

Submerged Technique of Partially De-Epithelialized Free Gingival Grafts for Gingival Phenotype Modification in the Maxillary Anterior Region: A Case Report of a 34-Year Follow-up


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
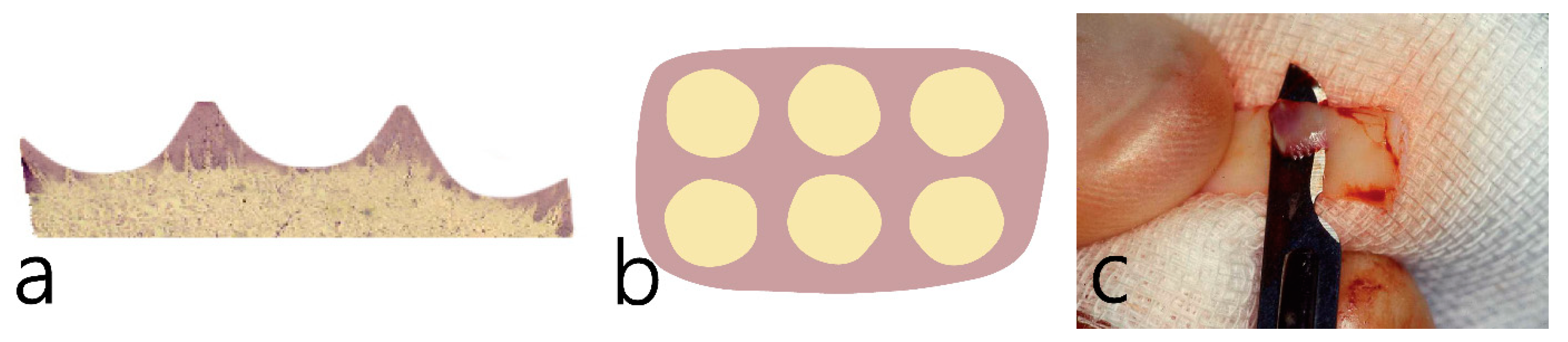
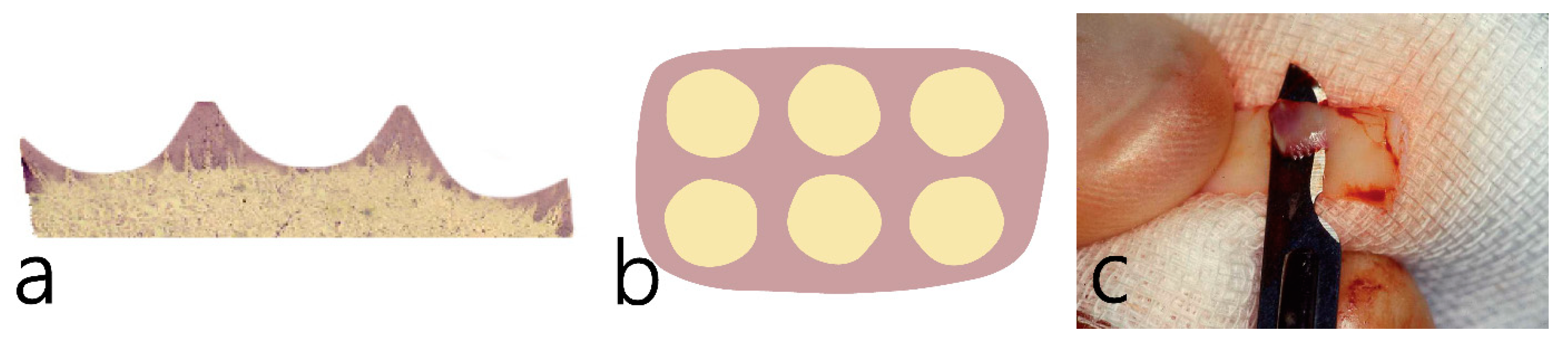
Surgical Procedure
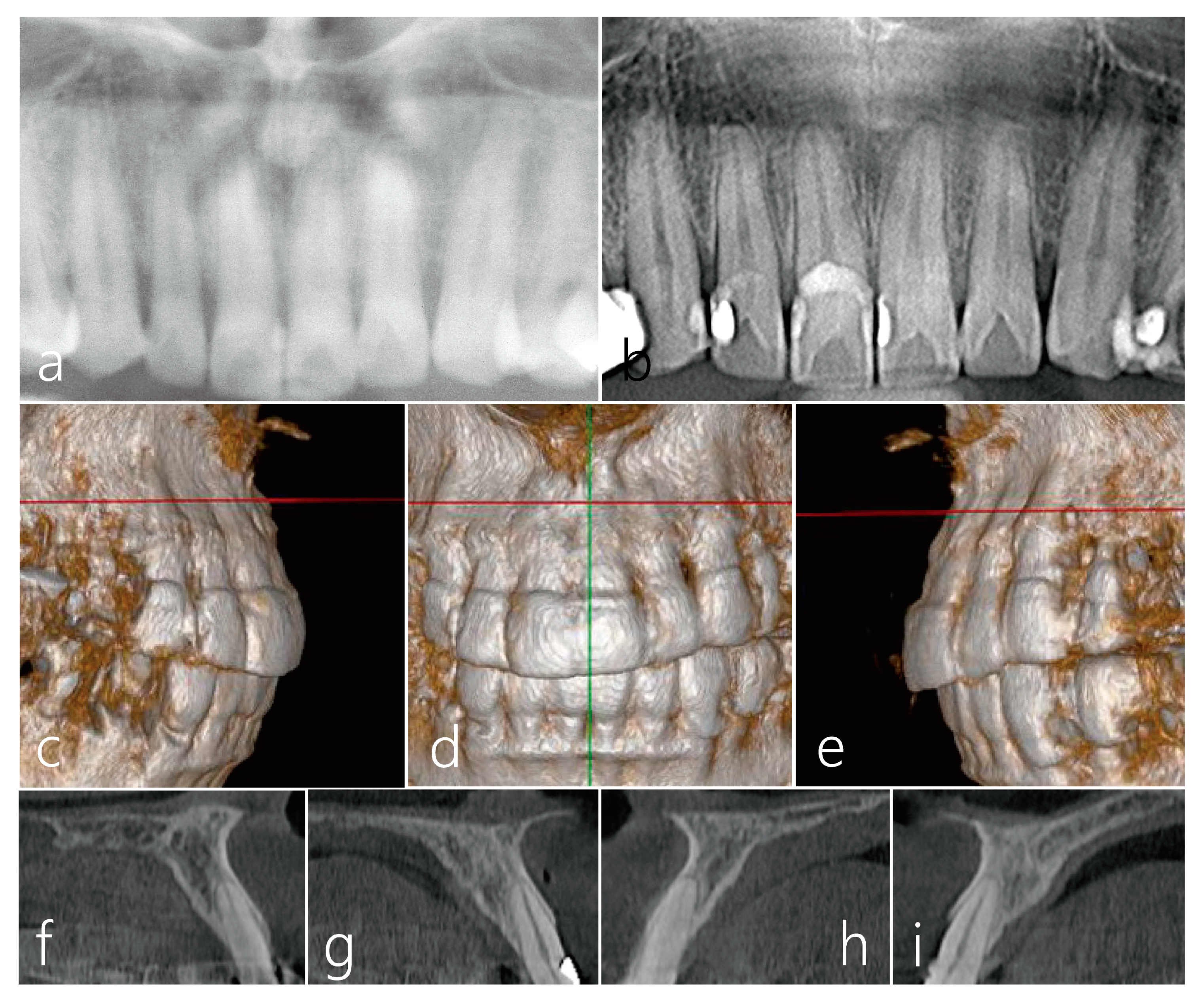
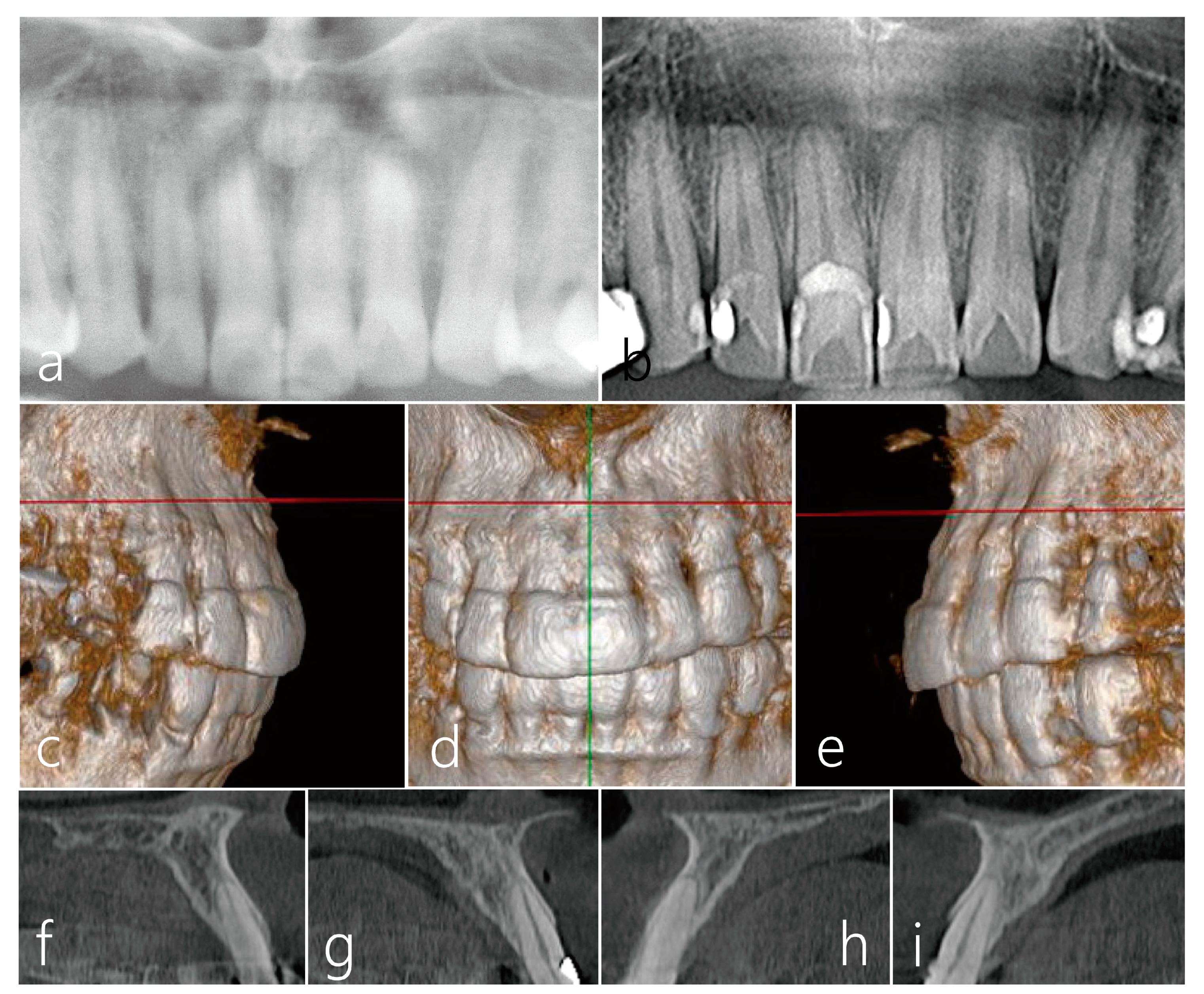
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, P.D., Jr. Root coverage with the free gingival graft. Factors associated with incomplete coverage. J. Periodontol. 1987, 58, 674–681. [Google Scholar] [CrossRef]
- Deo, S.D.; Shetty, S.K.; Kulloli, A.; Chavan, A.K.R.; Dholakia, P.; Ligade, S.; Dharmarajan, G. Efficacy of free gingival graft in the treatment of Miller Class I and Class II localized gingival recessions: A systematic review. J. Indian Soc. Periodontol. 2019, 23, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, T.; Ochsenbein, C. Complete coverage of the denuded root surface with a one-stage gingival graft. Int. J. Periodontics Restor. Dent. 1983, 3, 8–27. [Google Scholar]
- Miller, P.D. Root coverage using free soft tissue autografts following acid application. I. Technique. Int. J. Periodontics Restor. Dent. 1982, 2, 65–70. [Google Scholar]
- Jahnke, P.V.; Sandifer, J.B.; Gher, M.E.; Gray, J.L.; Richardson, A.C. Thick free gingival and connective tissue autografts for root coverage. J. Periodontol. 1993, 64, 315–322. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J. Dent. 2008, 36, 659–671. [Google Scholar] [CrossRef]
- Zucchelli, G.; Mele, M.; Stefanini, M.; Mazzotti, C.; Marzadori, M.; Montebugnoli, L.; de Sanctis, M. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: A comparative randomized-controlled clinical trial. J. Clin. Periodontol. 2010, 37, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Ripoll, S.; de Velasco-Tarilonte, Á.F.; Bullón, B.; Ríos-Carrasco, B.; Fernández-Palacín, A. Complications in the Use of Deepithelialized Free Gingival Graft vs. Connective Tissue Graft: A One-Year Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 4504. [Google Scholar]
- Zucchelli, G.; Bentivogli, V.; Ganz, S.; Bellone, P.; Mazzotti, C. The connective tissue graft wall technique to improve root coverage and clinical attachment levels in lingual gingival defects. Int. J. Esthet. Dent. 2016, 11, 538–548. [Google Scholar] [PubMed]
- Kinaia, B.M.; Kazerani, S.; Hsu, Y.T.; Neely, A.L. Partly Deepithelialized Free Gingival Graft for Treatment of Lingual Recession. Clin. Adv. Periodontics 2019, 9, 160–165. [Google Scholar] [CrossRef]
- Zucchelli, G.; Marzadori, M.; Mounssif, I.; Mazzotti, C.; Stefanini, M. Coronally advanced flap + connective tissue graft techniques for the treatment of deep gingival recession in the lower incisors. A controlled randomized clinical trial. J. Clin. Periodontol. 2014, 41, 806–813. [Google Scholar] [CrossRef]
- Fawzy, M.; Hosny, M.; El-Nahass, H. Evaluation of esthetic outcome of delayed implants with de-epithelialized free gingival graft in thin gingival phenotype with or without immediate temporization: A randomized clinical trial. Int. J. Implant Dent. 2023, 9, 5. [Google Scholar] [CrossRef]
- Cortellini, P.; Tonetti, M.; Prato, G.P. The partly epithelialized free gingival graft (pe-fgg) at lower incisors. A pilot study with implications for alignment of the mucogingival junction. J. Clin. Periodontol. 2012, 39, 674–680. [Google Scholar] [CrossRef]
- Cairo, F. Periodontal plastic surgery of gingival recessions at single and multiple teeth. Periodontol. 2000 2017, 75, 296–316. [Google Scholar] [CrossRef] [PubMed]
- Langer, B.; Langer, L. Subepithelial connective tissue graft technique for root coverage. J. Periodontol. 1985, 56, 715–720. [Google Scholar] [CrossRef]
- Chambrone, L.; Ortega, M.A.S.; Sukekava, F.; Rotundo, R.; Kalemaj, Z.; Buti, J.; Prato, G.P.P. Root coverage procedures for treating localised and multiple recession-type defects. Cochrane Database Syst. Rev. 2018, 10, CD007161. [Google Scholar] [CrossRef]
- Dembowska, E.; Drozdzik, A. Subepithelial connective tissue graft in the treatment of multiple gingival recession. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endo. 2007, 104, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Dani, S.; Dhage, A.; Gundannavar, G. The pouch and tunnel technique for management of multiple gingival recession defects. J. Indian Soc. Periodontol. 2014, 18, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Lee, D.; Kim, S.; Ku, Y.; Rhyu, I. Modified tunneling technique for root coverage of anterior mandible using minimal soft tissue harvesting and volume-stable collagen matrix: A retrospective study. J. Periodontal. Imp. Sci. 2021, 6, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Caffesse, R.G.; Guinard, E.A. Treatment of Localized Gingival Recessions. Part II. Coronally Repositioned Flap with a Free Gingival Graft. J. Periodontol. 1978, 49, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.J. The connective tissue and partial thickness double pedicle graft: A predictable method of obtaining root coverage. J. Periodontol. 1992, 63, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Hurzeler, M.B.; Weng, D.A. Single incision technique to harvest subepithelial connective tissue grafts from palate. Int. J. Periodontics Restor. Dent. 1999, 19, 279–287. [Google Scholar]
- Kumar, A.; Sood, V.; Masamatti, S.S.; Triveni, M.G.; Mehta, D.S.; Khatri, M.; Agarwal, V. Modified single incision technique to harvest subepithelial connective tissue graft. J. Indian Soc. Periodontol. 2013, 17, 676–680. [Google Scholar] [CrossRef]
- Bakhishov, H.; Isler, S.C.; Bozyel, B.; Yıldırım, B.; Tekindal, M.A.; Ozdemir, B. De-epithelialized gingival graft versus subepithelial connective tissue graft in the treatment of multiple adjacent gingival recessions using the tunnel technique: 1-Year results of a randomized clinical trial. J. Clin. Periodontol. 2021, 48, 970–983. [Google Scholar] [CrossRef] [PubMed]
- Bednarz, W.; Majer, J.; Pakuszy´nska-Błaszczyk, J.; Dominiak, M.; Gedrange, T.; Zielinska-Pałasz, A. Coronally Advanced Flap in the Treatment of Multiple Adjacent Gingival Recessions along with a Connective Tissue Graft Harvested from Augmented or Nonaugmented Palatal Mucous Membrane: A Two-Year Comparative Clinical Evaluation. Appl. Sci. 2021, 11, 1081. [Google Scholar] [CrossRef]
- Bertl, K.; Pifl, M.; Hirtler, L.; Rendl, B.; Nürnberger, S.; Stavropoulos, A.; Ulm, C. Relative Composition of Fibrous Connective and Fatty/Glandular Tissue in Connective Tissue Grafts Depends on the Harvesting Technique but not the Donor Site of the Hard Palate. J. Periodontol. 2015, 86, 1331–1339. [Google Scholar] [CrossRef]
- Zuhr, O.; Bäumer, D.; Hürzeler, M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: Critical elements in design and execution. J. Clin. Periodontol. 2014, 41 (Suppl. 15), S123–S142. [Google Scholar] [CrossRef]
- Harris, R.J. Formation of a cyst-like area after a connective tissue graft for root coverage. J. Periodontol. 2002, 73, 340–345. [Google Scholar] [CrossRef] [PubMed]
- de Castro, L.A.; Vêncio, E.F.; Mendonça, E.F. Epithelial inclusion cyst after free gingival graft: A case report. Int. J. Periodontics Restor. Dent. 2007, 27, 465–469. [Google Scholar]
- Harris, R.J. Treatment of a previously placed autogenous masticatory mucosa graft (free gingival graft). A case report. J. Periodontol. 1998, 69, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.O.; Ribeiro, E.D.P.; Sallum, A.W.; Tatakis, D.N. Free gingival grafts: Graft shrinkage and donor-site healing in smokers and non-smokers. J. Periodontol. 2010, 81, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Park, W.B.; Kang, K.L.; Han, J.Y. Long-Term Clinical and Radiographic Observation of Periimplant Tissues after Autogenous Soft Tissue Grafts: A 15-Year Retrospective Study. Implant Dent. 2017, 26, 762–769. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, W.-B.; Park, W.; Kang, P.; Lim, H.-C.; Han, J.-Y. Submerged Technique of Partially De-Epithelialized Free Gingival Grafts for Gingival Phenotype Modification in the Maxillary Anterior Region: A Case Report of a 34-Year Follow-up. Medicina 2023, 59, 1832. https://doi.org/10.3390/medicina59101832
Park W-B, Park W, Kang P, Lim H-C, Han J-Y. Submerged Technique of Partially De-Epithelialized Free Gingival Grafts for Gingival Phenotype Modification in the Maxillary Anterior Region: A Case Report of a 34-Year Follow-up. Medicina. 2023; 59(10):1832. https://doi.org/10.3390/medicina59101832
Chicago/Turabian StylePark, Won-Bae, Wonhee Park, Philip Kang, Hyun-Chang Lim, and Ji-Young Han. 2023. "Submerged Technique of Partially De-Epithelialized Free Gingival Grafts for Gingival Phenotype Modification in the Maxillary Anterior Region: A Case Report of a 34-Year Follow-up" Medicina 59, no. 10: 1832. https://doi.org/10.3390/medicina59101832
APA StylePark, W.-B., Park, W., Kang, P., Lim, H.-C., & Han, J.-Y. (2023). Submerged Technique of Partially De-Epithelialized Free Gingival Grafts for Gingival Phenotype Modification in the Maxillary Anterior Region: A Case Report of a 34-Year Follow-up. Medicina, 59(10), 1832. https://doi.org/10.3390/medicina59101832