
Ventilation Difficulty Caused by Obstructed Heated Breathing Circuit

 ,
, {kind=link}
{kind=link}
Abstract
1. Introduction
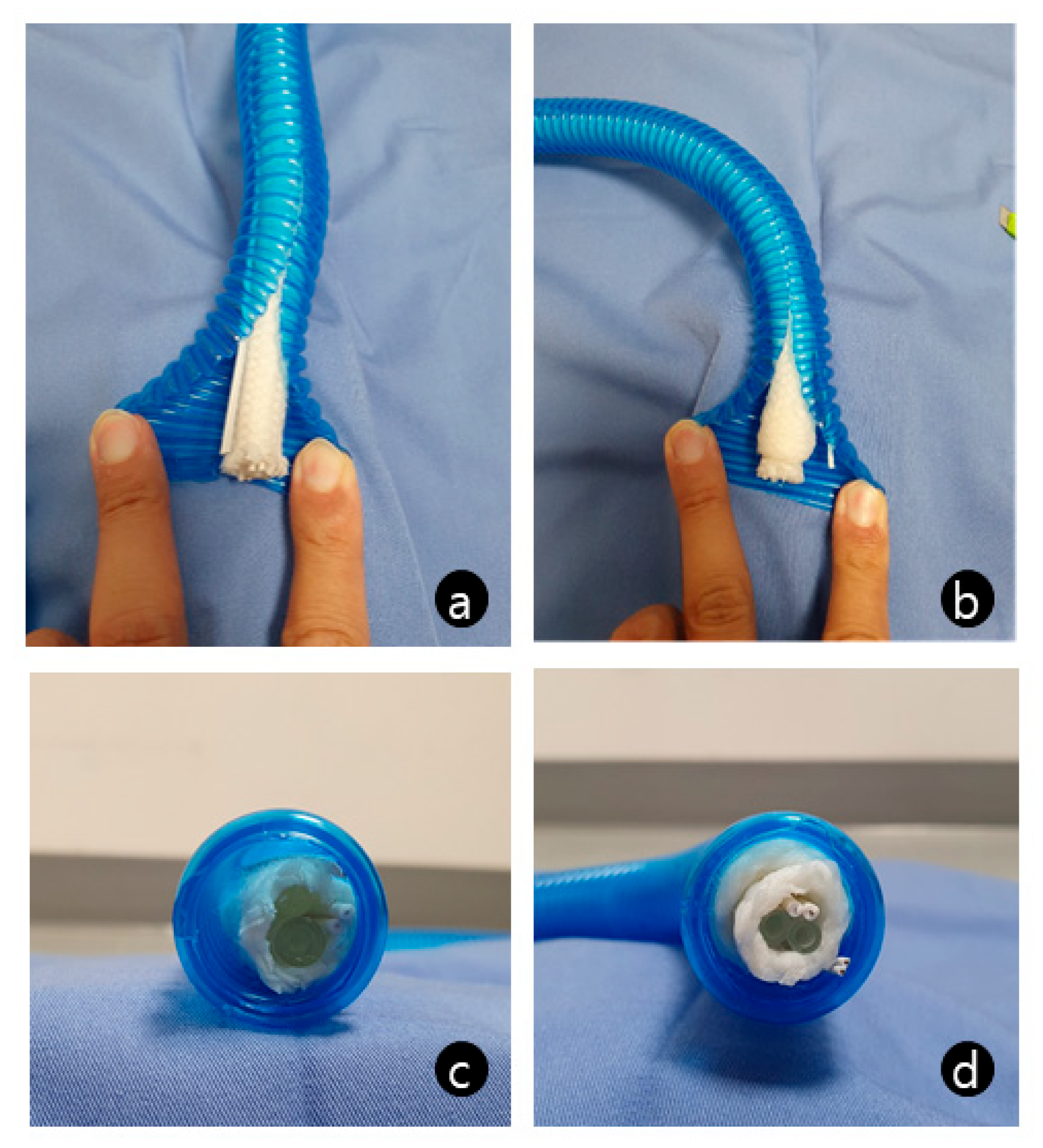
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajagopalan, S.; Mascha, E.; Na, J.; Sessler, D.I. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology 2008, 108, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.M.; Fleisher, L.A.; Breslow, M.J.; Higgins, M.S.; Olson, K.F.; Kelly, S.; Beattie, C. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA 1997, 277, 1127–1134. [Google Scholar] [CrossRef]
- Shakhar, G.; Ben-Eliyahu, S. Potential prophylactic measures against postoperative immunosuppression: Could they reduce recurrence rates in oncological patients? Ann. Surg. Oncol. 2003, 10, 972–992. [Google Scholar] [CrossRef]
- Kurz, A.; Sessler, D.I.; Lenhardt, R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group. N. Engl. J. Med. 1996, 334, 1209–1215. [Google Scholar] [CrossRef]
- Nakagawa, N.K.; Macchione, M.; Petrolino, H.M.; Guimarães, E.T.; King, M.; Saldiva, P.H.; Lorenzi-Filho, G. Effects of a heat and moisture exchanger and a heated humidifier on respiratory mucus in patients undergoing mechanical ventilation. Crit. Care Med. 2000, 28, 312–317. [Google Scholar] [CrossRef]
- Jung, T.H.; Rho, J.H.; Hwang, J.H.; Lee, J.H.; Cha, S.C.; Woo, S.C. The effect of the humidifier on sore throat and cough after thyroidectomy. Korean J. Anesthesiol. 2011, 61, 470–474. [Google Scholar] [CrossRef]
- Kim, E.; Lee, S.Y.; Lim, Y.J.; Choi, J.Y.; Jeon, Y.T.; Hwang, J.W.; Park, H.P. Effect of a new heated and humidified breathing circuit with a fluid-warming device on intraoperative core temperature: A prospective randomized study. J. Anesth. 2015, 29, 499–507. [Google Scholar] [CrossRef]
- Do, W.; Kang, D.; Hong, P.; Kim, H.J.; Baik, J.; Lee, D. Incidental operating room fire from a breathing circuit warmer system: A case report. BMC Anesthesiol. 2021, 21, 271. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Cho, K.R.; Lee, J.H. Contact burn due to a heated-wire breathing circuit. J. Anesth. 2014, 28, 802. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Chen, K.H.; Lee, Y.E.; Lin, C.R. Anesthetic breathing circuit obstruction mimicking severe bronchospasm: An unusual manufacturing defect. Acta Anaesthesiol. Taiwan 2012, 50, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Eckhout, G.V.; Bhatia, S. Another cause of difficulty in ventilating a patient. J. Clin. Anesth. 2003, 15, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Langeron, O.; Masso, E.; Huraux, C.; Guggiari, M.; Bianchi, A.; Coriat, P.; Riou, B. Prediction of difficult mask ventilation. Anesthesiology 2000, 92, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.P.; Eisenkraft, J.B.; Posner, K.L.; Domino, K.B. Patient injuries from anesthesia gas delivery equipment: A closed claims update. Anesthesiology 2013, 119, 788–795. [Google Scholar] [CrossRef] [PubMed]
- American Society of Anesthesiologists. Available online: https://www.asahq.org/standards-and-guidelines/2008-asa-recommendations-for-pre-anesthesia-checkout (accessed on 24 February 2023).
- Dosch, M.P. Automated checkout routines in anesthesia workstations vary in detection and management of breathing circuit obstruction. Anesth. Analg. 2014, 118, 1254–1257. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, J.; Kang, E.; Shin, S.; Lee, B.; Ko, M.; Kim, S.; Lee, S. Ventilation Difficulty Caused by Obstructed Heated Breathing Circuit. Medicina 2023, 59, 965. https://doi.org/10.3390/medicina59050965
Kwon J, Kang E, Shin S, Lee B, Ko M, Kim S, Lee S. Ventilation Difficulty Caused by Obstructed Heated Breathing Circuit. Medicina. 2023; 59(5):965. https://doi.org/10.3390/medicina59050965
Chicago/Turabian StyleKwon, Jiyeon, Eunsu Kang, Sunghyun Shin, Byeongcheol Lee, Myoungjin Ko, Sehun Kim, and Soojee Lee. 2023. "Ventilation Difficulty Caused by Obstructed Heated Breathing Circuit" Medicina 59, no. 5: 965. https://doi.org/10.3390/medicina59050965
APA StyleKwon, J., Kang, E., Shin, S., Lee, B., Ko, M., Kim, S., & Lee, S. (2023). Ventilation Difficulty Caused by Obstructed Heated Breathing Circuit. Medicina, 59(5), 965. https://doi.org/10.3390/medicina59050965