
Robot-Assisted Kyphoplasty versus Fluoroscopy-Assisted Kyphoplasty: A Meta-Analysis of Postoperative Outcomes

 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Selection
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment of the Included Studies
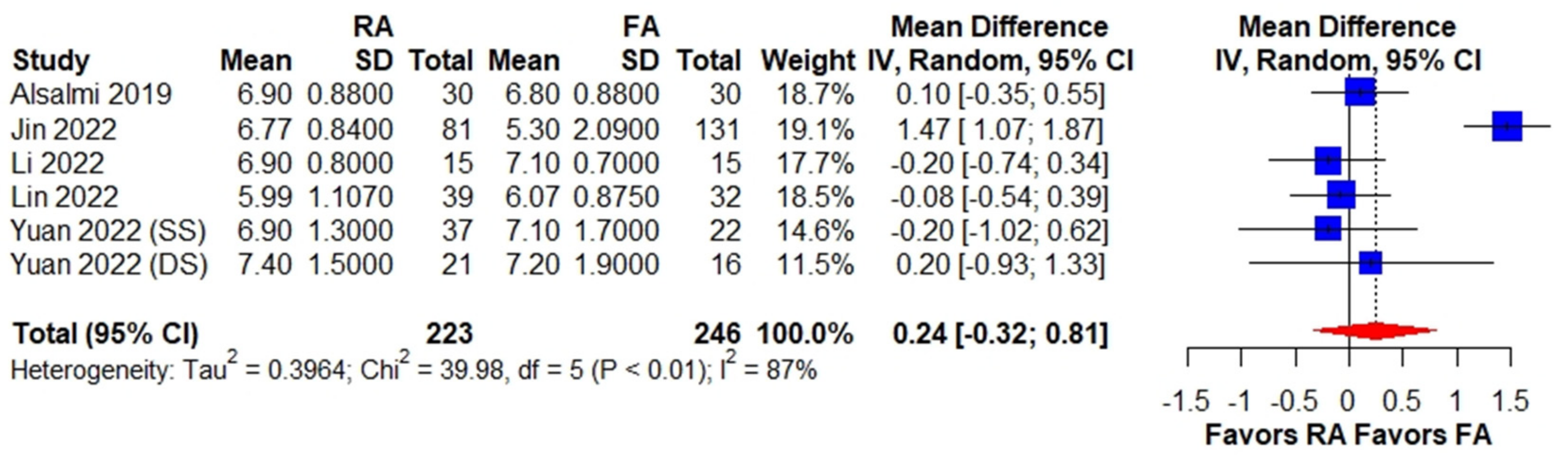
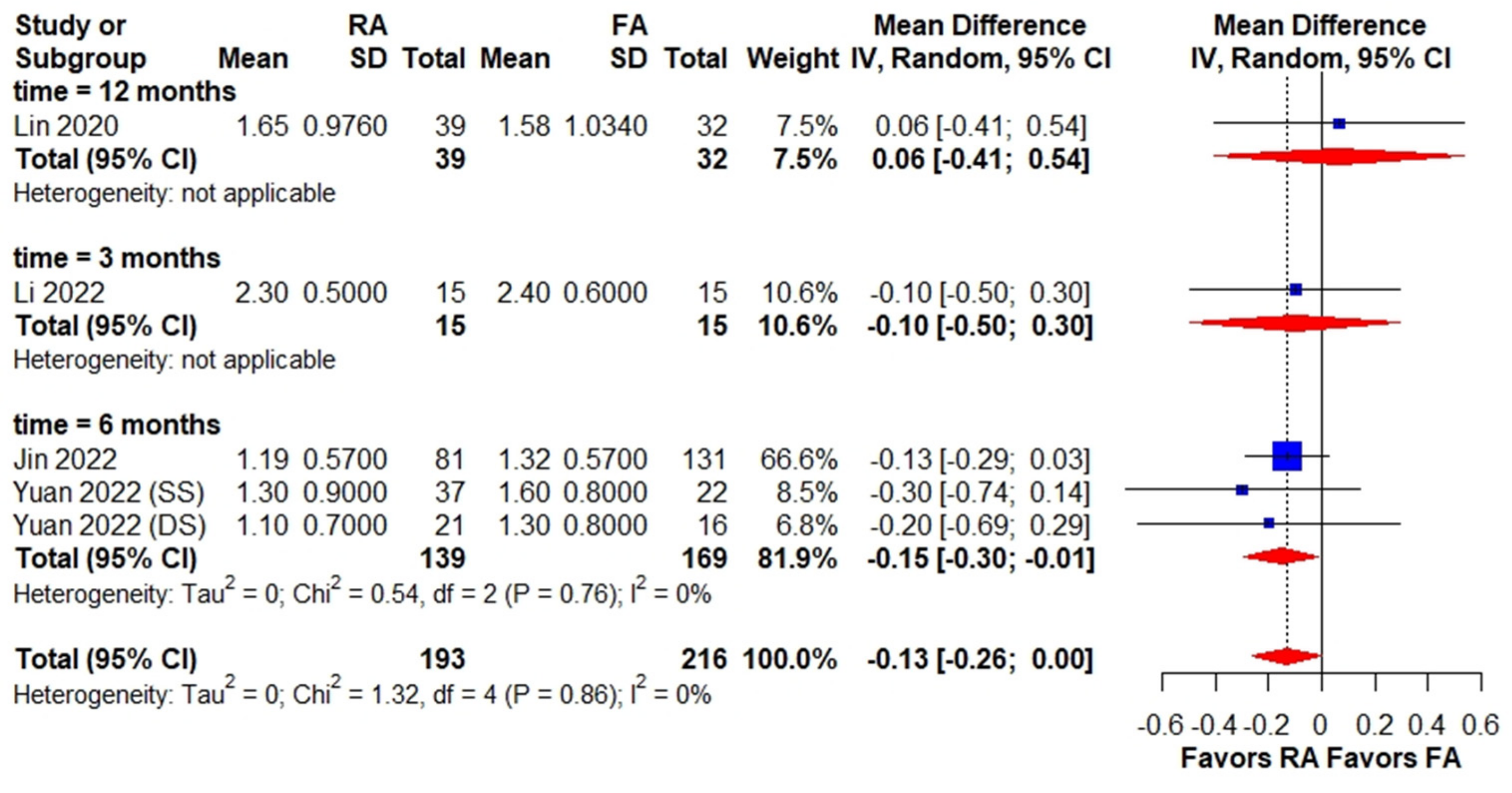
3.4. Clinical Outcomes of RA PKP versus FA PKP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, D.; Liu, J.; Ebraheim, N.A. Managements of osteoporotic vertebral compression fractures: A narrative review. World J. Orthop. 2022, 13, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Schousboe, J.T. Clinical practice. Vertebral fractures. N. Engl. J. Med. 2011, 364, 1634–1642. [Google Scholar] [CrossRef] [PubMed]
- Ballane, G.; Cauley, J.A.; Luckey, M.M.; El-Hajj Fuleihan, G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos. Int. 2017, 28, 1531–1542. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Parker, S.L.; Wolinsky, J.P.; Witham, T.F.; Bydon, A.; Gokaslan, Z.L. Vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: An evidenced-based review of the literature. Spine J. 2009, 9, 501–508. [Google Scholar] [CrossRef]
- Deng, L.; Lv, N.; Hu, X.; Guan, Y.; Hua, X.; Pan, Z.; Zhou, Q.; Wang, C.; Li, B.; Qian, Z. Comparison of efficacy of percutane vertebroplasty versus percutaneous kyphoplasty in the treatment of osteoporotic vertebral asymmetric compression fracture. World Neurosurg. 2022, 167, e1225–e1230. [Google Scholar] [CrossRef]
- Zhan, Y.; Jiang, J.; Liao, H.; Tan, H.; Yang, K. Risk factors for cement leakage after vertebroplasty or kyphoplasty: A meta-analysis of published evidence. World Neurosurg. 2017, 101, 633–642. [Google Scholar] [CrossRef]
- Chung, H.J.; Chung, K.J.; Yoon, H.S.; Kwon, I.H. Comparative study of balloon kyphoplasty with unilateral versus bilateral approach in osteoporotic vertebral compression fractures. Int. Orthop. 2008, 32, 817–820. [Google Scholar] [CrossRef]
- McKenzie, D.M.; Westrup, A.M.; O’Neal, C.M.; Lee, B.J.; Shi, H.H.; Dunn, I.F.; Snyder, L.A.; Smith, Z.A. Robotics in spine surgery: A systematic review. J. Clin. Neurosci. 2021, 89, 1–7. [Google Scholar] [CrossRef]
- Barzilay, Y.; Schroeder, J.E.; Hiller, N.; Singer, G.; Hasharoni, A.; Safran, O.; Liebergall, M.; Itshayek, E.; Kaplan, L. Robot-assisted vertebral body augmentation: A radiation reduction tool. Spine 2014, 39, 153–157. [Google Scholar] [CrossRef]
- Alsalmi, S.; Capel, C.; Chenin, L.; Peltier, J.; Lefranc, M. Robot-assisted intravertebral augmentation corrects local kyphosis more effectively than a conventional fluoroscopy-guided technique. J. Neurosurg. Spine 2018, 30, 289–295. [Google Scholar] [CrossRef]
- Jin, M.; Ge, M.; Lei, L.; Li, F.; Wu, M.; Zhang, G.; Pei, S.; Zheng, B. Clinical and radiologic outcomes of robot-assisted kyphoplasty versus fluoroscopy-assisted kyphoplasty in the treatment of osteoporotic vertebral compression fractures: A retrospective comparative study. World Neurosurg. 2022, 158, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Tang, L.Y.; Wang, F.; Yuan, X.W.; Hu, J.; Liang, W.M. TiRobot-assisted percutaneous kyphoplasty in the management of multilevel (more than three levels) osteoporotic vertebral compression fracture. Int. Orthop. 2022, 47, 319–327. [Google Scholar] [CrossRef]
- Yuan, W.; Meng, X.; Cao, W.; Zhu, Y. Robot-assisted versus fluoroscopy-assisted kyphoplasty in the treatment of osteoporotic vertebral compression fracture: A retrospective study. Glob. Spine J. 2022, 12, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.T.J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0. Cochrane. Available online: www.training.cochrane.org/handbook (accessed on 1 December 2022).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savovi’c, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. Robins-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Harville, D.A. Maximum likelihood approaches to variance component estimation and to related problems. J. Am. Stat. Assoc. 1977, 72, 320–338. [Google Scholar] [CrossRef]
- Hartung, J.; Knapp, G. A refined method for the meta-analysis of controlled clinical trials with binary outcome. Stat. Med. 2001, 20, 3875–3889. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Li, Q.; Wu, C.; Huang, Z.; Cao, J.; Chang, J.; Yin, G.; Yu, L.; Cao, X.; Sui, T. A comparison of robot-assisted and fluoroscopy-assisted kyphoplasty in the treatment of multi-segmental osteoporotic vertebral compression fractures. J. Biomed. Res. 2022, 36, 208–214. [Google Scholar] [CrossRef]
- Yu, H.; Luo, G.; Yu, B.; Sun, T.; Tang, Q.; Jia, Y. Robot-assisted kyphoplasty improves clinical and radiological features better than fluoroscopy-assisted kyphoplasty in the treatment of vertebral compression fractures: A meta-analysis. Front. Surg. 2022, 9, 955966. [Google Scholar] [CrossRef]
- Feltes, C.; Fountas, K.N.; Machinis, T.; Nikolakakos, L.G.; Dimopoulos, V.; Davydov, R.; Kassam, M.; Johnston, K.W.; Robinson, J.S. Immediate and early postoperative pain relief after kyphoplasty without significant restoration of vertebral body height in acute osteoporotic vertebral fractures. Neurosurg. Focus 2005, 18, e5. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Cao, J.; Chang, J.; Yin, G.; Cai, W.; Li, Q.; Huang, Z.; Yu, L.; Cao, X. Effectiveness of Tirobot-assisted vertebroplasty in treating thoracolumbar osteoporotic compression fracture. J. Orthop. Surg. Res. 2021, 16, 65. [Google Scholar] [CrossRef] [PubMed]
- Terracina, S.; Robba, C.; Prete, A.; Sergi, P.G.; Bilotta, F. Prevention and treatment of postoperative pain after lumbar spine procedures: A systematic review. Pain Pract. 2018, 18, 925–945. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Inclusion Period | Inclusion Criteria | Sample Size | Preoperative VAS, Mean (SD) | Postoperative VAS, Mean (SD) | Long-Term VAS, Mean (SD) | Cement Leaks Rate | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RA | FA | RA | FA | RA | FA | RA | FA | RA | FA | ||||
| Alsalmi 2019 [10] | RC | 2015–2016 | PKP for traumatic VBF | 30 | 30 | 6.9 (0.88) | 6.8 (0.88) | NA | NA | 2.56 (1.0) | 2.55 (1.1) | 45.8% | 71.9% |
| Jin 2022 [11] | RC | 2020 | PKP for OCVFs | 81 | 131 | 6.77 (0.84) | 5.30 (2.09) | 1.19 (0.57) | 1.32 (0.57) | 1.73 (0.85) | 2.10 (1.22) | 1.23% | 1.53% |
| Li 2022 [20] | RC | 2019–2021 | PKP for OCVFs | 15 | 15 | 6.9 (0.8) | 7.1 (0.7) | 2.3 (0.5) | 2.4 (0.6) | 2.5 (0.5) | 2.6 (0.5) | 6.67% | 60% |
| Lin 2022 [12] | RC | 2018–2021 | PKP for multi-segmental thoracolumbar OCVFs | 39 | 32 | 5.99 (1.11) | 6.07 (0.88) | 1.65 (0.98) | 1.58 (1.03) | 2.71 (0.96) | 3.05 (1.01) | 46.2% | 90.6 |
| Yuan 2022 [13] (SS) | RC | 2018–2019 | PKP for OCVFs | 37 | 22 | 6.9 (1.3) | 7.1 (1.7) | 1.3 (0.9) | 1.6 (0.8) | 2.0 (1.1) | 2.2 (0.9) | 8.1 | 27.3 |
| Yuan 2022 [13] (DS) | RC | 2018–2019 | PKP for OCVFs | 21 | 16 | 7.4 (1.5) | 7.2 (1.9) | 1.1 (0.7) | 1.3 (0.8) | 2.5(1.3) | 2.4 (1.1) | 9.5 | 28.1 |
| Study | Bias Due to Confounding | Bias in Selection of Participants | Bias in Classification of Intervention | Bias Due to Deviation from Intended Intervention | Bias Due to Missing Data | Bias in Measurement of Outcome | Bias in the Selection of Selected Results | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Alsalmi 2019 [10] | Moderate | Low | Low | Low | Low | Critical | Low | Critical |
| Jin 2022 [11] | Moderate | Low | Low | Low | Low | Critical | Low | Critical |
| Li 2022 [20] | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Lin 2022 [12] | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Yuan 2022 [13] | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.; Chen, W.-C.; Chi, K.-Y.; Huang, A.P.-H.; Jhang, S.-W.; Sun, L.-W.; Chen, C.-M. Robot-Assisted Kyphoplasty versus Fluoroscopy-Assisted Kyphoplasty: A Meta-Analysis of Postoperative Outcomes. Medicina 2023, 59, 662. https://doi.org/10.3390/medicina59040662
Chang Y, Chen W-C, Chi K-Y, Huang AP-H, Jhang S-W, Sun L-W, Chen C-M. Robot-Assisted Kyphoplasty versus Fluoroscopy-Assisted Kyphoplasty: A Meta-Analysis of Postoperative Outcomes. Medicina. 2023; 59(4):662. https://doi.org/10.3390/medicina59040662
Chicago/Turabian StyleChang, Yu, Wei-Cheng Chen, Kuan-Yu Chi, Abel Po-Hao Huang, Shang-Wun Jhang, Li-Wei Sun, and Chien-Min Chen. 2023. "Robot-Assisted Kyphoplasty versus Fluoroscopy-Assisted Kyphoplasty: A Meta-Analysis of Postoperative Outcomes" Medicina 59, no. 4: 662. https://doi.org/10.3390/medicina59040662
APA StyleChang, Y., Chen, W.-C., Chi, K.-Y., Huang, A. P.-H., Jhang, S.-W., Sun, L.-W., & Chen, C.-M. (2023). Robot-Assisted Kyphoplasty versus Fluoroscopy-Assisted Kyphoplasty: A Meta-Analysis of Postoperative Outcomes. Medicina, 59(4), 662. https://doi.org/10.3390/medicina59040662