
Evaluation of Possible Side Effects in the Treatment of Urinary Incontinence with Magnetic Stimulation

Abstract
1. Introduction
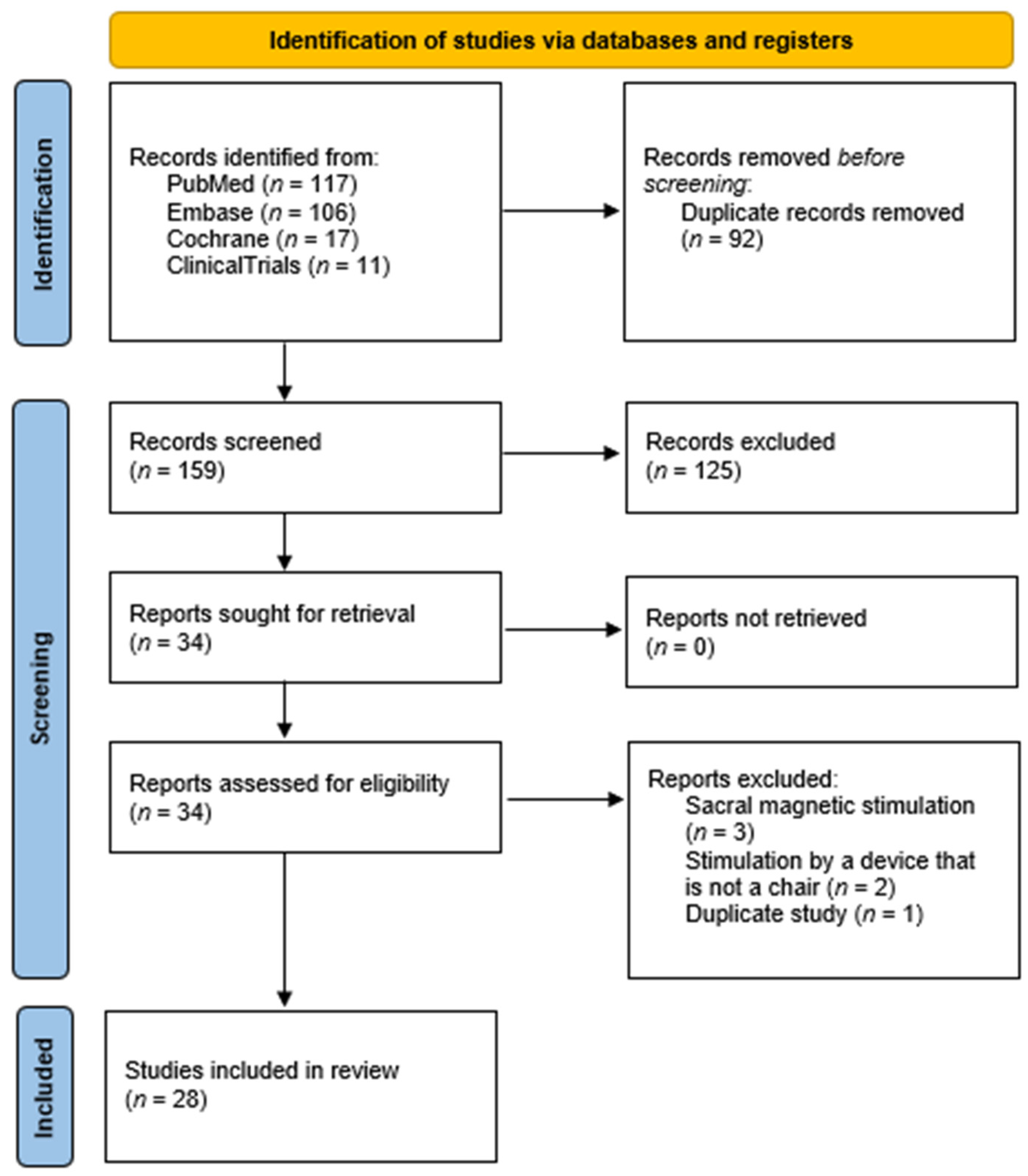
2. Methods
3. Magnetic Stimulation
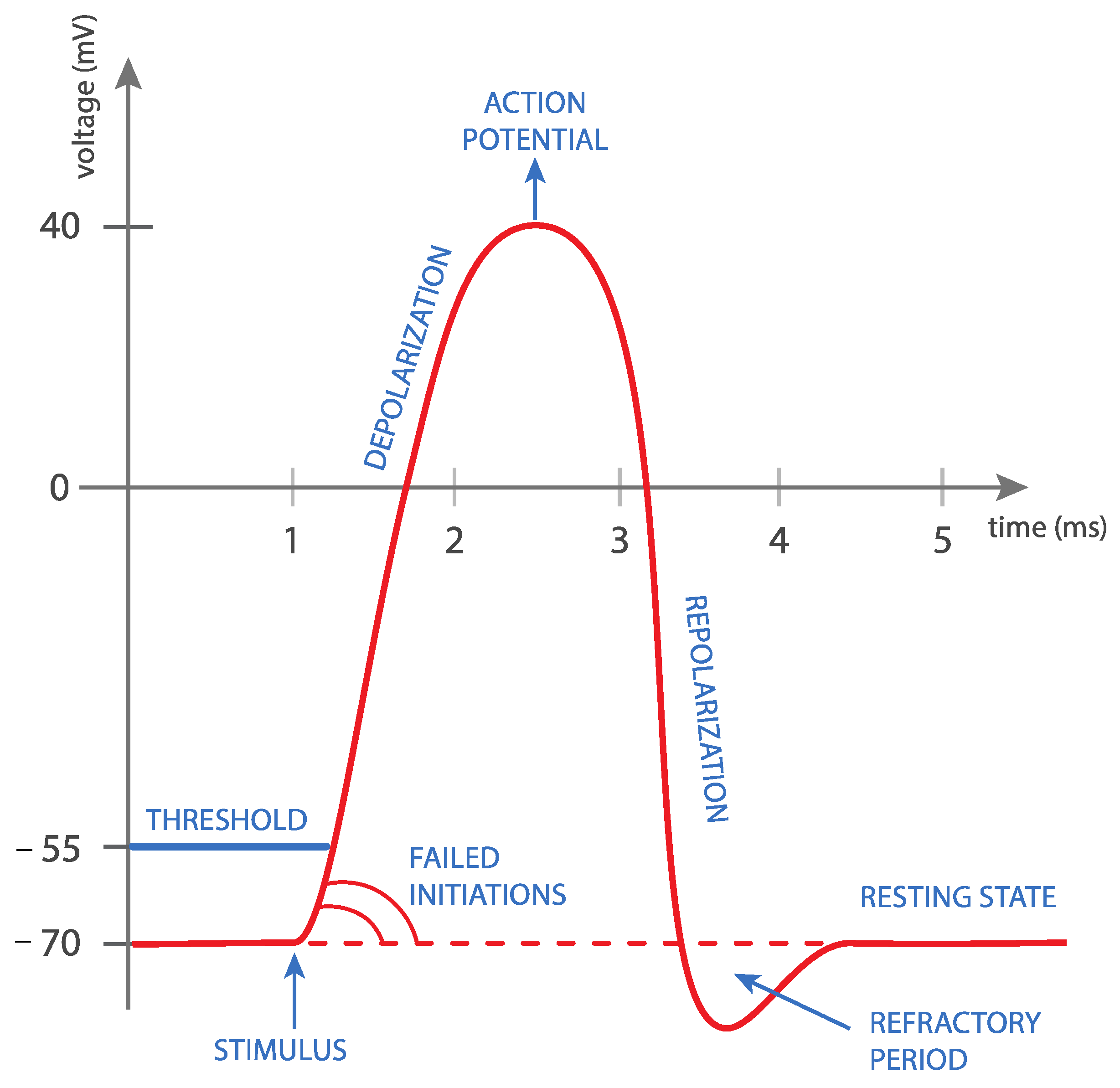
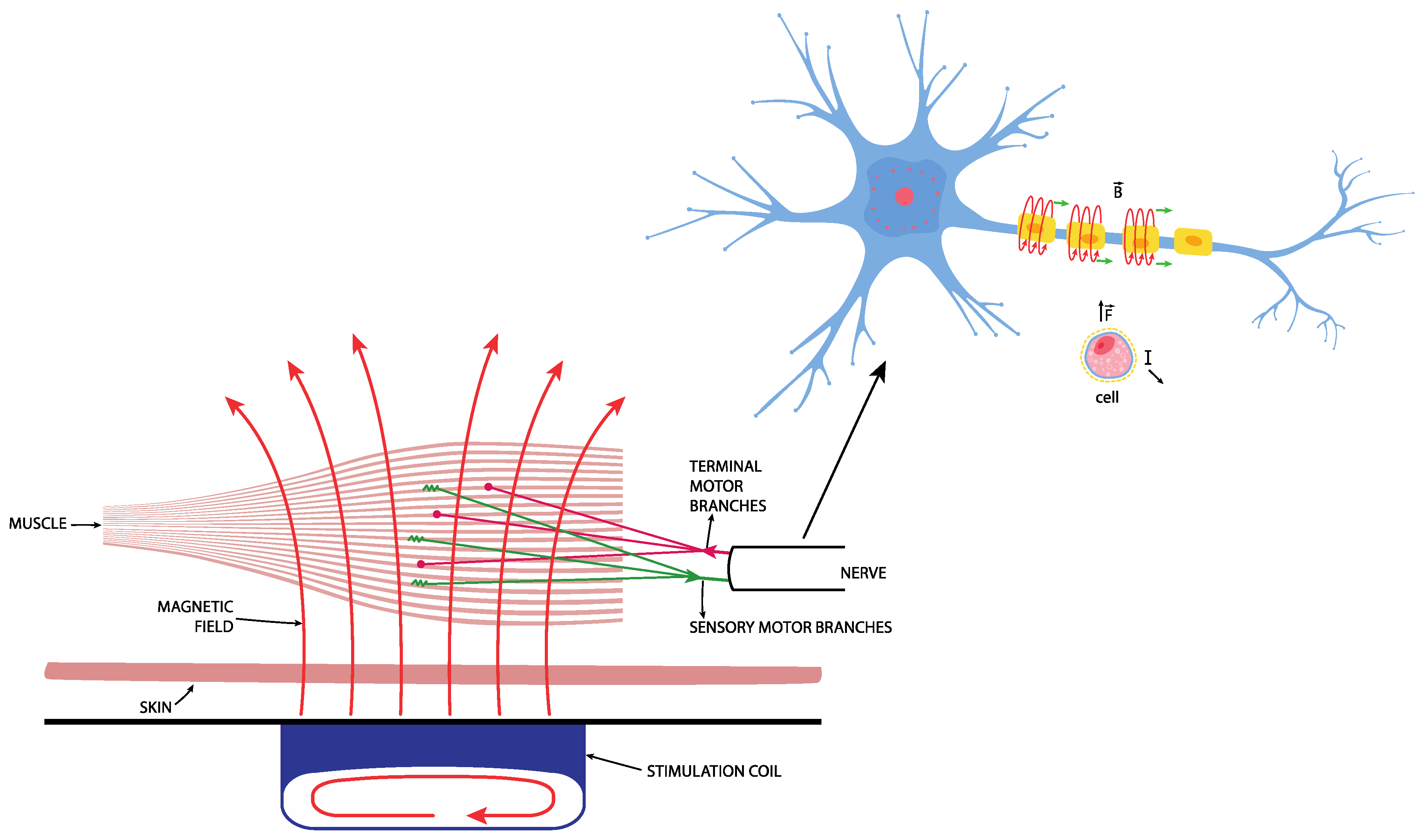
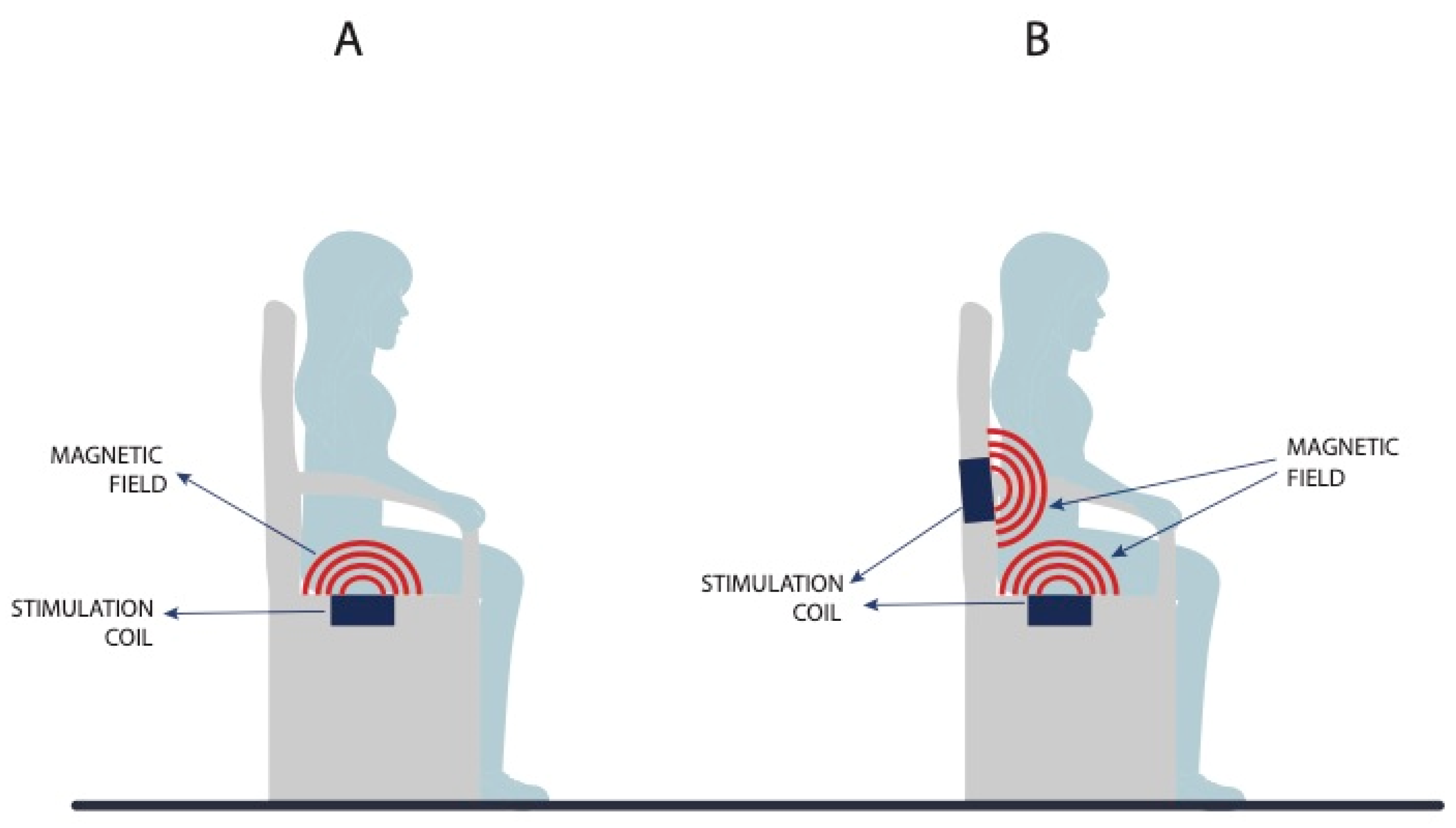
3.1. Basic Principle of Magnetic Stimulation
- 1.
- Activation of the hypogastric nerve (Lat. nervus hypogastricus);
- 2.
- Direct inhibition of the pelvic plexus (Lat. plexus hypogastricus inferior);
- 3.


3.2. Effectiveness of Magnetic Stimulation in the Treatment of UI
3.3. Magnetic Stimulation vs. Electrostimulation
3.4. Possible Side Effects of MS
- 1.
- Muscle overload: During therapies, the muscles that are located in the magnetic field of the MS device are constantly being activated by the device. If the magnetic field or the response of the patient’s muscles is intense, there is a possibility of muscle overload, leading to a longer recovery rate and temporarily weakened muscles.
- 2.
- Tissue damage: Although MS is mostly used for tissue repair and faster healing, intense treatment with MS that does not leave adequate time for recovery between pulses/treatments can damage already weakened tissues [42,43,44]. There is a theoretical possibility of electrical overload of the nerve fiber with the induced current. This could only happen if the magnetic field was high enough and directly focused on an already damaged nerve, resulting in an unacceptable level of activity for physiological structures [45]. The actual probability of such a scenario is only theoretical and has never been mentioned or occurred during treatments. It is presumed that such high-voltage exposure would result in visible tissue damage such as burns, and invisible tissue damage such as permanent numbness and/or pain in the skin in the treated area. On the other hand, it is presumed that, if such an electrical overload of the nerve fiber occurred during MS therapy, this resulted in improvements in the final outcome for the patient—presumably by forcing the body to repair the nerve fiber by promoting nerve regeneration with increased blood flow, increasing serum ceruloplasmin expression, improving angiogenesis, and facilitating nerve fiber growth indirectly from vascular tropism. There is also some evidence that this would have positive effects on remyelination [46].
- 3.
- Reduction in or loss of sensation on the fibers: If the patient’s nerves and tissue are exposed to an unsuitable duration and/or intensity of magnetic field during MS treatment, the result for the patient could be a tingling sensation, warm skin sensation, poor temperature perception, and so on. The recovery time in such scenarios is brief because it only affects the superficial nerves in the skin.
- 4.
- Ineffectiveness of MS therapy: The magnetic field density decreases by the cube root of length, which means that if we increase the distance from the magnetic-field-generating device to a specific point on the patient by a factor of two, we decrease the magnetic field density at the same spot by a factor of eight. We can conclude that the tissue closer to the device generating the magnetic field will always be exposed to a denser magnetic field. Knowledge of the effects and responsiveness of the patient’s body to the magnetic field are crucial when treating deeper areas with MS.
- 5.
- Heating or overheating of affected tissues: By exposing the patient’s body to the magnetic field, some energy is transferred to the patient’s body in the form of heat. Very high and intense MS therapies could lead to heating and/or overheating in some parts of the tissue located in the magnetic field. Patients with cardiovascular problems are more affected by this issue because the blood flow is restricted, and thus the tissue-cooling is compromised. More attention should be paid to the patient when there is a risk of seminal fluid being affected by the accumulating heat and when the accumulating heat could lead to an increased risk of vaginal or bladder infection because of the faster development of bacteria in the body. These problems have never been mentioned in the literature and are, therefore, only theoretical. We can conclude that they have a very low probability of occurrence. This kind of side effect is normally avoided by the manufacturers of MS devices with longer pause times in therapy programs that allow for heat to dissipate through the body faster that it can accumulate.
- 6.
- The effect of frequencies and magnetic fields on intestinal function and metabolism: During MS therapies, part of the intestine is located in the magnetic field. At present, no accurate measurement can be made determine the overall effect of MS on patients’ intestinal function, organs, and metabolism. The majority of the empirical evidence shows that MS therapy affects patients’ intestinal function in a beneficial way by increasing the metabolic rate, probably mostly through contractions in the surrounding muscles and tissue. Most patients feel a normal need to defecate or urinate after treatments with MS. However, this could lead to an altered metabolic rate, resulting in diarrhea or constipation.
4. Results of Our Literature Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction: Terminology for Female Pelvic Floor Dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Blaivas, J.G.; Stanton, S.L.; Andersen, J.T. Standardisation of Terminology of Lower Urinary Tract Function. Neurourol. Urodyn. 1988, 7, 403–427. [Google Scholar] [CrossRef]
- Abrams, P.; Andersson, K.E.; Birder, L.; Brubaker, L.; Cardozo, L.; Chapple, C.; Cottenden, A.; Davila, W.; De Ridder, D.; Dmochowski, R.; et al. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: Evaluation and Treatment of Urinary Incontinence, Pelvic Organ Prolapse, and Fecal Incontinence. Neurourol. Urodyn. 2010, 29, 213–240. [Google Scholar] [CrossRef]
- Lukanović, D.; Blaganje, M.; Barbič, M. Algoritem zdravljenja urinske inkontinence. Slov. Med. J. 2021, 90, 275–287. [Google Scholar] [CrossRef]
- Antić, A.; Pavčnik, M.; Lukanović, A.; Matjašič, M.; Lukanović, D. Magnetic Stimulation in the Treatment of Female Urgency Urinary Incontinence: A Systematic Review. Int. Urogynecol. J. 2023. Available online: https://link.springer.com/article/10.1007/s00192-023-05492-7#citeas (accessed on 12 April 2023). [CrossRef]
- Milsom, I.; Gyhagen, M. The Prevalence of Urinary Incontinence. Climacteric 2019, 22, 217–222. [Google Scholar] [CrossRef]
- Nambiar, A.K.; Arlandis, S.; Bø, K.; Cobussen-Boekhorst, H.; Costantini, E.; de Heide, M.; Farag, F.; Groen, J.; Karavitakis, M.; Lapitan, M.C.; et al. European Association of Urology Guidelines on the Diagnosis and Management of Female Non-Neurogenic Lower Urinary Tract Symptoms. Part 1: Diagnostics, Overactive Bladder, Stress Urinary Incontinence, and Mixed Urinary Incontinence. Eur. Urol. 2022, 82, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Serdinšek, T.; But, I. Začetna obravnava bolnice z uroginekološkimi težavami. Slov. Med. J. 2019, 87, 575–586. [Google Scholar] [CrossRef]
- Blaganje, M.; Šćepanović, D.; Žgur, L.; Verdenik, I.; Pajk, F.; Lukanović, A. Non-Ablative Er:YAG Laser Therapy Effect on Stress Urinary Incontinence Related to Quality of Life and Sexual Function: A Randomized Controlled Trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Tien, Y.-W.; Hsiao, S.-M.; Lee, C.-N.; Lin, H.-H. Effects of Laser Procedure for Female Urodynamic Stress Incontinence on Pad Weight, Urodynamics, and Sexual Function. Int. Urogynecol. J. 2017, 28, 469–476. [Google Scholar] [CrossRef]
- Reisenauer, C.; Hartlieb, S.; Schoenfisch, B.; Brucker, S.Y.; Neis, F. Vaginal Therapy of Mild and Moderate Stress Urinary Incontinence Using Er:YAG Laser: A Real Treatment Option. Arch. Gynecol. Obstet. 2019, 300, 1645–1650. [Google Scholar] [CrossRef]
- Kuszka, A.; Gamper, M.; Walser, C.; Kociszewski, J.; Viereck, V. Erbium:YAG Laser Treatment of Female Stress Urinary Incontinence: Midterm Data. Int. Urogynecol. J. 2020, 31, 1859–1866. [Google Scholar] [CrossRef]
- Lauterbach, R.; Aharoni, S.; Justman, N.; Farago, N.; Gruenwald, I.; Lowenstein, L. The Efficacy and Safety of a Single Maintenance Laser Treatment for Stress Urinary Incontinence: A Double-Blinded Randomized Controlled Trial. Int. Urogynecol.J. 2022, 33, 3499–3504. [Google Scholar] [CrossRef]
- Montera, R.; Ficarola, F.; Angioli, R.; Terranova, C.; Nardone, C.D.C.; Guzzo, F.; Plotti, F.; Luvero, D. Efficacy of Termoablative Fractional CO2 Laser (Monnalisa Touch) in Stress Urinary Incontinence. Neurourol. Urodyn. 2023, 42, 393–400. [Google Scholar] [CrossRef]
- on behalf of the IUGA Research and Development Committee; Shobeiri, S.A.; Kerkhof, M.H.; Minassian, V.A.; Bazi, T. IUGA Committee Opinion: Laser-Based Vaginal Devices for Treatment of Stress Urinary Incontinence, Genitourinary Syndrome of Menopause, and Vaginal Laxity. Int. Urogynecol. J. 2019, 30, 371–376. [Google Scholar] [CrossRef]
- Braga, A.; Castronovo, F.; Caccia, G.; Papadia, A.; Regusci, L.; Torella, M.; Salvatore, S.; Scancarello, C.; Ghezzi, F.; Serati, M. Efficacy of 3 Tesla Functional Magnetic Stimulation for the Treatment of Female Urinary Incontinence. J. Clin. Med. 2022, 11, 2805. [Google Scholar] [CrossRef]
- Burkhard, F.C.; Bosch, J.L.H.R.; Cruz, F.; Lemack, G.E.; Nambiar, A.K.; Thiruchelvam, A.; Tubaro, A. EAU Guidelines on Urinary Incontinence in Adults 2020. Available online: https://uroweb.org/eau-guidelines/discontinued-topics/urinary-incontinence (accessed on 10 April 2023).
- Harding, C.K.; Lapitan, M.C.; Arlandis, S.; Bø, K.; Cobussen-Boekhorst, H.; Costantini, E.; Groen, J.; Nambiar, A.K.; Omar, M.I.; Peyronnet, B.; et al. EAU Guidelines on Management of Non-Neurogenic Female Lower Urinary Tract Symptoms 2023. Available online: https://uroweb.org/guidelines/non-neurogenic-female-luts (accessed on 10 April 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Yamanishi, T.; Yasuda, K.; Suda, S.; Ishikawa, N.; Sakakibara, R.; Hattori, T. Effect of Functional Continuous Magnetic Stimulation for Urinary Incontinence. J. Urol. 2000, 163, 456–459. [Google Scholar] [CrossRef]
- Suzuki, T.; Yasuda, K.; Yamanishi, T.; Kitahara, S.; Nakai, H.; Suda, S.; Ohkawa, H. Randomized, Double-Blind, Sham-Controlled Evaluation of the Effect of Functional Continuous Magnetic Stimulation in Patients with Urgency Incontinence. Neurourol. Urodyn. 2007, 26, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Yamanishi, T.; Homma, Y.; Nishizawa, O.; Yasuda, K.; Yokoyama, O.; SMN-X Study Group. Multicenter, Randomized, Sham-Controlled Study on the Efficacy of Magnetic Stimulation for Women with Urgency Urinary Incontinence: Magnetic Stimulation for Incontinence. Int. J. Urol. 2014, 21, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Lukanović, D.; Kunič, T.; Batkoska, M.; Matjašič, M.; Barbič, M. Effectiveness of Magnetic Stimulation in the Treatment of Urinary Incontinence: A Systematic Review and Results of Our Study. J. Clin. Med. 2021, 10, 5210. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.P.; Sand, P.K. Electromagnetic Pelvic Floor Stimulation: Applications for the Gynecologist. Obstet. Gynecol. Surv. 2000, 55, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Galloway, N.T.M.; El-Galley, R.E.S.; Sand, P.K.; Appell, R.A.; Russell, H.W.; Carlan, S.J. Extracorporeal Magnetic Innervation Therapy for Stress Urinary Incontinence. Urology 1999, 53, 1108–1111. [Google Scholar] [CrossRef]
- Doğanay, M.; Kilic, S.; Yilmaz, N. Long-Term Effects of Extracorporeal Magnetic Innervations in the Treatment of Women with Urinary Incontinence: Results of 3-Year Follow-Up. Arch. Gynecol. Obstet. 2010, 282, 49–53. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Xiao, K.; Peng, L.; Lai, J.; Li, H.; Luo, D.; Wang, K. An Effective Meta-Analysis of Magnetic Stimulation Therapy for Urinary Incontinence. Sci. Rep. 2019, 9, 9077. [Google Scholar] [CrossRef]
- Lo, T.-S.; Tseng, L.-H.; Lin, Y.-H.; Liang, C.-C.; Lu, C.-Y.; Pue, L.B. Effect of Extracorporeal Magnetic Energy Stimulation on Bothersome Lower Urinary Tract Symptoms and Quality of Life in Female Patients with Stress Urinary Incontinence and Overactive Bladder: EMS for Women with SUI and OAB. J. Obstet. Gynaecol. Res. 2013, 39, 1526–1532. [Google Scholar] [CrossRef] [PubMed]
- Lopopolo, G.; Salsi, B.; Banfi, A.; Isaza, P.G.; Fusco, I. Is It Possible to Improve Urinary Incontinence and Quality of Life in Female Patients? A Clinical Evaluation of the Efficacy of Top Flat Magnetic Stimulation Technology. Bioengineering 2022, 9, 140. [Google Scholar] [CrossRef]
- Gözlersüzer, Ö.; Yalvaç, B.; Çakıroğlu, B. Investigation of the Effectiveness of Magnetic Field Therapy in Women with Urinary Incontinence: Literature Review. Urol. J. 2023, 90, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Zeng, X.; Shen, H.; Luo, D. Magnetic Stimulation for Female Patients with Stress Urinary Incontinence, a Meta-Analysis of Studies with Short-Term Follow-Up. Medicine 2019, 98, e15572. [Google Scholar] [CrossRef]
- Yokoyama, T.; Fujita, O.; Nishiguchi, J.; Nozaki, K.; Nose, H.; Inoue, M.; Ozawa, H.; Kumon, H. Extracorporeal Magnetic Innervation Treatment for Urinary Incontinence. Int. J. Urol. 2004, 11, 602–606. [Google Scholar] [CrossRef]
- Ünsal, A.; Saglam, R.; Cimentepe, E. Extracorporeal Magnetic Stimulation for the Treatment of Stress and Urge Incontinence in WomenResults of 1-year Follow-up. Scand. J. Urol. Nephrol. 2003, 37, 424–428. [Google Scholar] [CrossRef]
- Bradshaw, H.D.; Barker, A.T.; Radley, S.C.; Chapple, C.R. The Acute Effect of Magnetic Stimulation of the Pelvic Floor on Involuntary Detrusor Activity during Natural Filling and Overactive Bladder Symptoms: Magnetic stimulation of the pelvic floor and involuntary detrusor activity. BJU Int. 2003, 91, 810–813. [Google Scholar] [CrossRef]
- Voorham-Van Der Zalm, P.J.; Pelger, R.C.M.; Stiggelbout, A.M.; Elzevier, H.W.; Lycklama, A.; Nijeholt, G.A.B. Effects of Magnetic Stimulation in the Treatment of Pelvic Floor Dysfunction. BJU Int. 2006, 97, 1035–1038. [Google Scholar] [CrossRef]
- Mikuš, M.; Kalafatić, D.; Vrbanić, A.; Šprem Goldštajn, M.; Herman, M.; Živković Njavro, M.; Živković, K.; Marić, G.; Ćorić, M. Efficacy Comparison between Kegel Exercises and Extracorporeal Magnetic Innervation in Treatment of Female Stress Urinary Incontinence: A Randomized Clinical Trial. Medicina 2022, 58, 1863. [Google Scholar] [CrossRef]
- Yamanishi, T.; Kaga, K.; Fuse, M.; Shibata, C.; Uchiyama, T. Neuromodulation for the Treatment of Lower Urinary Tract Symptoms: Neuromodulation for LUTS. LUTS Low. Urin. Tract Symptoms 2015, 7, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Yamanishi, T.; Sakakibara, R.; Uchiyama, T.; Suda, S.; Hattori, T.; Ito, H.; Yasuda, K. Comparative Study of the Effects of Magnetic versus Electrical Stimulation on Inhibition of Detrusor Overactivity. Urology 2000, 56, 777–781. [Google Scholar] [CrossRef]
- Elena, S.; Dragana, Z.; Ramina, S.; Evgeniia, A.; Orazov, M. Electromyographic Evaluation of the Pelvic Muscles Activity after High-Intensity Focused Electromagnetic Procedure and Electrical Stimulation in Women with Pelvic Floor Dysfunction. Sex. Med. 2020, 8, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Fujishiro, T.; Enomoto, H.; Ugawa, Y.; Takahashi, S.; Ueno, S.; Kitamura, T. Magnetic Stimulation of the Sacral Roots for the Treatment of Stress Incontinence: An Investigational Study and Placebo Controlled Trial. J. Urol. 2000, 164, 1277–1279. [Google Scholar] [CrossRef]
- Panych, L.P.; Madore, B. The Physics of MRI Safety: Physics of MRI Safety. J. Magn. Reson. Imaging 2018, 47, 28–43. [Google Scholar] [CrossRef]
- Aaron, R.K.; Ciombor, D. McK. Therapeutic Effects of Electromagnetic Fields in the Stimulation of Connective Tissue Repair. J. Cell. Biochem. 1993, 52, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.L.; Harrison, B.S. The Use of Magnetic Field for the Reduction of Inflammation: A Review of the History and Therapeutic Results. Altern. Ther. Health Med. 2013, 19, 47–54. [Google Scholar]
- Ribeiro, T.P.; Flores, M.; Madureira, S.; Zanotto, F.; Monteiro, F.J.; Laranjeira, M.S. Magnetic Bone Tissue Engineering: Reviewing the Effects of Magnetic Stimulation on Bone Regeneration and Angiogenesis. Pharmaceutics 2023, 15, 1045. [Google Scholar] [CrossRef] [PubMed]
- Günter, C.; Delbeke, J.; Ortiz-Catalan, M. Safety of Long-Term Electrical Peripheral Nerve Stimulation: Review of the State of the Art. J. NeuroEng. Rehabil. 2019, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Cheng, Y.; Cai, J.; Zhao, X.; Ouyang, Y.; Yuan, W.-E.; Fan, C. Advances in Electrical and Magnetic Stimulation on Nerve Regeneration. Regen. Med. 2019, 14, 969–979. [Google Scholar] [CrossRef]
- Chandi, D.D.; Groenendijk, P.M.; Venema, P.L. Functional Extracorporeal Magnetic Stimulation as a Treatment for Female Urinary Incontinence: “The Chair”. BJU Int. 2004, 93, 539–542. [Google Scholar] [CrossRef]
- Almeida, F.G.; Bruschini, H.; Srougi, M. Urodynamic and clinical evaluation of 91 female patients with urinary incontinence treated with perineal magnetic stimulation: 1-year followup. J. Urol. 2004, 171, 1571–1575. [Google Scholar] [CrossRef]
- Choe, J.H.; Choo, M.-S.; Lee, K.-S. Symptom Change in Women with Overactive Bladder after Extracorporeal Magnetic Stimulation: A Prospective Trial. Int. Urogynecol. J. 2007, 18, 875–880. [Google Scholar] [CrossRef]
- Hoşcan, M.B.; Dilmen, C.; Perk, H.; Soyupek, S.; Armağan, A.; Tükel, O.; Ekinci, M. Extracorporeal Magnetic Innervation for the Treatment of Stress Urinary Incontinence: Results of Two-Year Follow-Up. Urol. Int. 2008, 81, 167–172. [Google Scholar] [CrossRef]
- Gilling, P.J.; Wilson, L.C.; Westenberg, A.M.; McAllister, W.J.; Kennett, K.M.; Frampton, C.M.; Bell, D.F.; Wrigley, P.M.; Fraundorfer, M.R. A Double-Blind Randomized Controlled Trial of Electromagnetic Stimulation of the Pelvic Floor vs. Sham Therapy in the Treatment of Women with Stress Urinary Incontinence. BJU Int. 2009, 103, 1386–1390. [Google Scholar] [CrossRef]
- Vadalà, M.; Palmieri, B.; Malagoli, A.; Laurino, C. High-Power Magnetotherapy: A New Weapon in Urinary Incontinence?: A New Weapon in Urinary Incontinence? LUTS Low. Urin. Tract Symptoms 2018, 10, 266–270. [Google Scholar] [CrossRef]
- Yamanishi, T.; Suzuki, T.; Sato, R.; Kaga, K.; Kaga, M.; Fuse, M. Effects of Magnetic Stimulation on Urodynamic Stress Incontinence Refractory to Pelvic Floor Muscle Training in a Randomized Sham-Controlled Study. LUTS Low. Urin. Tract Symptoms 2019, 11, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Silantyeva, E.; Zarkovic, D.; Astafeva, E.; Soldatskaia, R.; Orazov, M.; Belkovskaya, M.; Kurtser, M.; Academician of the Russian Academy of Sciences. A Comparative Study on the Effects of High-Intensity Focused Electromagnetic Technology and Electrostimulation for the Treatment of Pelvic Floor Muscles and Urinary Incontinence in Parous Women: Analysis of Posttreatment Data. Female Pelvic Med. Reconstr. Surg. 2021, 27, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shi, C.; Zhou, D.; Yu, W.; Jiao, W.; Shi, G. Efficacy of Optimized Pelvic Floor Training of YUN Combined with Pelvic Floor Magnetic Stimulation on Female Moderate Stress Urinary Incontinence and Sexual Function: A Retrospective Cohort Study. Transl. Androl. Urol. 2022, 11, 554–560. [Google Scholar] [CrossRef]
- González-Isaza, P.; Sánchez-Borrego, R.; Lugo Salcedo, F.; Rodríguez, N.; Vélez Rizo, D.; Fusco, I.; Callarelli, S. Pulsed Magnetic Stimulation for Stress Urinary Incontinence and Its Impact on Sexuality and Health. Medicina 2022, 58, 1721. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, A.P.; Isaza, P.G.; Pantoja, S.N.; Fusco, I. Role of Top Flat Magnetic Stimulation for Urinary Incontinence as a Debilitating Condition of Pelvic Floor Dysfunction: An Observational Evaluation of Latin American Population. World J. Urol. 2022, 41, 173–177. [Google Scholar] [CrossRef]
- Groenendijk, P.M.; Halilovic, M.; Chandi, D.D.; Heesakkers, J.P.F.A.; Voorham-Van Der Zalm, P.J.; Lycklama Ànijeholt, A.A.B. Extracorporeal Magnetic Innervation Therapy: Assessment of Clinical Efficacy in Relation to Urodynamic Parameters. Scand. J. Urol. Nephrol. 2008, 42, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.I.M.F.; Forward, G.; Bastin, L.; Wareham, K.; Emery, S.J.; Lucas, M. Extracorporeal Magnetic Energy Stimulation of Pelvic Floor Muscles for Urodynamic Stress Incontinence of Urine in Women. J. Obstet. Gynaecol. 2009, 29, 35–39. [Google Scholar] [CrossRef]
- Lim, R.; Liong, M.L.; Leong, W.S.; Karim Khan, N.A.; Yuen, K.H. Pulsed Magnetic Stimulation for Stress Urinary Incontinence: 1-Year Followup Results. J. Urol. 2017, 197, 1302–1308. [Google Scholar] [CrossRef]
- Tezer, T.; Yıldız, N.; Sarsan, A.; Alkan, H. Short-term Effect of Magnetic Stimulation Added to Bladder Training in Women with Idiopathic Overactive Bladder: A Prospective Randomized Controlled Trial. Neurourol. Urodyn. 2022, 41, 1380–1389. [Google Scholar] [CrossRef]
- Lim, R.; Lee, S.W.H.; Tan, P.Y.; Liong, M.L.; Yuen, K.H. Efficacy of Electromagnetic Therapy for Urinary Incontinence: A Systematic Review: Efficacy of Electromagnetic Therapy in Urinary Incontinence. Neurourol. Urodyn. 2015, 34, 713–722. [Google Scholar] [CrossRef]
- Lim, R.; Liong, M.L.; Leong, W.S.; Khan, N.A.K.; Yuen, K.H. Patients’ Perception and Satisfaction with Pulsed Magnetic Stimulation for Treatment of Female Stress Urinary Incontinence. Int. Urogynecol. J. 2018, 29, 997–1004. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n) | Type of UI | Treatment Regimen | Side Effects (n, %) | Examples of Side Effects (n) | |
|---|---|---|---|---|---|
| Yamanishi et al. [22] | 151 | UUI | Active vs. sham in 2:1 order. Active: 25 min MS, 10 Hz continuously. Sham: 25 min MS, 1 Hz, alternating 5 s on, 5 s off. Twice a week, 6 weeks. | Active: 16 (15.8%) Sham: 3 (6.0%) | Diarrhea (6), constipation (3), myalgia (3), somnolence (3), flatulence (1), muscular weakness (1), pain in extremity (1), limb discomfort (1), back pain (1), … |
| Voorham et al. [35] | 65 | SUI, UUI, MUI | 21 min MS SUI: 2 × 10 min at 50 Hz, 1-min break in between UUI: 2 × 10 min at 10 Hz, 1-min break in between MUI: 10 min at 10 Hz, 10 min at 50 Hz, 1-min break in between. Twice a week, 8 weeks. | 0 patient reported | EMG registered rest tone of the pelvic floor muscles was higher after treatment. |
| Ismail et al. [59] | 48 | SUI | 5 s on, 5 s off starting at 5 Hz, gradually increasing until 50 Hz. 2 × 10 min at 50 Hz, 2-min break in between. Twice a week, 8 weeks. | 25 (52.1%) | Lower limb pain (9), abdominal pain (7), cystitis (6), bowel symptoms (6), backache (5), chair powerful (3), difficult positioning (2), tingling (2), perineal pain (2), neck pain (1), etc. |
| Lim et al. [60] | 120 | SUI | Active vs. sham in 1:1 order. 20 min MS Active: 8 s on, 4 s off at 50 Hz. Sham: 8 s on, 4 s off with tilted magnetic coil. Twice a week, 8 weeks. | Active: 3 (5.3%) Sham: 5 (8.6%) | Pain at gluteal muscles and hipbone, yellow vaginal discharge, constipation, diarrhea, mouth ulcer, delayer menstruation, burning sensation or difficulty in passing urine. |
| Tezer et al. [61] | 76 | UUI | Bladder training vs. bladder training + MS in 1:1 order. 20 min MS, 10 Hz continuously Twice a week, 6 weeks. | MS: 4 (11.5%) | Temporary discomfort due to pelvic floor pain (3), malaise (1). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavčnik, M.; Antić, A.; Lukanović, A.; Krpan, Ž.; Lukanović, D. Evaluation of Possible Side Effects in the Treatment of Urinary Incontinence with Magnetic Stimulation. Medicina 2023, 59, 1286. https://doi.org/10.3390/medicina59071286
Pavčnik M, Antić A, Lukanović A, Krpan Ž, Lukanović D. Evaluation of Possible Side Effects in the Treatment of Urinary Incontinence with Magnetic Stimulation. Medicina. 2023; 59(7):1286. https://doi.org/10.3390/medicina59071286
Chicago/Turabian StylePavčnik, Maja, Anja Antić, Adolf Lukanović, Žan Krpan, and David Lukanović. 2023. "Evaluation of Possible Side Effects in the Treatment of Urinary Incontinence with Magnetic Stimulation" Medicina 59, no. 7: 1286. https://doi.org/10.3390/medicina59071286
APA StylePavčnik, M., Antić, A., Lukanović, A., Krpan, Ž., & Lukanović, D. (2023). Evaluation of Possible Side Effects in the Treatment of Urinary Incontinence with Magnetic Stimulation. Medicina, 59(7), 1286. https://doi.org/10.3390/medicina59071286