
Common Practice in the Treatment of Superficial Vein Thrombosis Involving the Sapheno-Femoral Junction: Results from a National Survey of the Italian Society of Angiology and Vascular Medicine (SIAPAV)

 ,
,  ,
on behalf of SIAPAV Members
,
on behalf of SIAPAV Members
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frappé, P.; Buchmuller-Cordier, A.; Bertoletti, L.; Bonithon-Kopp, C.; Couzan, S.; Lafond, P.; Leizorovicz, A.; Merah, A.; Presles, E.; Preynat, P.; et al. Annual diagnosis rate of superficial vein thrombosis of the lower limbs: The STEPH community-based study. J. Thromb. Haemost. 2014, 12, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Geersing, G.J.; Cazemier, S.; Rutten, F.; Fitzmaurice, D.A.; Hoes, A.W. Incidence of superficial vein thrombosis in primary care and risk of subsequent venous thromboembolic sequelae: A retrospective cohort study performed with routine healthcare data from the Netherlands. BMJ Open 2018, 8, e019967. [Google Scholar] [CrossRef] [PubMed]
- Decousus, H.; Quere, I.; Presles, E.; Becker, F.; Barrellier, M.T.; Chanut, M.; Gillet, J.L.; Guenneguez, H.; Leandri, C.; Mismetti, P.; et al. Superficial venous thrombosis and venous thromboembolism. A large, prospective epidemiologic study. Ann. Intern. Med. 2010, 152, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Genty, C.; Sevestre, M.-A.; Brisot, D.; Lausecker, M.; Gillet, J.-L.; Rolland, C.; Righini, M.; Leftheriotis, G.; Bosson, J.-L.; Quere, I.; et al. Predictive factors for concurrent deep-vein thrombosis and symptomatic venous thromboembolic recurrence in case of superficial venous thrombosis. The OPTIMEV Study. Thromb. Haemost. 2011, 105, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, B.; Filippini, M.; Tonti, D.; Avruscio, G.; Ghirarduzzi, A.; Bucherini, E.; Camporese, G.; Imberti, D.; Palareti, G.; The STEFLUX Investigators. A randomized double-blind study of low-molecular heparin (parnaparin) for superficial vein thrombosis: STEFLUX (Superficial ThromboEmbolism and Fluxum). J. Thromb. Haemost. 2012, 10, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Decousus, H.; Prandoni, P.; Mismetti, P.; Bauersachs, R.M.; Boda, Z.; Brenner, B.; Laporte, S.; Matyas, L.; Middeldorp, S.; Sokurenko, G.; et al. Fondaparinux for the treatment of superficial-vein thrombosis in the legs. N. Engl. J. Med. 2010, 363, 1222–1232. [Google Scholar] [CrossRef] [PubMed]
- Beyer-Westendorf, J.; Schellong, S.M.; Gerlach, H.; Rabe, E.; Weitz, J.I.; Jersemann, K.; Sahin, K.; Bauersachs, R.; SURPRISE Investigators. Prevention of thromboembolic complications in patients with superficial-vein thrombosis given rivaroxaban or fondaparinux: The open-label, randomized, non-inferiority SURPRISE phase 3b trial. Lancet Haematol. 2017, 4, e105–e113. [Google Scholar] [CrossRef] [PubMed]
- Beyer-Westendorf, J. Controversies in venous thromboembolism: To treat or not to treat superficial vein thrombosis. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.M.; Woller, S.C.; Kreuziger, L.B.; Bounameaux, H.; Doerschug, K.; Geersing, G.J.; Huisman, M.V.; Kearon, C.; King, C.S.; Knighton, A.J.; et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest 2021, 160, e545–e608. [Google Scholar] [CrossRef] [PubMed]
- Ortel, T.L.; Neumann, I.; Ageno, W.; Beyth, R.; Clark, N.P.; Cuker, A.; Hutten, B.A.; Jaff, M.R.; Manja, V.; Schulman, S.; et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: Treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020, 4, 4693–4738. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Pesavento, R.; Bilora, F.; Fernandez Reyes, J.L.; Madridano, O.; Soler, S.; Monreal, M.; the RIETE Investigators. No difference in outcome between therapeutic and preventive anticoagulation in patients with superficial vein thrombosis involving the saphenous-femoral junction. Vasc. Med. 2022, 27, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Q1 | What is your specialization? |
| Q2 | How many cases of superficial vein thrombosis do you see and treat annually? |
| Q3 | How many of these superficial venous thromboses affect the last 3 cm of the great saphenous vein or the small saphenous vein or extend close to the sapheno-femoral or sapheno-popliteal junctions? |
| Q4 | What is the first-choice pharmacological treatment for superficial vein thrombosis that is constantly adopted in the Center where you work? |
| Q5 | What is the optimal duration of the pharmacological treatment you use in the treatment of superficial vein thrombosis? |
| Q6 | With regard to the drug you use in the treatment of superficial vein thrombosis, how do you use the drug? |
| Q7 | Is the therapeutic regimen you use prescribed to all patients, regardless of comorbidities (e.g., known thrombophilia, cancer, previous VTE, etc.), or is it personalized on the basis of any concomitant disease with a strong thrombogenic drive that may be present? |
| Q8 | Which is your therapeutic strategy for the treatment of superficial vein thrombosis involving the last 3 cm of the great saphenous vein or of the small saphenous vein and extended close to the sapheno-femoral or sapheno-popliteal junctions, respectively? |
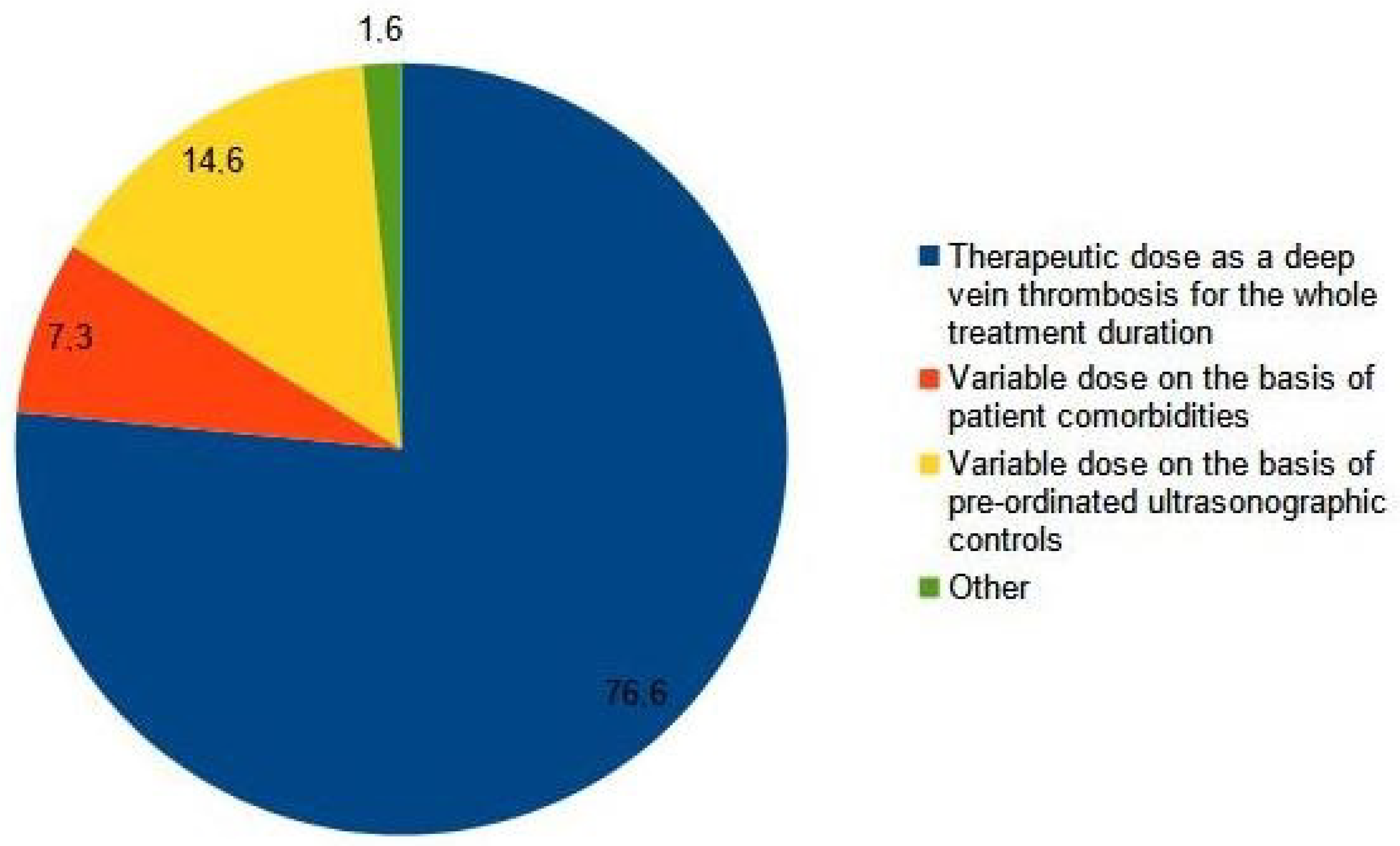
| Q9 | You prescribe the drug chosen for the treatment of the iuxta-femoral or iuxta-popliteal superficial vein thrombosis at: |
| Q10 | According to your experience, what should be the optimal duration of the treatment for iuxta-junctional superficial vein thrombosis? |
| Angiology | 34.54% |
| Vascular Surgery | 23.71% |
| Internal Medicine | 29.38% |
| Hematology | 1.03% |
| Other | 11.34% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camporese, G.; Di Micco, P.; Di Nisio, M.; Ageno, W.; Martini, R.C.; Prandoni, P., on behalf of SIAPAV Members. Common Practice in the Treatment of Superficial Vein Thrombosis Involving the Sapheno-Femoral Junction: Results from a National Survey of the Italian Society of Angiology and Vascular Medicine (SIAPAV). Medicina 2023, 59, 1068. https://doi.org/10.3390/medicina59061068
Camporese G, Di Micco P, Di Nisio M, Ageno W, Martini RC, Prandoni P on behalf of SIAPAV Members. Common Practice in the Treatment of Superficial Vein Thrombosis Involving the Sapheno-Femoral Junction: Results from a National Survey of the Italian Society of Angiology and Vascular Medicine (SIAPAV). Medicina. 2023; 59(6):1068. https://doi.org/10.3390/medicina59061068
Chicago/Turabian StyleCamporese, Giuseppe, Pierpaolo Di Micco, Marcello Di Nisio, Walter Ageno, Romeo Costanzo Martini, and Paolo Prandoni on behalf of SIAPAV Members. 2023. "Common Practice in the Treatment of Superficial Vein Thrombosis Involving the Sapheno-Femoral Junction: Results from a National Survey of the Italian Society of Angiology and Vascular Medicine (SIAPAV)" Medicina 59, no. 6: 1068. https://doi.org/10.3390/medicina59061068
APA StyleCamporese, G., Di Micco, P., Di Nisio, M., Ageno, W., Martini, R. C., & Prandoni, P., on behalf of SIAPAV Members. (2023). Common Practice in the Treatment of Superficial Vein Thrombosis Involving the Sapheno-Femoral Junction: Results from a National Survey of the Italian Society of Angiology and Vascular Medicine (SIAPAV). Medicina, 59(6), 1068. https://doi.org/10.3390/medicina59061068