
Can Routine Laboratory Tests Be Suggestive in Determining Suspicions of Malignancy in the Case of Thyroid Nodules?
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kobaly, K.; Kim, C.S.; Mandel, S.J. Contemporary Management of Thyroid Nodules. Annu. Rev. Med. 2022, 73, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Farrell, S.G.; Grossmann, M. Thyroid nodules: Diagnosis and management. Med. J. Aust. 2018, 209, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C. Thyroid carcinoma in nodules with Thy3 cytology: Retrospective study in a district general hospital. Acta Biomed. 2022, 93, e2022288. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Wang, F.; Yang, W.; Zheng, Y.; Liu, C.; Huang, L.; Li, L.; Cheng, H.; Cai, H.; Li, X.; et al. Association Between Genetic Risk, Adherence to Healthy Lifestyle Behavior, and Thyroid Cancer Risk. JAMA Netw. Open 2022, 5, e2246311. [Google Scholar] [CrossRef]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef]
- Malhi, H.S.; Grant, E.G. Ultrasound of Thyroid Nodules and the Thyroid Imaging Reporting and Data System. Neuroimaging Clin. N. Am. 2021, 31, 285–300. [Google Scholar] [CrossRef]
- Liang, F.; Li, X.; Ji, Q.; He, D.; Yang, M.; Xu, Z. Revised Thyroid Imaging Reporting and Data System (TIRADS): Imitating the American College of Radiology TIRADS, a single-center retrospective study. Quant. Imaging Med. Surg. 2023, 13, 3862–3872. [Google Scholar] [CrossRef]
- Tang, J.; Ma, J.; Xi, X.; Wang, L.; Li, H.; Huo, S.; Zhang, B. Real-life utility of five-gene panel test in preoperative thyroid fine-needle aspiration biopsy: A large cohort of 740 patients study. Endocrine 2022, 80, 552–562. [Google Scholar] [CrossRef]
- Wesoła, M.; Jeleń, M. Bethesda System in the evaluation of thyroid nodules: Review. Adv. Clin. Exp. Med. 2017, 26, 177–182. [Google Scholar] [CrossRef]
- Matei, S.C.; Matei, M.; Anghel, F.M.; Carabenciov, E.; Murariu, M.S.; Olariu, S. Utility of routine laboratory tests in the assessment of chronic venous disease progression in female patients. Exp. Ther. Med. 2022, 24, 571. [Google Scholar] [CrossRef]
- Cheong, T.Y.; Hong, S.D.; Jung, K.W.; So, Y.K. The diagnostic predictive value of neutrophil-to-lymphocyte ratio in thyroid cancer adjusted for tumor size. PLoS ONE 2021, 16, e0251446. [Google Scholar] [CrossRef] [PubMed]
- Guth, S.; Theune, U.; Aberle, J.; Galach, A.; Bamberger, C.M. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur. J. Clin. Investig. 2009, 39, 699–706. [Google Scholar] [CrossRef]
- Wang, W.; Chang, J.; Jia, B.; Liu, J. The Blood Biomarkers of Thyroid Cancer. Cancer Manag. Res. 2020, 12, 5431–5438. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Li, C.; Lu, W.; Wang, C.; Ai, Z. Quantitative assessment of preoperative serum thyrotropin level and thyroid cancer. Oncotarget 2016, 7, 34918–34929. [Google Scholar] [CrossRef]
- Aktas, G.; Sit, M.; Dikbas, O.; Erkol, H.; Altinordu, R.; Erkus, E.; Savli, H. Elevated neutrophil-to-lymphocyte ratio in the diagnosis of Hashimoto’s thyroiditis. Rev. Assoc. Medica Bras. (1992) 2017, 63, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, M.; Fiorentino, V.; Martini, M.; Capodimonti, S.; Cenci, T.; Lombardi, C.P.; Raffaelli, M.; Pontecorvi, A.; Fadda, G.; Pantanowitz, L.; et al. How limited molecular testing can also offer diagnostic and prognostic evaluation of thyroid nodules processed with liquid-based cytology: Role of TERT promoter and BRAF V600E mutation analysis. Cancer Cytopathol. 2021, 129, 819–829. [Google Scholar] [CrossRef]
- C-Vuong, H.G.; Altibi, A.M.A.; Duong, U.N.P.; Hassell, L. Prognostic implication of BRAF and TERT promoter mutation combina-tion in papillary thyroid carcinoma-A meta-analysis. Clin. Endocrinol. 2017, 87, 411–417. [Google Scholar] [CrossRef]
- D-Chijioke, O. The value of molecular testing of thy-roid aspirates. Pathologe 2022, 43, 105–108. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Off. J. Am. Thyroid Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M.; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid Off. J. Am. Thyroid Assoc. 2009, 19, 1167–1214. [Google Scholar] [CrossRef]
- Hoang, J. Thyroid nodules and evaluation of thyroid cancer risk. Australas. J. Ultrasound Med. 2010, 13, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, M.; Gravina, C.; Cocomazzi, A.; Capodimonti, S.; Musarra, T.; Sfregola, S.; Fiorentino, V.; Revelli, L.; Martini, M.; Fadda, G.; et al. A large series of hyalinizing trabecular tumors: Cytomorphology and ancillary techniques on fine needle aspiration. Cancer Cytopathol. 2019, 127, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Weng, M.; Zhao, W.; Yue, Y.; Guo, M.; Nan, K.; Liao, Q.; Sun, M.; Zhou, D.; Miao, C. High preoperative white blood cell count determines poor prognosis and is associated with an immunosuppressive microenvironment in colorectal cancer. Front. Oncol. 2022, 12, 943423. [Google Scholar] [CrossRef]
- Machairas, N.; Kostakis, I.D.; Prodromidou, A.; Stamopoulos, P.; Feretis, T.; Garoufalia, Z.; Damaskos, C.; Tsourouflis, G.; Kouraklis, G. Trends in white blood cell and platelet indices in a comparison of patients with papillary thyroid carcinoma and multinodular goiter do not permit differentiation between the conditions. Endocr. Res. 2017, 42, 311–317. [Google Scholar] [CrossRef]
- Lee, K.H.; Seok, E.Y.; Kim, E.Y.; Yun, J.S.; Park, Y.L.; Park, C.H. Different prognostic values of individual hematologic parameters in papillary thyroid cancer due to age-related changes in immunity. Ann. Surg. Treat. Res. 2019, 96, 70–77. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Haroon Al Rasheed, M.R.; Xu, B. Molecular Alterations in Thyroid Carcinoma. Surg. Pathol. Clin. 2019, 12, 921–930. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Bastid, J.; Bonnefoy, N.; Eliaou, J.F.; Bensussan, A. Lymphocyte-derived interleukin-17A adds another brick in the wall of inflammation-induced breast carcinogenesis. Oncoimmunology 2014, 3, e28273. [Google Scholar] [CrossRef]
- Ozmen, S.; Timur, O.; Calik, I.; Altinkaynak, K.; Simsek, E.; Gozcu, H.; Arslan, A.; Carlioglu, A. Neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) may be superior to C-reactive protein (CRP) for predicting the occurrence of differentiated thyroid cancer. Endocr. Regul. 2017, 51, 131–136. [Google Scholar] [CrossRef]
- Galdiero, M.R.; Varricchi, G.; Loffredo, S.; Bellevicine, C.; Lansione, T.; Ferrara, A.L.; Iannone, R.; di Somma, S.; Borriello, F.; Clery, E.; et al. Potential involvement of neutrophils in human thyroid cancer. PLoS ONE 2018, 13, e0199740. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.L.; Lee, J.J.; Liu, T.P.; Chang, Y.C.; Hsu, Y.C.; Cheng, S.P. Blood neutrophil-to-lymphocyte ratio correlates with tumor size in patients with differentiated thyroid cancer. J. Surg. Oncol. 2013, 107, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Du, J.; Fan, J.; Liu, K.; Zhang, B.; Wang, S.; Wang, W.; Wang, Z.; Cai, Y.; Li, C.; et al. The Neutrophil-to-Lymphocyte Ratio Correlates with Age in Patients with Papillary Thyroid Carcinoma. ORL 2015, 77, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Kutluturk, F.; Gul, S.S.; Sahin, S.; Tasliyurt, T. Comparison of Mean Platelet Volume, Platelet Count, Neutrophil/ Lymphocyte Ratio and Platelet/Lymphocyte Ratio in the Euthyroid, Overt Hypothyroid and Subclinical Hyperthyroid Phases of Papillary Thyroid Carcinoma. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Wang, Y.; Shan, G.; Gao, L. Clinical and prognostic value of neutrophil-lymphocyte ratio for patients with thyroid cancer: A meta-analysis. Medicine 2020, 99, e19686. [Google Scholar] [CrossRef] [PubMed]
- Yin, T.; He, S.; Liu, X.; Jiang, W.; Ye, T.; Lin, Z.; Sang, Y.; Su, C.; Wan, Y.; Shen, G.; et al. Extravascular red blood cells and hemoglobin promote tumor growth and therapeutic resistance as endogenous danger signals. J. Immunol. 2015, 194, 429–437. [Google Scholar] [CrossRef]
- Kawa, M.P.; Grymula, K.; Paczkowska, E.; Baskiewicz-Masiuk, M.; Dabkowska, E.; Koziolek, M.; Tarnowski, M.; Kłos, P.; Dziedziejko, V.; Kucia, M.; et al. Clinical relevance of thyroid dysfunction in human haematopoiesis: Biochemical and molecular studies. Eur. J. Endocrinol. 2010, 162, 295–305. [Google Scholar] [CrossRef]
- Imam, S.; Paparodis, R.D.; Rafiqi, S.I.; Ali, S.; Niaz, A.; Kanzy, A.; Tovar, Y.E.; Madkhali, M.A.; Elsherif, A.; Khogeer, F.; et al. Thyroid Cancer Screening Using Tumor-Associated DN T Cells as Immunogenomic Markers. Front. Oncol. 2022, 12, 891002. [Google Scholar] [CrossRef]
- Liu, Q.; Sun, W.; Zhang, H. Roles and new Insights of Macrophages in the Tumor Microenvironment of Thyroid Cancer. Front. Pharmacol. 2022, 13, 875384. [Google Scholar] [CrossRef]
- Ogilvie, J.B.; Piatigorsky, E.J.; Clark, O.H. Current status of fine needle aspiration for thyroid nodules. Adv. Surg. 2016, 40, 223–238. [Google Scholar] [CrossRef]
- Varricchi, G.; Galdiero, M.R.; Loffredo, S.; Lucarini, V.; Marone, G.; Mattei, F.; Marone, G.; Schiavoni, G. Eosinophils: The unsung heroes in cancer? Oncoimmunology 2017, 7, e1393134. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.; Mustata, T.; Enache, O.; Ion, O.; Chifulescu, A.; Sirbu, A.; Barbu, C.; Miron, A.; Giulea, C.; Andrei, F.; et al. Platelet Activation and Inflammation in Patients with Papillary Thyroid Cancer. Diagnostics 2021, 11, 1959. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.S.; Zhang, T.T.; Xue, D.X.; Wu, W.L.; Wang, Y.L.; Wang, Y.; Ji, Q.H.; Zhu, Y.X.; Qu, N.; Shi, R.L. Metabolic reprogramming and its clinical application in thyroid cancer. Oncol. Lett. 2019, 18, 1579–1584. [Google Scholar] [CrossRef]
- Destek, S.; Benturk, B.; Yapalak, Y.; Ozer, O.F. Clinical Significance of Erythrocyte Sedimentation Rate, Leukocyte, Fibrinogen, C-Reactive Protein, and Pentraxin 3 Values in Thyroid Nodules. Sisli Etfal Hastanesi Tip Bul. 2022, 56, 270–275. [Google Scholar] [CrossRef]
- Liotti, F.; Visciano, C.; Melillo, R.M. Inflammation in thyroid oncogenesis. Am. J. Cancer Res. 2012, 2, 286–297. [Google Scholar]
- Jianyong, L.; Zhihui, L.; Rixiang, G.; Jingqiang, Z. Using a nomogram based on preoperative serum fibrinogen levels to predict recurrence of papillary thyroid carcinoma. BMC Cancer 2018, 18, 390. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Cho, J.H.; Kim, J.H.; Yoo, E.G.; Kim, G.H.; Yoo, H.W. Variable Clinical Characteristics and Molecular Spectrum of Patients with Syndromes of Reduced Sensitivity to Thyroid Hormone: Genetic Defects in the THRB and SLC16A2 Genes. Horm. Res. Paediatr. 2018, 90, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Sasson, M.; Kay-Rivest, E.; Shoukrun, R.; Florea, A.; Hier, M.; Forest, V.I.; Tamilia, M.; Payne, R.J. The T4/T3 quotient as a risk factor for differentiated thyroid cancer: A case control study. J. Otolaryngol.–Head Neck Surg 2017, 46, 28. [Google Scholar] [CrossRef]
- Pasqualetti, G.; Schirripa, M.; Dochy, E.; Fassan, M.; Ziranu, P.; Puzzoni, M.; Scartozzi, M.; Alberti, G.; Lonardi, S.; Zagonel, V.; et al. Thyroid hormones ratio is a major prognostic marker in advanced metastatic colorectal cancer: Results from the phase IIIrandomised CORRECT trial. Eur. J. Cancer 2020, 133, 66–73. [Google Scholar] [CrossRef]
- Baliram, R.; Latif, R.; Zaidi, M.; Davies, T.F. Expanding the Role of Thyroid-Stimulating Hormone in Skeletal Physiology. Front. Endocrinol. 2017, 8, 252. [Google Scholar] [CrossRef]
- Estrada, J.M.; Soldin, D.; Buckey, T.M.; Burman, K.D.; Soldin, O.P. Thyrotropin isoforms: Implications for thyrotropin analysis and clinical practice. Thyroid Off. J. Am. Thyroid Assoc. 2014, 24, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Yuan, I.J.; Mirshahidi, S.; Simental, A.; Lee, S.C.; Yuan, X. Thyroid Carcinoma: Phenotypic Features, Underlying Biology and Potential Relevance for Targeting Therapy. Int. J. Mol. Sci. 2021, 22, 1950. [Google Scholar] [CrossRef] [PubMed]
- Ieni, A.; Vita, R.; Pizzimenti, C.; Benvenga, S.; Tuccari, G. Intratumoral Heterogeneity in Differentiated Thyroid Tumors: An Intriguing Reappraisal in the Era of Personalized Medicine. J. Pers. Med. 2021, 11, 333. [Google Scholar] [CrossRef]
- Razvi, S.; Bhana, S.; Mrabeti, S. Challenges in Interpreting Thyroid Stimulating Hormone Results in the Diagnosis of Thyroid Dysfunction. J. Thyroid Res. 2019, 2019, 4106816. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, V.; Dell’Aquila, M.; Musarra, T.; Martini, M.; Capodimonti, S.; Fadda, G.; Curatolo, M.; Traini, E.; Raffaelli, M.; Lombardi, C.P.; et al. The Role of Cytology in the Diagnosis of Subcentimeter Thyroid Lesions. Diagnostics 2021, 11, 1043. [Google Scholar] [CrossRef] [PubMed]
- Miao, S.; Jing, M.; Sheng, R.; Cui, D.; Lu, S.; Zhang, X.; Jing, S.; Zhang, X.; Shan, T.; Shan, H.; et al. The analysis of differential diagnosis of benign and malignant thyroid nodules based on ultrasound reports. Gland Surg. 2020, 9, 653–660. [Google Scholar] [CrossRef]
- King, A.D. Imaging for staging and management of thyroid cancer. Cancer Imaging 2008, 8, 57–69. [Google Scholar] [CrossRef]
- Livhits, M.J.; Zhu, C.Y.; Kuo, E.J.; Nguyen, D.T.; Kim, J.; Tseng, C.H.; Leung, A.M.; Rao, J.; Levin, M.; Douek, M.L.; et al. Effectiveness of Molecular Testing Techniques for Diagnosis of Indeterminate Thyroid Nodules: A Randomized Clinical Trial. JAMA Oncol. 2021, 7, 70–77. [Google Scholar] [CrossRef]
- Feldkamp, J.; Führer, D.; Luster, M.; Musholt, T.J.; Spitzweg, C.; Schott, M. Fine Needle Aspiration in the Investigation of Thyroid Nodules. Dtsch. Arztebl. Int. 2016, 113, 353–359. [Google Scholar] [CrossRef]

{kind=link}
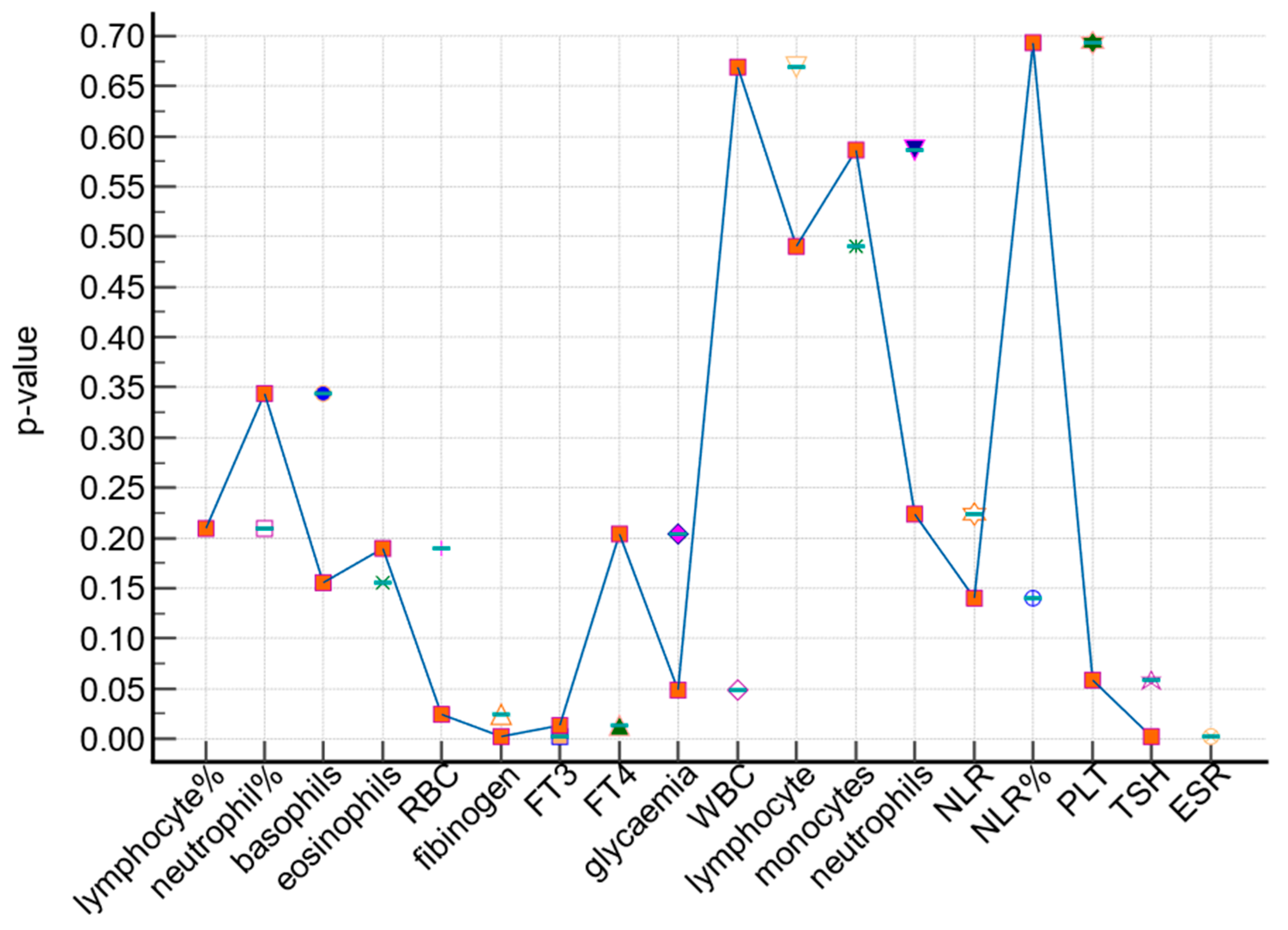
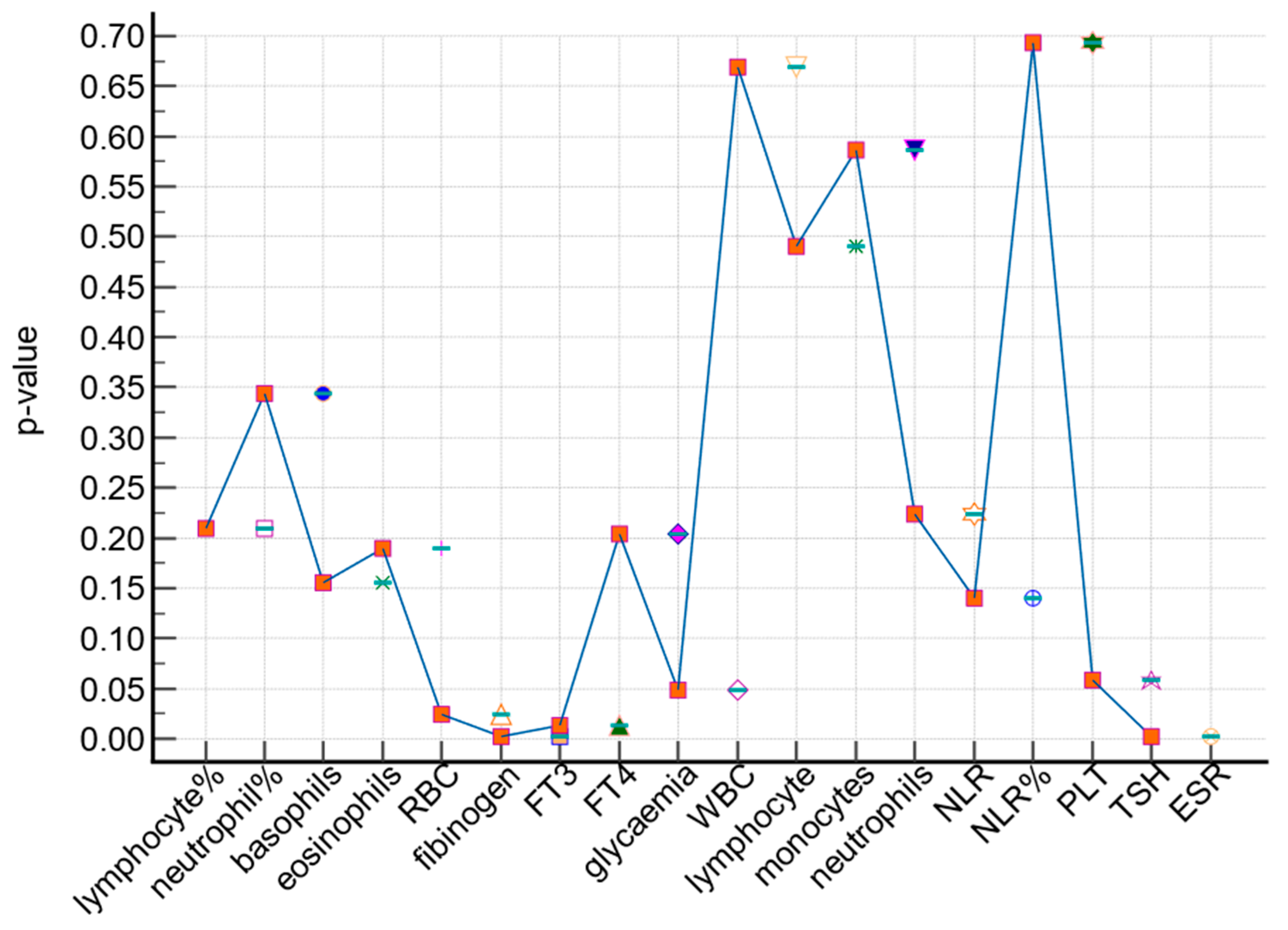
| Laboratory Parameters | Study Group (n = 251) | Control Group (n = 594) | p-Value * |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| RBC | 4.86 ± 2.73 | 4.63 ± 0.44 | 0.189 |
| WBC | 7.79 ± 2.15 | 7.48 ± 1.85 | 0.0486 |
| neutrophils | 5 ± 1.58 | 4.6 ± 1.53 | 0.587 |
| lymphocytes | 2.09 ± 0.68 | 2.08 ± 0.69 | 0.669 |
| monocytes | 0.53 ± 0.69 | 0.5 ± 0.66 | 0.49 |
| eosinophils | 0.14 ± 0.11 | 0.15 ± 0.16 | 0.155 |
| basophils | 0.035 ± 0.022 | 0.033 ± 0.027 | 0.3442 |
| neutrophil% | 63.04 ± 8.14 | 62.17 ± 11.29 | 0.2092 |
| lymphocyte% | 27.07 ± 7.45 | 28.20 ± 8.41 | 0.027 |
| PLT | 259.2 ± 60.77 | 261.13 ± 68.85 | 0.6938 |
| ESR | 16.07 ± 6.48 | 11.04 ± 5.52 | 0.002 |
| fibrinogen | 368.5 ± 97.57 | 352.9 ± 89.14 | 0.0238 |
| glycaemia | 109.02 ± 27.54 | 106.30 ± 28.44 | 0.2043 |
| FT3 | 5.17 ± 0.7 | 4.97 ± 1.08 | 0.0018 |
| FT4 | 15.5 ± 6.9 | 14.4 ± 3.45 | 0.0131 |
| TSH | 1.93 ± 1.88 | 1.98 ± 3.71 | 0.0581 |
| NLR% | 2.64 ± 1.33 | 2.55 ± 1.44 | 0.14 |
| NLR | 2.64 ± 1.33 | 2.49 ± 1.94 | 0.2242 |
| Laboratory Parameters | Study Group | Control Group | p-Value * |
|---|---|---|---|
| Papillary Thyroid Cancer | Nodular Goiter | ||
| (n = 133) | (n = 394) | ||
| Mean ± SD | Mean ± SD | ||
| RBC | 4.96 ± 3.75 | 4.62 ± 0.43 | 0.302 |
| WBC | 7.65 ± 2.15 | 7.54 ± 1.86 | 0.039 |
| neutrophils | 4.92 ± 1.45 | 4.65 ± 1.53 | 0.472 |
| lymphocytes | 2.03 ± 0.68 | 2.07 ± 0.69 | 0.830 |
| monocytes | 0.47 ± 0.18 | 0.53 ± 0.81 | 0.168 |
| eosinophils | 0.14 ± 0.11 | 0.16 ± 0.16 | 0.180 |
| basophils | 0.03 ± 0.02 | 0.03 ± 0.03 | 0.726 |
| neutrophil% | 63.80 ± 8.03 | 62.45 ± 12.24 | 0.152 |
| lymphocyte% | 26.33 ± 7.05 | 27.94 ± 8.31 | 0.050 |
| PLT | 257.94 ± 59.10 | 261.87 ± 65.78 | 0.544 |
| ESR | 16.12 ± 6.50 | 10.95 ± 5.63 | 0.038 |
| fibrinogen | 364.75 ± 90.18 | 357.46 ± 91.29 | 0.049 |
| glycaemia | 108.46 ± 27.77 | 107.64 ± 30.89 | 0.152 |
| FT3 | 5.15 ± 0.63 | 5.01 ± 1.00 | 0.050 |
| FT4 | 15.85 ± 9.26 | 14.83 ± 3.14 | 0.001 |
| TSH | 2.10 ± 2.38 | 2.10 ± 2.38 | 0.065 |
| NLR% | 2.77 ± 1.50 | 2.55 ± 1.30 | 0.041 |
| NLR | 2.72 ± 1.49 | 2.48 ± 1.30 | 0.054 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matei, M.; Vlad, M.M.; Golu, I.; Dumitru, C.Ș.; De Scisciolo, G.; Matei, S.-C. Can Routine Laboratory Tests Be Suggestive in Determining Suspicions of Malignancy in the Case of Thyroid Nodules? Medicina 2023, 59, 1488. https://doi.org/10.3390/medicina59081488
Matei M, Vlad MM, Golu I, Dumitru CȘ, De Scisciolo G, Matei S-C. Can Routine Laboratory Tests Be Suggestive in Determining Suspicions of Malignancy in the Case of Thyroid Nodules? Medicina. 2023; 59(8):1488. https://doi.org/10.3390/medicina59081488
Chicago/Turabian StyleMatei, Mervat, Mihaela Maria Vlad, Ioana Golu, Cristina Ștefania Dumitru, Graziano De Scisciolo, and Sergiu-Ciprian Matei. 2023. "Can Routine Laboratory Tests Be Suggestive in Determining Suspicions of Malignancy in the Case of Thyroid Nodules?" Medicina 59, no. 8: 1488. https://doi.org/10.3390/medicina59081488
APA StyleMatei, M., Vlad, M. M., Golu, I., Dumitru, C. Ș., De Scisciolo, G., & Matei, S.-C. (2023). Can Routine Laboratory Tests Be Suggestive in Determining Suspicions of Malignancy in the Case of Thyroid Nodules? Medicina, 59(8), 1488. https://doi.org/10.3390/medicina59081488