI | 25 (13–39) | 29 (25–39) | 22 (13–29) | 0.01 |
| Ethnicity | 0.27 | |||
| European | 27 (96) | 15 (100) | 12 (92) | |
| African | 1 (4) | 0 (0) | 1 (8) | |
| Greek nationality | 25 (89) | 15 (100) | 10 (77) | 0.09 |
| MSM | 19 (70) | 11 (79) | 8 (62) | 0.42 |
| Sexual practices | 0.64 | |||
| Heterosexual | 8 (30) | 3 (21) | 5 (38) | |
| Homosexual | 16 (59) | 9 (64) | 7 (54) | |
| Bisexual | 3 (11) | 2 (14) | 1 (8) | |
| Years from HIV diagnosis to recruitment visit | 7 (1–21) | 7 (1–15) | 7 (2–21) | 0.93 |
| Disease stage at diagnosis | 0.003 | |||
| A1 | 4 (14) | 4 (27) | 0 (0) | |
| A2 | 8 (29) | 7 (46) | 1 (8) | |
| B1 | 2 (7) | 1 (7) | 1 (8) | |
| B3 | 5 (18) | 2 (13) | 3 (23) | |
| C3 | 9 (32) | 1 (7) | 8 (61) | |
| AIDS or infection at diagnosis | 9 (32) | 1 (7) | 8 (62) | 0.004 |
| STIs at diagnosis | 8 (29) | 5 (33) | 3 (23) | 0.69 |
| Smoking at diagnosis | 0.006 | |||
| Never | 15 (54) | 7 (47) | 8 (62) | |
| Past | 6 (21) | 1 (6) | 5 (38) | |
| Current | 7 (25) | 7 (47) | (0) | |
| Alcohol at diagnosis | 0.06 | |||
| Never | 17 (61) | 7 (47) | 10 (77) | |
| Little | 8 (28) | 7 (47) | 1 (8) | |
| Moderate | 3 (11) | 1 (6) | 2 (15) | |
| Hypertension stage | 1.00 | |||
| High normal | 3 (11) | 2 (13) | 1 (8) | |
| Stage 1 | 2 (7) | 1 (7) | 1 (8) | |
| Stage 2 | 1 (4) | 1 (7) | 0 (0) | |
| Diabetes | 0.40 | |||
| Prediabetes | 7 (25) | 5 (33) | 2 (15) | |
| Diabetes | 1 (4) | 0 (0) | 1 (8) | |
| Coronary artery disease | 1 (4) | 1 (7) | 0 (0) | 1.00 |
| Laboratory tests at diagnosis | ||||
| CD4+ (cells/µL) | 222 (1–877) | 397 (47–877) | 64 (1–629) | <0.001 |
| CD8+ (cells/µL) | 881 (50–8770) | 1190 (563–8770) | 365 (50–1648) | 0.002 |
| CD4/CD8 ratio | 0.19 (0.01–1.25) | 0.25 (0.04–1.25) | 0.11 (0.01–1.00) | 0.04 |
| NK (cells/µL) | 131 (6–623) | 134 (38–623) | 102 (6–286) | 0.37 |
| HIV RNA (copies/mL) | 97,763 (240–11 × 106) | 65,800 (3500–11 × 106) | 211,100 (240–5.4 × 106) | 0.36 |
| Urea (mg/dL) | 32 (14–56) | 33 (26–56) | 29 (14–51) | 0.18 |
| Creatinine (mg/dL) | 0.9 (0.6–1.2) | 0.9 (0.7–1.2) | 1.0 (0.6–1.2) | 0.69 |
| Total cholesterol (mg/dL) | 150 (79–255) | 154 (100–255) | 144 (79–212) | 0.27 |
| LDL cholesterol (mg/dL) | 107 (31–178) | 96 (40–178) | 111 (31–148) | 0.93 |
| HDL cholesterol (mg/dL) | 35 (15–57) | 35 (15–47) | 35 (27–57) | 0.91 |
| Triglycerides (mg/dL) | 141 (46–282) | 133 (46–282) | 146 (87–177) | 0.71 |
| ALT (IU/L) | 24 (7–359) | 24 (10–359) | 21 (7–108) | 0.38 |
| AST (IU/L) | 23 (15–295) | 25 (15–295) | 20 (15–57) | 0.34 |
| gGT (IU/L) | 27 (4–112) | 27 (4–112) | 26 (13–73) | 0.67 |
| ALP (IU/L) | 77 (45–325) | 77 (47–325) | 77 (45–153) | 0.62 |
| Total bilirubin (mg/dL) | 0.38 (0.17–1.36) | 0.38 (0.17–1.36) | 0.40 (0.27–1.10) | 0.88 |
| Uric acid (mg/dL) | 4.8 (3.6–7.5) | 5.5 (3.9–7.3) | 4.7 (3.6–7.5) | 0.86 |
| Assessment | Overall n = 28 | INSTIs n = 15 | PIs n = 13 | p-Value |
|---|---|---|---|---|
| CD4+ (cells/µL) | 665 (351–2143) | 726 (383–2143) | 495 (351–988) | 0.01 |
| CD8+ (cells/µL) | 895 (292–1984) | 882 (445–1984) | 908 (292–1870) | 0.96 |
| CD4+/CD8+ ratio | 0.73 (0.24–2.43) | 0.99 (0.28–2.43) | 0.53 (0.24–2.22) | 0.07 |
| NK (cells/µL) | 288 (92–844) | 265 (92–844) | 336 (113–569) | 0.79 |
| HIV RNA (copies/mL) | 20 (20–40) | 20 (20–37) | 20 (20–40) | 0.22 |
| Urea (mg/dL) | 36 (17–66) | 37 (26–56) | 34 (17–66) | 0.26 |
| Creatinine (mg/dL) | 1.0 (0.6–1.9) | 1.0 (0.8–1.3) | 0.98 (0.6–1.9) | 0.66 |
| Total cholesterol (mg/dL) | 195 (127–302) | 191 (127–246) | 222 (156–302) | 0.005 |
| LDL cholesterol (mg/dL) | 121 (73–186) | 104 (73–153) | 140 (93–186) | 0.002 |
| HDL cholesterol (mg/dL) | 45 (29–74) | 46 (30–74) | 44 (29–65) | 0.60 |
| Triglycerides (mg/dL) | 140 (49–398) | 126 (49–275) | 150 (85–398) | 0.13 |
| Glucose (mg/dL) | 98 (66–175) | 106 (66–133) | 96 (73–175) | 0.47 |
| ALT (IU/L) | 21 (10–90) | 28 (10–90) | 17 (12–88) | 0.22 |
| AST (IU/L) | 22 (13–63) | 27 (15–63) | 20 (13–33) | 0.09 |
| gGT (IU/L) | 24 (6–178) | 29 (6–178) | 23 (17–87) | 1.00 |
| ALP (IU/L) | 76 (37–131) | 69 (37–131) | 82 (58–131) | 0.21 |
| Total bilirubin (mg/dL) | 0.50 (0.21–1.28) | 0.70 (0.21–1.28) | 0.47 (0.24–1.23) | 0.39 |
| Uric acid (mg/dL) | 6.0 (3.8–9.3) | 5.6 (3.8–9.3) | 6.1 (3.8–9.1) | 0.95 |
| sCD14 (×106 pg/mL) | 2.64 (1.37–4.40) | 2.74 (1.91–4.40) | 2.63 (1.37–3.97) | 0.68 |
| IL-6 (pg/mL) | 6.29 (3.66–49.24) | 5.65 (3.66–23.12) | 7.11 (5.18–49.24) | 0.03 |
| SuPAR (ng/mL) | 2.52 (1.34–28.07) | 1.93 (1.34–28.07) | 2.74 (1.61–16.40) | 0.62 |
| I-FABP (ng/mL) | 2.52 (1.34–5.38) | 2.58 (1.48–5.38) | 2.45 (1.34–4.06) | 0.44 |
| LBP (ng/mL) | 7677.9 (1265.5–16,193) | 5875.1 (1265.5–15,667.5) | 9137.7 (3129.4–16,193) | 0.44 |
| Assessment | Overall n = 28 | INSTIs n = 15 | PIs n = 13 | p-Value |
|---|---|---|---|---|
| sCD14 (×106 pg/mL) (<1.1) | 0 (0) | 0 (0) | 0 (0) | NA |
| IL-6 (pg/mL) (<0.8) | 0 (0) | 0 (0) | 0 (0) | NA |
| SuPAR (ng/mL) (<3) | 18 (64) | 9 (60) | 9 (69) | 0.71 |
| I-FABP (ng/mL) (<2.1) | 9 (32) | 4 (27) | 5 (38) | 0.69 |
| LBP (ng/mL) (<1700) | 5 (18) | 5 (33) | 0 (0) | 0.04 |
| Assessment | Overall n = 28 | INSTIs n = 15 | PIs n = 13 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HIV Diagnosis | Recruitment Visit | p | HIV Diagnosis | Recruitment Visit | p | HIV Diagnosis | Recruitment Visit | p-Value | |
| CD4+ (cells/µL) | 222 (1–877) | 665 (351–2143) | <0.001 | 397 (47–877) | 726 (383–2143) | <0.001 | 64 (1–629) | 495 (351–988) | <0.001 |
| CD8+ (cells/µL) | 881 (50–8770) | 895 (292–1984) | 0.88 | 1190 (563–8770) | 882 (445–1984) | 0.01 | 365 (50–1648) | 908 (292–1870) | 0.07 |
| CD4+/CD8+ ratio | 0.19 (0.01–1.25) | 0.73 (0.24–2.43) | <0.001 | 0.25 (0.04–1.25) | 0.99 (0.28–2.43) | <0.001 | 0.11 (0.01–1.00) | 0.53 (0.24–2.22) | <0.001 |
| NK (cells/µL) | 131 (6–623) | 288 (92–844) | <0.001 | 134 (38–623) | 265 (92–844) | 0.002 | 102 (6–286) | 336 (113–569) | 0.003 |
| HIV RNA (copies/mL) | 97,763 (240–11 × 106) | 20 (20–40) | <0.001 | 65,800 (3500–11 × 106) | 20 (20–37) | <0.001 | 211,100 (240–5.4 × 106) | 20 (20–40) | <0.001 |
| ALT (IU/L) | 24 (7–359) | 21 (10–90) | 0.09 | 24 (10–359) | 28 (10–90) | 0.31 | 21 (7–108) | 17 (12–88) | 0.15 |
| AST (IU/L) | 23 (15–295) | 22 (13–63) | 0.36 | 25 (15–295) | 27 (15–63) | 0.69 | 20 (15–57) | 20 (13–33) | 0.26 |
| gGT (IU/L) | 27 (4–112) | 24 (6–178) | 0.65 | 27 (4–112) | 29 (6–178) | 0.94 | 26 (13–73) | 23 (17–87) | 0.51 |
| ALP (IU/L) | 77 (45–325) | 76 (37–131) | 0.43 | 77 (47–325) | 69 (37–131) | 0.11 | 77 (45–153) | 82 (58–131) | 0.37 |
| Total bilirubin (mg/dL) | 0.38 (0.17–1.36) | 0.50 (0.21–1.28) | 0.22 | 0.38 (0.17–1.36) | 0.70 (0.21–1.28) | 0.41 | 0.40 (0.27–1.10) | 0.47 (0.24–1.23) | 0.34 |
| Uric acid (mg/dL) | 4.8 (3.6–7.5) | 6.0 (3.8–9.3) | <0.001 | 5.5 (3.9–7.3) | 5.6 (3.8–9.3) | 0.002 | 4.7 (3.6–7.5) | 6.1 (3.8–9.1) | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitsotolis, T.; Kyriakoulis, K.G.; Kollias, A.; Papalexandrou, A.; Kalampoka, H.; Mastrogianni, E.; Basoulis, D.; Psichogiou, M. Comparison of Integrase Strand Transfer Inhibitors (INSTIs) and Protease-Boosted Inhibitors (PIs) on the Reduction in Chronic Immune Activation in a Virally Suppressed, Mainly Male Population Living with HIV (PLWH). Medicina 2024, 60, 331. https://doi.org/10.3390/medicina60020331
Nitsotolis T, Kyriakoulis KG, Kollias A, Papalexandrou A, Kalampoka H, Mastrogianni E, Basoulis D, Psichogiou M. Comparison of Integrase Strand Transfer Inhibitors (INSTIs) and Protease-Boosted Inhibitors (PIs) on the Reduction in Chronic Immune Activation in a Virally Suppressed, Mainly Male Population Living with HIV (PLWH). Medicina. 2024; 60(2):331. https://doi.org/10.3390/medicina60020331
Chicago/Turabian StyleNitsotolis, Thomas, Konstantinos G. Kyriakoulis, Anastasios Kollias, Alexia Papalexandrou, Helen Kalampoka, Elpida Mastrogianni, Dimitrios Basoulis, and Mina Psichogiou. 2024. "Comparison of Integrase Strand Transfer Inhibitors (INSTIs) and Protease-Boosted Inhibitors (PIs) on the Reduction in Chronic Immune Activation in a Virally Suppressed, Mainly Male Population Living with HIV (PLWH)" Medicina 60, no. 2: 331. https://doi.org/10.3390/medicina60020331
APA StyleNitsotolis, T., Kyriakoulis, K. G., Kollias, A., Papalexandrou, A., Kalampoka, H., Mastrogianni, E., Basoulis, D., & Psichogiou, M. (2024). Comparison of Integrase Strand Transfer Inhibitors (INSTIs) and Protease-Boosted Inhibitors (PIs) on the Reduction in Chronic Immune Activation in a Virally Suppressed, Mainly Male Population Living with HIV (PLWH). Medicina, 60(2), 331. https://doi.org/10.3390/medicina60020331