
Imaging Modalities for Evaluating Lymphedema

Abstract
:1. Introduction
- Objective measurements [5]: limb volume measurement by perometry/CT/water dis-placement, skin tonometry, bioimpedance spectroscopy (BIS, L-dex score), bioimpedance analysis (BIA), and tissue dielectric constant (TDC);
- Imaging modalities (see Section 2);
- Self-assessment questionnaires: lymphedema life impact scale (LLIS) [8], lower limb functional index (LLFI) [9], lower extremity functional scale (LEFS) [10], disabilities of the arm, shoulder, and hand (DASH) [11], International Classification of Functioning, Disability and Health (ICF) [12], and general quality of life (QoL) [5,7,13,14].
2. Imaging Modalities
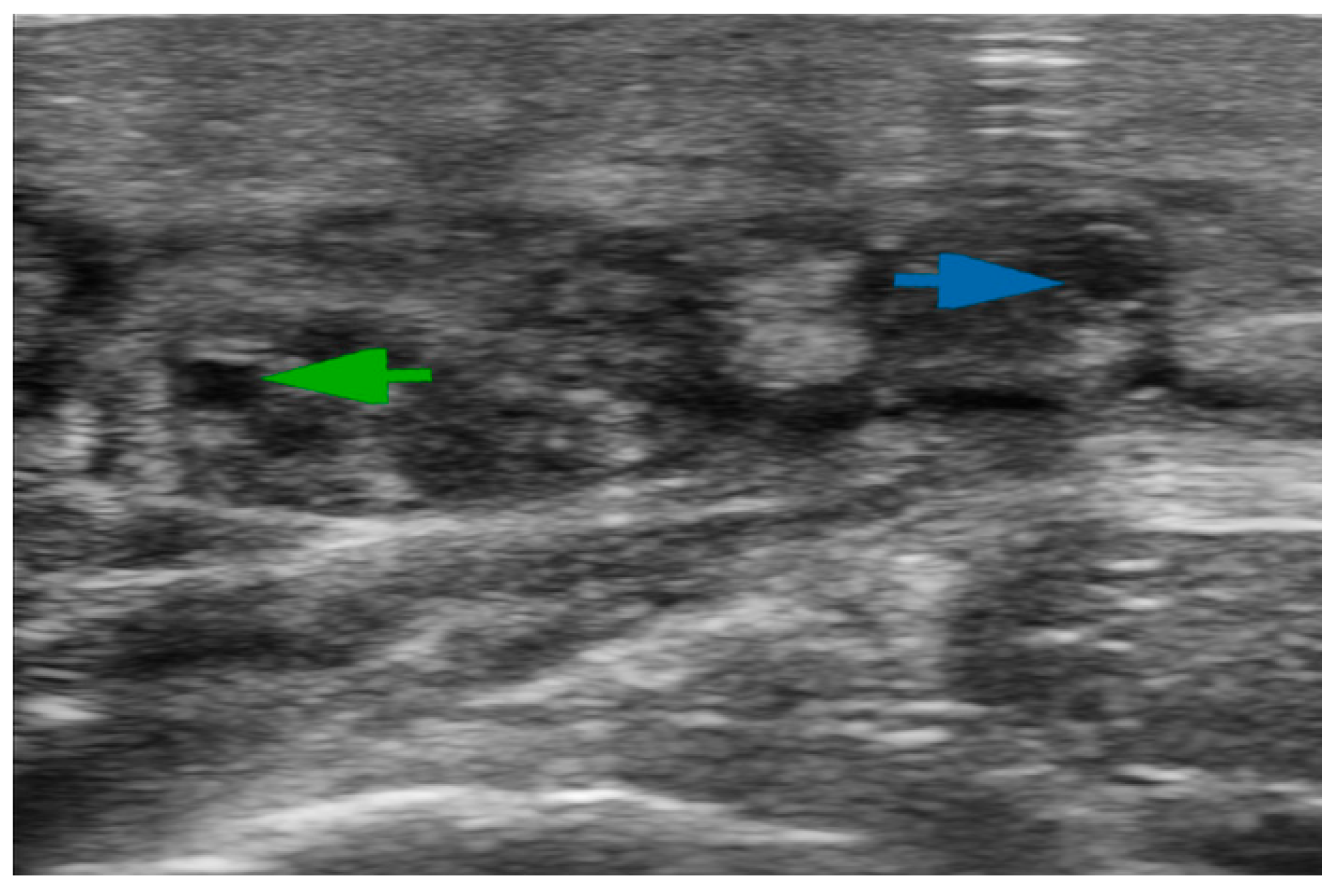
2.1. Ultrasonography (US)
2.2. Lymphoscintigraphy (LS)
2.3. Indocyanine Green Lymphography (ICG-L)
2.4. Magnetic Resonance Imaging Lymphography (MRL)
2.5. Computed Tomography (CT)
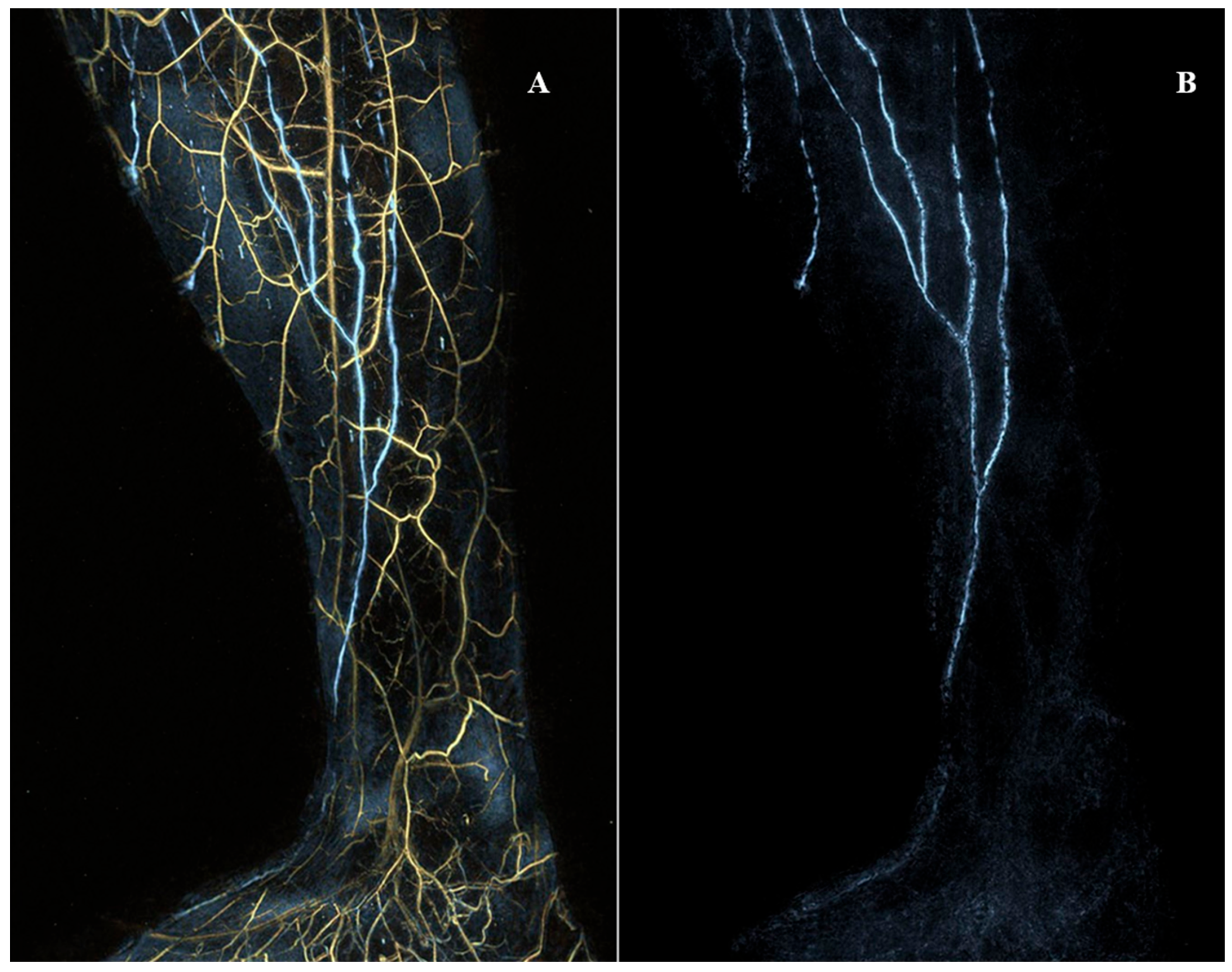
2.6. Photoacoustic Imaging (PAI)
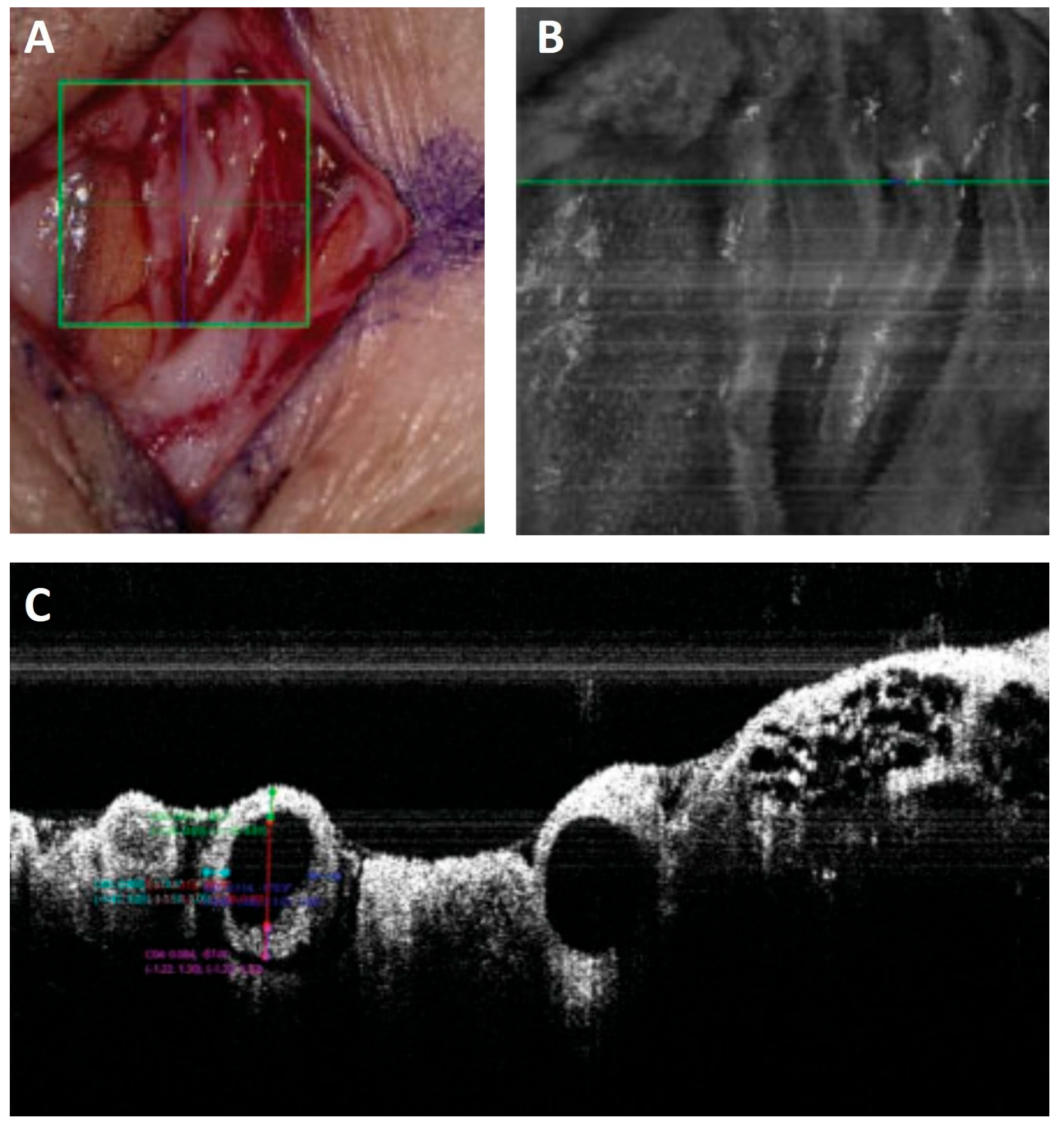
2.7. Optical Coherence Tomography (OCT)
2.8. Tracer Design and Delivery
3. An Imaging-Based Lymphedema Treatment Protocol
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ISL Stage | Clinical Signs or Symptoms |
|---|---|
| Stage 0 | No visible swelling. The patient reports sensations associated with swelling, for example, heaviness, tightness, and aching |
| Stage I | Intermittent swelling that resolves overnight or with elevation. Minimal or no pitting. |
| Stage IIa | Visible swelling. Significant pitting. Elevation rarely resolves swelling. |
| Stage IIb | Visible swelling. Tissue firmness is evident in the swollen area. Minimal or no pitting. |
| Stage III | Large, distorted swollen area. No pitting. Very hard skin and tissue, with skin changes including extra folds, discoloration, overgrowths, and lymphorrhea. |
| Level of Severity. | Increase in Limb Volume (%) |
|---|---|
| minimal | 5–10% |
| mild | 10–20% |
| moderate | 20–40% |
| severe | 40% |
References
- Finnane, A.; Hayes, S.C.; Obermair, A.; Janda, M. Quality of Life of Women with Lower-Limb Lymphedema Following Gynecological Cancer. Expert. Rev. Pharm. Outcomes Res. 2011, 11, 287–297. [Google Scholar] [CrossRef]
- Szuba, A.; Rockson, S.G. Lymphedema: Classification, Diagnosis and Therapy. Vasc. Med. 1998, 3, 145–156. [Google Scholar] [CrossRef]
- Partsch, H. Assessment of Abnormal Lymph Drainage for the Diagnosis of Lymphedema by Isotopic Lymphangiography and by Indirect Lymphography. Clin. Dermatol. 1995, 13, 445–450. [Google Scholar] [CrossRef]
- Cemal, Y.; Pusic, A.; Mehrara, B.J. Preventative Measures for Lymphedema: Separating Fact from Fiction. J. Am. Coll. Surg. 2011, 213, 543–551. [Google Scholar] [CrossRef]
- Executive Committee of the International Society of Lymphology. The Diagnosis and Treatment of Peripheral Lymphedema: 2020 Consensus Document of the International Society of Lymphology. Lymphology 2020, 53, 3–19. [Google Scholar]
- Chachaj, A.; Piller, N.; Boccardo, F.; Szuba, A. Lymphedema: General Pathophysiology, Prevention, and Management in Invasive Cancer BT—Cancer Metastasis Through the Lymphovascular System; Leong, S.P., Nathanson, S.D., Zager, J.S., Eds.; Springer International Publishing: Cham, Germany, 2022; pp. 261–271. ISBN 978-3-030-93084-4. [Google Scholar]
- Lee, T.S.; Morris, C.M.; Czerniec, S.A.; Mangion, A.J. Does Lymphedema Severity Affect Quality of Life? Simple Question. Challenging Answers. Lymphat. Res. Biol. 2018, 16, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Weiss, J.; Daniel, T. Validation of the lymphedema life impact scale (LLIS): A condition-specific measurement tool for persons with lymphedema. Lymphology 2015, 48, 128–138. [Google Scholar] [PubMed]
- Gabel, C.P.; Melloh, M.; Burkett, B.; Michener, L.A. Lower Limb Functional Index: Development and Clinimetric Properties. Phys. Ther. 2012, 92, 98–110. [Google Scholar] [CrossRef]
- Binkley, J.M.; Stratford, P.W.; Lott, S.A.; Riddle, D.L. The Lower Extremity Functional Scale (LEFS): Scale Development, Measurement Properties, and Clinical Application. North American Orthopaedic Rehabilitation Research Network. Phys. Ther. 1999, 79, 371–383. [Google Scholar]
- Angst, F. Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH). In Encyclopedia of Quality of Life and Well-Being Research; Springer: Berlin/Heidelberg, Germany, 2014; pp. 1635–1646. [Google Scholar] [CrossRef]
- Stucki, G.; Maksimović, M.; Davidović, D.; Jorga, J. International Classification of Functioning, Disability and Health. Srp. Arh. Celok. Lek. 2007, 135, 371–375. [Google Scholar] [CrossRef]
- Nakane, Y.; Tazaki, M.; Miyaoka, E. WHOQOL User Manual. Iryo Shakai 1999, 9, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Garza, R.M.; Ooi, A.S.H.; Falk, J.; Chang, D.W. The Relationship between Clinical and Indocyanine Green Staging in Lymphedema. Lymphat. Res. Biol. 2019, 17, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Feldman, J.L.; Stout, N.L.; Wanchai, A.; Stewart, B.R.; Cormier, J.N.; Armer, J.M. Intermittent Pneumatic Compression Therapy: A Systematic Review. Lymphology 2012, 45, 13–25. [Google Scholar] [PubMed]
- Mosti, G.; Cavezzi, A. Compression Therapy in Lymphedema: Between Past and Recent Scientific Data. Phlebology 2019, 34, 515–522. [Google Scholar] [CrossRef]
- Liu, N.F.; Olszewski, W. The Influence of Local Hyperthermia on Lymphedema and Lymphedematous Skin of the Human Leg. Lymphology 1993, 26, 28–37. [Google Scholar]
- Chang, T.S.; Gan, J.L.; Fu, K.D.; Huang, W.Y. The Use of 5,6 Benzo-[Alpha]-Pyrone (Coumarin) and Heating by Microwaves in the Treatment of Chronic Lymphedema of the Legs. Lymphology 1996, 29, 106–111. [Google Scholar]
- Joos, E.; Vultureanu, I.; Nonneman, T.; Adriaenssens, N.; Hamdi, M.; Zeltzer, A. Low-Energy Extracorporeal Shockwave Therapy as a Therapeutic Option for Patients with a Secondary Late-Stage Fibro-Lymphedema after Breast Cancer Therapy: A Pilot Study. Lymphat. Res. Biol. 2021, 19, 175–180. [Google Scholar] [CrossRef]
- Pak, C.S.; Suh, H.P.; Kwon, J.G.; Cho, M.-J.; Hong, J.P. Lymph Node to Vein Anastomosis (LNVA) for Lower Extremity Lymphedema. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 2059–2067. [Google Scholar] [CrossRef]
- Campisi, C.; Bellini, C.; Campisi, C.; Accogli, S.; Bonioli, E.; Boccardo, F. Microsurgery for Lymphedema: Clinical Research and Long-Term Results. Microsurgery 2010, 30, 256–260. [Google Scholar] [CrossRef]
- Cho, M.J.; Kwon, J.G.; Pak, C.J.; Suh, H.P.; Hong, J.P. The Role of Duplex Ultrasound in Microsurgical Reconstruction: Review and Technical Considerations. J. Reconstr. Microsurg. 2020, 36, 514–521. [Google Scholar] [CrossRef]
- Lee, Y.L.; Huang, Y.L.; Chu, S.Y.; Chan, W.H.; Cheng, M.H.; Lin, Y.H.; Chang, T.Y.; Yeh, C.K.; Tsui, P.H. Characterization of Limb Lymphedema Using the Statistical Analysis of Ultrasound Backscattering. Quant. Imaging Med. Surg. 2020, 10, 48–56. [Google Scholar] [CrossRef]
- Visconti, G.; Salgarello, M.; Hayashi, A. The Recipient Venule in Supermicrosurgical Lymphaticovenular Anastomosis: Flow Dynamic Classification and Correlation with Surgical Outcomes. J. Reconstr. Microsurg. 2018, 34, 581–589. [Google Scholar] [CrossRef]
- Mihara, M.; Hara, H.; Kawakami, Y. Ultrasonography for Classifying Lymphatic Sclerosis Types and Deciding Optimal Sites for Lymphatic-Venous Anastomosis in Patients with Lymphoedema. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1274–1281. [Google Scholar] [CrossRef]
- Bianchi, A.; Visconti, G.; Hayashi, A.; Santoro, A.; Longo, V.; Salgarello, M. Ultra-High Frequency Ultrasound Imaging of Lymphatic Channels Correlates with Their Histological Features: A Step Forward in Lymphatic Surgery. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1622–1629. [Google Scholar] [CrossRef]
- Masoodi, Z.; Steinbacher, J.; Tinhofer, I.E.; Czedik-Eysenberg, M.; Mohos, B.; Roka-Palkovits, J.; Huettinger, N.; Meng, S.; Tzou, C.-H.J. “Double Barrel” Lymphaticovenous Anastomosis: A Useful Addition to a Supermicrosurgeon’s Repertoire. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4267. [Google Scholar] [CrossRef]
- Jang, S.; Lee, C.U.; Hesley, G.K.; Knudsen, J.M.; Brinkman, N.J.; Tran, N.V. Lymphatic Mapping Using US Microbubbles before Lymphaticovenous Anastomosis Surgery for Lymphedema. Radiology 2022, 304, 218–224. [Google Scholar] [CrossRef]
- Lahtinen, O.; Vanninen, R.; Rautiainen, S. Contrast-Enhanced Ultrasound: A New Tool for Imaging the Superficial Lymphatic Vessels of the Upper Limb. Eur. Radiol. Exp. 2022, 6, 18. [Google Scholar] [CrossRef]
- Hayashi, A.; Yamamoto, T.; Yoshimatsu, H.; Hayashi, N.; Furuya, M.; Harima, M.; Narushima, M.; Koshima, I. Ultrasound Visualization of the Lymphatic Vessels in the Lower Leg. Microsurgery 2016, 36, 397–401. [Google Scholar] [CrossRef]
- Hayashi, A.; Hayashi, N.; Yoshimatsu, H.; Yamamoto, T. Effective and Efficient Lymphaticovenular Anastomosis Using Preoperative Ultrasound Detection Technique of Lymphatic Vessels in Lower Extremity Lymphedema. J. Surg. Oncol. 2018, 117, 290–298. [Google Scholar] [CrossRef]
- Mohos, B.; Czedik-Eysenberg, M.; Steinbacher, J.; Tinhofer, I.; Meng, S.; Tzou, C.-H.J. Long-Term Use of Ultrasound for Locating Optimal LVA Sites: A Descriptive Data Analysis. J. Reconstr. Microsurg. 2022, 38, 238–244. [Google Scholar] [CrossRef]
- Czedik-Eysenberg, M.; Steinbacher, J.; Obermayer, B.; Yoshimatsu, H.; Hara, H.; Mihara, M.; Tzou, C.-H.J.; Meng, S. Exclusive Use of Ultrasound for Locating Optimal LVA Sites-A Descriptive Data Analysis. J. Surg. Oncol. 2020, 121, 51–56. [Google Scholar] [CrossRef]
- Russo, A.; Reginelli, A.; Lacasella, G.V.; Grassi, E.; Ahmed, M.; Karaboue, A.; Quarto, T.; Busetto, G.M.; Aliprandi, A.; Grassi, R.; et al. Clinical Application of Ultra-High-Frequency Ultrasound. J. Pers. Med. 2022, 12, 1733. [Google Scholar] [CrossRef]
- Szuba, A.; Shin, W.S.; Strauss, H.W.; Rockson, S. The Third Circulation: Radionuclide Lymphoscintigraphy in the Evaluation of Lymphedema. J. Nucl. Med. 2004, 44, 43–57. [Google Scholar]
- Strand, S.E.; Bergqvist, L. Radiolabeled Colloids and Macromolecules in the Lymphatic System. Crit. Rev. Ther. Drug Carr. Syst. 1989, 6, 211–238. [Google Scholar]
- Polomska, A.K.; Proulx, S.T. Imaging Technology of the Lymphatic System. Adv. Drug Deliv. Rev. 2020, 170, 294–311. [Google Scholar] [CrossRef]
- Kramer, E.L. Lymphoscintigraphy: Defining a Clinical Role. Lymphat. Res. Biol. 2004, 2, 32–37. [Google Scholar] [CrossRef]
- Vaqueiro, M.; Gloviczki, P.; Fisher, J.; Hollier, L.H.; Schirger, A.; Wahner, H.W. Lymphoscintigraphy in Lymphedema: An Aid to Microsurgery. J. Nucl. Med. 1986, 27, 1125–1130. [Google Scholar]
- Cabrera, R.N.; Chone, C.T.; Zantut-Wittmann, D.E.; Matos, P.S.; Ferreira, D.M.; Pereira, P.S.; Ribeiro, M.P.; Santos, A.O.; Ramos, C.D.; Crespo, A.N.; et al. The Role of SPECT/CT Lymphoscintigraphy and Radioguided Sentinel Lymph Node Biopsy in Managing Papillary Thyroid Cancer. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 834–841. [Google Scholar] [CrossRef]
- Pappalardo, M.; Cheng, M.H. Lymphoscintigraphy for the Diagnosis of Extremity Lymphedema: Current Controversies Regarding Protocol, Interpretation, and Clinical Application. J. Surg. Oncol. 2020, 121, 37–47. [Google Scholar] [CrossRef]
- Lasso, J.M.; Alonso-Farto, J.C. Indocyanine Green-Guided Liposuction for Patients Presenting with Residual Nonpitting Edema after Lymphovenous Anastomosis. J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 2482–2492. [Google Scholar] [CrossRef]
- Yoneya, S.; Saito, T.; Komatsu, Y.; Koyama, I.; Takahashi, K.; Duvoll-young, J. Binding Properties of Indocyanine Green in Human Blood. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1286–1290. [Google Scholar]
- Robson, S.C.; Mutch, E.; Boys, R.J.; Woodhouse, K.W. Apparent Liver Blood Flow during Pregnancy: A Serial Study Using Indocyanine Green Clearance. Br. J. Obstet. Gynaecol. 1990, 97, 720–724. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, Y.; Yang, H.; Xu, Y. Maternal-Fetal Transfer of Indocyanine Green: A Systematic Review. J. Matern.-Fetal Neonatal Med. 2022, 35, 8181–8185. [Google Scholar] [CrossRef]
- Staurenghi, G.; Bottoni, F.; Giani, A. Clinical Applications of Diagnostic Indocyanine Green Angiography. Retin. Fifth Ed. 2012, 1, 51–81. [Google Scholar] [CrossRef]
- Belgrado, J.P.; Vandermeeren, L.; Vankerckhove, S.; Valsamis, J.B.; Malloizel-Delaunay, J.; Moraine, J.J.; Liebens, F. Near-Infrared Fluorescence Lymphatic Imaging to Reconsider Occlusion Pressure of Superficial Lymphatic Collectors in Upper Extremities of Healthy Volunteers. Lymphat. Res. Biol. 2016, 14, 70–77. [Google Scholar] [CrossRef]
- Yamamoto, T.; Narushima, M.; Doi, K.; Oshima, A.; Ogata, F.; Mihara, M.; Koshima, I.; Mundinger, G.S. Characteristic Indocyanine Green Lymphography Findings in Lower Extremity Lymphedema: The Generation of a Novel Lymphedema Severity Staging System Using Dermal Backflow Patterns. Plast. Reconstr. Surg. 2011, 127, 1979–1986. [Google Scholar] [CrossRef]
- Yamamoto, T.; Matsuda, N.; Doi, K.; Oshima, A.; Yoshimatsu, H.; Todokoro, T.; Ogata, F.; Mihara, M.; Narushima, M.; Iida, T.; et al. The Earliest Finding of Indocyanine Green Lymphography in Asymptomatic Limbs of Lower Extremity Lymphedema Patients Secondary to Cancer Treatment: The Modified Dermal Backflow Stage and Concept of Subclinical Lymphedema. Plast. Reconstr. Surg. 2011, 128, 314e–321e. [Google Scholar] [CrossRef]
- Yamamoto, T.; Narushima, M.; Koshima, I. Lymphatic Vessel Diameter in Female Pelvic Cancer-Related Lower Extremity Lymphedematous Limbs. J. Surg. Oncol. 2018, 117, 1157–1163. [Google Scholar] [CrossRef]
- Wiser, I.; Mehrara, B.J.; Coriddi, M.; Kenworthy, E.; Cavalli, M.; Encarnacion, E.; Dayan, J.H. Preoperative Assessment of Upper Extremity Secondary Lymphedema. Cancers 2020, 12, 135. [Google Scholar] [CrossRef]
- Yamamoto, T.; Yamamoto, N.; Doi, K.; Oshima, A.; Yoshimatsu, H.; Todokoro, T.; Ogata, F.; Mihara, M.; Narushima, M.; Iida, T.; et al. Indocyanine Green-Enhanced Lymphography for Upper Extremity Lymphedema: A Novel Severity Staging System Using Dermal Backflow Patterns. Plast. Reconstr. Surg. 2011, 128, 941–947. [Google Scholar] [CrossRef]
- Unno, N.; Nishiyama, M.; Suzuki, M.; Yamamoto, N.; Inuzuka, K.; Sagara, D.; Tanaka, H.; Konno, H. Quantitative Lymph Imaging for Assessment of Lymph Function Using Indocyanine Green Fluorescence Lymphography. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2008, 36, 230–236. [Google Scholar] [CrossRef]
- Granoff, M.D.; Johnson, A.R.; Lee, B.T.; Padera, T.P.; Bouta, E.M.; Singhal, D. A Novel Approach to Quantifying Lymphatic Contractility during Indocyanine Green Lymphangiography. Plast. Reconstr. Surg. 2019, 144, 1197–1201. [Google Scholar] [CrossRef]
- Pons, G.; Clavero, J.A.; Alomar, X.; Rodríguez-bauza, E.; Tom, L.K.; Masia, J. Preoperative Planning of Lymphaticovenous Anastomosis: The Use of Magnetic Resonance Lymphangiography as a Complement to Indocyanine Green Lymphography. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 884–891. [Google Scholar] [CrossRef]
- Mihara, M.; Hara, H.; Araki, J.; Kikuchi, K.; Narushima, M.; Yamamoto, T.; Iida, T.; Yoshimatsu, H.; Murai, N.; Mitsui, K.; et al. Indocyanine Green (ICG) Lymphography Is Superior to Lymphoscintigraphy for Diagnostic Imaging of Early Lymphedema of the Upper Limbs. PLoS ONE 2012, 7, e38182. [Google Scholar] [CrossRef]
- Mills, M.; Van Zanten, M.; Borri, M.; Mortimer, P.S.; Howe, F.A.; Gordon, K.; Ostergaard, P. Systematic Review of Magnetic Resonance Lymphangiography From a Technical Perspective. J. Magn. Reson. Imaging 2021, 53, 1766–1790. [Google Scholar] [CrossRef] [PubMed]
- Crescenzi, R.; Donahue, M.J. CEST MRI Quantification Procedures for Breast Cancer Treatment-Related Lymphedema Therapy Evaluation. Magn. Reson. Med. 2019, 83, 1760–1773. [Google Scholar] [CrossRef]
- Rane, S.; Donahue, P.M.C.; Towse, T.; Ridner, S.; Chappell, M.; Jordi, J.; Gore, J.; Donahue, M.J. Clinical Feasibility of Noninvasive Visualization of Lymphatic Flow with Principles of Spin Labeling MR Imaging: Implications for Lymphedema Assessment. Radiology 2013, 269, 893–902. [Google Scholar] [CrossRef]
- Neligan, P.C.; Kung, T.A.; Maki, J.H. MR Lymphangiography in the Treatment of Lymphedema. J. Surg. Oncol. 2017, 115, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Soga, S.; Onishi, F.; Mikoshi, A.; Okuda, S.; Jinzaki, M.; Shinmoto, H. Lower Limb Lymphedema Staging Based on Magnetic Resonance Lymphangiography. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 10, 445–453.e3. [Google Scholar] [CrossRef]
- Masia, J.; Pons, G.; Nardulli, M.L. Combined Surgical Treatment in Breast Cancer-Related Lymphedema. J. Reconstr. Microsurg. 2016, 32, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Giacalone, G.; Yamamoto, T.; Belva, F.; Hayashi, A. Bedside 3D Visualization of Lymphatic Vessels with a Handheld Multispectral Optoacoustic Tomography Device. J. Clin. Med. 2020, 9, 815. [Google Scholar] [CrossRef] [PubMed]
- Kajita, H.; Kishi, K. High-Resolution Imaging of Lymphatic Vessels with Photoacoustic Lymphangiography. Radiology 2019, 292, 35. [Google Scholar] [CrossRef]
- Kajita, H.; Oh, A.; Urano, M.; Takemaru, M.; Imanishi, N.; Otaki, M.; Yagi, T.; Aiso, S.; Kishi, K. Photoacoustic Lymphangiography. J. Surg. Oncol. 2020, 121, 48–50. [Google Scholar] [CrossRef]
- Nagae, K.; Asao, Y.; Sudo, Y.; Murayama, N.; Tanaka, Y.; Ohira, K.; Ishida, Y.; Otsuka, A.; Matsumoto, Y.; Saito, S.; et al. Real-Time 3D Photoacoustic Visualization System with a Wide Field of View for Imaging Human Limbs. F1000Research 2018, 7, 1813. [Google Scholar] [CrossRef]
- Schmitt, J.M. Optical Coherence Tomography: A Review. IEEE J. Sel. Top. Quantum Electron. 1999, 5, 1205–1215. [Google Scholar] [CrossRef]
- Yonetsu, T.; Bouma, B.E.; Kato, K.; Fujimoto, J.G.; Jang, I.K. Optical Coherence Tomography: 15 Years in Cardiology. Circ. J. 2013, 77, 1933–1940. [Google Scholar] [CrossRef]
- Baran, U.; Choi, W.J.; Wang, R.K. Potential Use of OCT-Based Microangiography in Clinical Dermatology. Ski. Res. Technol. 2016, 22, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, A.; Yoshimatsu, H.; Visconti, G.; Sujarittanakarn, S.; Giacalone, G.; Hayashi, N.; Yamamoto, T.; Yang, J.C.S.; Hong, J.P. Intraoperative Real-Time Visualization of the Lymphatic Vessels Using Microscope-Integrated Laser Tomography. J. Reconstr. Microsurg. 2021, 37, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.S.; Wu, S.C.; Chiang, M.H.; Lin, W.C.; Hsieh, C.H. Intraoperative Identification and Definition of “Functional” Lymphatic Collecting Vessels for Supermicrosurgical Lymphatico-Venous Anastomosis in Treating Lymphedema Patients. J. Surg. Oncol. 2018, 117, 994–1000. [Google Scholar] [CrossRef]
- Polomska, A.K.; Proulx, S.T.; Brambilla, D.; Fehr, D.; Bonmarin, M.; Brändli, S.; Meboldt, M.; Steuer, C.; Vasileva, T.; Reinke, N.; et al. Minimally Invasive Method for the Point-of-Care Quantification of Lymphatic Vessel Function. JCI Insight 2019, 4, e126515. [Google Scholar] [CrossRef]
- Kwon, S.; Velasquez, F.C.; Rasmussen, J.C.; Greives, M.R.; Turner, K.D.; Morrow, J.R.; Hwu, W.-J.; Ross, R.F.; Zhang, S.; Sevick-Muraca, E.M. Nanotopography-Based Lymphatic Delivery for Improved Anti-Tumor Responses to Checkpoint Blockade Immunotherapy. Theranostics 2019, 9, 8332–8343. [Google Scholar] [CrossRef] [PubMed]
- Narushima, M.; Yamamoto, T.; Ogata, F.; Yoshimatsu, H.; Mihara, M.; Koshima, I. Indocyanine Green Lymphography Findings in Limb Lymphedema. J. Reconstr. Microsurg. 2016, 32, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Hara, H.; Mihara, M. Multi-Area Lymphaticovenous Anastomosis with Multi-Lymphosome Injection in Indocyanine Green Lymphography: A Prospective Study. Microsurgery 2019, 39, 167–173. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]

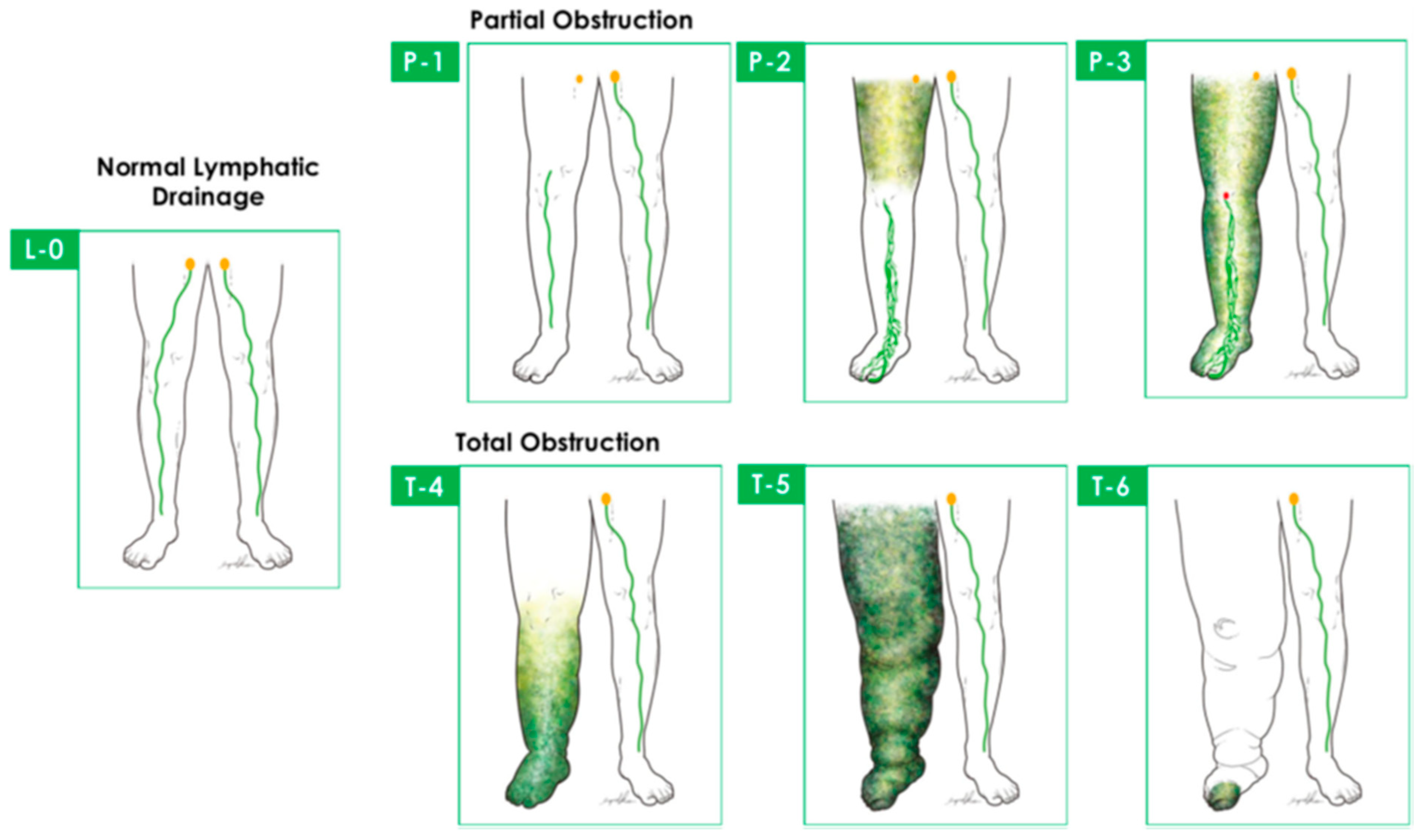

| Cheng’s Lymphedema Grade | Circumferential Difference (%) | Episodes of Cellulitis(Times/yr) | Taiwan Lymphoscintigraphy Staging | ICG Lymphography | Treatment | |
|---|---|---|---|---|---|---|
| 0 | 0–9 | 0–1 | L-0, P-1, P-2 | Patent lymphatic ducts | CDT, LVA | |
| I | IA | 10–19 | 1–2 | P-1, P-2, P-3 | Patent lymphatic ducts | LVA |
| IB | P-3, T-4 | Diffuse DB | VLNT | |||
| II | IIA | 20–29 | 2–3 | P-1, P-2, P-3 | Patent lymphatic ducts | LVA |
| IIB | P-3, T-4, T-5 | Diffuse DB | VLNT | |||
| III | 30–39 | 3–4 | P-3, T-4, T-5, T-6 | Not performed | VLNT + additional procedures | |
| IV | >40 | >4 | T-4, T-5, T-6 | Not performed | VLNT + additional procedures 1 |
| DB Stage | ICG Lymphography Findings |
|---|---|
| Stage 0 | No dermal backflow patterns |
| Stage I | Linear pattern + Splash pattern 1 |
| Stage II | Linear pattern + Stardust pattern (1 region) 2 |
| Stage III | Linear pattern + Stardust pattern (2 regions) 2 |
| Stage IV | Linear pattern + Stardust pattern (3 regions) 2 |
| Stage V | Stardust and/or Diffuse pattern 3 |
| DB Stage | ICG Lymphography Findings |
|---|---|
| Stage 0 | No dermal backflow patterns |
| Stage I | Splash pattern around the axilla |
| Stage II | Stardust pattern limited between the axilla and the olecranon |
| Stage III | Stardust pattern exceeding the olecranon |
| Stage IV | Stardust pattern observed throughout the limb |
| Stage V | Diffuse pattern and stardust |
| Modality | Applications | Advantages | Limitations |
|---|---|---|---|
| LS |
|
|
|
| US |
|
|
|
| ICG-L |
|
|
|
| MRL |
|
|
|
| PAI |
|
|
|
| OCT |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy, B.I.; Mohos, B.; Tzou, C.-H.J. Imaging Modalities for Evaluating Lymphedema. Medicina 2023, 59, 2016. https://doi.org/10.3390/medicina59112016
Nagy BI, Mohos B, Tzou C-HJ. Imaging Modalities for Evaluating Lymphedema. Medicina. 2023; 59(11):2016. https://doi.org/10.3390/medicina59112016
Chicago/Turabian StyleNagy, Bendeguz Istvan, Balazs Mohos, and Chieh-Han John Tzou. 2023. "Imaging Modalities for Evaluating Lymphedema" Medicina 59, no. 11: 2016. https://doi.org/10.3390/medicina59112016
APA StyleNagy, B. I., Mohos, B., & Tzou, C.-H. J. (2023). Imaging Modalities for Evaluating Lymphedema. Medicina, 59(11), 2016. https://doi.org/10.3390/medicina59112016