
The Problem of Antimalarial-Drug Abuse by the Inhabitants of Ghana
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
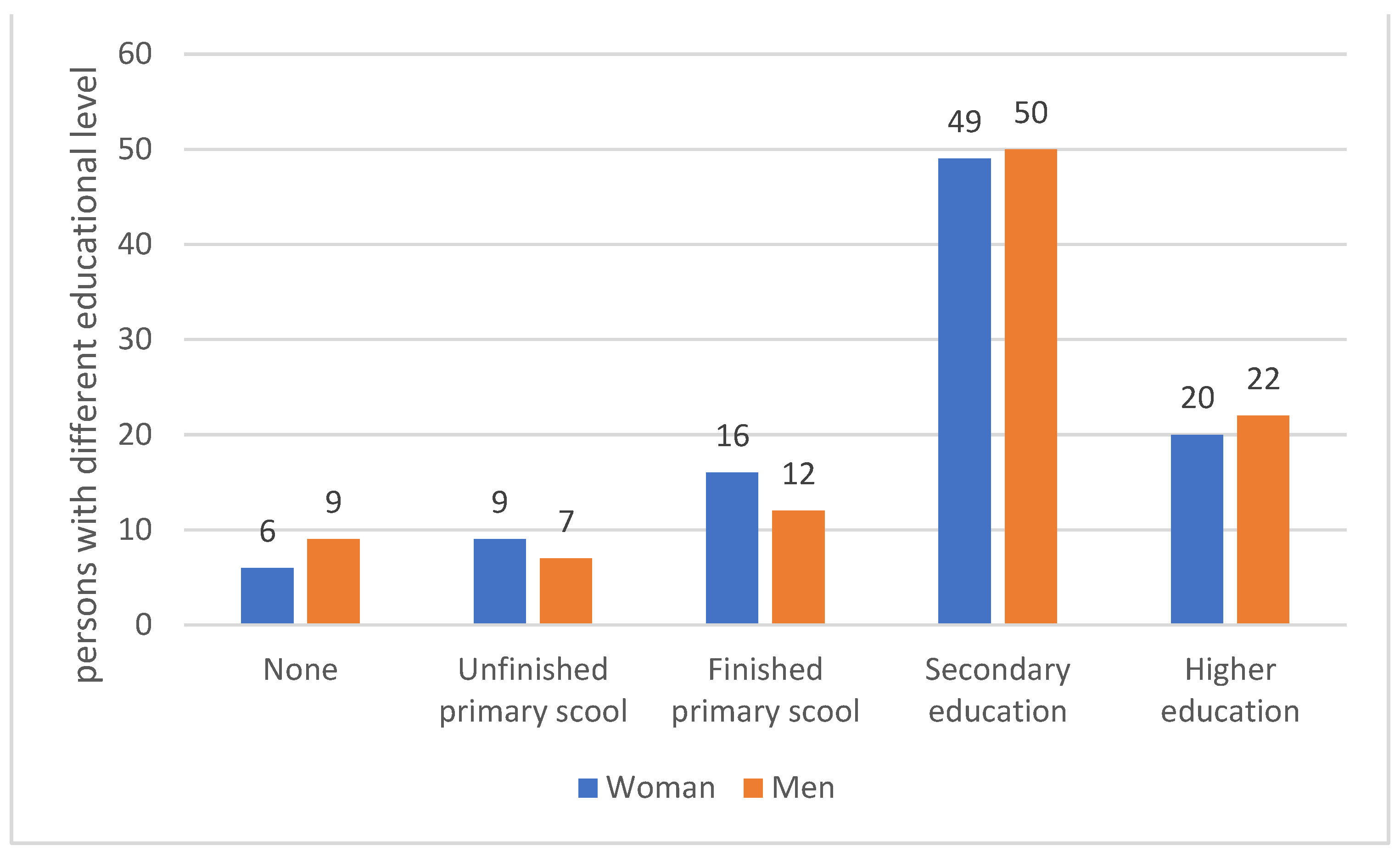
- The distribution of respondents by sex and age groups.
- Contact with malaria among family members.
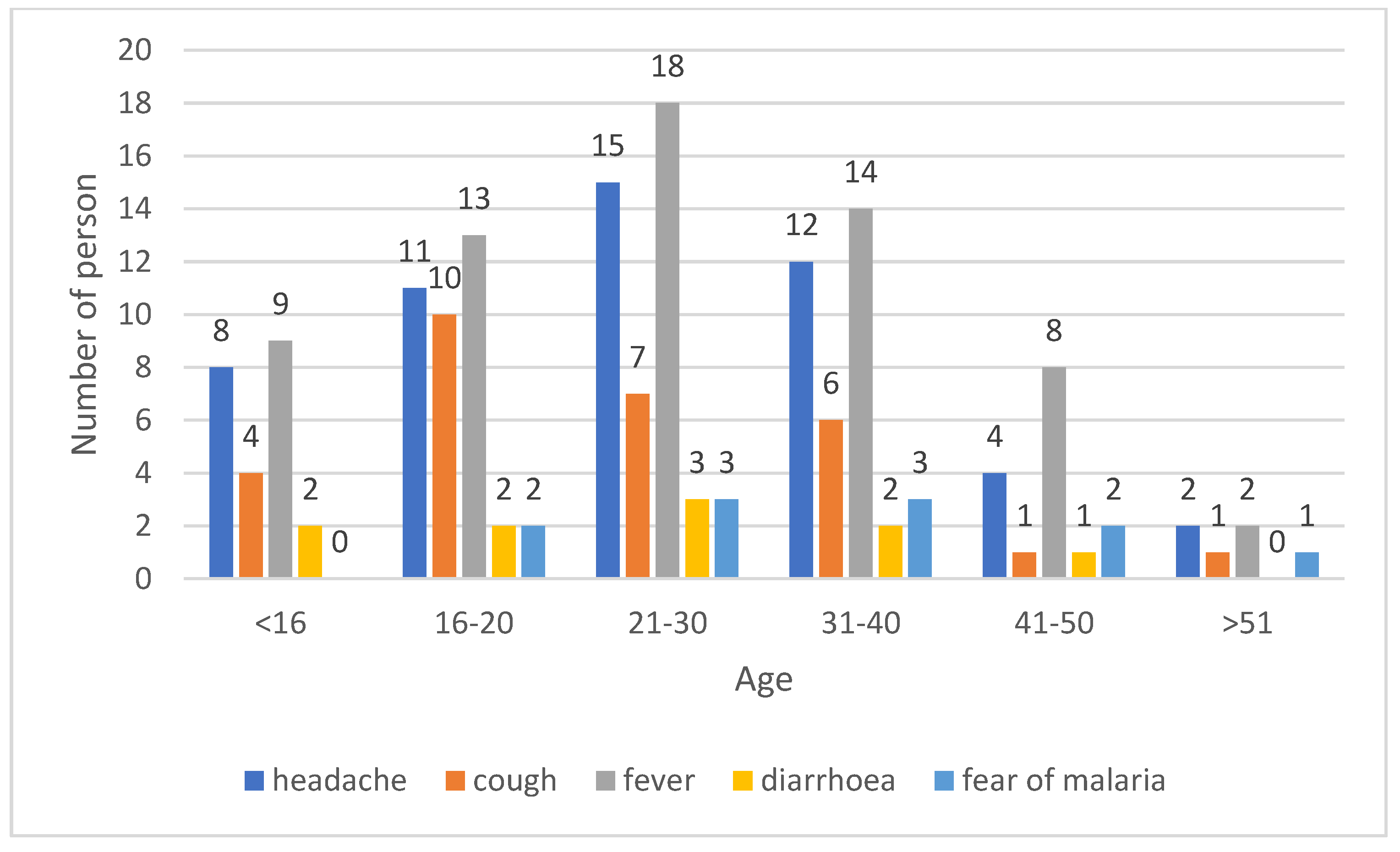
- Knowledge of malaria symptoms.
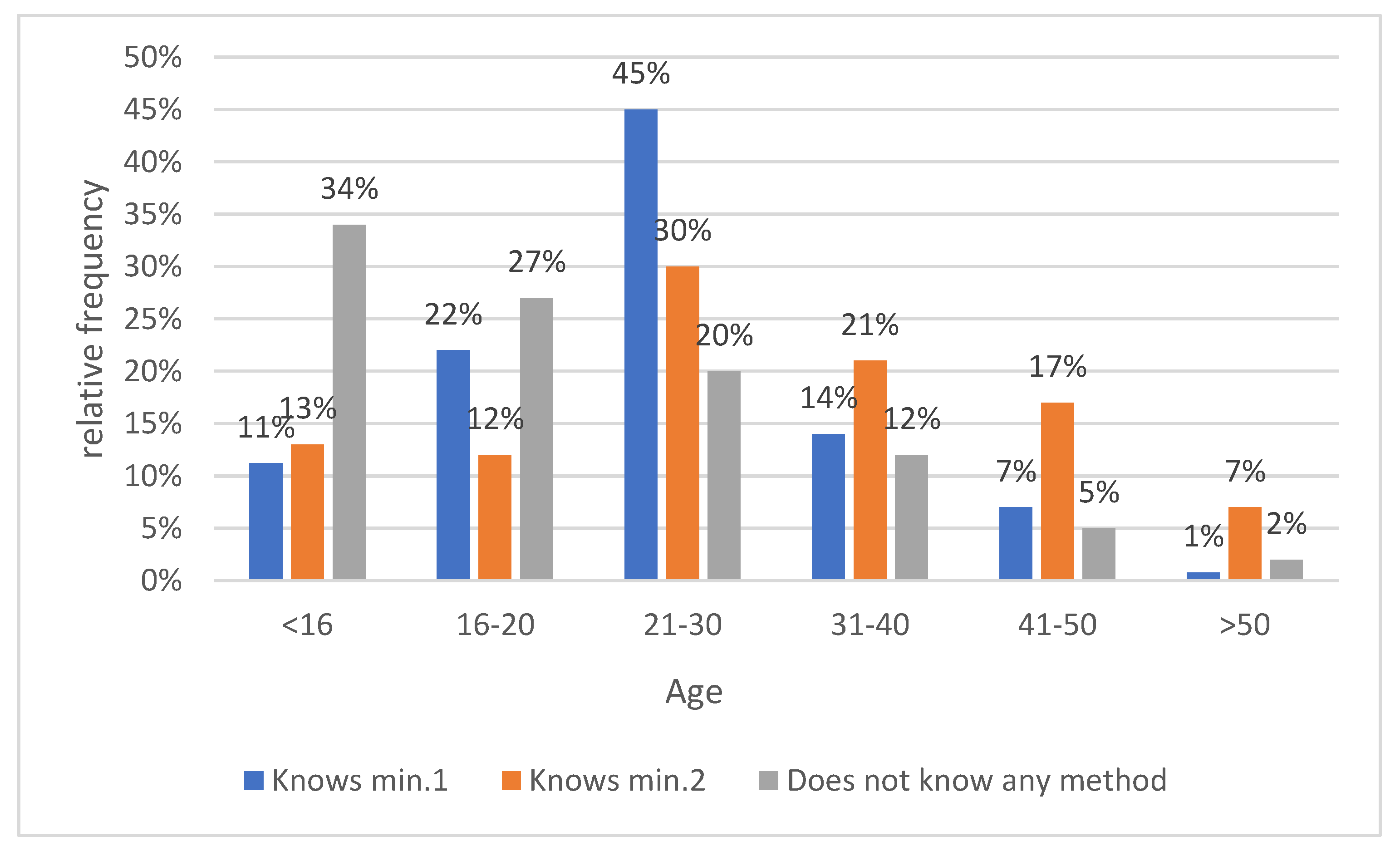
- Knowledge of the cause of malaria by age.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Distribution of People by Sex in Age Groups | Contact with Malaria among Family Members | Knowledge of Malaria Symptoms | Knowledge of the Cause of Malaria by Age | ||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Yes | No | Yes | No | Yes | No | |
| <16 | 12 | 28 | 37 | 3 | 31 | 9 | 11 | 29 |
| 16–20 | 18 | 31 | 45 | 4 | 44 | 5 | 31 | 18 |
| 21–30 | 39 | 49 | 81 | 7 | 82 | 6 | 49 | 39 |
| 31–40 | 28 | 17 | 42 | 3 | 39 | 6 | 31 | 14 |
| 41–50 | 8 | 11 | 14 | 5 | 13 | 6 | 15 | 4 |
| >51 | 3 | 4 | 6 | 1 | 5 | 2 | 5 | 2 |
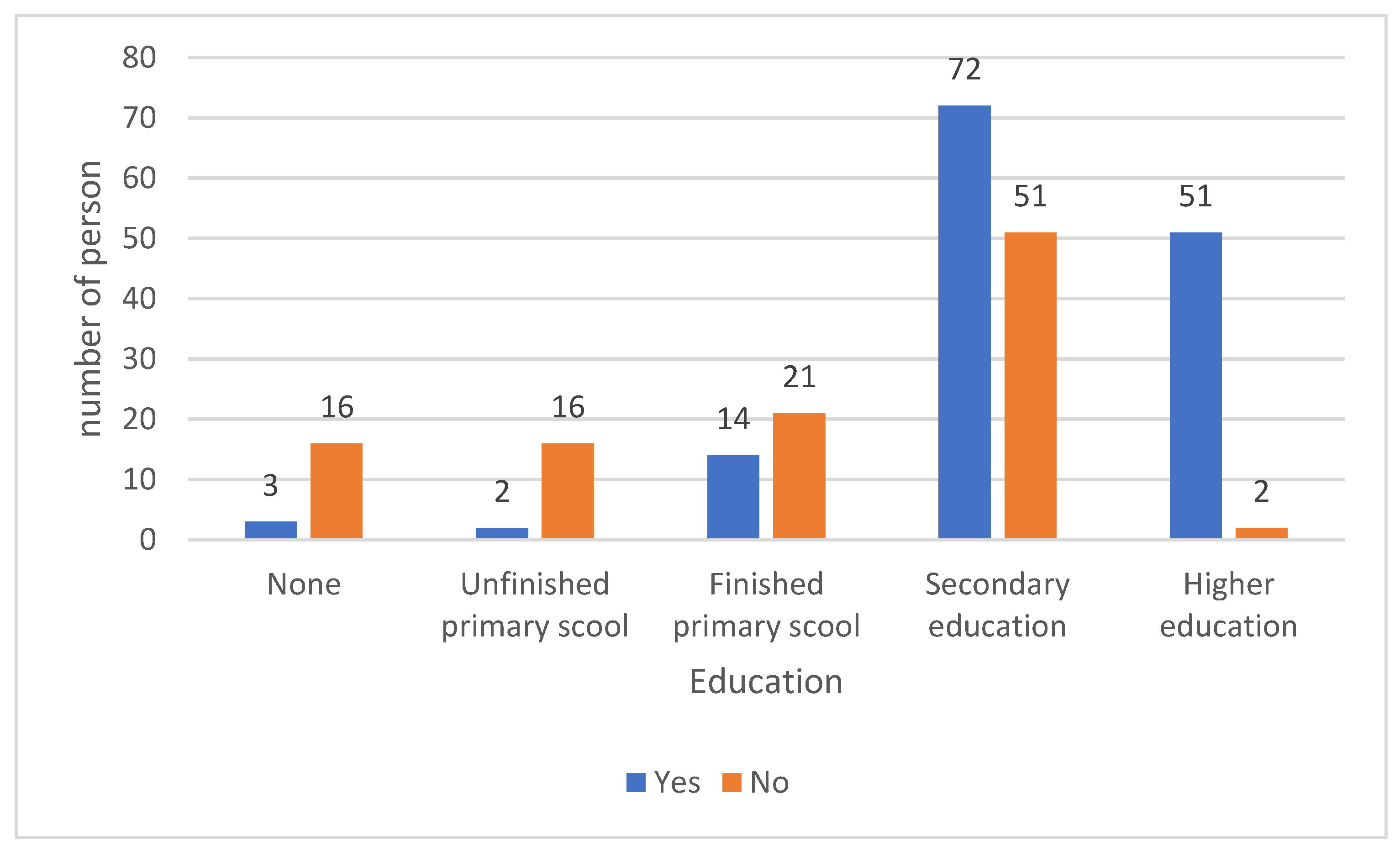
- Knowledge of how to purchase and perform a rapid diagnostic test for malaria (before using the drug without consulting medical staff).
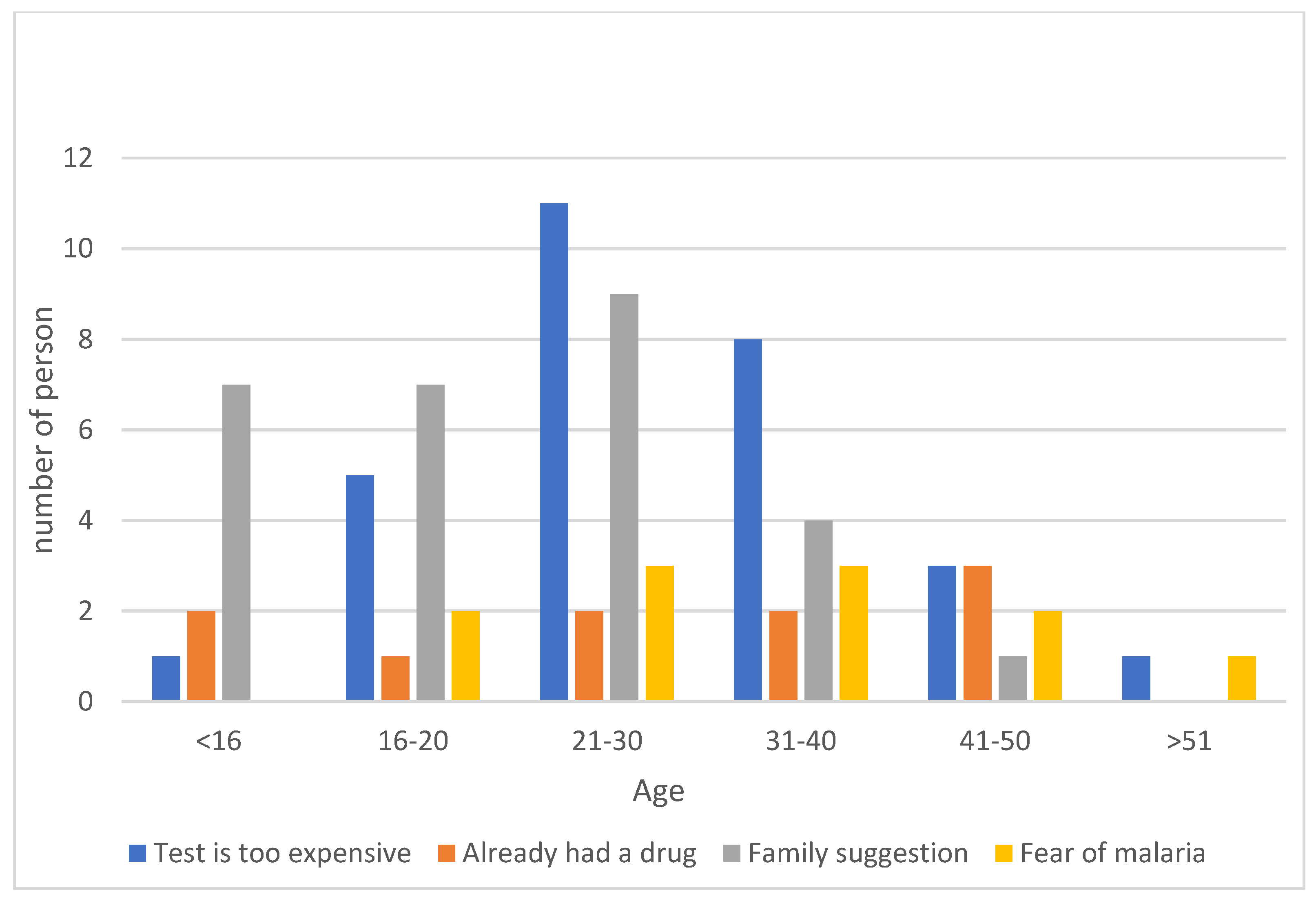
- Performing a rapid diagnostic test for malaria before purchasing antimalarial drugs.
| Age Group | Knows about the Possibility to a Purchase Rapid Test for Malaria | Did the Respondents Take a Rapid Test for Malaria before Purchasing Antimalarial Drugs? | ||
|---|---|---|---|---|
| Yes | No | Yes | No | |
| <16 | 2 | 7 | 1 | 15 |
| 16–20 | 6 | 5 | 2 | 9 |
| 21–30 | 11 | 6 | 2 | 9 |
| 31–40 | 9 | 7 | 3 | 12 |
| 41–50 | 5 | 3 | 1 | 7 |
| >51 | 1 | 1 | 0 | 2 |
4. Discussion
4.1. Knowledge of Malaria Symptoms
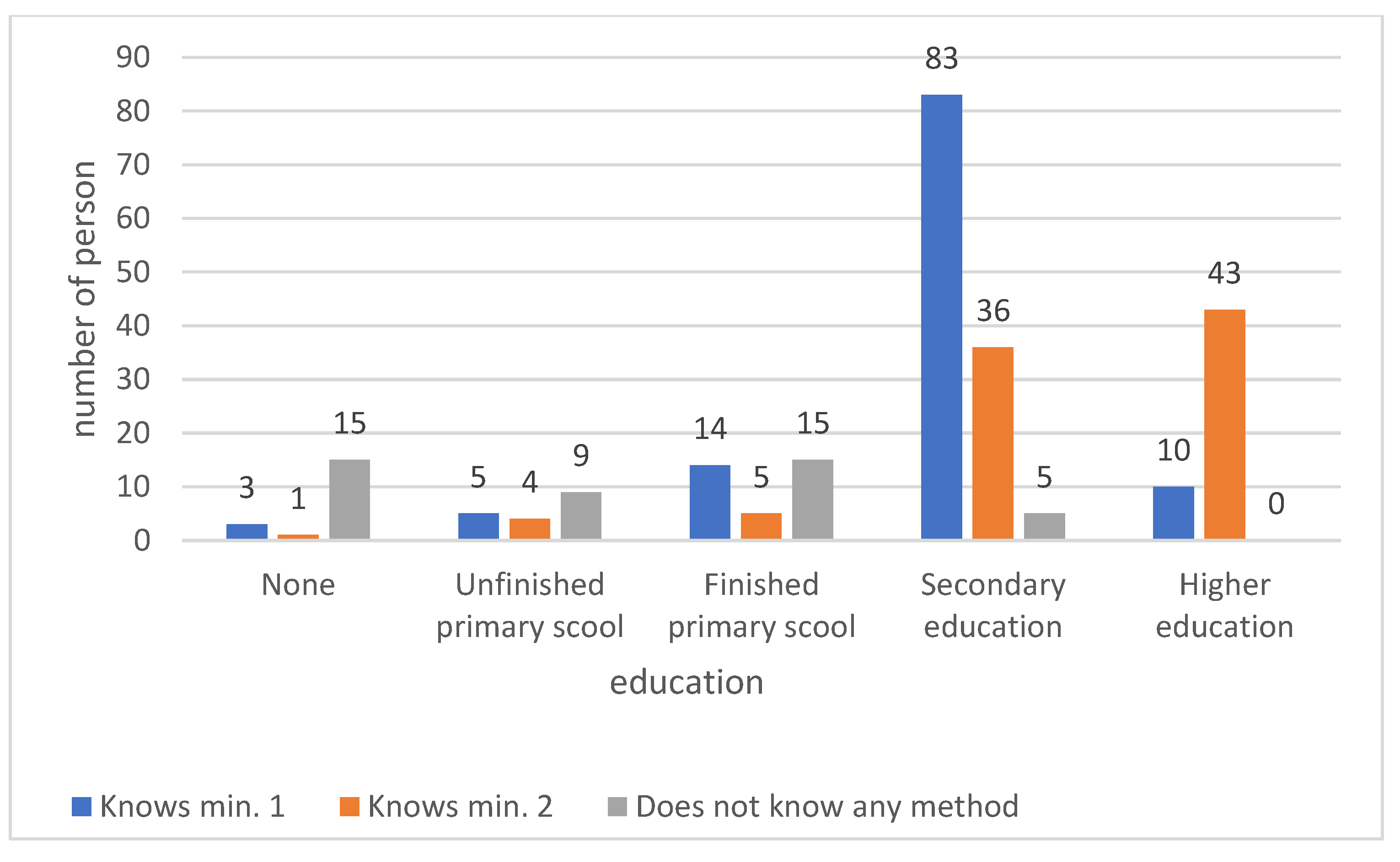
4.2. Knowledge of the Cause of Malaria
4.3. Knowledge of Malaria Prevention
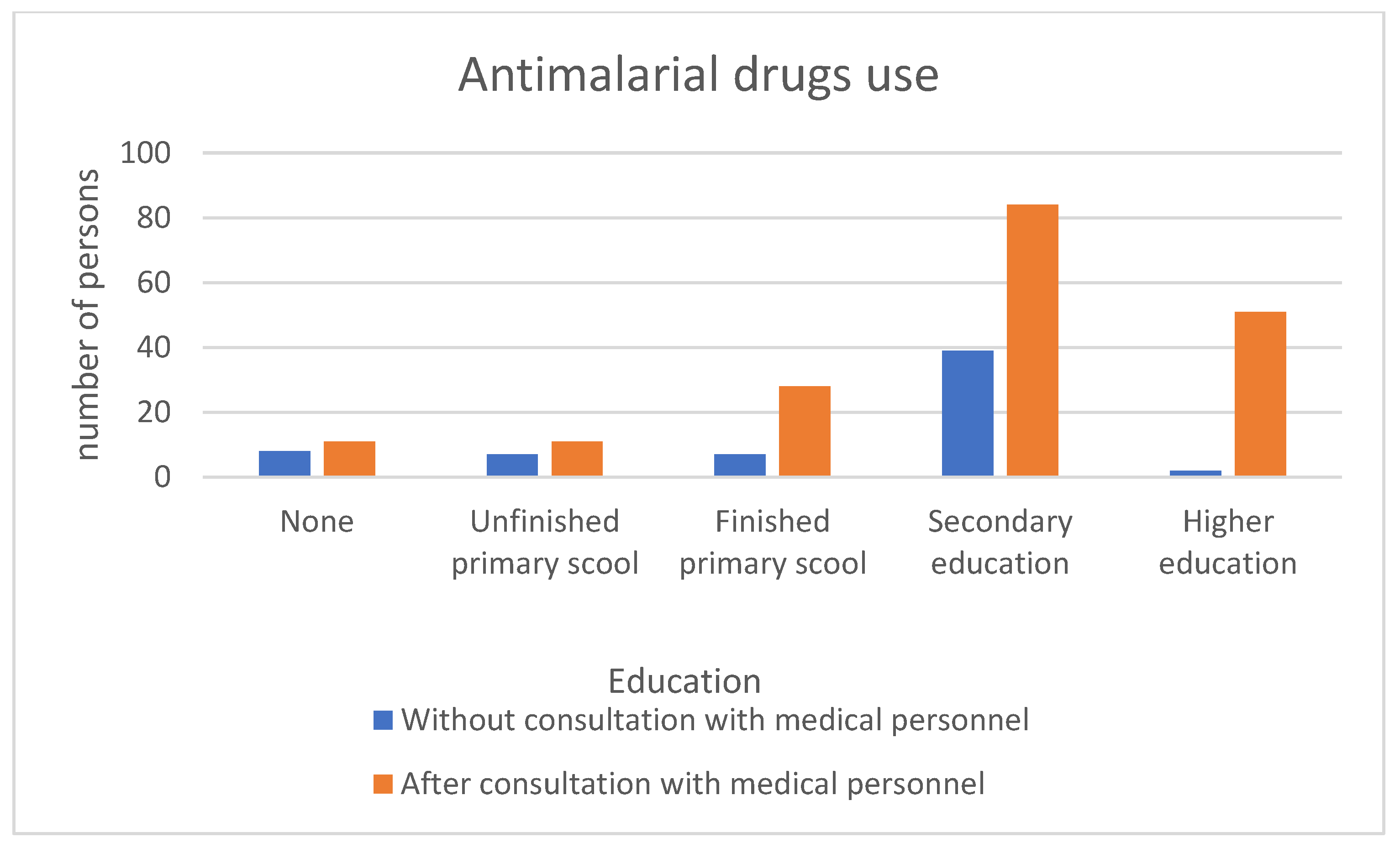
4.4. Consultation with Medical Personnel before Taking Antimalarial Drugs
4.5. Rapid Diagnostic Tests for Malaria
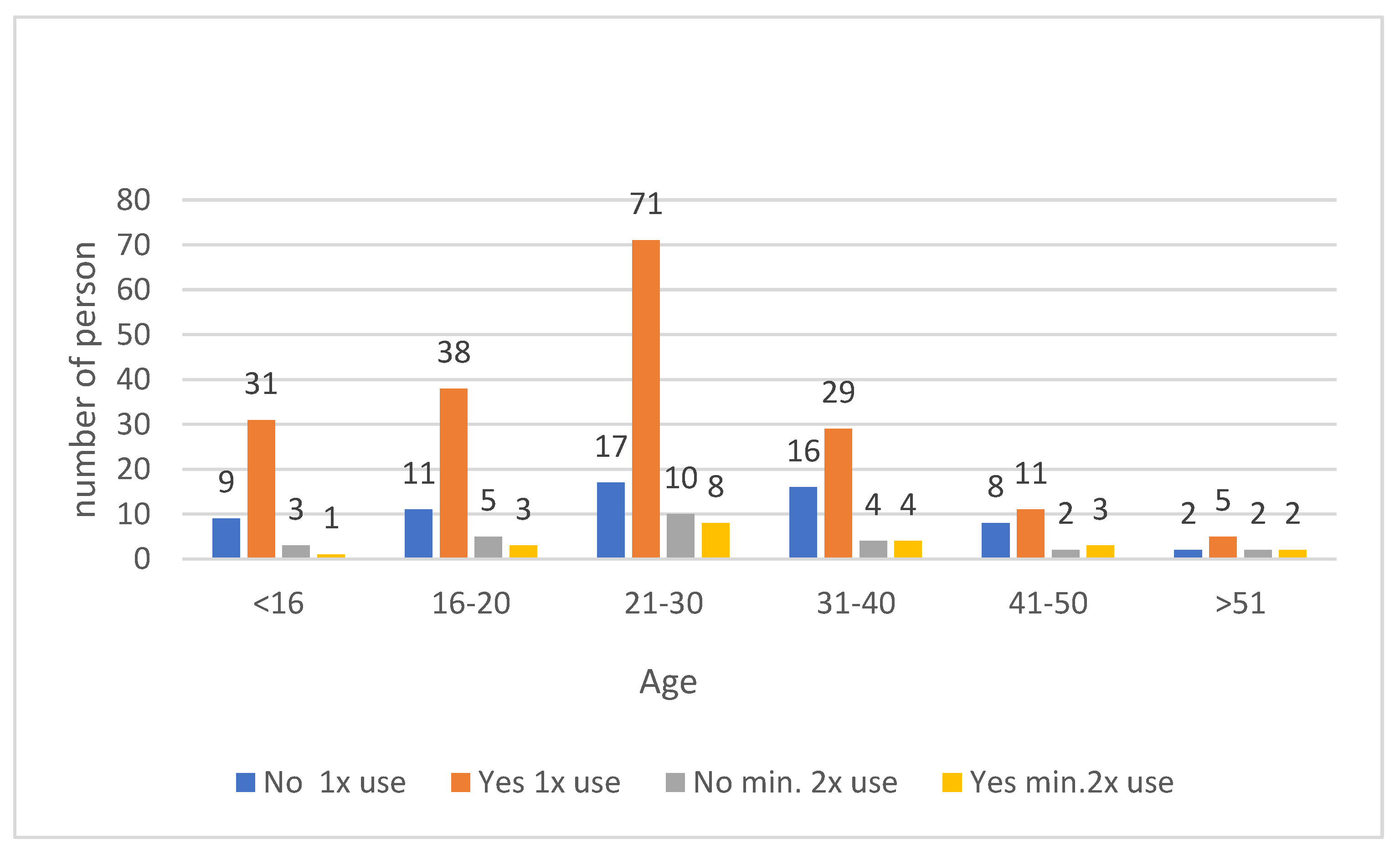
4.6. Appropriate Use of Antimalarial Drugs
5. Conclusions
- (1)
- Awareness among the people of Accra and Yendi about the causes, symptoms, and prevention of malaria is quite high.
- (2)
- Public education and awareness, as well as accessibility to places where antimalarial drugs are sold, play a very important role in the proper use of antimalarial drugs.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Malaria Report 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Website of World Bank. Available online: www.data.worldbank.org (accessed on 4 May 2021).
- Website of Centers for Disease Control and Prevention. Available online: www.cdc.gov (accessed on 4 May 2021).
- World Health Organization. WHO Briefing on Malaria Treatment Guidelines and Artemisinin Monotherapies; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Guidelines for Case Management of Malaria in Ghana. 2014. Available online: https://www.severemalaria.org/sites/mmv-smo/files/content/attachments/2017-03-09/Ghana%20GUIDELINE%20FOR%20CASE%20MANAGEMENT%20.pdf (accessed on 4 May 2021).
- Goodman, C.; Brieger, W.; Unwin, A.; Mills, A.; Meek, S.; Greer, G. Medicine sellers and malaria treatment in sub-Saharan Africa: What do they do and how can their practice be improved? Am. J. Trop. Med. Hyg. 2007, 77 (Suppl. 6), 203. [Google Scholar] [CrossRef] [PubMed]
- Malm, K.L.; Segbaya, S.; Forson, I.; Gakpey, K.D.; Sampong, L.B.; Adjei, E.A.; Bart-Plange, C. Implementation of the Affordable Medicines for Malaria Facility (AMFm) in Ghana: Processes, challenges and achievements. J. Public Health Policy 2013, 34, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Ndeffo Mbah, M.L.; Parikh, S.; Galvani, A.P. Comparing the impact of artemisinin-based combination therapies on malaria transmission in sub-Saharan Africa. Am. J. Trop. Med. Hyg. 2015, 92, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Tun, K.M.; Imwong, M.; Lwin, K.M.; Win, A.A.; Hlaing, T.M.; Hlaing, T.; Lin, K.; Kyaw, M.P.; Plewes, K.; Faiz, M.A.; et al. Spread of artemisinin-resistant Plasmodium falciparum in Myanmar: A cross-sectional survey of the K13 molecular marker. Lancet Infect. Dis. 2015, 15, 415–421. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for the treatment of malaria Third edition. Trans. R. Soc. Trop. Med. Hyg. 2015, 85–88. [Google Scholar]
- Baiden, F.; Malm, K.; Bart-Plange, C.; Hodgson, A.; Chandramohan, D.; Webster, J.; Owusu-Agyei, S. Shifting from presumptive to test-based management of malaria—Technical basis and implications for malaria control in Ghana. Ghana Med. J. 2014, 48, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Ghana, R.O. Anti-Malaria Drug Policy for Ghana. 2009; Volume 17. Available online: https://www.moh.gov.gh/wp-content/uploads/2016/02/ANTI-MALARIA-DRUG-POLICY.pdf (accessed on 15 September 2022).
- FAO. T3: Test. Treat. Track. In Scaling Up Diagnostic Testing, Treatment and Surveillance for Malaria; FAO: Geneva, Switzerland, 2012. [Google Scholar]
- Amponsah, A.O.; Vosper, H.; Marfo, A.F.A. Patient related factors affecting adherence to antimalarial medication in an urban estate in ghana. Malar. Res. Treat. 2015, 2015, 452539. [Google Scholar] [CrossRef] [PubMed]
- Buabeng, K.O.; Duwiejua, M.; Dodoo, A.N.O.; Matowe, L.K.; Enlund, H. Self-reported use of anti-malarial drugs and health facility management of malaria in Ghana. Malar. J. 2007, 6, 85. [Google Scholar] [CrossRef] [PubMed]
- Aborah, S.; Akweongo, P.; Adjuik, M.; Atinga, R.A.; Welaga, P.; Adongo, P.B. The use of non-prescribed anti-malarial drugs for the treatment of malaria in the Bolgatanga municipality, northern Ghana. Malar. J. 2013, 12, 266. [Google Scholar] [CrossRef] [PubMed]
- Diema Konlan, K.; Amu, H.; Konlan, K.D.; Japiong, M. Awareness and malaria prevention practices in a rural community in the Ho Municipality, Ghana. Interdiscip. Perspect. Infect. Dis. 2019, 2019, 9365823. [Google Scholar] [CrossRef] [PubMed]
- Ayi, I.; Nonaka, D.; Adjovu, J.K.; Hanafusa, S.; Jimba, M.; Bosompem, K.M.; Mizoue, T.; Takeuchi, T.; Al Boakye, D.; Kobayashi, J. School-based participatory health education for malaria control in Ghana: Engaging children as health messengers. Malar. J. 2010, 9, 98. [Google Scholar] [CrossRef] [PubMed]
- Azabre, B.A.; Teye, J.K.; Yaro, J.K. Malaria control strategies in the Kassena-Nankana East and West Districts of Ghana. Ghana J. Geogr. 2013, 5, 102–120. [Google Scholar]
- van der Wielen, N.; Channon, A.A.; Falkingham, J. Universal health coverage in the context of population ageing: What determines health insurance enrolment in rural Ghana? BMC Public Health 2018, 18, 657. [Google Scholar] [CrossRef] [PubMed]
- Website of Transformative Education for Health Professionals. Available online: www.whoeducationguidelines.org (accessed on 15 September 2022).
- Ghana National Health Insurance Authority. Annu. Rep. 2012, 1–41.
- Williams, H.A.; Jones, C.O.H. A critical review of behavioral issues related to malaria control in sub-Saharan Africa: What contributions have social scientists made? Soc. Sci. Med. 2004, 59, 501–523. [Google Scholar] [CrossRef] [PubMed]
- Yeboah, P.; Forkuo, A.D.; Amponsah, O.K.O.; Adomako, N.O.; Abdin, A.Y.; Nasim, M.J.; Werner, P.; Panyin, A.B.; Emrich, E.; Jacob, C. Antimalarial Drugs in Ghana: A Case Study on Personal Preferences. Science 2020, 2, 49. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zieliński, E.; Kowalczyk, M.; Osowiecka, K.; Klepacki, Ł.; Dyśko, Ł.; Wojtysiak, K. The Problem of Antimalarial-Drug Abuse by the Inhabitants of Ghana. Medicina 2023, 59, 257. https://doi.org/10.3390/medicina59020257
Zieliński E, Kowalczyk M, Osowiecka K, Klepacki Ł, Dyśko Ł, Wojtysiak K. The Problem of Antimalarial-Drug Abuse by the Inhabitants of Ghana. Medicina. 2023; 59(2):257. https://doi.org/10.3390/medicina59020257
Chicago/Turabian StyleZieliński, Ewa, Marek Kowalczyk, Karolina Osowiecka, Łukasz Klepacki, Łukasz Dyśko, and Katarzyna Wojtysiak. 2023. "The Problem of Antimalarial-Drug Abuse by the Inhabitants of Ghana" Medicina 59, no. 2: 257. https://doi.org/10.3390/medicina59020257
APA StyleZieliński, E., Kowalczyk, M., Osowiecka, K., Klepacki, Ł., Dyśko, Ł., & Wojtysiak, K. (2023). The Problem of Antimalarial-Drug Abuse by the Inhabitants of Ghana. Medicina, 59(2), 257. https://doi.org/10.3390/medicina59020257