


Comparative Study of Hematological Parameters and Biomarkers of Immunity and Inflammation in Patients with Psoriasis and Atopic Dermatitis

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
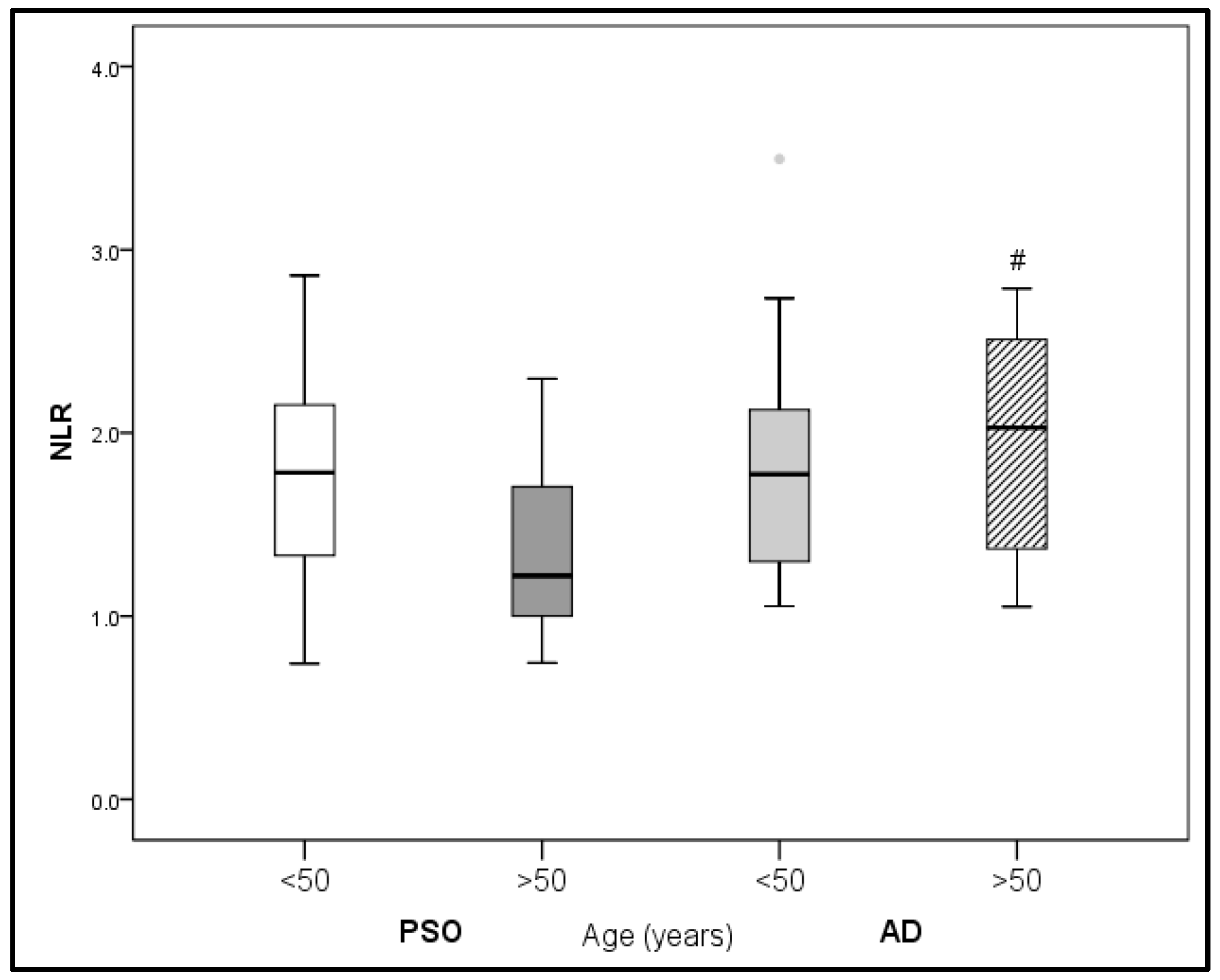
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, J.; Xiao, M.; Ma, K.; Li, H.; Ran, M.; Yang, S.; Yang, Y.; Fu, X.; Yang, S. Therapeutic effects of mesenchymal stem cells and their derivatives in common skin inflammatory diseases: Atopic dermatitis and psoriasis. Front. Immunol. 2023, 14, 1092668. [Google Scholar] [CrossRef] [PubMed]
- Ferroni, P.; Basili, S.; Falco, A.; Davì, G. Platelet activation in type 2 diabetes mellitus. J. Thromb. Haemost 2004, 2, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Kasperska-Zajac, A.; Brzoza, Z.; Rogala, B. Platelet function in cutaneous diseases. Platelets 2008, 19, 317–321, Erratum in Platelets 2009, 20, 74. [Google Scholar] [CrossRef]
- Sugimoto, E.; Matsuda, H.; Shibata, S.; Mizuno, Y.; Koyama, A.; Li, L.; Taira, H.; Ito, Y.; Awaji, K.; Yamashita, T.; et al. Impact of Pretreatment Systemic Inflammatory Markers on Treatment Persistence with Biologics and Conventional Systemic Therapy: A Retrospective Study of Patients with Psoriasis Vulgaris and Psoriatic Arthritis. J. Clin. Med. 2023, 12, 3046. [Google Scholar] [CrossRef]
- Klisic, A.; Radoman Vujačić, I.; Vučković, L.J.; Ninic, A. Total leukocyte count, leukocyte subsets and their indexes in relation to cardiovascular risk in adolescent population. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3038–3044. [Google Scholar] [CrossRef]
- Klisic, A.; Scepanovic, A.; Kotur-Stevuljevic, J.; Ninic, A. Novel leukocyte and thrombocyte indexes in patients with prediabetes and type 2 diabetes mellitus. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2775–2781. [Google Scholar] [CrossRef]
- Vukicevic, P.; Klisic, A.; Neskovic, V.; Babic, L.; Mikic, A.; Bogavac-Stanojevic, N.; Matkovic, M.; Putnik, S.; Aleksic, N.; Kotur-Stevuljevic, J. New Markers of Platelet Activation and Reactivity and Oxidative Stress Parameters in Patients Undergoing Coronary Artery Bypass Grafting. Oxid. Med. Cell. Longev. 2021, 2021, 8915253. [Google Scholar] [CrossRef]
- Zhou, G.; Ren, X.; Tang, Z.; Li, W.; Chen, W.; He, Y.; Wei, B.; Zhang, H.; Ma, F.; Chen, X.; et al. Exploring the association and causal effect between white blood cells and psoriasis using large-scale population data. Front. Immunol. 2023, 14, 1043380. [Google Scholar] [CrossRef]
- Liu, Z.; Perry, L.A.; Morgan, V. The association between platelet indices and presence and severity of psoriasis: A systematic review and meta-analysis. Clin. Exp. Med. 2023, 23, 333–346. [Google Scholar] [CrossRef]
- Akcal, O.; Taskırdı, İ. Do Platelet Count and mean Platelet Volume have a Predictive Role as a Marker in Children with Atopic Dermatitis? Indian. J. Dermatol. 2022, 67, 688–692. [Google Scholar] [CrossRef]
- Bakic, M.; Klisic, A.; Kocic, G.; Kocic, H.; Karanikolic, V. Oxidative stress and metabolic biomarkers in patients with psoriasis. J. Med. Biochem. 2023, 42, 1–9. [Google Scholar]
- Davizon-Castillo, P.; McMahon, B.; Aguila, S.; Bark, D.; Ashworth, K.; Allawzi, A.; Campbell, R.A.; Montenont, E.; Nemkov, T.; D’Alessandro, A.; et al. TNF-α-driven inflammation and mitochondrial dysfunction define the platelet hyperreactivity of aging. Blood 2019, 134, 727–740. [Google Scholar] [CrossRef]
- Yi, P.; Jiang, J.; Wang, Z.; Wang, X.; Zhao, M.; Wu, H.; Ding, Y. Comparison of mean platelet volume (MPV) and red blood cell distribution width (RDW) between psoriasis patients and controls: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0264504. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Geat, D.; Lippi, G.; Montagnana, M.; Girolomoni, G. Increased red blood cell distribution width in patients with plaque psoriasis. J. Med. Biochem. 2021, 40, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Conic, R.R.; Damiani, G.; Schrom, K.P.; Ramser, A.E.; Zheng, C.; Xu, R.; McCormick, T.S.; Cooper, K.D. Psoriasis and Psoriatic Arthritis Cardiovascular Disease Endotypes Identified by Red Blood Cell Distribution Width and Mean Platelet Volume. J. Clin. Med. 2020, 9, 186. [Google Scholar] [CrossRef] [PubMed]
- Krupka-Olek, M.; Bozek, A.; Drewienkowska, M.; Dryjka, K.; Medrala, A. Immunological differences between atopic dermatitis, psoriasis, and their combination in adult patients. Allergol. Immunopathol. 2022, 50, 143–146. [Google Scholar] [CrossRef]
- Bozek, A.; Zajac, M.; Krupka, M. Atopic Dermatitis and Psoriasis as Overlapping Syndromes. Mediat. Inflamm. 2020, 2020, 7527859. [Google Scholar] [CrossRef]
- Zhou, L.; Leonard, A.; Pavel, A.B.; Malik, K.; Raja, A.; Glickman, J.; Estrada, Y.D.; Peng, X.; Del Duca, E.; Sanz-Cabanillas, J.; et al. Age-specific changes in the molecular phenotype of patients with moderate-to-severe atopic dermatitis. J. Allergy Clin. Immunol. 2019, 144, 144–156. [Google Scholar] [CrossRef]
- Ferrucci, L.; Corsi, A.; Lauretani, F.; Bandinelli, S.; Bartali, B.; Taub, D.D.; Guralnik, J.M.; Longo, D.L. The origins of age-related proinflammatory state. Blood 2005, 105, 2294–2299. [Google Scholar] [CrossRef]
- Ventura, M.T.; Casciaro, M.; Gangemi, S.; Buquicchio, R. Immunosenescence in aging: Between immune cells depletion and cytokines up-regulation. Clin. Mol. Allergy 2017, 15, 21. [Google Scholar] [CrossRef]
- Cordoro, K.M.; Hitraya-Low, M.; Taravati, K.; Sandoval, P.M.; Kim, E.; Sugarman, J.; Pauli, M.L.; Liao, W.; Rosenblum, M.D. Skin-infiltrating, interleukin-22-producing T cells differentiate pediatric psoriasis from adult psoriasis. J. Am. Acad. Dermatol. 2017, 77, 417–424. [Google Scholar] [CrossRef]
- Hao, J.Q. Targeting interleukin-22 in psoriasis. Inflammation 2014, 37, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Tokura, Y.; Mori, T.; Hino, R. Psoriasis and other Th17-mediated skin diseases. J. UOEH 2010, 32, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Irvine, A.D.; Brunner, P.M.; Kim, B.S.; Boguniewicz, M.; Parmentier, J.; Platt, A.M.; Kabashima, K. The Role of Janus Kinase Signaling in the Pathology of Atopic Dermatitis. J. Allergy Clin. Immunol. 2023; in press. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Brunner, P.M.; Neumann, A.U.; Khattri, S.; Pavel, A.B.; Malik, K.; Singer, G.K.; Baum, D.; Gilleaudeau, P.; Sullivan-Whalen, M.; et al. Efficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by conventional treatments: A randomized, double-blind, phase 2a trial. J. Am. Acad. Dermatol. 2018, 78, 872–881.e6. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Li, Y.; Zhou, Y.; Follansbee, T.; Hwang, T.S. Immune mediators and therapies for pruritus in atopic dermatitis and psoriasis. J. Cutan. Immunol. Allergy 2019, 2, 4–14. [Google Scholar] [CrossRef]
- Sun, L.; Zhang, X. The immunological and genetic aspects in psoriasis. Appl. Inform. 2014, 1, 3. [Google Scholar] [CrossRef]
- Kaur, S.; Zilmer, K.; Leping, V.; Zilmer, M. Comparative study of systemic inflammatory responses in psoriasis vulgaris and mild to moderate allergic contact dermatitis. Dermatology 2012, 225, 54–61. [Google Scholar] [CrossRef]
- Kurtovic, N.O.; Halilovic, E.K. Serum Concentrations of Interferon Gamma (IFN-γ) in Patients with Psoriasis: Correlation with Clinical Type and Severity of the Disease. Med. Arch. 2018, 72, 410–413. [Google Scholar] [CrossRef]
- Arican, O.; Aral, M.; Sasmaz, S.; Ciragil, P. Serum levels of TNF-alpha, IFN-gamma, IL-6, IL-8, IL-12, IL-17, and IL-18 in patients with active psoriasis and correlation with disease severity. Mediat. Inflamm. 2005, 2005, 273–279. [Google Scholar] [CrossRef]
- Takahashi, H.; Tsuji, H.; Hashimoto, Y.; Ishida-Yamamoto, A.; Iizuka, H. Serum cytokines and growth factor levels in Japanese patients with psoriasis. Clin. Exp. Dermatol. 2010, 35, 645–649. [Google Scholar] [CrossRef]
- Wawrzycki, B.; Pietrzak, A.; Grywalska, E.; Krasowska, D.; Chodorowska, G.; Roliński, J. Interleukin-22 and Its Correlation with Disease Activity in Plaque Psoriasis. Arch. Immunol. Ther. Exp. 2019, 67, 103–108. [Google Scholar] [CrossRef]
- Nakajima, H.; Nakajima, K.; Tarutani, M.; Morishige, R.; Sano, S. Kinetics of circulating Th17 cytokines and adipokines in psoriasis patients. Arch. Dermatol. Res. 2011, 303, 451–455. [Google Scholar] [CrossRef][Green Version]
- Lo, Y.H.; Torii, K.; Saito, C.; Furuhashi, T.; Maeda, A.; Morita, A. Serum IL-22 correlates with psoriatic severity and serum IL-6 correlates with susceptibility to phototherapy. J. Dermatol. Sci. 2010, 58, 225–227. [Google Scholar] [CrossRef]
- Meephansan, J.; Ruchusatsawat, K.; Sindhupak, W.; Thorner, P.S.; Wongpiyabovorn, J. Effect of methotrexate on serum levels of IL-22 in patients with psoriasis. Eur. J. Dermatol. 2011, 21, 501–504. [Google Scholar] [CrossRef]
- Camela, E.; Potestio, L.; Fabbrocini, G.; Ruggiero, A.; Megna, M. New frontiers in personalized medicine in psoriasis. Expert Opin. Biol. Ther. 2022, 22, 1431–1433. [Google Scholar] [CrossRef]
- Bieber, T. Atopic dermatitis: An expanding therapeutic pipeline for a complex disease. Nat. Rev. Drug Discov. 2022, 21, 21–40. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | PsO | AD | p |
|---|---|---|---|
| WBC ×109/L | 7.14 (5.51–9.25) | 8.12 (5.41–9.13) | 0.950 |
| RBC ×1012/L | 4.76 (4.38–5.07) | 4.67 (4.40–4.99) | 0.736 |
| Hgb (g/L) | 147 (129–154) | 138 (125–147) | 0.104 |
| HCT (L/L) | 0.444 (0.409–0.458) | 0.424 (0.400–0.454) | 0.229 |
| MCV (fl) | 92.1 (89.4–94.7) | 90.6 (88.6–91.8) | 0.040 |
| MCH (pg) | 30.0 (29.2–31.9) | 29.4 (28.9–30.4) | 0.064 |
| MCHC (g/L) | 329 (323–336) | 323 (321–332) | 0.129 |
| RDW CV (%) | 12.7 (12.3–13.6) | 13.3 (12.6–13.7) | 0.058 |
| PLT ×109/L | 240 (200–308) | 261 (213–313) | 0.384 |
| MPV (fl) | 9.85 (8.95–10.65) | 9.43 (8.85–10.15) | 0.179 |
| PCT (L/L) | 0.0023 (0.0020–0.0029) | 0.0024 (0.0022–0.0028) | 0.503 |
| PDW (fl) | 11.1 (9.2–12.6) | 10.4 (9.0–11.3) | 0.173 |
| Neutrophils ×109/L | 3.66 (2.60–4.89) | 4.62 (2.52–5.07) | 0.373 |
| Lymphocytes ×109/L | 2.29 (2.04–2.98) | 2.26 (1.85–2.56) | 0.400 |
| Monocytes ×109/L | 0.63 (0.51–0.79) | 0.62 (0.51–0.76) | 0.583 |
| Eosinophils ×109/L | 0.19 (0.11–0.27) | 0.19 (0.13–0.39) | 0.335 |
| Basophils ×109/L | 0.05 (0.03–0.07) | 0.06 (0.03–0.06) | 0.672 |
| MPR | 0.042 (0.032–0.051) | 0.038 (0.030–0.045) | 0.233 |
| RPR | 0.055 (0.043–0.079) | 0.051 (0.043–0.063) | 0.773 |
| Parameter | PsO | AD | p |
|---|---|---|---|
| CRP (mg/L) | 1.55 (0.70–4.55) | 1.80 (0.60–4.20) | 0.682 |
| NLR | 1.51 (1.05–2.08) | 1.77 (1.29–2.27) | 0.100 |
| PLR | 100 (82–120) | 109 (82–139) | 0.252 |
| IFN-γ (pg/mL) | 20.3 (17.1–24.5) | 19.0 (16.9–22.5) | 0.381 |
| IL-22 (pg/mL) | 59.2 (57.6–69.0) | 68.5 (57.0–76.5) | 0.216 |
| Parameter | PsO | AD | p | ||
|---|---|---|---|---|---|
| Without Comorbidities n = 19 | With Comorbidities n = 21 | Without Comorbidities n = 20 | With Comorbidities n = 20 | ||
| PLT ×109/L | 265 (233–316) | 223 (158–244) a | 267 (237–315) | 234 (172–275) | 0.059 |
| PCT (L/L) | 0.0027 (0.0022–0.0029) | 0.0021 (0.0018–0.0025) a | 0.0026 (0.0024–0.0029) | 0.0023 (0.0018–0.0024) c | 0.044 |
| Lymphocytes (%) | 31.1 (26.5–36.4) | 37.4 (31.6–42.5) a | 29.9 (24.2–34.7) | 33.5 (27.8–40.8) | 0.030 |
| PLR | 112 (97–137) | 96 (60–107) a | 124 (98–165) | 96 (81–115) c | 0.008 |
| MPR | 0.033 (0.029–0.044) | 0.044 (0.036–0.062) a | 0.038 (0.029–0.040) | 0.040 (0.031–0.054) | 0.052 |
| RPR | 0.050 (0.040–0.058) | 0.057 (0.052–0.087) a | 0.050 (0.043–0.055) | 0.058 (0.044–0.088) c | 0.103 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakic, M.; Klisic, A.; Karanikolic, V. Comparative Study of Hematological Parameters and Biomarkers of Immunity and Inflammation in Patients with Psoriasis and Atopic Dermatitis. Medicina 2023, 59, 1622. https://doi.org/10.3390/medicina59091622
Bakic M, Klisic A, Karanikolic V. Comparative Study of Hematological Parameters and Biomarkers of Immunity and Inflammation in Patients with Psoriasis and Atopic Dermatitis. Medicina. 2023; 59(9):1622. https://doi.org/10.3390/medicina59091622
Chicago/Turabian StyleBakic, Mirjana, Aleksandra Klisic, and Vesna Karanikolic. 2023. "Comparative Study of Hematological Parameters and Biomarkers of Immunity and Inflammation in Patients with Psoriasis and Atopic Dermatitis" Medicina 59, no. 9: 1622. https://doi.org/10.3390/medicina59091622
APA StyleBakic, M., Klisic, A., & Karanikolic, V. (2023). Comparative Study of Hematological Parameters and Biomarkers of Immunity and Inflammation in Patients with Psoriasis and Atopic Dermatitis. Medicina, 59(9), 1622. https://doi.org/10.3390/medicina59091622