
Robotic Single-Site Hysterectomy in Gynecologic Benign Pathology: A Systematic Review of the Literature


Abstract
1. Introduction
2. Materials and Methods
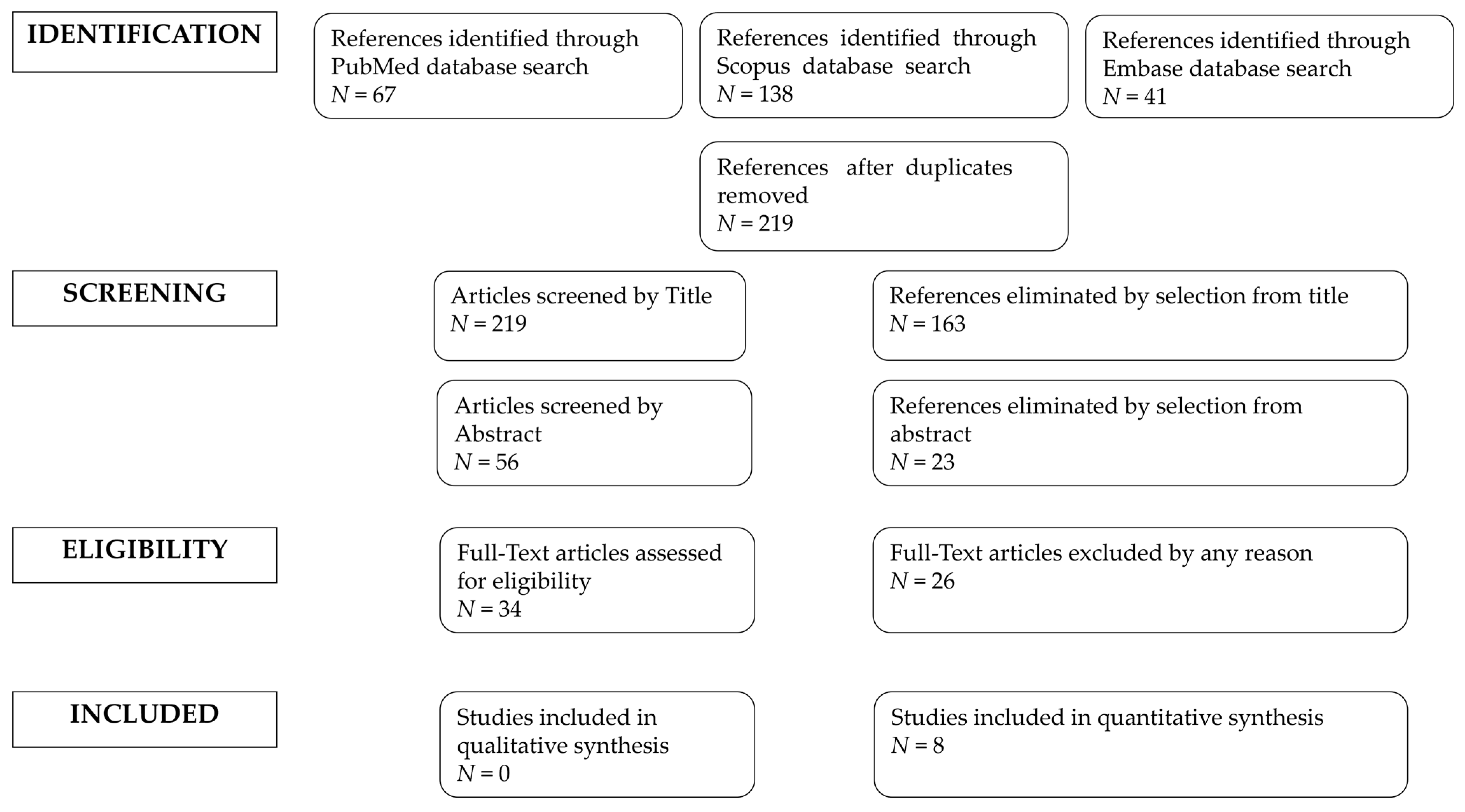
2.1. Search Methods
2.2. Studies Selection
2.3. Quality Assessment
3. Results
3.1. Studies’ Characteristics
3.2. Patients’ Characteristics
3.3. Outcomes
3.4. Direct Comparison with Other Techniques
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Selection | Comparability | Outcome | |||||||
| Cohort Study | Representativeness of exposed cohort | Selection of non-exposed cohort | Ascertainment of exposure | Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts | Assessment Outcome | Follow-Up Long Enough for Outcome to Occur? | Adequacy of Follow-Up | Quality Score |
| Bogliolo, 2014 [15] | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 3 |
| Lopez, 2015 [18] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 6 |
| Jayakumaran, 2017 [20] | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 3 |
| Misal, 2020 [22] | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 5 |
| Selection | Comparability | Exposure | |||||||
| Case-Control Study | Is the case definition adequate? | Representativeness of the cases | Selection of Controls | Definition of Controls | Comparability of cases and controls | Ascertainment of exposure | Same method of ascertainment for cases and controls | Non-Response rate | Quality Score |
| Akdemir, 2015 [16] | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Paek, 2015 [17] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Bogliolo, 2016 [19] | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Chien-Wen, 2019 [21] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
References
- Baskett, T.F. Hysterectomy: Evolution and trends. Best Pract. Res. Clin. Obstet. Gynaecol. 2005, 19, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.; Barlow, D. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2006, 2, CD003677. [Google Scholar]
- Neis, K.J.; Zubke, W.; Römer, T.; Schwerdtfeger, K.; Schollmeyer, T.; Rimbach, S.; Holthaus, B.; Solomayer, E.; Bojahr, B.; Neis, F.; et al. Indications and Route of Hysterectomy for Benign Diseases. Guideline of the DGGG, OEGGG and SGGG (S3 Level, AWMF Registry No. 015/070, April 2015). GebFra 2016, 76, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Albright, B.B.; Witte, T.; Tofte, A.N.; Chou, J.; Black, J.D.; Desai, V.B.; Erekson, E.A. Robotic versus laparoscopic hysterectomy for benign disease: A systematic review and meta-analysis of randomized trials. J. Minim. Invasive Gynecol. 2016, 23, 18–27. [Google Scholar] [CrossRef]
- Warren, L.; Ladapo, J.A.; Borah, B.J.; Gunnarsson, C.L. Open abdominal versus laparoscopic and vaginal hysterectomy: Analysis of a large United States payer measuring quality and cost of care. J. Minim. Invasive Gynecol. 2009, 16, 581–588. [Google Scholar] [CrossRef]
- Corrado, G.; Calagna, G.; Cutillo, G.; Insinga, S.; Mancini, E.; Baiocco, E.; Zampa, A.; Bufalo, A.; Perino, A.; Vizza, E. The patient and observer scar assessment scale to evaluate the cosmetic outcomes of the robotic single-site hysterectomy in endometrial cancer. Int. J. Gynecol. Cancer. 2018, 28, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Fader, A.N.; Cohen, S.; Escobar, P.F.; Gunderson, C. Laparoendoscopic single-site surgery in gynecology. Curr. Opin. Obstet. Gynecol. 2010, 22, 331–338. [Google Scholar] [CrossRef]
- Wilson, G.J. Laparoendoscopic Single Site Hysterectomy: Literature Review and Procedure Description. J. Clin. Med. 2021, 10, 2073. [Google Scholar] [CrossRef]
- Gala, R.B.; Margulies, R.; Steinberg, A.; Murphy, M.; Lukban, J.; Jeppson, P.; Aschkenazi, S.; Olivera, C.; Olivera, M.; Lowenstein, L.; et al. Systematic review of robotic surgery in gynecology: Robotic techniques compared with laparoscopy and laparotomy. J. Minim. Invasive Gynecol. 2014, 21, 353–361. [Google Scholar] [CrossRef]
- Visco, A.G.; Advincula, A.P. Robotic gynecologic surgery. Obstet. Gynecol. 2008, 112, 1369–1384. [Google Scholar] [CrossRef]
- El Hachem, L.; Momeni, M.; Friedman, K.; Moshier, E.L.; Chuang, L.T.; Gretz, H.F., III. Safety, feasibility and learning curve of robotic single-site surgery in gynecology. Int. J. Med. Robot. Comput. Assist. Surg. 2016, 12, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal 8 with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Kansagara, D.; O’Neil, M.; Nugent, S.; Freeman, M.; Low, A.; Kondo, K.; Elven, C.; Zakher, B.; Motu’apuaka, M.; Paynter, R.; et al. Quality Assessment Criteria for Observational Studies, Based on the Newcastle-Ottawa Scale. 2017. Available online: https://www.ncbi.nlm.nih.gov/books/NBK476448/table/appc.t4 (accessed on 27 March 2022).
- Jayakumaran, J.; Wiercinski, K.; Buffington, C.; Caceres, A. Robotic laparoendoscopic single-site benign gynecologic surgery: A single-center experience. J. Robot. Surg. 2017, 12, 447–454. [Google Scholar] [CrossRef]
- Misal, M.; Magtibay, P.M.; Yi, J. Robotic LESS and Reduced-Port Hysterectomy Using the da Vinci SP Surgical System: A Single-Institution Case Series. J. Minim. Invasive Gynecol. 2020, 28, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Bogliolo, S.; Cassani, C.; Babilonti, L.; Gardella, B.; Zanellini, F.; Dominoni, M.; Santamaria, V.; Nappi, R.E.; Spinillo, A. Robotic Single-Site Surgery for Female-to-Male transsexuals: Preliminary Experience. Sci. World J. 2014, 2014, 674579. [Google Scholar] [CrossRef] [PubMed]
- Akdemir, A.; Yildirim, N.; Zeybek, B.; Karaman, S.; Sendag, F. Single incision trans-umbilical total hysterectomy: Robotic or laparoscopic? Gynecol. Obstet. Investig. 2015, 80, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Paek, J.; Lee, J.-D.; Kong, T.W.; Chang, S.-J.; Ryu, H.-S. Robotic single-site versus laparoendoscopic single-site hysterectomy: A propensity score matching study. Surg. Endosc. 2015, 30, 1043–1050. [Google Scholar] [CrossRef]
- Lopez, S.; Mulla, Z.D.; Hernandez, L.; Garza, D.M.; Payne, T.N.; Farnam, R.W. A Comparison of Outcomes Between Robotic-Assisted, Single-Site Laparoscopy Versus Laparoendoscopic Single Site for Benign Hysterectomy. J. Minim. Invasive Gynecol. 2016, 23, 84–88. [Google Scholar] [CrossRef]
- Bogliolo, S.; Ferrero, S.; Cassani, C.; Musacchi, V.; Zanellini, F.; Dominoni, M.; Spinillo, A.; Gardella, B. Single-site Versus Multiport Robotic Hysterectomy in Benign Gynecologic Diseases: A Retrospective Evaluation of Surgical Outcomes and Cost Analysis. J. Minim. Invasive Gynecol. 2016, 23, 603–609. [Google Scholar] [CrossRef]
- Chen, C.-W.; Chang, H.-C.; Huang, T.-F.; Liao, C.-C.; Huang, R.-L.; Lai, H.-C. Transition from multiport to single-site surgery: A single institution experience in robotic supracervical hysterectomy for benign gynecological diseases. Taiwan J. Obs. Gynecol. 2019, 58, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Alletti, S.G.; Restaino, S.; Finelli, A.; Ronsini, C.; Lucidi, A.; Scambia, G.; Fanfani, F. Step by step total laparoscopic hysterectomy with uterine arteries ligation at the origin. J. Minim. Invasive Gynecol. 2019, 27, 22–23. [Google Scholar] [CrossRef] [PubMed]
- Restaino, S.; Ronsini, C.; Finelli, A.; Santarelli, A.; Scambia, G.; Fanfani, F. Laparoscopic Approach for Shull Repair of Pelvic Floor Defects. J. Minim. Invasive Gynecol. 2017, 25, 954. [Google Scholar] [CrossRef] [PubMed]
- Garry, R. Laparoscopic surgery. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 20, 89–104. [Google Scholar] [CrossRef]
- Bartels, H.C.; Rogers, A.C.; Janda, M.; Obermair, A.; Brennan, D.J. Quality of life following minimally invasive hysterectomy compared to abdominal hysterectomy: A metanalysis. Eur. J. Obstet. Gynecol. 2020, 252, 206–212. [Google Scholar] [CrossRef]
- Song, T.; Cho, J.; Kim, T.-J.; Kim, I.-R.; Hahm, T.S.; Kim, B.-G.; Bae, D.-S. Cosmetic Outcomes of Laparoendoscopic Single-Site Hysterectomy Compared With Multi-Port Surgery: Randomized Controlled Trial. J. Minim. Invasive Gynecol. 2013, 20, 460–467. [Google Scholar] [CrossRef]
- Nam, E.J.; Kim, S.W.; Lee, M.; Yim, G.W.; Paek, J.H.; Lee, S.H.; Kim, S.; Kim, J.H.; Kim, J.W.; Kim, Y.T. Robotic single-port transumbilical total hysterectomy: A pilot study. J. Gynecol. Oncol. 2011, 22, 120–126. [Google Scholar] [CrossRef]
- Lee, D.H.; Nam, S.H.; Song, T.; Kim, W.Y.; Lee, K.W.; Kim, K.H. Public perception of ‘scarless’ laparoendoscopic single-site surgery in gynecology. Obstet. Gynecol. Sci. 2015, 58, 289. [Google Scholar] [CrossRef]
- Kane, S.; Stepp, K.J. Laparo-endoscopic single-site surgery hysterectomy using robotic lightweight endoscope assistants. J. Robot. Surg. 2010, 3, 253–255. [Google Scholar] [CrossRef]
- Truong, M.; Kim, J.H.; Scheib, S.; Patzkowsky, K. Advantages of robotics in benign gynecologic surgery. Curr. Opin. Obstet. 2016, 28, 304–310. [Google Scholar] [CrossRef]
- Paraiso, M.F.R.; Ridgeway, B.; Park, A.J.; Jelovsek, J.E.; Barber, M.D.; Falcone, T.; Einarsson, J.I. A randomized trial comparing conventional and robotically assisted total laparoscopic hysterectomy. Am. J. Obstet. Gynecol. 2013, 208, 368.e1–368.e7. [Google Scholar] [CrossRef] [PubMed]
- Sarlos, D.; Kots, L.; Stevanovic, N.; von Felten, S.; Schär, G. Robotic compared with conventional laparoscopic hysterectomy. A randomized controlled trial. Obstet. Gynecol. 2012, 120, 604–611. [Google Scholar] [CrossRef] [PubMed]

| Autor; Year | Country | Study Design | Years Range | N of Participant | Type of Surgery | Type of Robot |
|---|---|---|---|---|---|---|
| S. Bogliolo, 2014 [17] | Italy | Retrospective cohort study, monocentric | April 2013 to December 2013 | 10 | Total hysterectomy + bilateral adnexectomy | da Vinci Si surgical system |
| A. Akdemir, 2015 [18] | Turkey | Retrospective case-control study, monocentric | January 2012 to December 2013 | 24 | Total hysterectomy | da Vinci Si surgical system |
| J. Paek, 2015 [19] | Korea | Retrospective case-control study, monocentric | March 2011 to December 2014 | 25 | Total hysterectomy | da Vinci Si surgical platform |
| S. Lopez, 2015 [20] | USA | Retrospective cohort study, multicentric | 18 March 2013 to 30 December 2013 | 50 | Total hysterectomy | da Vinci surgical system |
| S. Bogliolo, 2016 [21] | Italy | Retrospective case-control study, monocentric | March 2011 to October 2014 | 45 | Total hysterectomy +/− bilateral adnexectomy | da Vinci Si surgical system |
| J. Jayakumaran, 2017 [15] | UK | Retrospective cohort study, monocentric | June 2016 and January 2017 | 24 | Total hysterectomy +/− bilateral adnexectomy | da Vinci Xi robotic system |
| C. Chien-Wen, 2019 [22] | Taiwan | Retrospective case-control study, monocentric | June 2014 to December 2017 | 26 | Subtotal hysterectomy | da Vinci Si surgical system |
| M. Misal, 2020 [16] | USA | Retrospective cohort study, monocentric | December 2019 to March 2020 | 8 | Total or radical hysterectomy | da Vinci SP surgical system |
| Author; Year | Patient n | Median Age, yr (Range) | Median BMI kg/m2 (Range) | Previous Abdominal Surgery, n of pt (%) | Presence of Adhesion, n of pt (%) | Cause of Hysterectomy, n of pt (%) | Uterine Weight, gr (Range) |
|---|---|---|---|---|---|---|---|
| S. Bogliolo, 2014 [17] | 10 | 28 ± 5.7 (20–40) | 22 ± 1.7 (19–25) | 4 (40) | NA | Female-to-male transsexualism 10 (100) | 89 ± 15 (60–120) |
| A. Akdemir, 2015 [18] | 24 | 49.5 (40–61) | 28.5 (21.7–34.2) | 18 (75) | NA | NA | 192.5 (65–520) |
| J. Paek, 2015 [19] | 25 | 48.0 ± 4.1 (NA) | 24.3 ± 2.5 (NA) | 16 (64) | 12 (48) | Leiomyoma: 16 (64); Adenomyosis: 3 (12); CIN: 2 (8); Endometrial hyperplasia: 4 (16) | 271 ± 119 (NA) |
| S. Lopez, 2015 [20] | 50 | 46.0 ± 9.4 (NA) | 25.9 ± 6.1 (NA) | NA | NA | NA | 125.6 ± 68.5 (NA) |
| S. Bogliolo, 2016 [21] | 45 | 46 ± 10.9 (34–64) | 25 ± 5 (18–38) | 38 (84.4) | NA | Uterine myomas adenomyosis genetic risk of cancer * 33 (73.3) 5 (11.1) 4 (8.9) | 137 ± 39 (NA) |
| J. Jayakumaran, 2017 [15] | 24 | 45 (17–70) | 27 (18.4–41.9) | NA | 1 (4.2%) | Pelvic pain 16 (45.7%) Fibroids 11 (31.4%) Adenomyosis 2 (5.7%) Uterine prolapse 2 (5.7%) Bleeding 2 (5.7%) Cervical dysplasia 1 (2.9%) Paratubal/mullerian cyst 1 (2.9%) | 176 (46–532) |
| C. Chien-Wen, 2019 [22] | 26 | 43.9 ± 5.9 (34–60) | 23.0 ± 3.4 (18.0–32.4) | NA | 10 (38.5) | Myoma: 20 (76.9) Adenomyosis: 20 (76.9) | 264.6 ± 140.9 (100–750) |
| M. Misal, 2020 [16] | 8 | 46.3 ± 13.6 (NA) | 27.8 ± 7.5 (22.2–40) | 5 | NA | Leiomyoma: 1; leiomyoma + endometriosis: 1; leiomyoma + paratubal cyst: 1; adenomyosis: 1; adenomyosis + endometriosis: 2; postmenopausal bleeding:2 | 136.1 ± 61.5 (87–246) |
| Author; Year | Median Pre-Surgical Time *, min (Range) | Median Console Time, min (Range) | Median Operative Time, min (Range) | Median Estimated Blood Loss, mL (Range) | Intra-Operative Complications, n (%) | Postoperative Complications (%) | Conversion to Multiport/LPS/LPT | Median Hospital Stay, d ± SD (Range) | Reoperation (%) | Readmission within 30 Days, n |
|---|---|---|---|---|---|---|---|---|---|---|
| S. Bogliolo, 2014 [17] | 9 ± 2 (6–18) § | 79 ± 15 (55–110) | 137 ± 32 (90–210) | 30 ± 24 (15–100) | 0 | 1 (0.1) | 0 | 2.4 ± 0.9 (2–5) | NA | NA |
| A. Akdemir, 2015 [18] | 13.5 (3–11) | 74.5 (60–160) | 98.5 (71–183) | 22.5 (40–61) | 0 | 0 | 0 | 1.6 (1–3) | NA | NA |
| J. Paek, 2015 [19] | 14.0 ± 4.7 | 99.6 ± 49.7 | 170.9 ± 65.5 | 20 (30) | 0 | 0 | NA | 3.5 ± 0.7 | NA | NA |
| S. Lopez, 2015 [20] | NA | NA | 139.3 ± 45.8 | 37.2 ± 30.7 | 1 (2) | NA | 8 (16.0) | 0.96 ± 0.3 (NA) | NA | NA |
| S. Bogliolo, 2016 [21] | 17 ± 6 (7–30) § | 115 ± 26 (NA) | 144 ± 41 (82–265) | 46 ± 52 (10–200) | 0 | 1 (2.2%) | 0 | 1.5 ± 1 (NA) | NA | NA |
| J. Jayakumaran, 2017 [15] | 19 (4–47) | 41 (25–120) | 132 (60–294) | 75 (20–300) | 1 | NA | 2 | 0.96 (0.96–5) | NA | NA |
| C. Chien-Wen, 2019 [22] | 15.8 ± 5.5 (9–28) § | 61.1 ± 35.6 (25–180) | 140.3 ± 34.4 (63–205) | 71.2 ± 40.4 (50–200) | 0 | NA | 0 | 2.4 ± 0.7 (1–4) | NA | 0 |
| M. Misal, 2020 [16] | NA | NA | 86.5 ± 27.1 (60–132) | NA (20–100) | 0 | 1 | 0 | NA | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riemma, G.; Pasanisi, F.; Reino, A.; Solazzo, M.C.; Ronsini, C. Robotic Single-Site Hysterectomy in Gynecologic Benign Pathology: A Systematic Review of the Literature. Medicina 2023, 59, 411. https://doi.org/10.3390/medicina59020411
Riemma G, Pasanisi F, Reino A, Solazzo MC, Ronsini C. Robotic Single-Site Hysterectomy in Gynecologic Benign Pathology: A Systematic Review of the Literature. Medicina. 2023; 59(2):411. https://doi.org/10.3390/medicina59020411
Chicago/Turabian StyleRiemma, Gaetano, Francesca Pasanisi, Antonella Reino, Maria Cristina Solazzo, and Carlo Ronsini. 2023. "Robotic Single-Site Hysterectomy in Gynecologic Benign Pathology: A Systematic Review of the Literature" Medicina 59, no. 2: 411. https://doi.org/10.3390/medicina59020411
APA StyleRiemma, G., Pasanisi, F., Reino, A., Solazzo, M. C., & Ronsini, C. (2023). Robotic Single-Site Hysterectomy in Gynecologic Benign Pathology: A Systematic Review of the Literature. Medicina, 59(2), 411. https://doi.org/10.3390/medicina59020411