
The Role of Gender in Patients with Borderline Personality Disorder: Differences Related to Hopelessness, Alexithymia, Coping Strategies, and Sensory Profile

 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
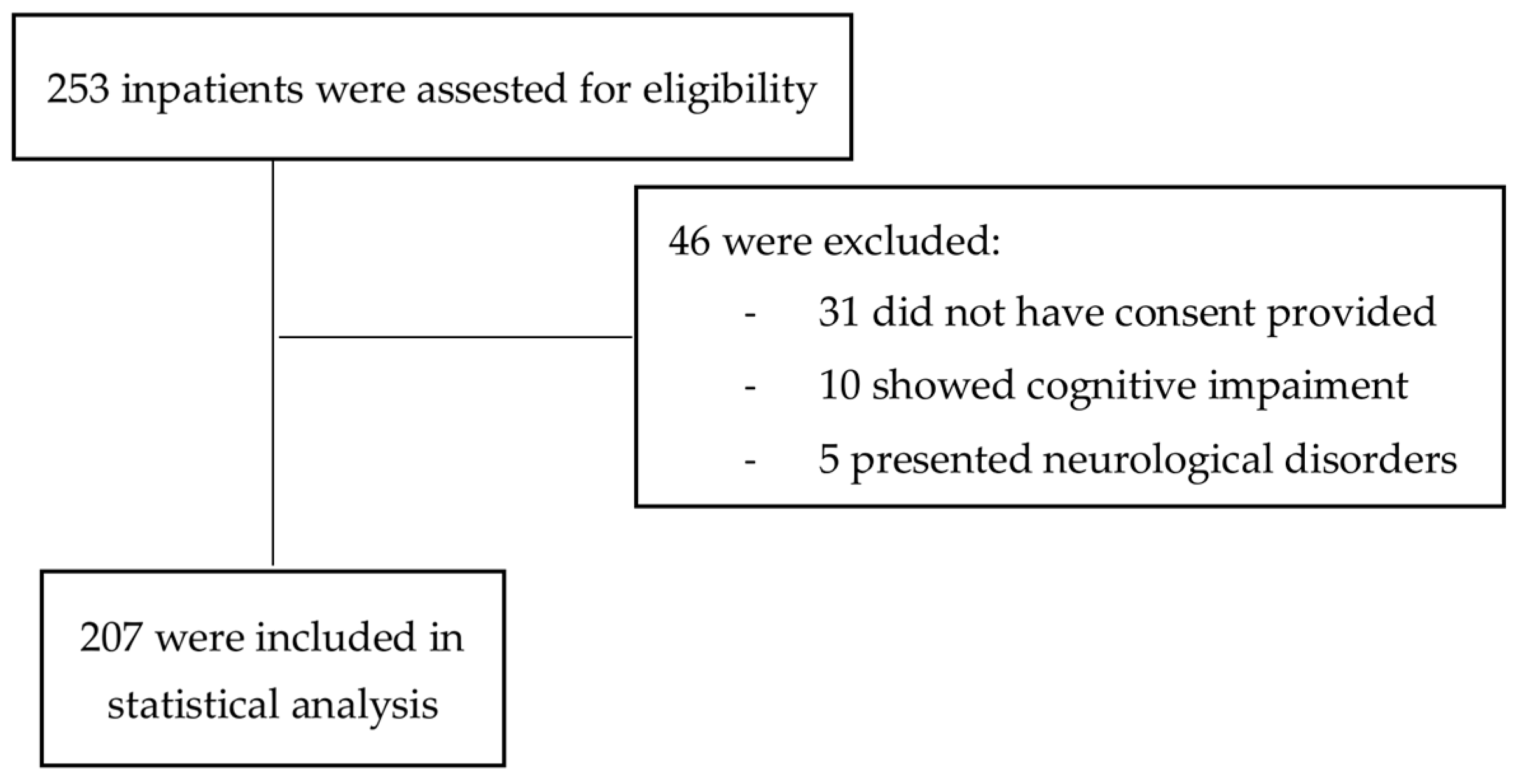
2.1. Study Design and Participants
2.2. Assessment and Procedures
2.3. Statistical Analysis
3. Results
3.1. Gender Differences in Sociodemographic and Clinical Characteristics
3.2. Gender Differences in Sensory Profile, Alexithymia, Suicidal Attitudes, and Coping Strategies
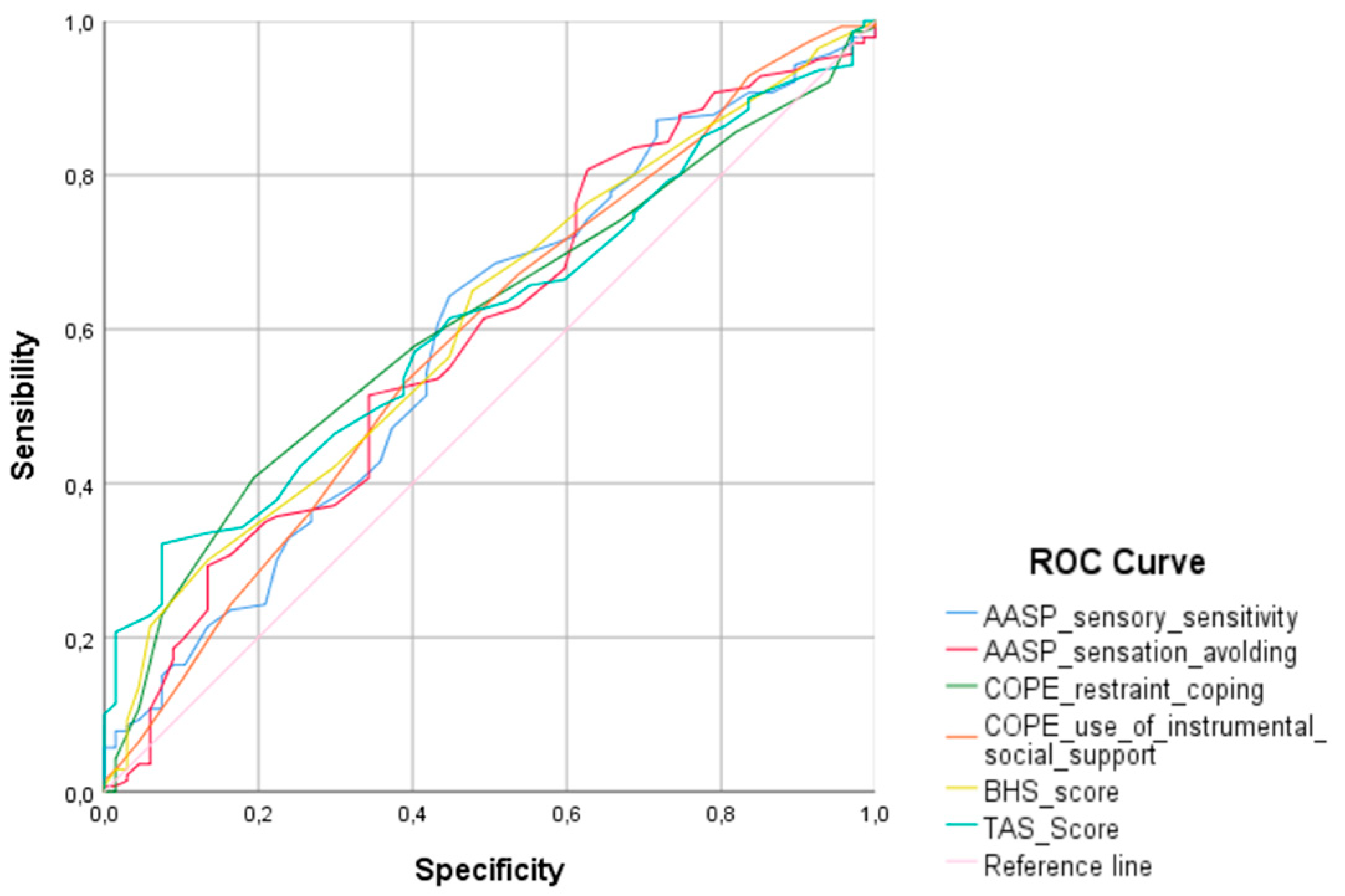
3.3. ROC Curve
3.4. Logistic Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AASP | Adolescent/Adult Sensory Profile |
| BHS | Beck Hopelessness Scale |
| BPD | Borderline Personality Disorder |
| COPE | Coping Orientation to Problems Experienced |
| DiNOGMI | Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health |
| DSM 5-TR | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision |
| IRCCS | Istituto di Ricovero e Cura a Carattere Scientifico |
| PTSD | Post-Traumatic Stress Disorder |
| SD | Standard Deviation |
| SPSS | Statistical Package for the Social Sciences |
| TAS-20 | Toronto Alexithymia Scale |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Paris, J. Suicidality in Borderline Personality Disorder. Medicina 2019, 55, 223. [Google Scholar] [CrossRef] [PubMed]
- Bohus, M.; Stoffers-Winterling, J.; Sharp, C.; Krause-Utz, A.; Schmahl, C.; Lieb, K. Borderline personality disorder. Lancet 2021, 398, 1528–1540. [Google Scholar] [CrossRef] [PubMed]
- Furnes, D.; Gjestad, R.; Mehlum, L.; Hodgekins, J.; Kroken, R.A.; Oedegaard, K.; Mellesdal, L. Borderline Personality Disorder: What Predicts Acute Psychiatric Readmissions? J. Pers. Disord. 2021, 35, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, S.; Bateman, A.; Bohus, M.; Dalewijk, H.J.; Doering, S.; Kaera, A.; Moran, P.; Renneberg, B.; Ribaudi, J.S.; Taubner, S.; et al. European guidelines for personality disorders: Past, present and future. Borderline Pers. Disord. Emot. Dysregulat. 2019, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Lenzenweger, M.F. Epidemiology of Personality Disorders. Psychiatr. Clin. N. Am. 2008, 31, 395–403. [Google Scholar] [CrossRef]
- Gunderson, J.G. Borderline Personality Disorder: Ontogeny of a Diagnosis. Am. J. Psychiatr. 2009, 166, 530–539. [Google Scholar] [CrossRef]
- Lenzenweger, M.F. Current Status of the Scientific Study of the Personality Disorders: An Overview of Epidemiological, Longitudinal, Experimental Psychopathology, and Neurobehavioral Perspectives. J. Am. Psychoanal. Assoc. 2010, 58, 741–778. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders–Text Revision (DSM 5-TR); American Psychiatric Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Grant, B.F.; Chou, S.P.; Goldstein, R.B.; Huang, B.; Stinson, F.S.; Saha, T.D.; Smith, S.M.; Dawson, D.S.; Pulay, A.J.; Pickering, R.P.; et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: Results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatr. 2008, 69, 533–545. [Google Scholar] [CrossRef]
- Hoertel, N.; Peyre, H.; Wall, M.M.; Limosin, F.; Blanco, C. Examining sex differences in DSM-IV borderline personality disorder symptom expression using Item Response Theory (IRT). J. Psychiatr. Res. 2014, 59, 213–219. [Google Scholar] [CrossRef]
- Silberschmidt, A.; Lee, S.; Zanarini, M.; Schulz, S.C. Gender Differences in Borderline Personality Disorder: Results from a Multinational, Clinical Trial Sample. J. Pers. Disord. 2015, 29, 828–838. [Google Scholar] [CrossRef]
- Skodol, A.E.; Bender, D.S. Why Are Women Diagnosed Borderline More Than Men? Psychiatr. Q. 2003, 74, 349–360. [Google Scholar] [CrossRef]
- Sansone, R.A.; Wiederman, M.W. Sex and age differences in symptoms in borderline personality symptomatology. Int. J. Psychiatr. Clin. Pr. 2013, 18, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Black, D.W.; Blum, N.; Pfohl, B.; Hale, N. Suicidal Behavior in Borderline Personality Disorder: Prevalence, Risk Factors, Prediction, and Prevention. J. Pers. Disord. 2004, 18, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Brown, G.; Steer, R.A. Prediction of eventual suicide in psychiatric inpatients by clinical ratings of hopelessness. J. Consult. Clin. Psychol. 1989, 57, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Franza, F.; Zarrella, A.; Calabrese, L.; Ferrara, I.; Solomita, B.; Tavormina, G. Hope in Psychiatric Patients: An Observational Study in a Psychiatric Rehabilitation Centre. Psychiatr. Danub. 2022, 34 (Suppl. 8), 60–63. [Google Scholar]
- Marco, J.H.; Guillén, V.; Botella, C. The buffer role of meaning in life in hopelessness in women with borderline personality disorders. Psychiatr. Res. 2017, 247, 120–124. [Google Scholar] [CrossRef]
- Costanza, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Amore, M. Meaning in Life and Demoralization Constructs in Light of the Interpersonal Theory of Suicide: A Trans-Theoretical Hypothesis for a Cross-Sectional Study. Psychol. Res. Behav. Manag. 2020, 13, 855–858. [Google Scholar] [CrossRef]
- Costanza, A.; Amerio, A.; Odone, A.; Baertschi, M.; Richard-Lepouriel, H.; Weber, K.; Di Marco, S.; Prelati, M.; Aguglia, A.; Escelsior, A.; et al. Suicide prevention from a public health perspective.: What makes life meaningful? The opinion of some suicidal patients. Acta Biomed. 2020, 91, 128–134. [Google Scholar] [CrossRef]
- Costanza, A.; Vasileios, C.; Ambrosetti, J.; Shah, S.; Amerio, A.; Aguglia, A.; Serafini, G.; Piguet, V.; Luthy, C.; Cedraschi, C.; et al. Demoralization in suicide: A systematic review. J. Psychosom. Res. 2022, 157, 110788. [Google Scholar] [CrossRef]
- Conklin, C.Z.; Bradley, R.; Westen, D. Affect Regulation in Borderline Personality Disorder. J. Nerv. Ment. Dis. 2006, 194, 69–77. [Google Scholar] [CrossRef]
- Domes, G.; Schulze, L.; Herpertz, S.C. Emotion Recognition in Borderline Personality Disorder—A Review of the Literature. J. Pers. Disord. 2009, 23, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D. The 20-Item Toronto Alexithymia Scale. IV. Reliability and factorial validity in different languages and cultures. J. Psychosom. Res. 2003, 55, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Kılıç, F.; Demirdaş, A.; Işık, Ü.; Akkuş, M.; Atay, I.M.; Kuzugüdenlioğlu, D. Empathy, Alexithymia, and Theory of Mind in Borderline Personality Disorder. J. Nerv. Ment. Dis. 2020, 208, 736–741. [Google Scholar] [CrossRef] [PubMed]
- Starcevic, V.; Janca, A. Personality dimensions and disorders and coping with the COVID-19 pandemic. Curr. Opin. Psychiatr. 2021, 35, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.R.; Rose, N.L.J.; Gromatsky, M.; Feinberg, A.; Kimhy, D.; Doucette, J.T.; Goodman, M.; McClure, M.M.; Perez-Rodriguez, M.M.; New, A.S.; et al. Alexithymia, Affective Lability, Impulsivity, and Childhood Adversity in Borderline Personality Disorder. J. Pers. Disord 2021, 35 (Suppl. A), 114–131. [Google Scholar] [CrossRef]
- Linehan, M.M.; Bohus, M.; Lynch, T.R. Dialectical Behavior Therapy for Pervasive Emotion Dysregulation. In Gross J. Handbook of Emotion Regulation; Guilford Press: New York, NY, USA, 2007; pp. 581–605. [Google Scholar]
- Almeida, D.M.; Kessler, R.C. Everyday stressors and gender differences in daily distress. J. Pers. Soc. Psychol. 1998, 75, 670–680. [Google Scholar] [CrossRef]
- Kremers, I.; Spinhoven, P.; Van der Does, A.; Van Dyck, R. Social problem solving, autobiographical memory and future specificity in outpatients with borderline personality disorder. Clin. Psychol. Psychother. 2006, 13, 131–137. [Google Scholar] [CrossRef]
- Carlson, E.M.; Cox, D.W.; Kealy, D.; Chapman, A.L.; Ogrodniczuk, J.S. Social role dysfunction and coping in borderline personality disorder. Pers. Ment. Health 2020, 14, 227–239. [Google Scholar] [CrossRef]
- Chaudhury, S.R.; Galfalvy, H.; Biggs, E.; Choo, T.-H.; Mann, J.J.; Stanley, B. Affect in response to stressors and coping strategies: An ecological momentary assessment study of borderline personality disorder. Borderline Pers. Disord. Emot. Dysregulat. 2017, 4, 8. [Google Scholar] [CrossRef]
- Brown, S.; Shankar, R.; Smith, K. Borderline personality disorder and sensory processing impairment. Prog. Neurol. Psychiatr. 2009, 13, 10–16. [Google Scholar] [CrossRef]
- Meyer, B.; Ajchenbrenner, M.; Bowles, D.P. Sensory Sensitivity, Attachment Experiences, and Rejection Responses Among Adults with Borderline and Avoidant Features. J. Pers. Disord. 2005, 19, 641–658. [Google Scholar] [CrossRef] [PubMed]
- Jakobson, L.S.; Rigby, S.N. Alexithymia and Sensory Processing Sensitivity: Areas of Overlap and Links to Sensory Processing Styles. Front. Psychol. 2021, 12, 583786. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Brown, C.; Tollefson, N.; Dunn, W.; Cromwell, R.; Filion, D. The Adult Sensory Profile: Measuring Patterns of Sensory Processing. Am. J. Occup. Ther. 2001, 55, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The Hopelessness Scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M.; Saffer, B.Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Taylor, G.J.; Ryan, D.; Bagby, R.M. Toward the Development of a New Self-Report Alexithymia Scale. Psychother. Psychosom. 1985, 44, 191–199. [Google Scholar] [CrossRef]
- Sher, L.; Rutter, S.B.; New, A.S.; Siever, L.J.; Hazlett, E.A. Gender differences and similarities in aggression, suicidal behaviour, and psychiatric comorbidity in borderline personality disorder. Acta Psychiatr. Scand. 2018, 139, 145–153. [Google Scholar] [CrossRef]
- Hazlett, E.A.; Speiser, L.J.; Goodman, M.; Roy, M.; Carrizal, M.; Wynn, J.K.; Williams, W.C.; Romero, M.; Minzenberg, M.J.; Siever, L.J.; et al. Exaggerated Affect-Modulated Startle During Unpleasant Stimuli in Borderline Personality Disorder. Biol. Psychiatr. 2007, 62, 250–255. [Google Scholar] [CrossRef]
- New, A.S.; Rot, M.A.H.; Ripoll, L.H.; Perez-Rodriguez, M.M.; Lazarus, S.; Zipursky, E.; Weinstein, S.R.; Koenigsberg, H.W.; Hazlett, E.A.; Goodman, M.; et al. Empathy and Alexithymia in Borderline Personality Disorder: Clinical and Laboratory Measures. J. Pers. Disord. 2012, 26, 660–675. [Google Scholar] [CrossRef] [PubMed]
- Derks, Y.P.M.J.; Westerhof, G.J.; Bohlmeijer, E.T. A Meta-analysis on the Association Between Emotional Awareness and Borderline Personality Pathology. J. Pers. Disord. 2017, 31, 362–384. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.R.; Wupperman, P. Emotion Regulation Mediates Effects of Alexithymia and Emotion Differentiation on Impulsive Aggressive Behavior. Deviant Behav. 2017, 3810, 1160–1171. [Google Scholar] [CrossRef]
- Kealy, D.; Ogrodniczuk, J.S.; Rice, S.M.; Oliffe, J.L. Alexithymia, suicidal ideation and health-risk behaviours: A survey of Canadian men. Int. J. Psychiatr. Clin. Pr. 2018, 22, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Le, H.-N.; Berenbaum, H.; Raghavan, C. Culture and alexithymia: Mean levels, correlates and the role of parental socialization of emotions. Emotion 2002, 2, 341–360. [Google Scholar] [CrossRef]
- Thorberg, F.A.; Young, R.M.; Sullivan, K.A.; Lyvers, M. Parental bonding and alexithymia: A meta-analysis. Eur. Psychiatr. 2011, 26, 187–193. [Google Scholar] [CrossRef]
- Edwards, E.; Shivaji, S.; Wupperman, P. The Emotion Mapping Activity: Preliminary evaluation of a mindfulness-informed exercise to improve emotion labeling in alexithymic persons. Scand. J. Psychol. 2018, 59, 319–327. [Google Scholar] [CrossRef]
- Gaher, R.M.; Arens, A.M.; Shishido, H. Alexithymia as a Mediator Between Childhood Maltreatment and Impulsivity. Stress Health 2015, 31, 274–280. [Google Scholar] [CrossRef]
- Fang, S.; Chung, M.C. The impact of past trauma on psychological distress among Chinese students: The roles of cognitive distortion and alexithymia. Psychiatr. Res. 2019, 271, 136–143. [Google Scholar] [CrossRef]
- Frewen, P.A.; Dozois, D.J.; Neufeld, R.W.; Lanius, R.A. Meta-analysis of alexithymia in posttraumatic stress disorder. J. Trauma. Stress 2008, 21, 243–246. [Google Scholar] [CrossRef]
- Nowakowski, M.E.; McFarlane, T.; Cassin, S. Alexithymia and eating disorders: A critical review of the literature. J. Eat. Disord. 2013, 1, 21. [Google Scholar] [CrossRef]
- Brown, G.K.; Beck, A.T.; Steer, R.A.; Grisham, J.R. Risk factors for suicide in psychiatric outpatients: A 20-year prospective study. J. Consult. Clin. Psychol. 2000, 68, 371–377. [Google Scholar] [CrossRef]
- Pompili, M.; Iliceto, P.; Luciano, D.; Innamorati, M.; Serafini, G.; Del Casale, A.; Tatarelli, R.; Girardi, P.; Lester, D. Higher hopelessness and suicide risk predict lower self-deception among psychiatric patients and non-clinical individuals. Riv. Psichiatr. 2011, 46, 24–30. [Google Scholar] [CrossRef]
- Serafini, G.; Lamis, D.A.; Aguglia, A.; Amerio, A.; Nebbia, J.; Geoffroy, P.A.; Pompili, M.; Amore, M. Hopelessness and its correlates with clinical outcomes in an outpatient setting. J. Affect. Disord. 2020, 263, 472–479. [Google Scholar] [CrossRef]
- Norman, H.; Marzano, L.; Oskis, A.; Coulson, M. “I can’t describe it and they can’t see the rain.” an interpretative phenomenological analysis of the experience of self-harm in young adults who report difficulties identifying and describing their feelings. Curr. Psychol. 2021; epub ahead of print. [Google Scholar] [CrossRef]
- Ostertag, L.; Golay, P.; Dorogi, Y.; Brovelli, S.; Bertran, M.; Cromec, I.; Van Der Vaeren, B.; Khan, R.; Costanza, A.; Wyss, K.; et al. The implementation and first insights of the French-speaking Swiss programme for monitoring self-harm. Swiss Med. Wkly. 2019, 149, w20016. [Google Scholar] [CrossRef]
- Aron, E.N.; Aron, A.; Jagiellowicz, J. Sensory Processing Sensitivity. Pers. Soc. Psychol. Rev. 2012, 16, 262–282. [Google Scholar] [CrossRef]
- Machingura, T.; Kaur, G.; Lloyd, C.; Mickan, S.; Shum, D.; Rathbone, E.; Green, H. An exploration of sensory processing patterns and their association with demographic factors in healthy adults. Ir. J. Occup. Ther. 2019, 48, 3–16. [Google Scholar] [CrossRef]
- Blanche, E.I.; Parham, D.; Chang, M.; Mallinson, T. Development of an Adult Sensory Processing Scale (ASPS). Am. J. Occup. Ther. 2014, 68, 531–538. [Google Scholar] [CrossRef]
- Costanza, A.; Amerio, A.; Aguglia, A.; Magnani, L.; Serafini, G.; Amore, M.; Merli, R.; Ambrosetti, J.; Bondolfi, G.; Marzano, L.; et al. Hard to Say, Hard to Understand, Hard to Live": Possible Associations between Neurologic Language Impairments and Suicide Risk. Brain Sci. 2021, 11, 1594. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) or Mean ± SD | Total Sample (n = 207) | Males (n = 67) | Females (n = 140) | X2/t | p |
|---|---|---|---|---|---|
| Current age | 33.87 ± 13.57 | 34.72 ± 13.41 | 33.46 ± 13.68 | 0.620 | 0.536 |
| Marital status | 4.171 | 0.244 | |||
| Single | 142 (68.6) | 49 (73.1) | 93 (66.4) | ||
| Married | 35 (16.9) | 13 (19.4) | 22 (15.7) | ||
| Divorced | 29 (14.0) | 5 (7.5) | 24 (17.1) | ||
| Widowed | 1 (0.5) | 0 (0.0) | 1 (0.7) | ||
| Educational level | 11.57 ± 3.36 | 11.28 ± 3.15 | 11.71 ± 3.45 | −0.849 | 0.397 |
| Nationality | 1.758 | 0.185 | |||
| Italian | 182 (87.9) | 56 (83.6) | 126 (90.0) | ||
| Others | 25 (12.1) | 11 (16.4) | 14 (10.0) | ||
| Number of hospitalizations | 3.29 ± 3.32 | 3.15 ± 3.21 | 3.35 ± 3.38 | −0.406 | 0.685 |
| Involuntary admissions | 67 (32.4) | 28 (41.8) | 39 (27.9) | 4.019 | 0.045 |
| Suicide ideation | 112 (54.1) | 33 (49.3) | 79 (56.4) | 0.939 | 0.332 |
| Suicide attempts | 130 (59.7) | 40 (59.7) | 90 (64.3) | 0.408 | 0.523 |
| Number of suicide attempts | 2.41 ± 2.54 | 2.55 ± 3.29 | 2.34 ± 2.14 | 0.425 | 0.672 |
| Alcohol use lifetime | 120 (58.0) | 44 (65.7) | 76 (54.3) | 2.411 | 0.120 |
| Alcohol use current | 83 (40.1) | 35 (52.2) | 48 (34.3) | 6.081 | 0.014 |
| Substance use lifetime | 123 (59.4) | 47 (70.1) | 76 (54.3) | 4.729 | 0.030 |
| Substance use current | 79 (38.2) | 35 (52.2) | 44 (31.4) | 8.316 | 0.004 |
| Medication abuse lifetime | 73 (35.3) | 17 (25.4) | 56 (40.0) | 4.247 | 0.039 |
| Medication abuse current | 48 (23.2) | 9 (13.4) | 39 (27.9) | 5.293 | 0.021 |
| n (%) or Mean ± SD | Males (n = 67) | Females (n = 140) | t-Test | p |
|---|---|---|---|---|
| AASP Low Registration | 26.91 ± 11.46 | 28.70 ± 10.96 | −1.083 | 0.280 |
| AASP Sensation Seeking | 33.63 ± 11.37 | 35.24 ± 10.12 | −1.028 | 0.305 |
| AASP Sensory Sensitivity | 32.18 ± 11.80 | 37.21 ± 16.31 | −2.259 | 0.025 |
| AASP Sensation Avoiding | 31.73 ± 11.09 | 35.24 ± 11.08 | −2.128 | 0.035 |
| Toronto Alexithymia Scale-20 | 58.25 ± 10.30 | 63.44 ± 13.03 | −2.856 | 0.005 |
| Presence of Alexithymia (TAS-20 ≥ 61) | 27 (40.3) | 80 (57.1) | 5.149 | 0.023 |
| Beck Hopelessness Scale | 8.82 ± 3.99 | 10.39 ± 4.09 | −2.597 | 0.010 |
| Presence of Hopelessness (BHS ≥ 9) | 36 (53.7) | 98 (70.0) | 5.254 | 0.022 |
| Mean ± SD | Males (n = 67) | Females (n = 140) | t-Test | p |
|---|---|---|---|---|
| COPE Problem-focused coping | ||||
| Active coping | 10.57 ± 2.73 | 10.53 ± 2.49 | 0.101 | 0.920 |
| Planning | 9.96 ± 2.79 | 10.37 ± 2.63 | −1.045 | 0.297 |
| Suppression of competing activities | 9.96 ± 2.59 | 10.24 ± 2.49 | −0.768 | 0.443 |
| Restraint coping | 9.13 ± 1.87 | 9.85 ± 2.19 | −2.305 | 0.022 |
| Use of instrumental social support | 9.67 ± 2.89 | 10.66 ± 3.00 | −2.236 | 0.026 |
| COPE Emotion-focused coping | ||||
| Use of social-emotional support | 9.76 ± 2.80 | 9.74 ± 2.76 | 0.045 | 0.964 |
| Positive reinterpretation and growth | 10.42 ± 4.76 | 9.84 ± 3.26 | 1.017 | 0.310 |
| Acceptance | 10.06 ± 2.67 | 10.10 ± 2.72 | −0.100 | 0.920 |
| Humor | 8.67 ± 2.71 | 8.91 ± 3.12 | −0.546 | 0.586 |
| Venting of emotions | 9.99 ± 3.02 | 10.72 ± 2.69 | −1.770 | 0.078 |
| Turning to religion | 8.51 ± 3.23 | 8.39 ± 3.64 | 0.233 | 0.816 |
| COPE Potentially disadaptive strategies | ||||
| Denial | 9.18 ± 2.65 | 9.26 ± 3.16 | −0.175 | 0.861 |
| Behavioral disengagement | 9.39 ± 2.65 | 9.23 ± 2.35 | 0.438 | 0.662 |
| Alcohol and drug disengagement | 9.04 ± 3.30 | 9.24 ± 3.19 | −0.414 | 0.680 |
| Mental disengagement | 9.78 ± 2.55 | 10.27 ± 2.35 | −1.381 | 0.169 |
| Variables | p | OR | 95% CI |
|---|---|---|---|
| Involuntary admissions lifetime | 0.038 | 0.484 | 0.244–0.962 |
| Current alcohol use | 0.006 | 0.402 | 0.208–0.775 |
| Current medication abuse | 0.015 | 3.056 | 1.244–7.505 |
| Presence of hopelessness (BHS ≥ 9) | 0.010 | 2.582 | 1.253–5.321 |
| Presence of alexithymia (TAS-20 ≥ 61) | 0.039 | 2.053 | 1.037–4.065 |
| COPE restraint coping | 0.049 | 1.174 | 1.001–1.377 |
| COPE use of instrumental social support | 0.005 | 1.201 | 1.058–1.363 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amerio, A.; Natale, A.; Gnecco, G.B.; Lechiara, A.; Verrina, E.; Bianchi, D.; Fusar-Poli, L.; Costanza, A.; Serafini, G.; Amore, M.; et al. The Role of Gender in Patients with Borderline Personality Disorder: Differences Related to Hopelessness, Alexithymia, Coping Strategies, and Sensory Profile. Medicina 2023, 59, 950. https://doi.org/10.3390/medicina59050950
Amerio A, Natale A, Gnecco GB, Lechiara A, Verrina E, Bianchi D, Fusar-Poli L, Costanza A, Serafini G, Amore M, et al. The Role of Gender in Patients with Borderline Personality Disorder: Differences Related to Hopelessness, Alexithymia, Coping Strategies, and Sensory Profile. Medicina. 2023; 59(5):950. https://doi.org/10.3390/medicina59050950
Chicago/Turabian StyleAmerio, Andrea, Antimo Natale, Giovanni Battista Gnecco, Alessio Lechiara, Edoardo Verrina, Davide Bianchi, Laura Fusar-Poli, Alessandra Costanza, Gianluca Serafini, Mario Amore, and et al. 2023. "The Role of Gender in Patients with Borderline Personality Disorder: Differences Related to Hopelessness, Alexithymia, Coping Strategies, and Sensory Profile" Medicina 59, no. 5: 950. https://doi.org/10.3390/medicina59050950
APA StyleAmerio, A., Natale, A., Gnecco, G. B., Lechiara, A., Verrina, E., Bianchi, D., Fusar-Poli, L., Costanza, A., Serafini, G., Amore, M., & Aguglia, A. (2023). The Role of Gender in Patients with Borderline Personality Disorder: Differences Related to Hopelessness, Alexithymia, Coping Strategies, and Sensory Profile. Medicina, 59(5), 950. https://doi.org/10.3390/medicina59050950