
The Effect of Whole-Body Electromyostimulation Program on Physical Performance and Selected Cardiometabolic Markers in Obese Young Females


 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
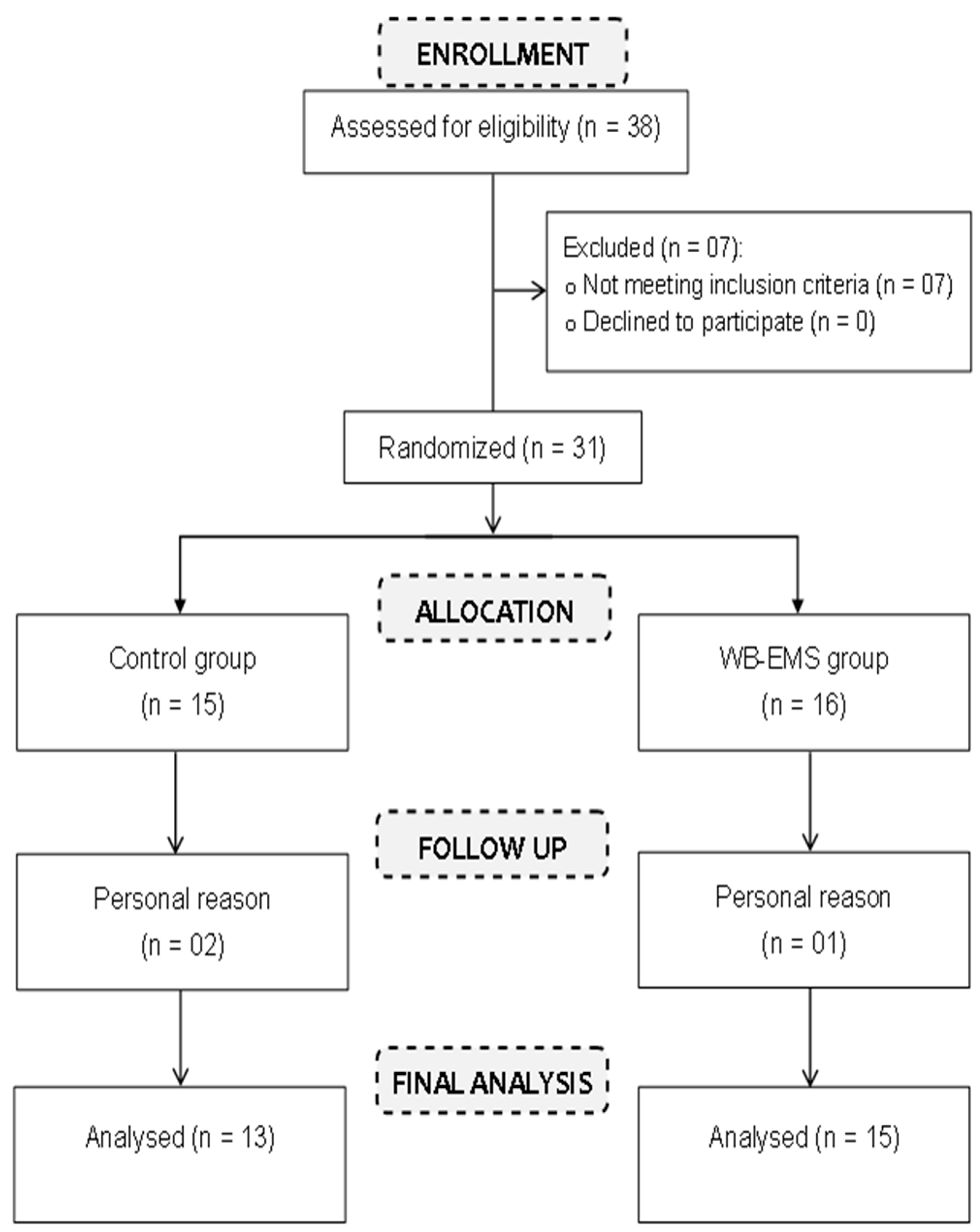
2.1. Trial Design and Participants
2.2. Intervention
2.3. Mesurements
2.3.1. Anthropometric Assessment
2.3.2. Blood Pressure Assessment
2.3.3. Physical Measures
- Incremental running test
- Performance Tests
- Squat Jump (SJ):
- Procedure:
- Measurement:
- Counter Movement Jump (CMJ):
- Procedure:
- Measurement:
- Five-Jump Test (FJT):
- Procedure:
- Measurement:
- Sprint Tests:
- Procedure:
- Measurement:
2.3.4. Blood Sample Analysis
2.3.5. Sample Size
2.3.6. Randomization
2.4. Statistical Analysis
3. Results
3.1. Test Reliability
3.2. Physical Performance
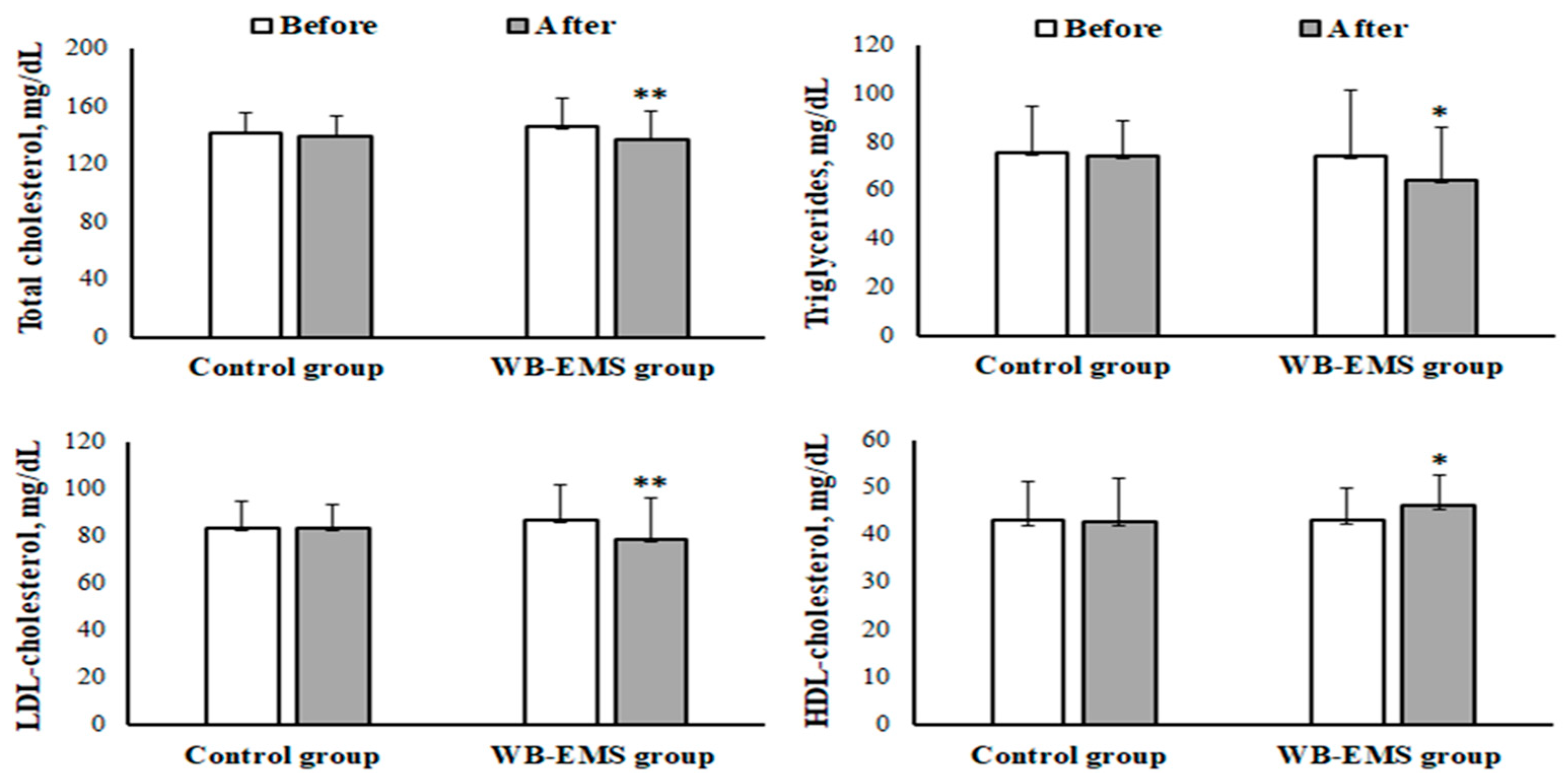
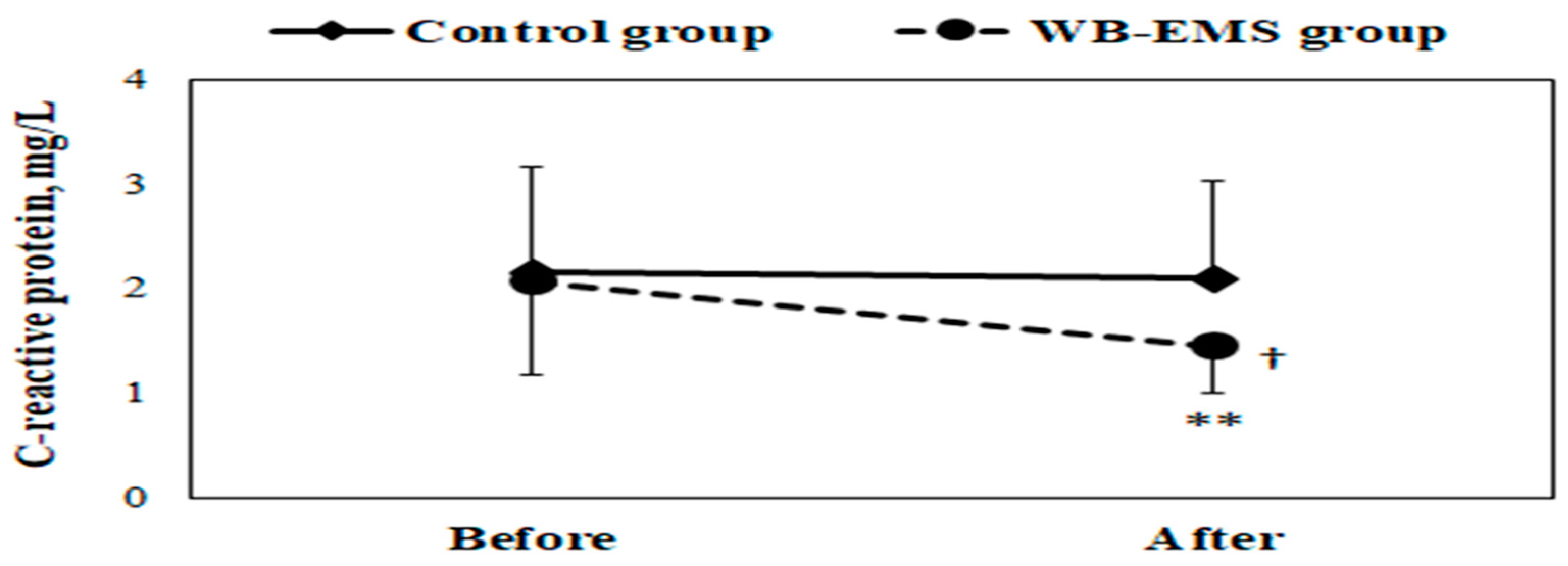
3.3. Cardiometabolic Markers
4. Discussion
4.1. Physical Performance
4.2. Cardiometabolic Markers
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. More Active People for a Healthier World: Global Action Plan Onphysical Activity 2018–2030; World Health Organization: Geneva, Switzerland, 2018.
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef]
- Smith, K.B.; Smith, M.S. Obesity statistics. Prim. Care Clin. Off. Pract. 2016, 43, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Abassi, W.; Ouerghi, N.; Nikolaidis, P.T.; Hill, L.; Racil, G.; Knechtle, B.; Feki, M.; Bouassida, A. Interval training with different intensities in overweight/obese adolescent females. Int. J. Sports Med. 2022, 43, 434–443. [Google Scholar] [CrossRef]
- Ouerghi, N.; Fradj, M.K.; Duclos, M.; Bouassida, A.; Feki, M.; Weiss, K.; Knechtle, B. Effects of High-Intensity Interval Training on Selected Adipokines and Cardiometabolic Risk Markers in Normal-Weight and Overweight/Obese Young Males—A Pre-Post Test Trial. Biology 2022, 11, 853. [Google Scholar] [CrossRef]
- Rodrigues-Santana, L.; Adsuar, J.C.; Louro, H.; Pérez-Gómez, J.; Hernández-Mocholí, M.A.; Carlos-Vivas, J.; Gomez-Campos, R.; Campos, L. The effects of whole-body muscle stimulation on body composition and strength parameters: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e25139. [Google Scholar] [CrossRef]
- Reljic, D.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Iron Beats Electricity: Resistance Training but Not Whole-Body Electromyostimulation Improves Cardiometabolic Health in Obese Metabolic Syndrome Patients during Caloric Restriction—A Randomized-Controlled Study. Nutrients 2021, 13, 1640. [Google Scholar] [CrossRef] [PubMed]
- Willert, S.; Weissenfels, A.; Kohl, M.; von Stengel, S.; Fröhlich, M.; Kleinöder, H.; Schöne, D.; Teschler, M.; Kemmler, W. Effects of Whole-Body Electromyostimulation on the Energy-Restriction-Induced Reduction of Muscle Mass During Intended Weight Loss. Front. Physiol. 2019, 10, 1012. [Google Scholar] [CrossRef]
- Woessner, M.N.; Tacey, A.; Levinger-Limor, A.; Parker, A.G.; Levinger, P.; Levinger, I. The Evolution of Technology and Physical Inactivity: The Good, the Bad, and the Way Forward. Front. Public Health 2021, 9, 655491. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Effect of whole-body electromyostimulation and / or protein supplementation on obesity and cardiometabolic risk in older men with sarcopenic obesity: The randomized controlled FranSO trial. BMC Geriatr. 2018, 18, 70. [Google Scholar] [CrossRef]
- Teschler, M.; Heimer, M.; Schmitz, B.; Kemmler, W.; Mooren, F.C. Four weeks of electromyostimulation improves muscle function and strength in sarcopenic patients: A three-arm parallel randomized trial. J. Cachexia Sarcopenia Muscle 2021, 12, 843–854. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la, O.A.; Sanchez-Delgado, G.; Robles-Gonzalez, L.; Jurado-Fasoli, L.; Ruiz, J.R.; Gutierrez, A. Whole-Body Electromyostimulation Improves Performance-Related Parameters in Runners. Front. Physiol. 2018, 9, 1576. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la, O.A.; Jurado-Fasoli, L.; Ruiz, J.R.; Castillo, M.J.; Gutiérrez, Á. Effects of different exercise training programs on body composition: A randomized control trial. Scand. J. Med. Sci. Sports 2019, 29, 968–979. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weißenfels, A.; Bebenek, M.; Fröhlich, M.; Kohl, M.; von Stengel, S. Effects of Whole-Body Electromyostimulation versus High-Intensity Resistance Exercise on Body Composition and Strength: A Randomized Controlled Study. Evid. Based Complement. Altern. Med. 2016, 2016, 9236809. [Google Scholar] [CrossRef]
- Kemmler, W.; von Stengel, S. Whole-body electromyostimulation as a means to impact muscle mass and abdominal body fat in lean, sedentary, older female adults: Subanalysis of the TEST-III trial. Clin. Interv. Aging 2013, 8, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, K.; Sieber, C.; von Stengel, S.; Kohl, M.; Freiberger, E.; Jakob, F.; Lell, M.; Engelke, K.; Kemmler, W. Impact of whole body electromyostimulation on cardiometabolic risk factors in older women with sarcopenic obesity: The randomized controlled FORMOsA-sarcopenic obesity study. Clin. Interv. Aging 2016, 11, 1697–1706. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Dieterich, W.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. HIIT the Inflammation”: Comparative Effects of Low-Volume Interval Training and Resistance Exercises on Inflammatory Indices in Obese Metabolic Syndrome Patients Undergoing Caloric Restriction. Nutrients 2022, 14, 1996. [Google Scholar] [CrossRef]
- Park, H.K.; Na, S.M.; Choi, S.L.; Seon, J.K.; Do, W.H. Physiological Effect of Exercise Training with Whole Body Electric Muscle Stimulation Suit on Strength and Balance in Young Women: A Randomized Controlled Trial. Chonnam Med. J. 2021, 57, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Jee, Y.S. The efficacy and safety of whole-body electromyostimulation in applying to human body: Based from graded exercise test. J. Exerc. Rehabil. 2018, 14, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Borg, E.; Kaijser, L. A comparison between three rating scales for perceived exertion and two different work tests. Scand. J. Med. Sci. Sports 2006, 16, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.; Becker, S.; Backfisch, M.; Eifler, C.; Kemmler, W.; Fröhlich, M. Adjustment Effects of Maximum Intensity Tolerance During Whole-Body Electromyostimulation Training. Front. Physiol. 2019, 10, 920. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.H.; Laurent, D.; Baumker, E.; Petosa, R.L. Rates of Obesity and Obesogenic Behaviors of Rural Appalachian Adolescents: How Do They Compare to Other Adolescents or Recommendations? J. Phys. Act. Health 2018, 15, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Abassi, W.; Ouerghi, N.; Ghouili, H.; Haouami, S.; Bouassida, A. Greater effects of high- compared with moderate-intensity interval training on thyroid hormones in overweight/obese adolescent girls. Horm. Mol. Biol. Clin. Investig. 2020, 41, 20200031. [Google Scholar] [CrossRef] [PubMed]
- Ouerghi, N.; Fradj, M.K.B.; Bezrati, I.; Khammassi, M.; Feki, M.; Kaabachi, N.; Bouassida, A. Effects of high-intensity interval training on body composition, aerobic and anaerobic performance and plasma lipids in overweight/obese and normal-weight young men. Biol. Sport 2017, 34, 385–392. [Google Scholar] [CrossRef]
- Bosco, C.; Luhtanen, P.; Komi, P.V. A simple method for measurement of mechanical power in jumping. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 50, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Chamari, K.; Chaouachi, A.; Hambli, M.; Kaouech, F.; Wisløff, U.; Castagna, C. The Five-Jump Test for Distance as a Field Test to Assess Lower Limb Explosive Power in Soccer Players. J. Strength Cond. Res. 2008, 22, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation—A Systematic Review of the Influence of Training Regimens and Stimulation Parameters on Effectiveness in Electromyostimulation Training of Selected Strength Parameters. J. Strength Cond. Res. 2011, 25, 3218–3238. [Google Scholar] [CrossRef]
- Nuhr, M.; Crevenna, R.; Gohlsch, B.; Bittner, C.; Pleiner, J.; Wiesinger, G.; Fialka-Moser, V.; Quittan, M.; Pette, D. Functional and biochemical properties of chronically stimulated human skeletal muscle. Eur. J. Appl. Physiol. 2003, 89, 202–208. [Google Scholar] [CrossRef]
- Filipovic, A.; Grau, M.; Kleinöder, H.; Zimmer, P.; Hollmann, W.; Bloch, W. Effects of a Whole-Body Electrostimulation Program on Strength, Sprinting, Jumping, and Kicking Capacity in Elite Soccer Players. J. Sports Sci. Med. 2016, 15, 639–648. [Google Scholar]
- Berger, J.; Ludwig, O.; Becker, S.; Backfisch, M.; Kemmler, W.; Fröhlich, M. Effects of an Impulse Frequency Dependent 10-Week Whole-body Electromyostimulation Training Program on Specific Sport Performance Parameters. J. Sports Sci. Med. 2020, 19, 271–281. [Google Scholar]
- Reljic, D.; Konturek, P.; Herrmann, H.; Neurath, M.; Zopf, Y. Effects of whole-body electromyostimulation exercise and caloric restriction on cardiometabolic risk profile and muscle strength in obese women with the metabolic syndrome: A pilot study. J. Physiol. Pharmacol. 2020, 71, 89–98. [Google Scholar]
- Ricci, P.A.; Di Thommazo-Luporini, L.; Jürgensen, S.P.; André, L.D.; Haddad, G.F.; Arena, R.; Borghi-Silva, A. Effects of Whole-Body Electromyostimulation Associated with Dynamic Exercise on Functional Capacity and Heart Rate Variability After Bariatric Surgery: A Randomized, Double-Blind, and Sham-Controlled Trial. Obes. Surg. 2020, 30, 3862–3871. [Google Scholar] [CrossRef]
- Kemmler, W.; Schliffka, R.; Mayhew, J.L.; von Stengel, S. Effects of Whole-Body Electromyostimulation on Resting Metabolic Rate, Body Composition, and Maximum Strength in Postmenopausal Women: The Training and ElectroStimulation Trial. J. Strength Cond. Res. 2010, 24, 1880–1887. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Bebenek, M.; Engelke, K.; von Stengel, S. Impact of whole-body electromyostimulation on body composition in elderly women at risk for sarcopenia: The Training and ElectroStimulation Trial (TEST-III). AGE 2014, 36, 395–406. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Teschler, M.; Willert, S.; Bebenek, M.; Shojaa, M.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Whole-body electromyostimulation and protein supplementation favorably affect sarcopenic obesity in community-dwelling older men at risk: The randomized controlled FranSO study. Clin. Interv. Aging 2017, 12, 1503–1513. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Maffiuletti, N.A. Neural adaptations to electrical stimulation strength training. Eur. J. Appl. Physiol. 2011, 111, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Eun, D.; Jee, Y.-S. Higher Impulse Electromyostimulation Contributes to Psychological Satisfaction and Physical Development in Healthy Men. Medicina 2021, 57, 191. [Google Scholar] [CrossRef] [PubMed]
- Batacan, R.B.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Reverter-Masia, J.; Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Lecube, A.; Sánchez, E.; Hernández-González, V. Effect of a Training Program on Hepatic Fat Content and Cardiometabolic Risk in Postmenopausal Women: The Randomized Controlled Trial. Appl. Sci. 2021, 11, 6409. [Google Scholar] [CrossRef]
- Swan, I.R.C.; Tew, Z.Y.; Dillon, J.F.; Abboud, R.J. Electrostimulation of Muscles Mimics the Effect of Physical Exercise on Non-alcoholic Fatty Liver Disease: A Systematic Review. AASCIT J. Med. 2017, 3, 1–9. [Google Scholar]
- Schink, K.; Reljic, D.; Herrmann, H.J.; Meyer, J.; Mackensen, A.; Neurath, M.F.; Zopf, Y. Whole-Body Electromyostimulation Combined With Individualized Nutritional Support Improves Body Composition in Patients With Hematological Malignancies—A Pilot Study. Front. Physiol. 2018, 9, 1808. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| WB-EMS Group (n = 15) | Control Group (n = 13) | |
|---|---|---|
| Age (year) | 18.6 ± 0.98 | 18.8 ± 0.83 |
| Body mass (kg) | 82.0 ± 10.6 | 82.1 ± 6.75 |
| BMI (kg/m2) | 31.3 ± 2.74 | 31.7 ± 2.90 |
| Waist circumference (cm) | 103 ± 8.60 | 105 ± 6.44 |
| Body fat (%) | 35.4 ± 2.16 | 35.8 ± 2.13 |
| Skeletal muscle mass (kg) | 31.1 ± 1.02 | 31.3 ± 0.98 |
| SBP (mm Hg) | 124 ± 3.96 | 124 ± 3.81 |
| DBP (mm Hg) | 77.1 ± 3.47 | 77.2 ± 3.72 |
| Crunch | Bridge | Leg raise | Side plank |
| Back extension | Front plank | Lunge | Squat |
| Intraclass Correlation Coefficient | 95% Confidence Intervals | |
|---|---|---|
| MAS (km/h) | 0.777 | 0.573–0.890 |
| VO2max (mL/kg/min) | 0.777 | 0.573–0.890 |
| Squat jump (cm) | 0.645 | 0.364–0.819 |
| CMJ (cm) | 0.766 | 0.555–0.885 |
| Five-jump test (m) | 0.638 | 0.354–0.814 |
| 10 m sprint test (s) | 0.648 | 0.369–0.820 |
| 30 m sprint test (s) | 0.925 | 0.846–0.965 |
| Control Group (n = 13) | WB-EMS Group (n = 15) | Time Effect | Group Effect | Interaction (Time × Group) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |
| Body mass (kg) | 82.1 ± 6.75 | 81.3 ± 6.61 | 82.0 ± 10.6 | 79.4 ± 9.91 *** | 17.8 | <0.001 | 0.41 | 0.09 | 0.76 | 0.00 | 4.80 | 0.038 | 0.16 |
| BMI (kg/m2) | 31.7 ± 2.90 | 31.4 ± 2.84 | 31.3 ± 2.74 | 30.3 ± 2.60 *** | 18.1 | <0.001 | 0.41 | 0.58 | 0.46 | 0.02 | 4.76 | 0.038 | 0.16 |
| Waist circumference (cm) | 105 ± 6.44 | 106 ± 6.41 | 103 ± 8.60 | 100 ± 8.01 ** | 4.73 | 0.39 | 0.15 | 0.93 | 0.34 | 0.04 | 4.29 | 0.048 | 0.14 |
| Body fat (%) | 35.8 ± 2.13 | 35.2 ± 2.40 | 35.4 ± 2.16 | 33.5 ± 2.65 ** | 17.4 | 0.00 | 0.40 | 1.40 | 0.25 | 0.05 | 4.41 | 0.046 | 0.15 |
| Skeletal muscle mass (kg) | 31.3 ± 0.98 | 31.0 ± 0.75 | 31.1 ± 1.02 | 32.4 ± 1.95 **,† | 5.24 | 0.03 | 0.17 | 2.213 | 0.15 | 0.08 | 9.95 | 0.004 | 0.28 |
| SBP (mm Hg) | 124 ± 3.81 | 124 ± 2.81 | 124 ± 3.96 | 122 ± 3.18 **,† | 5.20 | 0.03 | 0.17 | 1.09 | 0.31 | 0.04 | 4.56 | 0.042 | 0.15 |
| DBP (mm Hg) | 77.2 ± 3.72 | 77.1 ± 2.47 | 77.1 ± 3.47 | 75.5 ± 3.68 * | 4.53 | 0.04 | 0.15 | 0.48 | 0.49 | 0.02 | 3.73 | 0.060 | 0.13 |
| Maximal heart rate (bpm) | 197.8 ± 3.56 | 197.9 ± 2.76 | 198.0 ± 3.23 | 197.0 ± 3.14 | 1.37 | 0.25 | 0.05 | 0.07 | 0.79 | 0.00 | 1.86 | 0.180 | 0.07 |
| MAS (km/h) | 10.3 ± 1.17 | 10.2 ± 0.95 | 10.3 ± 1.03 | 10.8 ± 0.96 ** | 3.03 | 0.09 | 0.10 | 0.74 | 0.40 | 0.03 | 4.21 | 0.050 | 0.14 |
| VO2max (mL/kg/min) | 37.7 ± 4.09 | 37.6 ± 3.32 | 37.9 ± 3.62 | 39.6 ± 3.35 ** | 3.00 | 0.09 | 0.10 | 0.74 | 0.40 | 0.03 | 4.22 | 0.050 | 0.14 |
| Squat jump (cm) | 14.7 ± 2.60 | 15.2 ± 2.79 | 14.9 ± 2.64 | 18.1 ± 3.12 ***,† | 21.8 | <0.001 | 0.46 | 2.41 | 0.13 | 0.09 | 11.3 | 0.002 | 0.30 |
| CMJ (cm) | 17.0 ± 3.47 | 17.3 ± 3.39 | 17.1 ± 2.53 | 19.8 ± 1.95 ***,† | 22.9 | <0.001 | 0.47 | 1.54 | 0.23 | 0.06 | 14.3 | 0.001 | 0.36 |
| Five-jump test (m) | 6.87 ± 0.62 | 6.94 ± 0.80 | 7.03 ± 0.64 | 8.03 ± 0.62 ***,††† | 37.2 | <0.001 | 0.50 | 6.95 | 0.014 | 0.21 | 28.1 | 0.000 | 0.52 |
| 10 m sprint test (s) | 2.90 ± 0.42 | 2.95 ± 0.44 | 2.82 ± 0.36 | 2.70 ± 0.29 | 0.40 | 0.53 | 0.02 | 1.52 | 0.23 | 0.06 | 1.95 | 0.180 | 0.07 |
| 30 m sprint test (s) | 6.77 ± 0.67 | 6.78 ± 0.73 | 6.72 ± 0.46 | 6.53 ± 0.43 ** | 5.39 | 0.03 | 0.17 | 0.49 | 0.49 | 0.02 | 6.46 | 0.017 | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salhi, A.; Ouerghi, N.; Zouhal, H.; Baaziz, M.; Salhi, A.; Ben Salah, F.Z.; Ben Abderrahman, A. The Effect of Whole-Body Electromyostimulation Program on Physical Performance and Selected Cardiometabolic Markers in Obese Young Females. Medicina 2024, 60, 230. https://doi.org/10.3390/medicina60020230
Salhi A, Ouerghi N, Zouhal H, Baaziz M, Salhi A, Ben Salah FZ, Ben Abderrahman A. The Effect of Whole-Body Electromyostimulation Program on Physical Performance and Selected Cardiometabolic Markers in Obese Young Females. Medicina. 2024; 60(2):230. https://doi.org/10.3390/medicina60020230
Chicago/Turabian StyleSalhi, Amal, Nejmeddine Ouerghi, Hassane Zouhal, Mohamed Baaziz, Amine Salhi, Fatma Zohra Ben Salah, and Abderraouf Ben Abderrahman. 2024. "The Effect of Whole-Body Electromyostimulation Program on Physical Performance and Selected Cardiometabolic Markers in Obese Young Females" Medicina 60, no. 2: 230. https://doi.org/10.3390/medicina60020230
APA StyleSalhi, A., Ouerghi, N., Zouhal, H., Baaziz, M., Salhi, A., Ben Salah, F. Z., & Ben Abderrahman, A. (2024). The Effect of Whole-Body Electromyostimulation Program on Physical Performance and Selected Cardiometabolic Markers in Obese Young Females. Medicina, 60(2), 230. https://doi.org/10.3390/medicina60020230