
Rituximab in the Management of Autoimmune Bullous Diseases: A Treatment-Resistant Case Series from a Single Central European Referral Center

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
- -
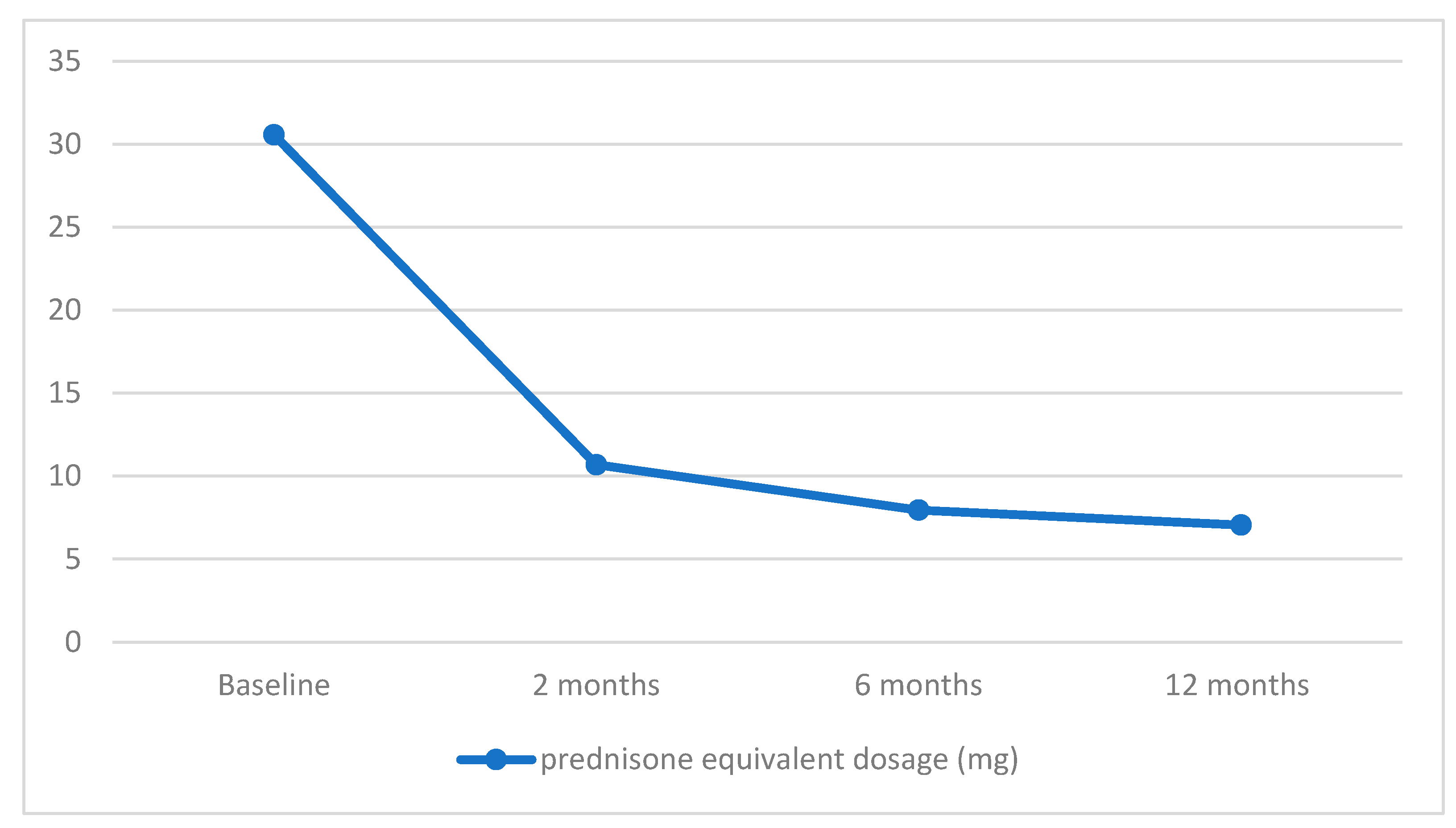
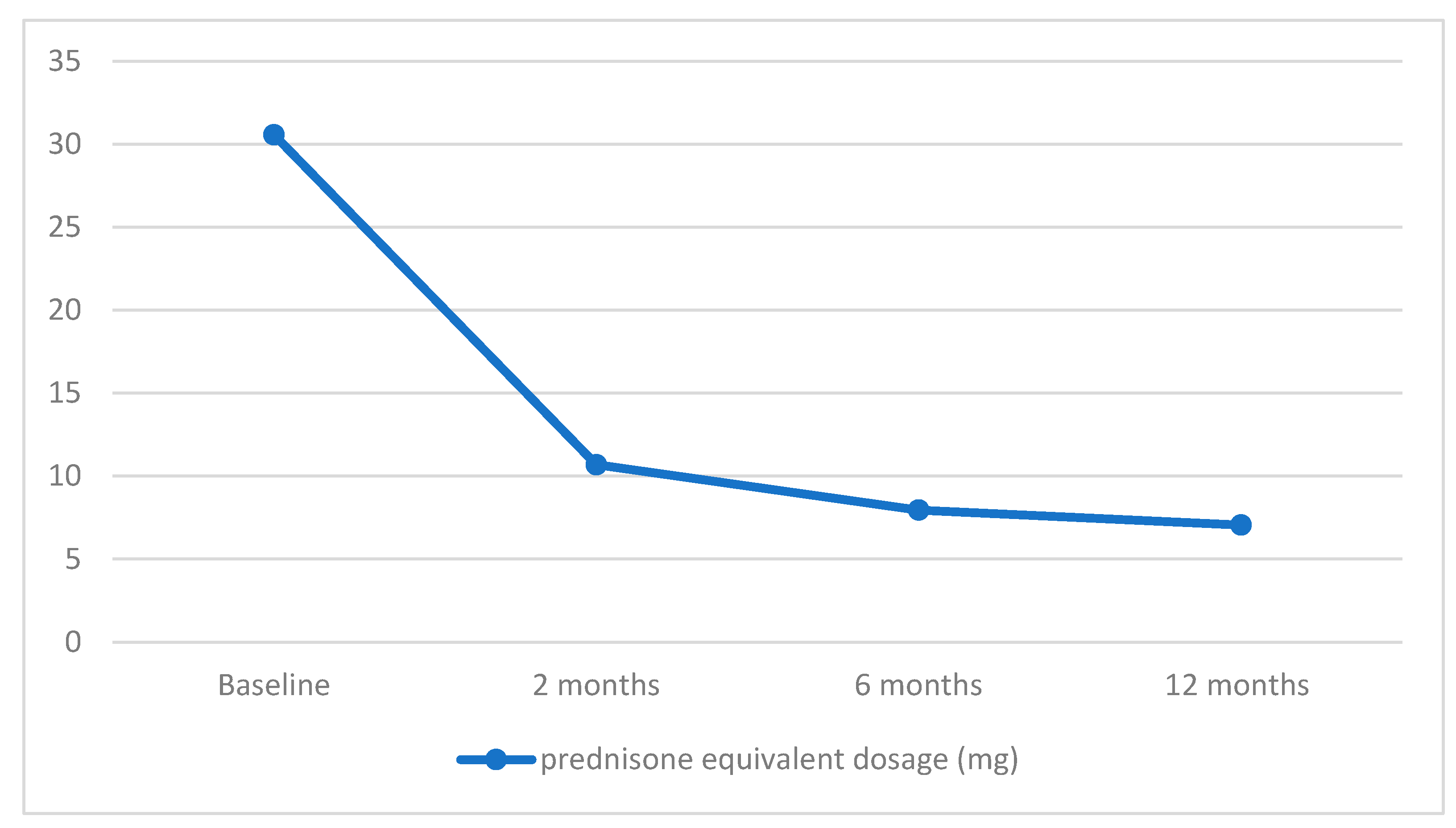
- Patients with a prednisolone equivalent dosage below 10 mg/day before their initial RTX infusion, with the exclusion of those with absolute contraindications to GCS;
- -
- Individuals presenting with less than 10 active lesions (encompassing blisters, erosions, or new areas of erythema) prior to their initial RTX infusion;
- -
- Subjects lacking follow-up data for at least one year after completing the last RTX cycle;
- -
- Individuals with a history of hypersensitivity reactions to the administered medication;
- -
- Subjects with active and severe infections;
- -
- Patients diagnosed with severe congestive heart failure (New York Heart Association Class IV).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dmochowski, M.; Jałowska, M.; Bowszyc-Dmochowska, M. Issues Occupying Our Minds: Nomenclature of Autoimmune Blistering Diseases Requires Updating, Pemphigus Vulgaris Propensity to Affect Areas Adjacent to Natural Body Orifices Unifies Seemingly Diverse Clinical Features of This Disease. Front. Immunol. 2022, 13, 1103375. [Google Scholar] [CrossRef] [PubMed]
- Jałowska, M.; Gornowicz-Porowska, J.; Bowszyc-Dmochowska, M.; Dmochowski, M. Sacral Dimple, Conjunctiva, and Nipple as Less Obvious Pemphigus Vulgaris Locations around Natural Body Orifices: A Report of Three Cases. J. Clin. Med. 2022, 11, 2855. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, T.; Waschke, J. Autoantibody-Specific Signalling in Pemphigus. Front. Med. 2021, 8, 701809. [Google Scholar] [CrossRef] [PubMed]
- Szymański, K.M.; Kowalewski, C.; Pietrzyk, E.; Woźniak, K. Case Report: Biological Treatment of Epidermolysis Bullosa Acquisita: Report on Four Cases and Literature Review. Front. Immunol. 2023, 14, 1214011. [Google Scholar] [CrossRef]
- Iwata, H.; Vorobyev, A.; Koga, H.; Recke, A.; Zillikens, D.; Prost-Squarcioni, C.; Ishii, N.; Hashimoto, T.; Ludwig, R.J. Meta-Analysis of the Clinical and Immunopathological Characteristics and Treatment Outcomes in Epidermolysis Bullosa Acquisita Patients. Orphanet J. Rare Dis. 2018, 13, 153. [Google Scholar] [CrossRef]
- Fan, B.; Wang, M. Treatment of Recurrent Epidermolysis Bullosa Acquisita with Tofacitinib. JAMA Dermatol. 2023, 159, 342–344. [Google Scholar] [CrossRef]
- Joly, P.; Horváth, B.; Patsatsi, A.; Uzun, S.; Bech, R.; Beissert, S.; Bergman, R.; Bernard, P.; Borradori, L.; Caproni, M.; et al. Updated S2K Guidelines on the Management of Pemphigus Vulgaris and Foliaceus Initiated by the European Academy of Dermatology and Venereology (EADV). J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1900–1913. [Google Scholar] [CrossRef]
- Tan, W.H.; Sim, J.; Sultana, R.; Lee, H.Y. Rituximab in Subepidermal Blistering Diseases. Dermatology 2022, 239, 5–11. [Google Scholar] [CrossRef]
- Jałowska, M.; Gornowicz-Porowska, J.; Seraszek-Jaros, A.; Bowszyc-Dmochowska, M.; Kaczmarek, E.; Dmochowski, M. Conceptualization and Validation of an Innovative Direct Immunofluorescence Technique Utilizing Fluorescein Conjugate against IgG + IgG4 for Routinely Diagnosing Autoimmune Bullous Dermatoses. Cent. Eur. J. Immunol. 2021, 46, 183–190. [Google Scholar] [CrossRef]
- Murrell, D.F.; Dick, S.; Ahmed, A.R.; Amagai, M.; Barnadas, M.A.; Borradori, L.; Bystryn, J.C.; Cianchini, G.; Díaz, L.A.; Fivenson, D.P.; et al. Consensus Statement on Definitions of Disease, End Points, and Therapeutic Response for Pemphigus. J. Am. Acad. Dermatol. 2008, 58, 1043–1046. [Google Scholar] [CrossRef]
- Wang, H.H.; Liu, C.W.; Li, Y.-C.; Huang, Y. Efficacy of Rituximab for Pemphigus: A Systematic Review and Meta-Analysis of Different Regimens. Acta Derm. Venerol. 2015, 95, 928–932. [Google Scholar] [CrossRef]
- Zhao, W.; Wang, J.; Zhu, H.; Pan, M. Comparison of Guidelines for Management of Pemphigus: A Review of Systemic Corticosteroids, Rituximab, and Other Immunosuppressive Therapies. Clin. Rev. Allergy Immunol. 2021, 61, 351–362. [Google Scholar] [CrossRef]
- Balighi, K.; Daneshpazhooh, M.; Mahmoudi, H.; Badakhsh, M.; Teimourpour, A.; Ehsani, A.H.; Azizpour, A.; Akbari, Z.; Mahdavinia, M.; Ghasemiadl, M.; et al. Comparing Early and Late Treatments with Rituximab in Pemphigus Vulgaris: Which One Is Better? Arch. Dermatol. Res. 2018, 311, 63–69. [Google Scholar] [CrossRef]
- Joly, P.; Maho-Vaillant, M.; Prost-Squarcioni, C.; Hebert, V.; Houivet, E.; Calbo, S.; Caillot, F.; Golinski, M.L.; Labeille, B.; Picard-Dahan, C.; et al. French study group on autoimmune bullous skin diseases. First-line rituximab combined with short-term prednisone versus prednisone alone for the treatment of pemphigus (Ritux 3): A prospective, multicentre, parallel-group, open-label randomised trial. Lancet 2017, 20, 2031–2040. [Google Scholar] [CrossRef]
- Chen, D.M.; Odueyungbo, A.; Csinady, E.; Gearhart, L.; Lehane, P.; Cheu, M.; Maho-Vaillant, M.; Prost-Squarcioni, C.; Hebert, V.; Houivet, E.; et al. French Study Group on Autoimmune Bullous Diseases. Rituximab is an effective treatment in patients with pemphigus vulgaris and demonstrates a steroid-sparing effect. Br. J. Dermatol. 2020, 182, 1111–1119. [Google Scholar] [CrossRef]
- Werth, V.P.; Joly, P.; Mimouni, D.; Maverakis, E.; Caux, F.; Lehane, P.; Gearhart, L.; Kapre, A.; Pordeli, P.; Chen, D.M. Rituximab versus Mycophenolate Mofetil in Patients with Pemphigus Vulgaris. N. Engl. J. Med. 2021, 17, 2295–2305. [Google Scholar] [CrossRef]
- Amber, K.T.; Valdebran, M.; Grando, S.A. Non-Desmoglein Antibodies in Patients with Pemphigus Vulgaris. Front. Immunol. 2018, 9, 1190. [Google Scholar] [CrossRef]
- Schmidt, E.; Hennig, K.; Mengede, C.; Zillikens, D.; Kromminga, A. Immunogenicity of Rituximab in Patients with Severe Pemphigus. Clin. Immunol. 2009, 132, 334–341. [Google Scholar] [CrossRef]
- Lunardon, L.; Payne, A. Inhibitory Human Antichimeric Antibodies to Rituximab in a Patient with Pemphigus. J. Allergy Clin. Immunol. 2012, 130, 800–803. [Google Scholar] [CrossRef]
- Zhou, S.; Liu, Z.; Yuan, H.-K.; Zhao, X.; Zou, Y.; Zheng, J.; Pan, M. Autoreactive B Cell Differentiation in Diffuse Ectopic Lymphoid-Like Structures of Inflamed Pemphigus Lesions. J. Investig. Dermatol. 2020, 140, 309–318.e8. [Google Scholar] [CrossRef]
- Welc, N.; Bowszyc-Dmochowska, M.; Jałowska, M.; Dmochowski, M. The cutaneous form of pemphigus vulgaris of the pemphigus chancre type: Clinical and therapeutic implications. Dermatol. Rev. 2023, 110, 633–636. [Google Scholar] [CrossRef]
- Abasq, C.; Mouquet, H.; Gilbert, D.; Tron, F.; Grassi, V.; Musette, P.; Joly, P. ELISA Testing of Anti–Desmoglein 1 and 3 Antibodies in the Management of Pemphigus. Arch. Dermatol. 2009, 145, 529–535. [Google Scholar] [CrossRef]
- Balighi, K.; Sakhi, R.-S.; Daneshpazhooh, M.; Mahmoudi, H.; Teimourpour, A.; Tavakolpour, S. Anti-Desmoglein-1 Levels as Predictor of Prednisolone Tapering in Pemphigus Vulgaris Patients Treated with Rituximab. Dermatol. Ther. 2018, 31, e12671. [Google Scholar] [CrossRef]
- Kakuta, R.; Kurihara, Y.; Yamagami, J.; Miyamoto, J.; Funakoshi, T.; Tanikawa, A.; Amagai, M. Results of the Guideline-based Treatment for Pemphigus: A Single-centre Experience with 84 Cases. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1324–1330. [Google Scholar] [CrossRef]
- Yamagami, J.; Kurihara, Y.; Funakoshi, T.; Saito, Y.; Tanaka, R.; Takahashi, H.; Ujiie, H.; Iwata, H.; Hirai, Y.; Iwatsuki, K.; et al. Rituximab Therapy for Intractable Pemphigus: A Multicenter, Open-label, Single-arm, Prospective Study of 20 Japanese Patients. J. Dermatol. 2022, 50, 175–182. [Google Scholar] [CrossRef]
- Zhou, X.; Hu, W.; Qin, X. The Role of Complement in the Mechanism of Action of Rituximab for B-Cell Lymphoma: Implications for Therapy. Oncologist 2008, 13, 954–966. [Google Scholar] [CrossRef]
- Ellebrecht, C.T.; Mukherjee, E.M.; Zheng, Q.; Choi, E.J.; Reddy, S.; Mao, X.; Payne, A. Autoreactive IgG and IgA B Cells Evolve through Distinct Subclass Switch Pathways in the Autoimmune Disease Pemphigus Vulgaris. Cell Rep. 2018, 24, 2370–2380. [Google Scholar] [CrossRef]
- Colliou, N.; Picard, D.; Caillot, F.; Calbo, S.; Corre, S.L.; Lim, A.; Lemercier, B.; Mauff, B.L.; Maho-Vaillant, M.; Jacquot, S.; et al. Long-Term Remissions of Severe Pemphigus After Rituximab Therapy Are Associated with Prolonged Failure of Desmoglein B Cell Response. Sci. Transl. Med. 2013, 5, 175ra30. [Google Scholar] [CrossRef]
- Maho-Vaillant, M.; Pérals, C.; Golinski, M.-L.; Hébert, V.; Caillot, F.; Mignard, C.; Riou, G.; Petit, M.; Viguier, M.; Hertl, M.; et al. Rituximab and Corticosteroid Effect on Desmoglein-Specific B Cells and Desmoglein-Specific T Follicular Helper Cells in Pemphigus. J. Investig. Dermatol. 2021, 141, 2132–2140.e1. [Google Scholar] [CrossRef]
- Bevans, S.L.; Sami, N. The Use of Rituximab in Treatment of Epidermolysis Bullosa Acquisita: Three New Cases and a Review of the Literature. Dermatol. Ther. 2018, 31, e12726. [Google Scholar] [CrossRef]
- Mendes, S.R.; Coutinho, I.; Cardoso, J.C. Epidermolysis Bullosa Acquisita Treated with Rituximab. BMJ Case Rep. 2021, 14, e243432. [Google Scholar] [CrossRef]
- Bieber, K.; Witte, M.; Sun, S.; Hundt, J.E.; Kalies, K.; Dräger, S.; Kasprick, A.; Twelkmeyer, T.; Manz, R.A.; König, P.; et al. T Cells Mediate Autoantibody-Induced Cutaneous Inflammation and Blistering in Epidermolysis Bullosa Acquisita. Sci. Rep. 2016, 6, 38357. [Google Scholar] [CrossRef]
- Becker, M.; Schumacher, N.; Schmidt, E.; Zillikens, D.; Sadik, C.D. Evaluation and Comparison of Clinical and iLaboratory Characteristics of Patients with IGA Epidermolysis Bullosa Acquisita, Linear IGA Bullous Dermatosis, and IGG Epidermolysis Bullosa Acquisita. JAMA Dermatol. 2021, 157, 917–923. [Google Scholar] [CrossRef]
- Dasdar, S.; Kianfar, N.; Tavakolpour, S.; Balighi, K.; Mahmoudi, H.; Daneshpazhooh, M. Rituximab for the Treatment of Epidermolysis Bullosa Acquisita: A Large Case Series of 15 Patients. J. Dtsch. Dermatol. Ges. 2023, 21, 779–784. [Google Scholar] [CrossRef]
- Grøn, K.L.; Arkema, E.V.; Glintborg, B.; Mehnert, F.; Østergaard, M.; Dreyer, L.; Nørgaard, M.; Krogh, N.S.; Askling, J.; Hetland, M.L. Risk of Serious Infections in Patients with Rheumatoid Arthritis Treated in Routine Care with Abatacept, Rituximab and Tocilizumab in Denmark and Sweden. Ann. Rheum. Dis. 2019, 78, 320–327. [Google Scholar] [CrossRef]
- Cao, P.; Xu, W.; Zhang, L. Rituximab, Omalizumab, and Dupilumab Treatment Outcomes in Bullous Pemphigoid: A Systematic Review. Front. Immunol. 2022, 13, 928621. [Google Scholar] [CrossRef]
- Varley, C.D.; Winthrop, K. Long-Term Safety of Rituximab (Risks of Viral and Opportunistic Infections). Curr. Rheumatol. Rep. 2021, 23, 74. [Google Scholar] [CrossRef] [PubMed]
- Corbaux, C.; Joly, P. Bullous Diseases. In Current Problems in Dermatology; Karger Publishers: Basel, Switzerland, 2017; pp. 64–69. [Google Scholar]
- Chung, C.H. Managing Premedications and the Risk for Reactions to Infusional Monoclonal Antibody Therapy. Oncologist 2008, 13, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Hartinger, J.M.; Satrapová, V.; Hrušková, Z.; Tesař, V. Tolerance and Safety of Rapid 2-Hour Infusion of Rituximab in Patients with Kidney-Affecting Autoimmune Diseases and Glomerulonephritides: A Single-Centre Experience. Eur. J. Hosp. Pharm. 2018, 26, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Zhou, B.; Dong, C.; Zhang, R.; Xie, D.; Tian, Y. Lactobacillus Reuteri Alleviates Gastrointestinal Toxicity of Rituximab by Regulating the Proinflammatory T Cells in Vivo. Front. Microbiol. 2021, 12, 645500. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
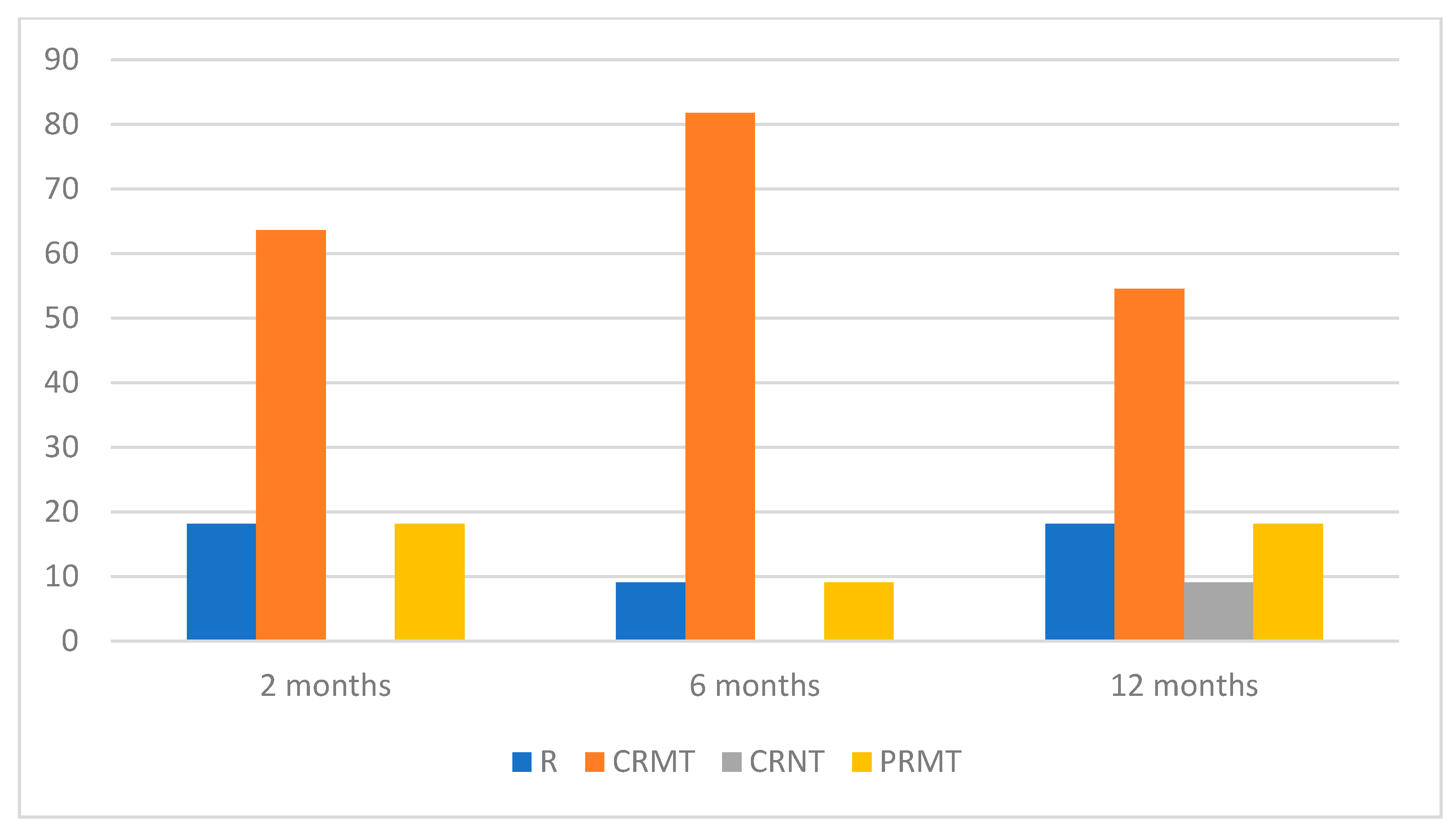
| Patient | Gender/Age (Years) | Disease Type | Duration of Disease Prior to RTX Therapy (Years) | Prior Treatments | Supplementary Medications | Adverse Reactions | Management of Disease Activity after | ||
|---|---|---|---|---|---|---|---|---|---|
| 2 Months | 6 Months | 12 Months | |||||||
| 1 | F/62 | PV | 7 | OGCS, IGCS, DP, CPH, PPH, IVIG | None | None | CRMT | CRMT | CRMT |
| 2 | M/68 | PF | 10 | OGCS | None | Nausea | CRMT | CRMT | PRMT |
| 3 | F/27 | PV | 3.5 | OGCS, IGCS, RTX (2 × 1 g) | DP 25 mg/day | None | CRMT | CRMT | CRMT |
| 4 | F/38 | PV | 1 | OGCS, IGCS | None | Infection | PRMT | R | PRMT |
| 5 | M/68 | PV | 3.5 | OGCS, CPH | None | None | R | CRMT | CRMT |
| 6 | F/69 | PV | 10 | OGCS, DP, PPH | None | Hypotension | CRMT | CRMT | CRMT |
| 7 | F/40 | PF | 1 | OGCS, DP | DP 25 mg/day | None | CRMT | CRMT | CRMT |
| 8 | F/46 | PV | 12 | OGCS, IGCS, DP, CPH | None | Infection | CRMT | CRMT | CRNT |
| 9 | F/46 | PV | 2 | OGCS, IGCS, CPH, IVIG (1 infusion) | None | None | PRMT | CRMT | R |
| 10 | M/54 | PV | 2.5 | OGCS, DP | DP 50 mg/day | None | CRMT | PRMT | R |
| 11 | F/62 | EBA | 3.5 | OCGS, PPH, DP, AZA, MTX, CPH | 3xIGCS 1 g | None | R | CRMT | CRMT |
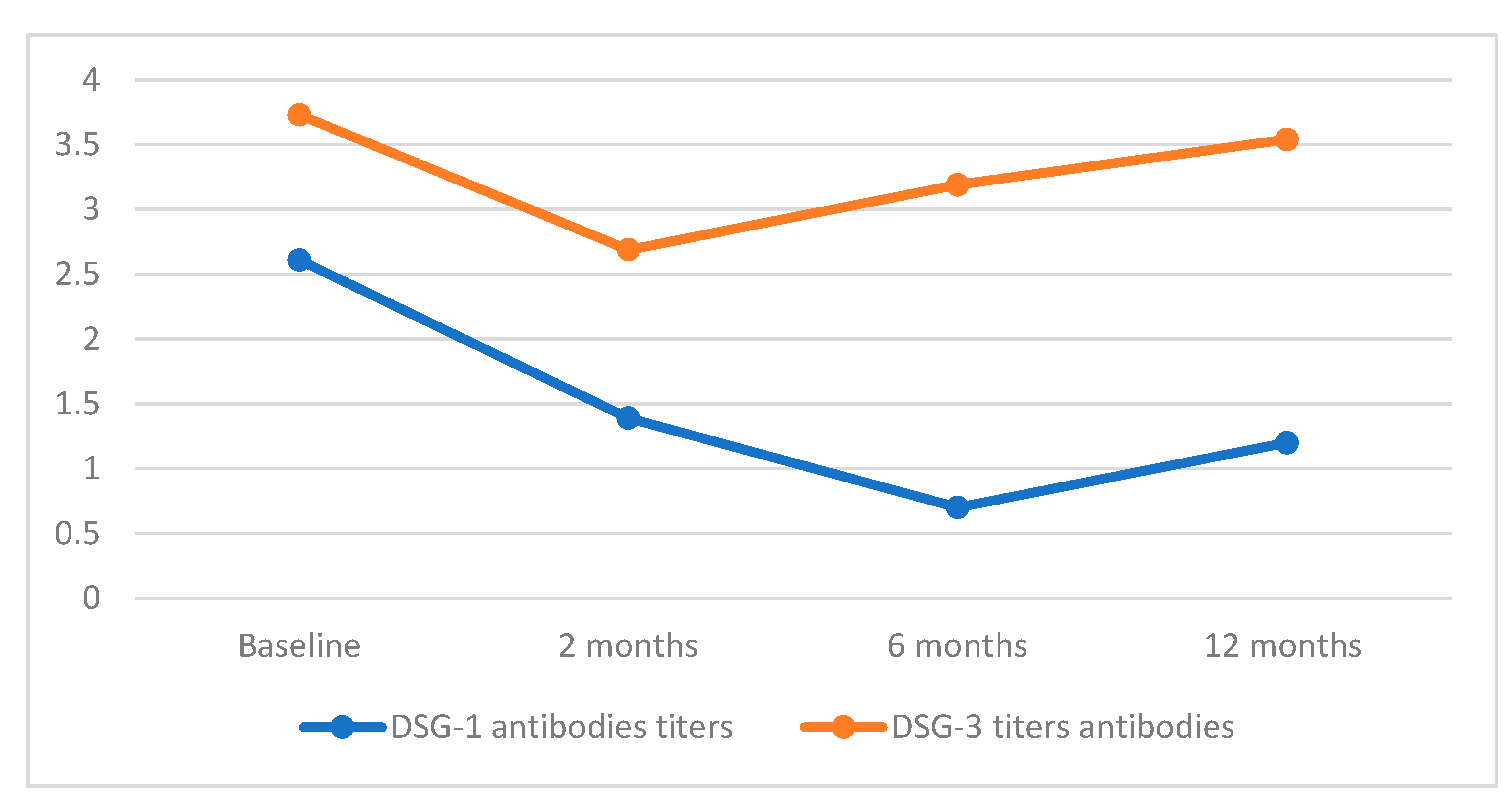
| Patient | DSG-1 Level | DSG-3 Level | ||||||
|---|---|---|---|---|---|---|---|---|
| Before RTX | 2 Months | 6 Months | 12 Months | Before RTX | 2 Months | 6 Months | 12 Months | |
| 1 | 5.87 | 4.42 | 0.25 | 0.22 | 0.63 | 0.25 | 3.01 | 3.35 |
| 2 | 6.25 | 3.67 | 2.21 | 3.06 | 0.15 | 0 | 0.14 | 0.26 |
| 3 | 1.03 | 0.27 | 0.22 | 0.25 | 4.42 | 2.17 | 2.46 | 3.45 |
| 4 | 0.85 | 0.55 | 1.12 | 1.53 | 7.03 | 4.44 | 6.44 | 6.13 |
| 5 | 0.72 | 0.67 | 0.15 | 0.19 | 6.22 | 5.46 | 5.74 | 5.65 |
| 6 | 0.63 | 0.38 | 0.73 | 0.77 | 3.48 | 2.92 | 2.88 | 2.6 |
| 7 | 1.86 | 0.84 | 0.64 | 0.62 | 0.15 | 0.12 | 0.11 | 0.1 |
| 8 | 0.44 | 0.33 | 0.12 | 0.2 | 2.8 | 1.7 | 1.03 | 0.92 |
| 9 | 7.47 | 2.54 | 1.28 | 3.96 | 6.86 | 6.7 | 5.62 | 6.62 |
| 10 | 0.94 | 0.23 | 0.32 | 1.33 | 5.57 | 3.14 | 4.56 | 6.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spałek, M.M.; Jałowska, M.; Bowszyc-Dmochowska, M.; Dmochowski, M. Rituximab in the Management of Autoimmune Bullous Diseases: A Treatment-Resistant Case Series from a Single Central European Referral Center. Medicina 2024, 60, 270. https://doi.org/10.3390/medicina60020270
Spałek MM, Jałowska M, Bowszyc-Dmochowska M, Dmochowski M. Rituximab in the Management of Autoimmune Bullous Diseases: A Treatment-Resistant Case Series from a Single Central European Referral Center. Medicina. 2024; 60(2):270. https://doi.org/10.3390/medicina60020270
Chicago/Turabian StyleSpałek, Maciej Marek, Magdalena Jałowska, Monika Bowszyc-Dmochowska, and Marian Dmochowski. 2024. "Rituximab in the Management of Autoimmune Bullous Diseases: A Treatment-Resistant Case Series from a Single Central European Referral Center" Medicina 60, no. 2: 270. https://doi.org/10.3390/medicina60020270
APA StyleSpałek, M. M., Jałowska, M., Bowszyc-Dmochowska, M., & Dmochowski, M. (2024). Rituximab in the Management of Autoimmune Bullous Diseases: A Treatment-Resistant Case Series from a Single Central European Referral Center. Medicina, 60(2), 270. https://doi.org/10.3390/medicina60020270