

Radiation Therapy Changed the Second Malignancy Pattern in Rectal Cancer Survivors
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patients
2.3. Statistical Analyses
3. Results
3.1. Demographics of Patients with First Primary Rectal Cancer
3.2. Second Cancer Site Analysis between the No Radiotherapy (RT) and RT Patients
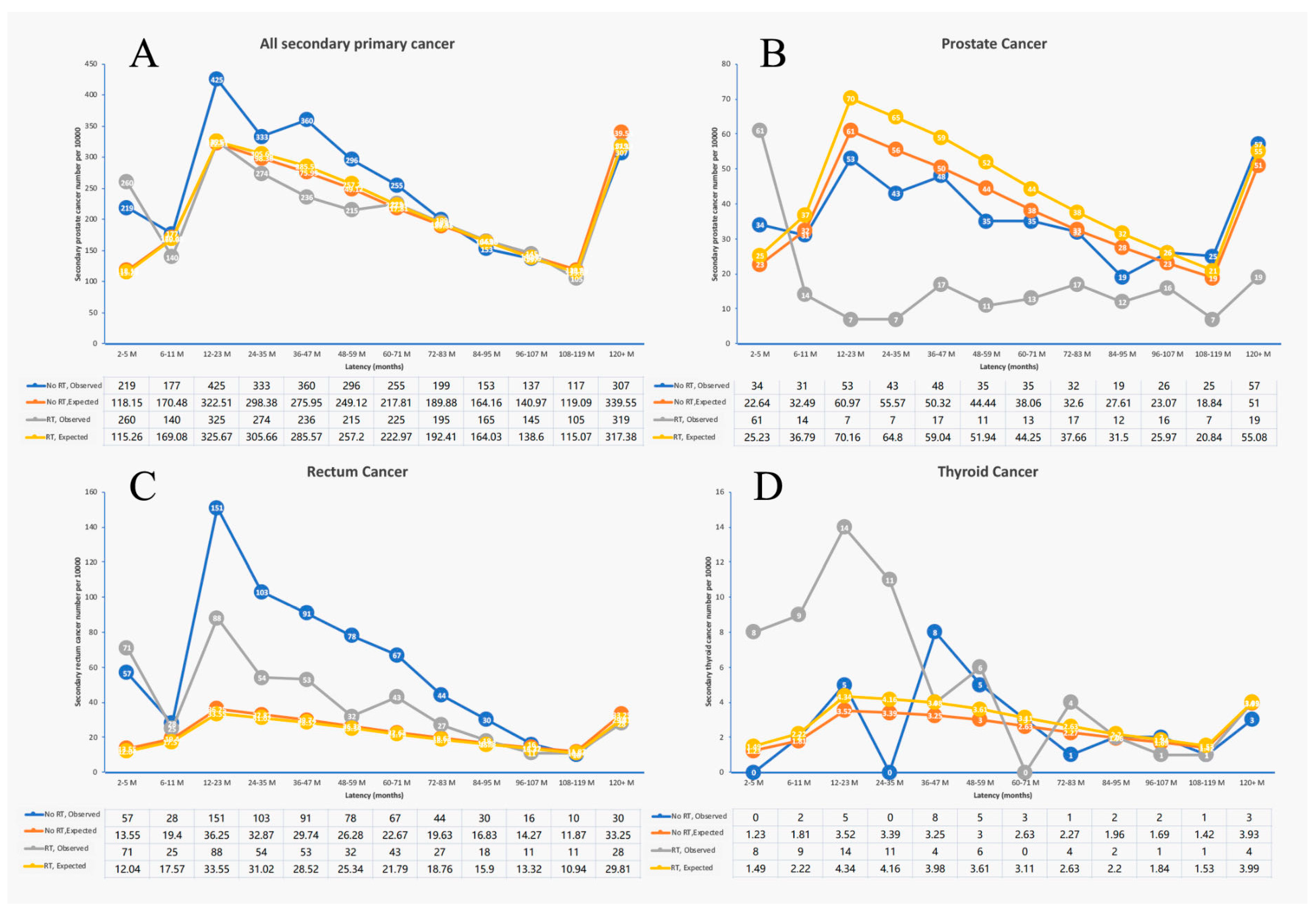
3.3. Latency Period Analysis of Second Primary Malignancy between the No RT and RT Patients
3.4. Clinical–Pathological Characteristics between Secondary Prostate Cancer of Rectal Cancer after RT or without RT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SEER | Surveillance, Epidemiology, and End Results |
| SPM | Second primary malignancy |
| IMRT | Intensity-modulated radiation therapy |
| RT | Radiotherapy |
| SIR | Standardized incidence ratios |
References
- Patel, S.G.; Karlitz, J.J.; Yen, T.; Lieu, C.H.; Boland, C.R. The rising tide of early-onset colorectal cancer: A comprehensive review of epidemiology, clinical features, biology, risk factors, prevention, and early detection. Lancet Gastroenterol. Hepatol. 2022, 7, 262–274. [Google Scholar] [CrossRef]
- Biller, L.H.; Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. JAMA 2021, 325, 669–685. [Google Scholar] [CrossRef]
- Yang, J.; Wu, F.; An, H.; Gan, H. Incidence and risk outcomes of second primary malignancy of patients with post-operative colorectal cancer. Int. J. Colorectal. Dis. 2023, 38, 88. [Google Scholar] [CrossRef]
- Wang, T.-H.; Liu, C.-J.; Chao, T.-F.; Chen, T.-J.; Hu, Y.-W. Second primary malignancy risk after radiotherapy in rectal cancer survivors. World J. Gastroenterol. 2018, 24, 4586–4595. [Google Scholar] [CrossRef] [PubMed]
- Shirvani, S.M.; Huntzinger, C.J.; Melcher, T.; Olcott, P.D.; Voronenko, Y.; Bartlett-Roberto, J.; Mazin, S. Biology-guided radiotherapy: Redefining the role of radiotherapy in metastatic cancer. Br. J. Radiol. 2021, 94, 20200873. [Google Scholar] [CrossRef]
- Yu, S.; Wang, Y.; He, P.; Shao, B.; Liu, F.; Xiang, Z.; Yang, T.; Zeng, Y.; He, T.; Ma, J.; et al. Effective Combinations of Immunotherapy and Radiotherapy for Cancer Treatment. Front. Oncol. 2022, 12, 809304. [Google Scholar] [CrossRef]
- Diefenhardt, M.; Ludmir, E.B.; Hofheinz, R.-D.; Ghadimi, M.; Minsky, B.D.; Rödel, C.; Fokas, E. Association of Sex with Toxic Effects, Treatment Adherence, and Oncologic Outcomes in the CAO/ARO/AIO-94 and CAO/ARO/AIO-04 Phase 3 Randomized Clinical Trials of Rectal Cancer. JAMA Oncol. 2020, 6, 294–296. [Google Scholar] [CrossRef]
- Hong, T.S.; Ryan, D.P. Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer-The New Standard of Care? JAMA Oncol. 2018, 4, e180070. [Google Scholar] [CrossRef] [PubMed]
- Arezzo, A.; Arolfo, S.; Allaix, M.E.; Munoz, F.; Cassoni, P.; Monagheddu, C.; Ricardi, U.; Ciccone, G.; Morino, M. Results of neoadjuvant short-course radiation therapy followed by transanal endoscopic microsurgery for t1-t2 n0 extraperitoneal rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Rombouts, A.J.M.; Hugen, N.; Elferink, M.A.G.; Feuth, T.; Poortmans, P.M.P.; Nagtegaal, I.D.; de Wilt, J.H.W. Incidence of second tumors after treatment with or without radiation for rectal cancer. Ann. Oncol. 2017, 28, 535–540. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, T.; Liu, C.; Wang, W.; Zhai, J.; Han, X.; Nie, C.; Ren, X.; Zhu, X.; Xiang, G.; et al. Risk and Prognosis of Second Primary Cancers among Ovarian Cancer Patients, Based on SEER Database. Cancer Investig. 2022, 40, 604–620. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Gao, J.; Hu, J.; Hu, W.; Qiu, X.; Huang, Q.; Kong, L.; Lu, J.J. Carbon-ion radiotherapy in the treatment of radiation-induced second primary malignancies. Ann. Transl. Med. 2022, 10, 1200. [Google Scholar] [CrossRef]
- Avgousti, R.; Antypas, C.; Armpilia, C.; Simopoulou, F.; Liakouli, Z.; Karaiskos, P.; Kouloulias, V.; Kyrodimos, E.; Moulopoulos, L.A.; Zygogianni, A. Adaptive radiation therapy: When, how and what are the benefits that literature provides? Cancer Radiother. 2022, 26, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Pointer, K.B.; Pitroda, S.P.; Weichselbaum, R.R. Radiotherapy and immunotherapy: Open questions and future strategies. Trends Cancer 2022, 8, 9–20. [Google Scholar] [CrossRef]
- Lu, M.; Liu, H.; Zheng, B.; Sun, S.; Chen, C. Links between Breast and Thyroid Cancer: Hormones, Genetic Susceptibility and Medical Interventions. Cancers 2022, 14, 5117. [Google Scholar] [CrossRef] [PubMed]
- Warschkow, R.; Güller, U.; Cerny, T.; Schmied, B.M.; Plasswilm, L.; Putora, P.M. Secondary malignancies after rectal cancer resection with and without radiation therapy: A propensity-adjusted, population-based SEER analysis. Radiother. Oncol. 2017, 123, 139–146. [Google Scholar] [CrossRef]
- Jahreiß, M.-C.; Heemsbergen, W.D.; van Santvoort, B.; Hoogeman, M.; Dirkx, M.; Pos, F.J.; Janssen, T.; Dekker, A.; Vanneste, B.; Minken, A.; et al. Impact of Advanced Radiotherapy on Second Primary Cancer Risk in Prostate Cancer Survivors: A Nationwide Cohort Study. Front. Oncol. 2021, 11, 771956. [Google Scholar] [CrossRef]
- Nugent, T.S.; Low, E.Z.; Fahy, M.R.; Donlon, N.E.; McCormick, P.H.; Mehigan, B.J.; Cunningham, M.; Gillham, C.; Kavanagh, D.O.; Kelly, M.E.; et al. Prostate radiotherapy and the risk of secondary rectal cancer-a meta-analysis. Int. J. Colorectal. Dis. 2022, 37, 437–447. [Google Scholar] [CrossRef]
- Bruheim, K.; Svartberg, J.; Carlsen, E.; Dueland, S.; Haug, E.; Skovlund, E.; Tveit, K.M.; Guren, M.G. Radiotherapy for rectal cancer is associated with reduced serum testosterone and increased FSH and LH. Int. J. Radiat Oncol. Biol. Phys. 2008, 70, 722–727. [Google Scholar] [CrossRef]
- Dueland, S.; Guren, M.G.; Olsen, D.R.; Poulsen, J.P.; Tveit, K.M. Radiation therapy induced changes in male sex hormone levels in rectal cancer patients. Radiother. Oncol. 2003, 68, 249–253. [Google Scholar] [CrossRef]
- Hermann, R.M.; Henkel, K.; Christiansen, H.; Vorwerk, H.; Hille, A.; Hess, C.F.; Schmidberger, H. Testicular dose and hormonal changes after radiotherapy of rectal cancer. Radiother. Oncol. 2005, 75, 83–88. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| No RT, Surgery Only | RT + Surgery | Total | p-Value | |||
|---|---|---|---|---|---|---|
| Total | 23,192 | 46% | 26,769 | 54% | 49,961 | |
| Age | ||||||
| <60 | 8017 | 38% | 13,299 | 62% | 21,316 | <0.001 |
| >60 | 15,175 | 53% | 13,470 | 47% | 28,645 | |
| Gender | ||||||
| Male | 12,809 | 44% | 16,615 | 56% | 29,424 | <0.001 |
| Female | 10,383 | 51% | 10,154 | 49% | 20,537 | |
| Race | ||||||
| White | 19,380 | 47% | 22,065 | 53% | 41,445 | <0.001 |
| Black | 1640 | 43% | 2148 | 57% | 3788 | |
| Other | 2172 | 46% | 2556 | 54% | 4728 | |
| Diagnosis year of the primary cancer | ||||||
| 2000–2004 | 10,120 | 51% | 9734 | 49% | 19,854 | <0.001 |
| 2005–2008 | 6813 | 45% | 8496 | 55% | 15,309 | |
| 2009–2012 | 6259 | 42% | 8539 | 58% | 14,798 | |
| Tumor grade | 0 | |||||
| 1 | 2702 | 61% | 1719 | 39% | 4421 | <0.001 |
| 2 | 14,984 | 45% | 18,614 | 55% | 33,598 | |
| 3 | 2188 | 37% | 3796 | 63% | 5984 | |
| 4 | 155 | 39% | 239 | 61% | 394 | |
| Unknown | 3163 | 57% | 2401 | 43% | 5564 | |
| Stage | ||||||
| Localized | 17,696 | 65% | 9409 | 35% | 27,105 | <0.001 |
| Regional | 5472 | 24% | 17,358 | 76% | 22,830 | |
| Unknown | 24 | 92% | 2 | 8% | 26 | |
| Chemo | ||||||
| Yes | 2189 | 47% | 2481 | 53% | 4670 | <0.001 |
| No/unknown | 21,003 | 92% | 1908 | 8% | 22,911 | |
| No RT, Surgery Only | RT + Surgery | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Observed | Expected | O/E | Lower CI | Upper CI | Observed | Expected | O/E | Lower CI | Upper CI | |
| All Sites | 2978 | 2606.05 | 1.14 # | 1.1 | 1.18 | 2604 | 2608.88 | 1 | 0.96 | 1.04 |
| All Solid Tumors | 2713 | 2292.03 | 1.18 # | 1.14 | 1.23 | 2334 | 2311.65 | 1.01 | 0.97 | 1.05 |
| Oral Cavity and Pharynx | 54 | 61.43 | 0.88 | 0.66 | 1.15 | 64 | 67.66 | 0.95 | 0.73 | 1.21 |
| Esophagus | 33 | 30.43 | 1.08 | 0.75 | 1.52 | 39 | 31.85 | 1.22 | 0.87 | 1.67 |
| Stomach | 58 | 48.02 | 1.21 | 0.92 | 1.56 | 37 | 45.95 | 0.81 | 0.57 | 1.11 |
| Colon, Rectum, and Anus | 705 | 276.6 | 2.55 # | 2.36 | 2.74 | 461 | 258.56 | 1.78 # | 1.62 | 1.95 |
| Liver | 51 | 42.33 | 1.2 | 0.9 | 1.58 | 37 | 47.67 | 0.78 | 0.55 | 1.07 |
| Pancreas | 75 | 83.02 | 0.9 | 0.71 | 1.13 | 52 | 77.29 | 0.67 # | 0.5 | 0.88 |
| Lung and Bronchus | 428 | 399.05 | 1.07 | 0.97 | 1.18 | 468 | 385.94 | 1.21 # | 1.11 | 1.33 |
| Soft Tissue including Heart | 19 | 14.89 | 1.28 | 0.77 | 1.99 | 25 | 14.92 | 1.68 # | 1.08 | 2.47 |
| Melanoma of the Skin | 90 | 118.99 | 0.76 # | 0.61 | 0.93 | 99 | 123.93 | 0.80 # | 0.65 | 0.97 |
| Breast | 243 | 254.93 | 0.95 | 0.84 | 1.08 | 193 | 232.25 | 0.83 # | 0.72 | 0.96 |
| Female Genital System | 90 | 97.39 | 0.92 | 0.74 | 1.14 | 124 | 88.57 | 1.40 # | 1.16 | 1.67 |
| Cervix Uteri | 8 | 7.94 | 1.01 | 0.43 | 1.98 | 6 | 8.08 | 0.74 | 0.27 | 1.62 |
| Ovary | 21 | 26.63 | 0.79 | 0.49 | 1.21 | 10 | 22.63 | 0.44 # | 0.21 | 0.81 |
| Male Genital System | 443 | 463.19 | 0.96 | 0.87 | 1.05 | 213 | 530.14 | 0.40 # | 0.35 | 0.46 |
| Prostate | 438 | 457.62 | 0.96 | 0.87 | 1.05 | 201 | 523.25 | 0.38 # | 0.33 | 0.44 |
| Urinary Bladder | 155 | 162.82 | 0.95 | 0.81 | 1.11 | 177 | 156.09 | 1.13 | 0.97 | 1.31 |
| Kidney | 96 | 78.05 | 1.23 | 1 | 1.5 | 116 | 85 | 1.36 # | 1.13 | 1.64 |
| Endocrine System | 35 | 32.53 | 1.08 | 0.75 | 1.5 | 73 | 37.75 | 1.93 # | 1.52 | 2.43 |
| Thyroid | 32 | 30.1 | 1.06 | 0.73 | 1.5 | 64 | 35.1 | 1.82 # | 1.4 | 2.33 |
| All Lymphatic and Hematopoietic Diseases | 200 | 238.45 | 0.84 # | 0.73 | 0.96 | 217 | 231.75 | 0.94 | 0.82 | 1.07 |
| Mesothelioma | 9 | 8.11 | 1.11 | 0.51 | 2.11 | 6 | 7.64 | 0.79 | 0.29 | 1.71 |
| Kaposi Sarcoma | 4 | 1.54 | 2.59 | 0.71 | 6.63 | 0 | 1.64 | 0 | 0 | 2.25 |
| Miscellaneous | 52 | 62.03 | 0.84 | 0.63 | 1.1 | 40 | 53.24 | 0.75 | 0.54 | 1.02 |
| No RT, Surgery Only | RT + Surgery | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Site | Latency | Observed | Expected | O/E | Lower CI | Upper CI | Observed | Expected | O/E | Lower CI | Upper CI |
| All Sites | 2–5 m | 219 | 118.15 | 1.85 # | 1.62 | 2.12 | 260 | 115.26 | 2.26 # | 1.99 | 2.55 |
| All Sites | 6–11 m | 177 | 170.48 | 1.04 | 0.89 | 1.2 | 140 | 169.08 | 0.83 # | 0.7 | 0.98 |
| All Sites | 12–23 m | 425 | 322.51 | 1.32 # | 1.2 | 1.45 | 325 | 325.67 | 1 | 0.89 | 1.11 |
| All Sites | 24–35 m | 333 | 298.38 | 1.12 | 1 | 1.24 | 274 | 305.66 | 0.9 | 0.79 | 1.01 |
| All Sites | 36–47 m | 360 | 275.95 | 1.30 # | 1.17 | 1.45 | 236 | 285.57 | 0.83 # | 0.72 | 0.94 |
| All Sites | 48–59 m | 296 | 249.12 | 1.19 # | 1.06 | 1.33 | 215 | 257.2 | 0.84 # | 0.73 | 0.96 |
| All Sites | 60–71 m | 255 | 217.81 | 1.17 # | 1.03 | 1.32 | 225 | 222.97 | 1.01 | 0.88 | 1.15 |
| All Sites | 72–83 m | 199 | 189.88 | 1.05 | 0.91 | 1.2 | 195 | 192.41 | 1.01 | 0.88 | 1.17 |
| All Sites | 84–95 m | 153 | 164.16 | 0.93 | 0.79 | 1.09 | 165 | 164.03 | 1.01 | 0.86 | 1.17 |
| All Sites | 96–107 m | 137 | 140.97 | 0.97 | 0.82 | 1.15 | 145 | 138.6 | 1.05 | 0.88 | 1.23 |
| All Sites | 108–119 m | 117 | 119.09 | 0.98 | 0.81 | 1.18 | 105 | 115.07 | 0.91 | 0.75 | 1.1 |
| All Sites | 120+ m | 307 | 339.55 | 0.9 | 0.81 | 1.01 | 319 | 317.38 | 1.01 | 0.9 | 1.12 |
| All Sites | Total | 2978 | 2606.05 | 1.14 # | 1.1 | 1.18 | 2604 | 2608.88 | 1 | 0.96 | 1.04 |
| Colon, Rectum, and Anus | 2–5 m | 57 | 13.55 | 4.21 # | 3.19 | 5.45 | 71 | 12.04 | 5.90 # | 4.61 | 7.44 |
| Colon, Rectum, and Anus | 6–11 m | 28 | 19.4 | 1.44 | 0.96 | 2.09 | 25 | 17.57 | 1.42 | 0.92 | 2.1 |
| Colon, Rectum, and Anus | 12–23 m | 151 | 36.25 | 4.17 # | 3.53 | 4.89 | 88 | 33.55 | 2.62 # | 2.1 | 3.23 |
| Colon, Rectum, and Anus | 24–35 m | 103 | 32.87 | 3.13 # | 2.56 | 3.8 | 54 | 31.02 | 1.74 # | 1.31 | 2.27 |
| Colon, Rectum, and Anus | 36–47 m | 91 | 29.74 | 3.06 # | 2.46 | 3.76 | 53 | 28.52 | 1.86 # | 1.39 | 2.43 |
| Colon, Rectum, and Anus | 48–59 m | 78 | 26.28 | 2.97 # | 2.35 | 3.7 | 32 | 25.34 | 1.26 | 0.86 | 1.78 |
| Colon, Rectum, and Anus | 60–71 m | 67 | 22.67 | 2.96 # | 2.29 | 3.75 | 43 | 21.79 | 1.97 # | 1.43 | 2.66 |
| Colon, Rectum, and Anus | 72–83 m | 44 | 19.63 | 2.24 # | 1.63 | 3.01 | 27 | 18.76 | 1.44 | 0.95 | 2.09 |
| Colon, Rectum, and Anus | 84–95 m | 30 | 16.83 | 1.78 # | 1.2 | 2.55 | 18 | 15.9 | 1.13 | 0.67 | 1.79 |
| Colon, Rectum, and Anus | 96–107 m | 16 | 14.27 | 1.12 | 0.64 | 1.82 | 11 | 13.32 | 0.83 | 0.41 | 1.48 |
| Colon, Rectum, and Anus | 108–119 m | 10 | 11.87 | 0.84 | 0.4 | 1.55 | 11 | 10.94 | 1.01 | 0.5 | 1.8 |
| Colon, Rectum, and Anus | 120+ m | 30 | 33.25 | 0.9 | 0.61 | 1.29 | 28 | 29.81 | 0.94 | 0.62 | 1.36 |
| Colon, Rectum, and Anus | Total | 705 | 276.6 | 2.55 # | 2.36 | 2.74 | 461 | 258.56 | 1.78 # | 1.62 | 1.95 |
| Prostate | 2–5 m | 34 | 22.64 | 1.50 # | 1.04 | 2.1 | 61 | 25.23 | 2.42 # | 1.85 | 3.11 |
| Prostate | 6–11 m | 31 | 32.49 | 0.95 | 0.65 | 1.35 | 14 | 36.79 | 0.38 # | 0.21 | 0.64 |
| Prostate | 12–23 m | 53 | 60.97 | 0.87 | 0.65 | 1.14 | 7 | 70.16 | 0.10 # | 0.04 | 0.21 |
| Prostate | 24–35 m | 43 | 55.57 | 0.77 | 0.56 | 1.04 | 7 | 64.8 | 0.11 # | 0.04 | 0.22 |
| Prostate | 36–47 m | 48 | 50.32 | 0.95 | 0.7 | 1.26 | 17 | 59.04 | 0.29 # | 0.17 | 0.46 |
| Prostate | 48–59 m | 35 | 44.44 | 0.79 | 0.55 | 1.1 | 11 | 51.94 | 0.21 # | 0.11 | 0.38 |
| Prostate | 60–71 m | 35 | 38.06 | 0.92 | 0.64 | 1.28 | 13 | 44.25 | 0.29 # | 0.16 | 0.5 |
| Prostate | 72–83 m | 32 | 32.6 | 0.98 | 0.67 | 1.39 | 17 | 37.66 | 0.45 # | 0.26 | 0.72 |
| Prostate | 84–95 m | 19 | 27.61 | 0.69 | 0.41 | 1.07 | 12 | 31.5 | 0.38 # | 0.2 | 0.67 |
| Prostate | 96–107 m | 26 | 23.07 | 1.13 | 0.74 | 1.65 | 16 | 25.97 | 0.62 | 0.35 | 1 |
| Prostate | 108–119 m | 25 | 18.84 | 1.33 | 0.86 | 1.96 | 7 | 20.84 | 0.34 # | 0.14 | 0.69 |
| Prostate | 120+ m | 57 | 51 | 1.12 | 0.85 | 1.45 | 19 | 55.08 | 0.34 # | 0.21 | 0.54 |
| Prostate | Total | 438 | 457.62 | 0.96 | 0.87 | 1.05 | 201 | 523.25 | 0.38 # | 0.33 | 0.44 |
| Thyroid | 2–5 m | 0 | 1.23 | 0 | 0 | 3 | 8 | 1.49 | 5.35 # | 2.31 | 10.55 |
| Thyroid | 6–11 m | 2 | 1.81 | 1.1 | 0.13 | 3.99 | 9 | 2.22 | 4.06 # | 1.86 | 7.7 |
| Thyroid | 12–23 m | 5 | 3.52 | 1.42 | 0.46 | 3.31 | 14 | 4.34 | 3.23 # | 1.76 | 5.42 |
| Thyroid | 24–35 m | 0 | 3.39 | 0 | 0 | 1.09 | 11 | 4.16 | 2.64 # | 1.32 | 4.73 |
| Thyroid | 36–47 m | 8 | 3.25 | 2.46 # | 1.06 | 4.85 | 4 | 3.98 | 1.01 | 0.27 | 2.57 |
| Thyroid | 48–59 m | 5 | 3 | 1.67 | 0.54 | 3.89 | 6 | 3.61 | 1.66 | 0.61 | 3.62 |
| Thyroid | 60–71 m | 3 | 2.63 | 1.14 | 0.24 | 3.34 | 0 | 3.11 | 0 | 0 | 1.19 |
| Thyroid | 72–83 m | 1 | 2.27 | 0.44 | 0.01 | 2.45 | 4 | 2.63 | 1.52 | 0.42 | 3.9 |
| Thyroid | 84–95 m | 2 | 1.96 | 1.02 | 0.12 | 3.69 | 2 | 2.2 | 0.91 | 0.11 | 3.28 |
| Thyroid | 96–107 m | 2 | 1.69 | 1.19 | 0.14 | 4.28 | 1 | 1.84 | 0.54 | 0.01 | 3.02 |
| Thyroid | 108–119 m | 1 | 1.42 | 0.7 | 0.02 | 3.91 | 1 | 1.53 | 0.65 | 0.02 | 3.65 |
| Thyroid | 120+ m | 3 | 3.93 | 0.76 | 0.16 | 2.23 | 4 | 3.99 | 1 | 0.27 | 2.57 |
| Thyroid | Total | 32 | 30.1 | 1.06 | 0.73 | 1.5 | 64 | 35.1 | 1.82 # | 1.4 | 2.33 |
| No RT, Surgery Only | RT + Surgery | Total | p-Value | |||
|---|---|---|---|---|---|---|
| Total | 521 | 275 | 796 | |||
| Age | 0.675 | |||||
| <60 | 61 | 11.70% | 35 | 12.70% | 96 | |
| >60 | 460 | 88.30% | 240 | 87.30% | 700 | |
| Race | 0.904 | |||||
| White | 427 | 82.00% | 223 | 81.10% | 650 | |
| Black | 64 | 12.30% | 34 | 12.40% | 98 | |
| Other | 30 | 5.80% | 18 | 6.50% | 48 | |
| Tumor grade | 0.331 | |||||
| 1 | 31 | 6.00% | 13 | 4.70% | 44 | |
| 2 | 221 | 42.40% | 121 | 44.00% | 342 | |
| 3 | 221 | 42.40% | 104 | 37.80% | 325 | |
| 4 | 1 | 0.20% | 1 | 0.40% | 2 | |
| Unknown | 47 | 9.00% | 36 | 13.10% | 83 | |
| Stage | 0.044 | |||||
| Localized | 418 | 80.20% | 200 | 72.70% | 618 | |
| Regional | 38 | 7.30% | 31 | 11.30% | 69 | |
| Distant/unknown | 65 | 12.50% | 44 | 16.00% | 109 | |
| Chemo | 0.001 | |||||
| Yes | 3 | 0.60% | 10 | 3.60% | 13 | |
| No/unknown | 518 | 99.40% | 265 | 964% | 783 | |
| Median latency months | 51 (21.75, 95) | 47 (4.5, 86) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, X.; Tan, Y.; Ma, R.; Lou, P.; Yuan, Y. Radiation Therapy Changed the Second Malignancy Pattern in Rectal Cancer Survivors. Medicina 2023, 59, 1463. https://doi.org/10.3390/medicina59081463
Ye X, Tan Y, Ma R, Lou P, Yuan Y. Radiation Therapy Changed the Second Malignancy Pattern in Rectal Cancer Survivors. Medicina. 2023; 59(8):1463. https://doi.org/10.3390/medicina59081463
Chicago/Turabian StyleYe, Xiaoxian, Yinuo Tan, Ruishuang Ma, Pengrong Lou, and Ying Yuan. 2023. "Radiation Therapy Changed the Second Malignancy Pattern in Rectal Cancer Survivors" Medicina 59, no. 8: 1463. https://doi.org/10.3390/medicina59081463
APA StyleYe, X., Tan, Y., Ma, R., Lou, P., & Yuan, Y. (2023). Radiation Therapy Changed the Second Malignancy Pattern in Rectal Cancer Survivors. Medicina, 59(8), 1463. https://doi.org/10.3390/medicina59081463