
Acute Effects of Short-Term Massage Procedures on Neuromechanical Contractile Properties of Rectus Femoris Muscle

 ,
, 
 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Experimental Protocol
2.4. Experimental Procedures
2.4.1. TMG Measurements
2.4.2. MVIC, Warm-Up, and Fatigue Procedures
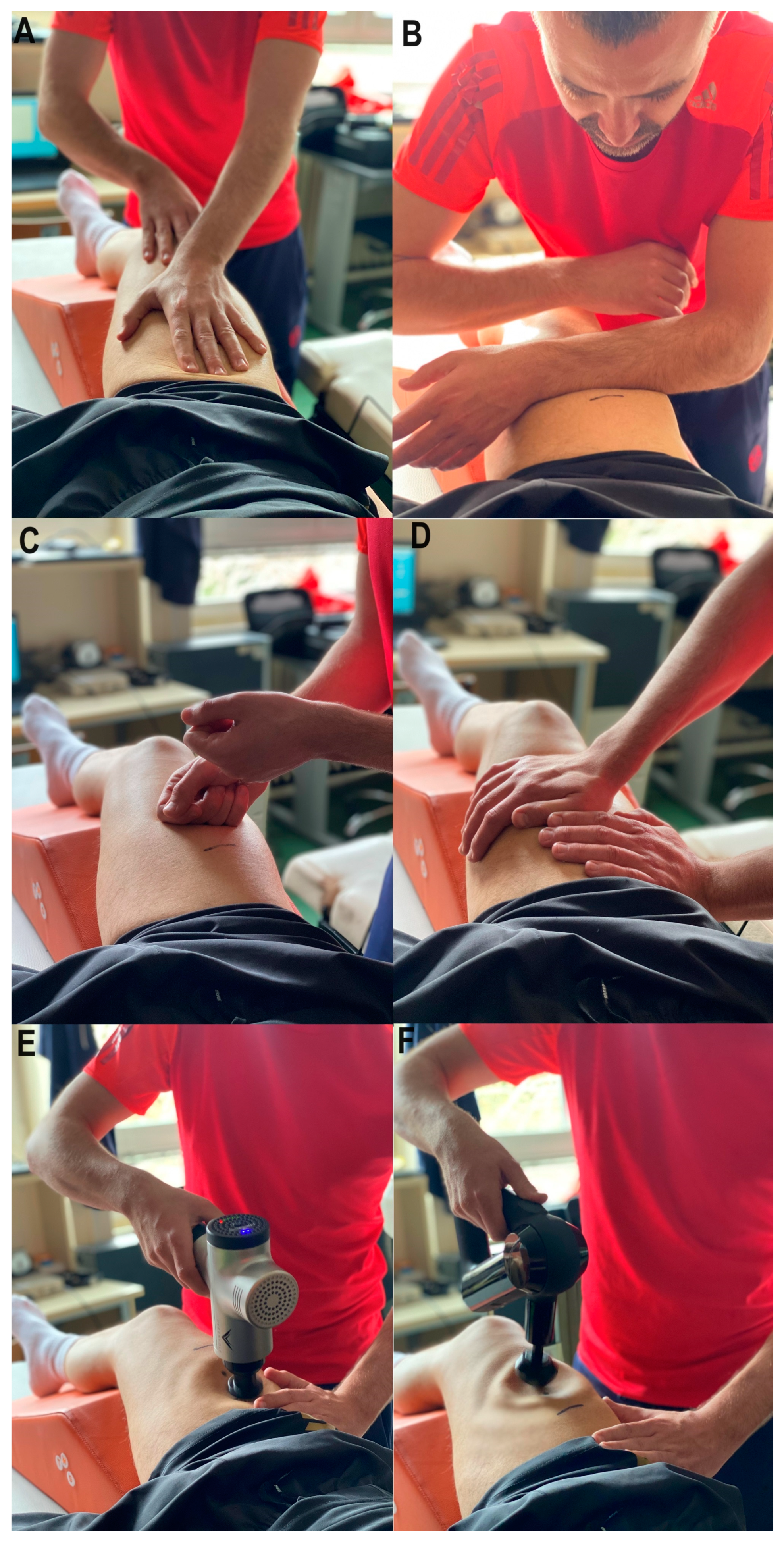
2.4.3. Recovery Treatments
2.5. Statistical Analysis
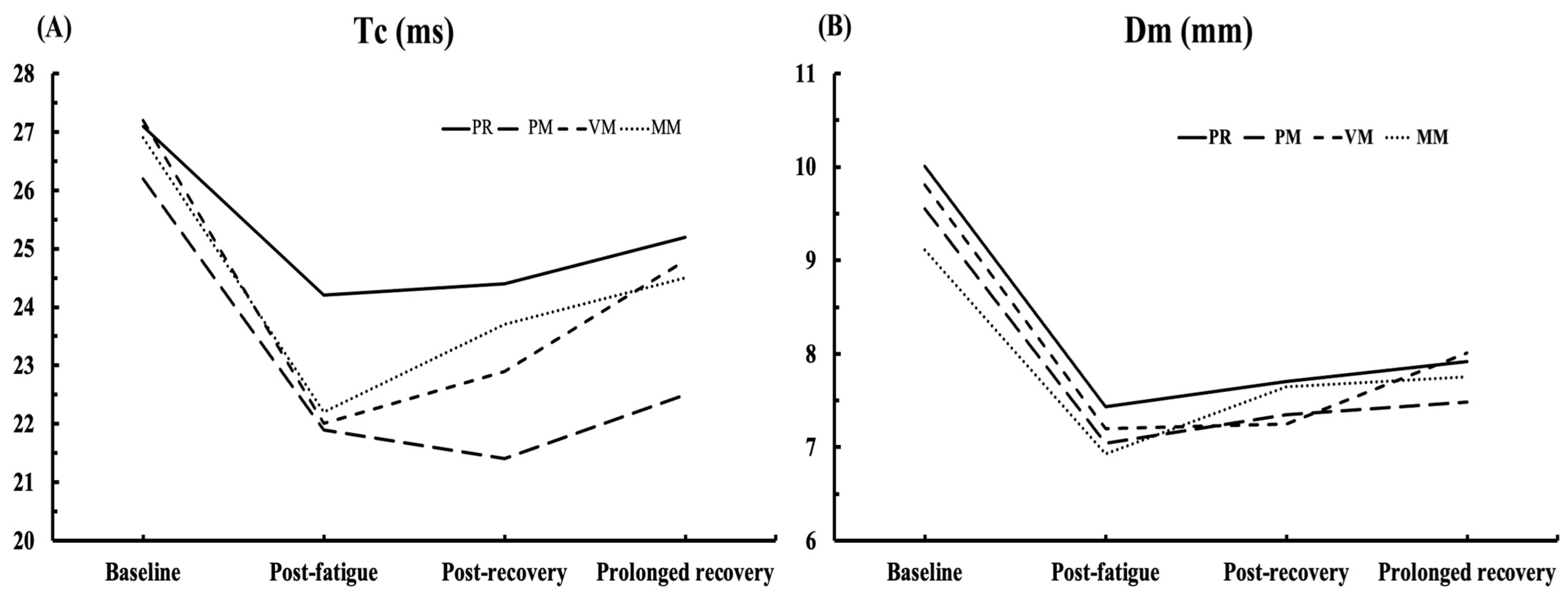
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Windt, J.; Gabbett, T.J. How do training and competition workloads relate to injury? The workload—Injury aetiology model. Br. J. Sports Med. 2016, 51, 428–435. [Google Scholar] [CrossRef]
- Mika, A.; Oleksy, Ł.; Kielnar, R.; Wodka-Natkaniec, E.; Twardowska, M.; Kamiński, K.; Małek, Z. Comparison of two different modes of active recovery on muscles performance after fatiguing exercise in mountain canoeist and football players. PLoS ONE 2016, 11, e0164216. [Google Scholar] [CrossRef]
- Kenney, W.L.; Wilmore, J.H.; Costill, D.L. Physiology of Sport and Exercise, 5th ed.; Human Kinetics: Champaign, IL, USA, 2011; ISBN 978-0-7360-9409-2. [Google Scholar]
- Mika, A.; Mika, P.; Fernhall, B.; Unnithan, V.B. Comparison of recovery strategies on muscle performance after fatiguing exercise. Am. J. Phys. Med. Rehabil. 2007, 86, 474–481. [Google Scholar] [CrossRef]
- Einstein, A. Massage Techniques, Mobilizations, Stretches, Endangerment Sites, and Contraindications. In Massage Techniques: Principles and Practice; Elsevier: St. Louis, MI, USA, 2022; p. 136. [Google Scholar]
- Atchison, J.W.; Tolchin, R.B.; Ross, B.S.; Eubanks, J.E. Manipulation, traction, and massage. In Braddom’s Physical Medicine and Rehabilitation; Elsevier: Amsterdam, The Netherlands, 2021; pp. 316–337. [Google Scholar]
- Ward, K. Routledge Handbook of Sports Therapy, Injury Assessment and Rehabilitation; Routledge: London, UK, 2015; ISBN 9780203807194. [Google Scholar]
- Miake-Lye, I.M.; Mak, S.; Lee, J.; Luger, T.; Taylor, S.L.; Shanman, R.; Beroes-Severin, J.M.; Shekelle, P.G. Massage for pain: An evidence map. J. Altern. Complement. Med. 2019, 25, 475–502. [Google Scholar] [CrossRef]
- Brancaccio, P.; Limongelli, F.M.; D’Aponte, A.; Narici, M.; Maffulli, N. Changes in skeletal muscle architecture following a cycloergometer test to exhaustion in athletes. J. Sci. Med. Sport 2008, 11, 538–541. [Google Scholar] [CrossRef]
- Seymour, J.M.; Ward, K.; Sidhu, P.S.; Puthucheary, Z.; Steier, J.; Jolley, C.J.; Rafferty, G.; Polkey, M.I.; Moxham, J. Ultrasound measurement of rectus femoris cross-sectional area and the relationship with quadriceps strength in COPD. Thorax 2009, 64, 418–423. [Google Scholar] [CrossRef]
- Ekstrand, J.; Healy, J.C.; Waldén, M.; Lee, J.C.; English, B.; Hägglund, M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br. J. Sports Med. 2012, 46, 112–117. [Google Scholar] [CrossRef]
- Sidhu, S.K.; Bentley, D.J.; Carroll, T.J. Cortical voluntary activation of the human knee extensors can be reliably estimated using transcranial magnetic stimulation. Muscle Nerve 2009, 39, 186–196. [Google Scholar] [CrossRef]
- Ebersole, K.T.; Housh, T.J.; Johnson, G.O.; Evetovich, T.K.; Smith, D.B.; Perry, S.R. MMG and EMG responses of the superficial quadriceps femoris muscles. J. Electromyogr. Kinesiol. 1999, 9, 219–227. [Google Scholar] [CrossRef]
- Perry-Rana, S.R.; Housh, T.J.; Johnson, G.O.; Bull, A.J.; Berning, J.M.; Cramer, J.T. MMG and EMG responses during fatiguing isokinetic muscle contractions at different velocities. Muscle Nerve 2002, 26, 367–373. [Google Scholar] [CrossRef]
- Mooney, K.; Warner, M.; Stokes, M. Symmetry and within-session reliability of mechanical properties of biceps brachii muscles in healthy young adult males using the MyotonPRO device. Work. Pap. Health Sci. 2013, 1, 3. [Google Scholar]
- Šimunič, B. Between-day reliability of a method for non-invasive estimation of muscle composition. J. Electromyogr. Kinesiol. 2012, 22, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Valenčič, V.; Knez, N. Measuring of skeletal muscles’ dynamic properties. Artif. Organs 1997, 21, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Tous-Fajardo, J.; Moras, G.; Rodríguez-Jiménez, S.; Usach, R.; Doutres, D.M.; Maffiuletti, N.A. Inter-rater reliability of muscle contractile property measurements using non-invasive tensiomyography. J. Electromyogr. Kinesiol. 2010, 20, 761–766. [Google Scholar] [CrossRef] [PubMed]
- García-García, O.; Cuba-Dorado, A.; Álvarez-Yates, T.; Carballo-López, J.; Iglesias-Caamaño, M. Clinical utility of tensiomyography for muscle function analysis in athletes. Open Access J. Sports Med. 2019, 10, 49–69. [Google Scholar] [CrossRef]
- Macgregor, L.J.; Fairweather, M.M.; Bennett, R.M.; Hunter, A.M. The effect of foam rolling for three consecutive days on muscular efficiency and range of motion. Sports Med.-Open 2018, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Cabrera, F.I.; Núñez-Sánchez, F.J. Acute effect of a foam roller on the mechanical properties of the rectus femoris based on tensiomyography in soccer players. Int. J. Hum. Mov. Sports Sci. 2016, 4, 26–32. [Google Scholar] [CrossRef]
- Murray, A.M.; Jones, T.W.; Horobeanu, C.; Turner, A.P.; Sproule, J. Sixty seconds of foam rolling does not affect functional flexibility or change muscle temperature in adolescent athletes. Int. J. Sprots Phys. Ther. 2016, 11, 765–776. [Google Scholar]
- Pérez-Bellmunt, A.; Labata-Lezaun, N.; Llurda-Almuzara, L.; Rodríguez-Sanz, J.; González-Rueda, V.; Bueno-Gracia, E.; Celik, D.; López-De-Celis, C. Effects of a massage protocol in tensiomyographic and myotonometric proprieties. Int. J. Environ. Res. Public Health 2021, 18, 3891. [Google Scholar] [CrossRef]
- García-Sillero, M.; Benítez-Porres, J.; García-Romero, J.; Bonilla, D.A.; Petro, J.L.; Vargas-Molina, S. Comparison of interventional strategies to improve recovery after eccentric exercise-induced muscle fatigue. Int. J. Environ. Res. Public Health 2021, 18, 647. [Google Scholar] [CrossRef]
- Fernández-Echeverría, C.; González-Silva, J.; Castro, I.T.; Moreno, M.P. The Timeout in Sports: A Study of Its Effect on Volleyball. Front. Psychol. 2019, 10, 2437. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, J.; Lago-Peñas, C.; Gómez, M.A. Brief exploration of short and mid-term timeout effects on basketball scoring according to situational variables. Eur. J. Sport Sci. 2013, 13, 25–30. [Google Scholar] [CrossRef]
- Cuk, I.; Markovic, M.; Nedeljkovic, A.; Ugarkovic, D.; Kukolj, M.; Jaric, S. Force–velocity relationship of leg extensors obtained from loaded and unloaded vertical jumps. Eur. J. Appl. Physiol. 2014, 114, 1703–1714. [Google Scholar] [CrossRef] [PubMed]
- Kassarjian, A.; Rodrigo, R.; Santisteban, J. Current concepts in MRI of rectus femoris musculotendinous (myotendinous) and myofascial injuries in elite athletes. Eur. J. Radiol. 2012, 81, 3763–3771. [Google Scholar] [CrossRef] [PubMed]
- Toskić, L.; Dopsaj, M.; Stanković, V.; Marković, M. Concurrent and predictive validity of isokinetic dynamometry and tensiomyography in differently trained women and men. Isokinet. Exerc. Sci. 2019, 27, 31–39. [Google Scholar] [CrossRef]
- Toskić, L.D.; Dopsaj, M.J.; Marković, M.R.; Toskić, D.R.; Ignjatović, A.M. Mechanical and contractile properties of knee joint muscles measured by the method of tensiomyography in differently trained men and women. J. Strength Cond. Res. 2022, 36, 1532–1539. [Google Scholar] [CrossRef]
- Rey, E.; Lago-Peñas, C.; Lago-Ballesteros, J. Tensiomyography of selected lower-limb muscles in professional soccer players. J. Electromyogr. Kinesiol. 2012, 22, 866–872. [Google Scholar] [CrossRef]
- Martín-Rodríguez, S.; Loturco, I.; Hunter, A.M.; Rodríguez-Ruiz, D.; Munguia-Izquierdo, D. Reliability and measurement error of tensiomyography to assess mechanical muscle function: A systematic review. J. Strength Cond. Res. 2017, 31, 3524–3536. [Google Scholar] [CrossRef]
- Hunter, A.M.; Galloway, S.D.; Smith, I.J.; Tallent, J.; Ditroilo, M.; Fairweather, M.M.; Howatson, G. Assessment of eccentric exercise-induced muscle damage of the elbow flexors by tensiomyography. J. Electromyogr. Kinesiol. 2012, 22, 334–341. [Google Scholar] [CrossRef]
- Pišot, R.; Narici, M.V.; Šimunič, B.; De Boer, M.; Seynnes, O.; Jurdana, M.; Biolo, G.; Mekjavić, I.B. Whole muscle contractile parameters and thickness loss during 35-day bed rest. Eur. J. Appl. Physiol. 2008, 104, 409–414. [Google Scholar] [CrossRef]
- Marshall, P.W.; Finn, H.T.; Enoka, R.M. Declines in muscle contractility and activation during isometric contractions of the knee extensors vary with contraction intensity and exercise volume. Exp. Physiol. 2021, 106, 2096–2106. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Baker, R.T.; Behm, D.G.; Stull, K.; Kolber, M.J. Mechanical Percussion Devices: A Survey of Practice Patterns Among Healthcare Professionals. Int. J. Sports Phys. Ther. 2021, 16, 766–777. [Google Scholar] [CrossRef] [PubMed]
- García-Sillero, M.; Jurado-Castro, J.M.; Benítez-Porres, J.; Vargas-Molina, S. Acute effects of a percussive massage treatment on movement velocity during resistance training. Int. J. Environ. Res. Public Health 2021, 18, 7726. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.J.; Dixon, M.W.; Thompson, D.; Cherkin, D.C. Development of a taxonomy to describe massage treatments for musculoskeletal pain. BMC Complement. Altern. Med. 2006, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, M.J. The role of massage in the management of the athlete: A review. Br. J. Sports Med. 1993, 27, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Goats, G.C. Massage—The scientific basis of an ancient art: Part 1. The techniques. Br. J. Sports Med. 1994, 28, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Moraska, A. Sports massage. A comprehensive review. J. Sports Med. Phys. Fit. 2005, 45, 370–380. [Google Scholar]
- Cohen, J. Statistical power analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- de Paula Simola, R.Á.; Harms, N.; Raeder, C.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Assessment of neuromuscular function after different strength training protocols using tensiomyography. J. Strength Cond. Res. 2015, 29, 1339–1348. [Google Scholar] [CrossRef]
- Dahmane, R.; Valenčič, V.; Knez, N.; Eržen, I. Evaluation of the ability to make non-invasive estimation of muscle contractile properties on the basis of the muscle belly response. Med. Biol. Eng. Comput. 2001, 39, 51–55. [Google Scholar] [CrossRef]
- Križaj, D.; Šimunič, B.; Žagar, T. Short-term repeatability of parameters extracted from radial displacement of muscle belly. J. Electromyogr. Kinesiol. 2008, 18, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Dahmane, R.; Djordjevič, S.; Šimunič, B.; Valenčič, V. Spatial fiber type distribution in normal human muscle: Histochemical and tensiomyographical evaluation. J. Biomech. 2005, 38, 2451–2459. [Google Scholar] [CrossRef] [PubMed]
- García-García, O.; Cuba-Dorado, A.; Riveiro-Bozada, A.; Carballo-López, J.; Álvarez-Yates, T.; López-Chicharro, J. A maximal incremental test in cyclists causes greater peripheral fatigue in biceps femoris. Res. Q. Exerc. Sport 2020, 91, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-López, A.; De Hoyo, M.; Nuñez, F.J.; Sañudo, B. Using tensiomyography to assess changes in knee muscle contraction properties after concentric and eccentric fatiguing muscle actions. J. Strength Cond. Res. 2022, 36, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Kalc, M.; Puš, K.; Paravlic, A.; Urbanc, J.; Šimunič, B. Diagnostic accuracy of Tensiomyography parameters for monitoring peripheral neuromuscular fatigue. J. Electromyogr. Kinesiol. 2023, 70, 102775. [Google Scholar] [CrossRef] [PubMed]
- García-Manso, J.M.; Rodríguez-Ruiz, D.; Rodríguez-Matoso, D.; de Saa, Y.; Sarmiento, S.; Quiroga, M. Assessment of muscle fatigue after an ultra-endurance triathlon using tensiomyography (TMG). J. Sports Sci. 2011, 29, 619–625. [Google Scholar] [CrossRef]
- Muñoz-Pérez, I.; Varela-Sanz, A.; Lago-Fuentes, C.; Navarro-Patón, R.; Mecías-Calvo, M. Central and peripheral fatigue in recreational trail runners: A pilot study. Int. J. Environ. Res. Public Health 2022, 20, 402. [Google Scholar] [CrossRef]
- Ping, N.; Li, H. Projection of fatigue and neuromuscular changes caused by different excises. Rev. Bras. de Med. do Esporte 2022, 28, 565–568. [Google Scholar] [CrossRef]
- Wilson, M.T.; Ryan, A.M.F.; Vallance, S.R.; Dias-Dougan, A.; Dugdale, J.H.; Hunter, A.M.; Hamilton, D.L.; Macgregor, L.J. Tensiomyography derived parameters reflect skeletal muscle architectural adaptations following 6-weeks of lower body resistance training. Front. Physiol. 2019, 10, 1493. [Google Scholar] [CrossRef]
- Fitts, R.H. The cross-bridge cycle and skeletal muscle fatigue. J. Appl. Physiol. 2008, 104, 551–558. [Google Scholar] [CrossRef]
- Boyas, S.; Guével, A. Neuromuscular fatigue in healthy muscle: Underlying factors and adaptation mechanisms. Ann. Phys. Rehabil. Med. 2011, 54, 88–108. [Google Scholar] [CrossRef] [PubMed]
- Dumke, C.L.; Pfaffenroth, C.M.; McBride, J.M.; McCauley, G.O. Relationship between muscle strength, power and stiffness and running economy in trained male runners. Int. J. Sports Physiol. Perform. 2010, 5, 249–261. [Google Scholar] [CrossRef] [PubMed]
- Robbins, D.W. Postactivation potentiation and its practical applicability: A brief review. J. Strength Cond. Res. 2005, 19, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Beato, M.; Madruga-Parera, M.; Piqueras-Sanchiz, F.; Moreno-Pérez, V.; Romero-Rodriguez, D. Acute effect of eccentric overload exercises on change of direction performance and lower-limb muscle contractile function. J. Strength Cond. Res. 2021, 35, 3327–3333. [Google Scholar] [CrossRef] [PubMed]
- Sale, D.G. Postactivation potentiation: Role in human performance. Exerc. Sport Sci. Rev. 2002, 30, 138–143. [Google Scholar] [CrossRef]
- Abazović, E.; Paravlić, A.; Zubac, D.; Kovačević, E.; Šimunič, B. Decomposition of tensiomyogram and comparison with torque twitch responses after post-activation potentiation. J. Musculoskelet. Neuronal Interact. 2022, 22, 316. [Google Scholar]
- Benjamin, P.J.; Lamp, S.P. Understanding Sports Massage; Human Kinetics Champaign: Champaign, IL, USA, 1996. [Google Scholar]
- Dakić, M.; Toskić, L.; Ilić, V.; Đurić, S.; Dopsaj, M.; Šimenko, J. The Effects of Massage Therapy on Sport and Exercise Performance: A Systematic Review. Sports 2023, 11, 110. [Google Scholar] [CrossRef]
- Wilke, J.; Vleeming, A.; Wearing, S. Overuse injury: The result of pathologically altered myofascial force transmission? Exerc. Sport Sci. Rev. 2019, 47, 230–236. [Google Scholar] [CrossRef]
- Lee, C.-L.; Chu, I.-H.; Lyu, B.-J.; Chang, W.-D.; Chang, N.-J. Comparison of vibration rolling, nonvibration rolling, and static stretching as a warm-up exercise on flexibility, joint proprioception, muscle strength, and balance in young adults. J. Sports Sci. 2018, 36, 2575–2582. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Measurement | Post-Fatigue Measurement | Post-Recovery Measurement | Prolonged Recovery Time Measurement | |||||
|---|---|---|---|---|---|---|---|---|
| Tc | Dm | Tc | Dm | Tc | Dm | Tc | Dm | |
| PR | 27.1 ± 4.1 | 10.0 ± 2.7 | 24.2 ± 5.1 | 7.4 ± 2.5 | 24.4 ± 4.1 | 7.7 ± 2.4 | 25.2 ± 3.8 | 7.9 ± 2.5 |
| PM | 26.2 ± 4.8 | 9.5 ± 3.5 | 21.9 ± 6.0 | 7.4 ± 3.1 | 21.4 ± 4.0 | 7.3 ± 3.1 | 22.5 ± 4.3 | 7.5 ± 3.1 |
| VM | 27.2 ± 5.0 | 9.8 ± 3.3 | 22.0 ± 5.5 | 7.2 ± 3.1 | 22.9 ± 5.0 | 7.2 ± 2.5 | 24.8 ± 5.8 | 8.0 ± 2.7 |
| MM | 26.9 ± 4.6 | 9.1 ± 2.6 | 22.2 ± 4.0 | 6.9 ± 2.9 | 23.7 ± 3.9 | 7.6 ± 2.8 | 24.5 ± 4.9 | 7.7 ± 2.5 |
| Interaction of Recovery Procedures | Wilks’ Lambda | F | Sig. | Eta Squared |
|---|---|---|---|---|
| Passive rest | 0.432 | 4.831 | 0.022 * | 0.568 |
| Percussive mechanical massage | 0.302 | 8.486 | 0.003 ** | 0.698 |
| Vibro-mechanical massage | 0.311 | 8.112 | 0.004 ** | 0.689 |
| Manual massage | 0.504 | 3.611 | 0.049 * | 0.496 |
| Recovery procedure × Measurement time point | 0.873 | 0.778 | 0.637 | 0.044 |
| Passive Rest | Percussive Mechanical Massage | Vibro-Mechanical Massage | Manual Massage | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Tc | Dm | Tc | Dm | Tc | Dm | Tc | Dm | ||
| BL | PF | 0.049 * | 0.002 ** | 0.049 * | 0.004 ** | 0.014 * | 0.022 * | 0.042 * | 0.047 * |
| PRC | 0.008 ** | 0.002 ** | 0.001 ** | 0.018 * | 0.043 * | 0.027 * | 0.030 * | 0.148 | |
| PRT | 0.028 * | 0.005 ** | 0.001 ** | 0.009 ** | 0.399 | 0.105 | 0.287 | 0.205 | |
| PF | PRC | 1 | 1 | 1 | 1 | 1 | 1 | 0.739 | 0.803 |
| PRT | 1 | 0.719 | 1 | 1 | 0.028 * | 0.246 | 0.45 | 1 | |
| PRC | PRT | 0.335 | 1 | 0.174 | 1 | 0.121 | 0.199 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dakić, M.; Ilić, V.; Toskić, L.; Duric, S.; Šimenko, J.; Marković, M.; Dopsaj, M.; Cuk, I. Acute Effects of Short-Term Massage Procedures on Neuromechanical Contractile Properties of Rectus Femoris Muscle. Medicina 2024, 60, 125. https://doi.org/10.3390/medicina60010125
Dakić M, Ilić V, Toskić L, Duric S, Šimenko J, Marković M, Dopsaj M, Cuk I. Acute Effects of Short-Term Massage Procedures on Neuromechanical Contractile Properties of Rectus Femoris Muscle. Medicina. 2024; 60(1):125. https://doi.org/10.3390/medicina60010125
Chicago/Turabian StyleDakić, Miloš, Vladimir Ilić, Lazar Toskić, Sasa Duric, Jožef Šimenko, Milan Marković, Milivoj Dopsaj, and Ivan Cuk. 2024. "Acute Effects of Short-Term Massage Procedures on Neuromechanical Contractile Properties of Rectus Femoris Muscle" Medicina 60, no. 1: 125. https://doi.org/10.3390/medicina60010125
APA StyleDakić, M., Ilić, V., Toskić, L., Duric, S., Šimenko, J., Marković, M., Dopsaj, M., & Cuk, I. (2024). Acute Effects of Short-Term Massage Procedures on Neuromechanical Contractile Properties of Rectus Femoris Muscle. Medicina, 60(1), 125. https://doi.org/10.3390/medicina60010125