
Post VV-ECMO Weaning Hyperinflammation—Can Prophylactic Hemoadsorption Treatment Prevent Complications?

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Case Series Report
1.2. Patient 1
1.3. Patient 2
1.4. Patient 3
2. Discussion/Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, D.; Ferguson, N.D.; Brochard, L.; Fan, E.; Mercat, A.; Combes, A.; Pellegrino, V.; Schmidt, M.; Slutsky, A.S.; Brodie, D. ECMO for ARDS: From salvage to standard of care? Lancet Respir. Med. 2019, 7, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Tisminetzky, M.; Ferreyro, B.L.; Fan, E. Extracorporeal Membrane Oxygenation in COVID-19. Crit. Care Clin. 2022, 38, 535–552. [Google Scholar] [CrossRef] [PubMed]
- Wieruszewski, P.M.; Ortoleva, J.P.; Cormican, D.S.; Seelhammer, T.G. Extracorporeal Membrane Oxygenation in Acute Respiratory Failure. Pulm. Ther. 2023, 9, 109–126. [Google Scholar]
- Chakraborty, A.; Majumdar, H.S.; Das, W.; Chatterjee, D.; Sarkar, K. Discontinuation of ECMO-a review with a note on Indian scenario. Indian J. Thorac. Cardiovasc. Surg. 2023, 39, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Kirupaharan, P.; Blazoski, C.; Hilton, R.; Feduska, E.; Leong, R.; Baram, M. Systemic Inflammatory Response Syndrome After Extracorporeal Membrane Oxygenation Decannulation in COVID-19 Patients. Cureus 2023, 15, e36436. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Ki, K.K.; Passmore, M.R.; Chan, C.H.H.; Malfertheiner, M.V.; Bouquet, M.; Cho, H.J.; Suen, J.Y.; Fraser, J.F. Effect of ex vivo extracorporeal membrane oxygenation flow dynamics on immune response. Perfusion 2019, 34, 5–14. [Google Scholar] [CrossRef]
- Warren, O.J.; Watret, A.L.; de Wit, K.L.; Alexiou, C.; Vincent, C.; Darzi, A.W.; Athanasiou, T. The inflammatory response to cardiopulmonary bypass: Part 2--anti-inflammatory therapeutic strategies. J. Cardiothorac. Vasc. Anesth. 2009, 23, 384–393. [Google Scholar]
- Shekar, K.; Badulak, J.; Peek, G.; Boeken, U.; Dalton, H.J.; Arora, L.; Bishoy, Z.; Kollengode, R.; Joanne, S.; Bindu, A.; et al. Extracorporeal Life Support Organization Coronavirus Disease 2019 Interim Guidelines: A Consensus Document from an International Group of Interdisciplinary Extracorporeal Membrane Oxygenation Providers. ASAIO J. 2020, 66, 707–721. [Google Scholar] [CrossRef]
- Persic, V.; Jerman, A.; Malgaj Vrecko, M.; Berden, J.; Gorjup, V.; Stecher, A.; Lukic, M.; Jereb, M.; Taleska Stupica, G.; Gubensek, J. Effect of CytoSorb Coupled with Hemodialysis on Interleukin-6 and Hemodynamic Parameters in Patients with Systemic Inflammatory Response Syndrome: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 7500. [Google Scholar] [CrossRef]
- Vallhonrat, H.; Swinford, R.D.; Ingelfinger, J.R.; Williams, W.W.; Ryan, D.P.; Tolkoff-Rubin, N.; Benedict, C.A.; Manljel, P. Rapid activation of the alternative pathway of complement by extracorporeal membrane oxygenation. ASAIO J. 1999, 45, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Boyle, E.M.; Jr Pohlman, T.H.; Johnson, M.C.; Verrier, E.D. Endothelial cell injury in cardiovascular surgery: The systemic inflammatory response. Ann. Thorac. Surg. 1997, 63, 277–284. [Google Scholar] [PubMed]
- Haneke, F.; Schildhauer, T.A.; Schlebes, A.D.; Strauch, J.T.; Swol, J. Infections and Extracorporeal Membrane Oxygenation: Incidence, Therapy, and Outcome. ASAIO J. 2016, 62, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The inflammatory response to extracorporeal membrane oxygenation (ECMO): A review of the pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [PubMed]
- Edmunds, L.H., Jr. Inflammatory response to cardiopulmonary bypass. Ann. Thorac. Surg. 1998, 66, S12–S16; discussion S25–S28. [Google Scholar] [CrossRef]
- Datzmann, T.; Traeger, K. Extracorporeal membrane oxygenation and cytokine adsorption. J. Thorac. Dis. 2018, 10, S653–S660. [Google Scholar] [CrossRef]
- Yeo, H.J.; Yoon, S.H.; Lee, S.E.; Cho, W.H.; Kim, D.; Jeon, D.; Kyung-Hwa, S.; Seong, K.Y. Bacterial Biofilms on Extracorporeal Membrane Oxygenation Catheters. ASAIO J. 2018, 64, e48–e54. [Google Scholar] [CrossRef]
- Yu, Y.; Kim, Y.H.; Cho, W.H.; Son, B.S.; Yeo, H.J. Biofilm microbiome in extracorporeal membrane oxygenator catheters. PLoS ONE 2021, 16, e0257449. [Google Scholar]
- Esposito, E.C.; Jones, K.M.; Galvagno, S.M., Jr.; Kaczorowski, D.J.; Mazzeffi, M.A.; DiChiacchio, L.; Deatrick, K.B.; Madathil, R.J.; Herrold, J.A.; Rabinowitz, R.P.; et al. Incidence of healthcare-associated infections in patients with fever during the first 48 hours after decannulation from veno-venous extracorporeal membrane oxygenation. Perfusion 2021, 36, 421–428. [Google Scholar] [CrossRef]
- Thangappan, K.; Cavarocchi, N.C.; Baram, M.; Thoma, B.; Hirose, H. Systemic inflammatory response syndrome (SIRS) after extracorporeal membrane oxygenation (ECMO): Incidence, risks and survivals. Heart Lung 2016, 45, 449–453. [Google Scholar] [CrossRef]
- Heuts, S.; Makhoul, M.; Mansouri, A.N.; Taccone, F.S.; Obeid, A.; Belliato, M.; Broman, L.M.; Broman, L.M.; Meani, P.; Raffa, G.M.; et al. Defining and understanding the “extra-corporeal membrane oxygenation gap” in the veno-venous configuration: Timing and causes of death. Artif. Organs 2022, 46, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Akil, A.; Napp, L.C.; Rao, C.; Klaus, T.; Scheier, J.; Pappalardo, F. Use of CytoSorb(c) Hemoadsorption in Patients on Veno-Venous ECMO Support for Severe Acute Respiratory Distress Syndrome: A Systematic Review. J. Clin. Med. 2022, 11, 5990. [Google Scholar] [CrossRef] [PubMed]
- Hayanga, J.W.A.; Song, T.; Durham, L.; Garrison, L.; Smith, D.; Molnar, Z.; Scheier, J.; Deliargyris, E.N.; Moazami, N. Extracorporeal hemoadsorption in critically ill COVID-19 patients on VV ECMO: The CytoSorb therapy in COVID-19 (CTC) registry. Crit. Care 2023, 27, 243. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | |
|---|---|---|---|
| Sex | ♀ | ♂ | ♀ |
| Age (years) | 33 | 35 | 50 |
| BMI | 21 | 26.1 | 24.5 |
| Comorbidity | / | / | HTA |
| HR/min | 80 | 130 | 115 |
| RR/min | 30 | 33 | 33 |
| MAP (mmHg) | 80 | 85 | 80 |
| FiO2 (%) | 1.0 | 1.0 | 1.0 |
| PEEP (cm H2O) | 16 | 22 | 16 |
| PaO2/FiO2 (ratio) | 34.4 | 84 | 74 |
| Murray Score (Lung Injury Score) | 3.8 | 3.5 | 4 |
| Vasopressors | / | / | / |
| Microbial isolates (BAL—bronchoalveolar lavage; HC—hemoculture) | BAL: Klebsiella spp. 105 | BAL: Acinetobacter | BAL: Acinetobacter HC: Staphylococcus epidermidis |
| Days on vvECMO | 4 | 7 | 11 |
| Different colors in columns correspond to colors of graphs and other elements in Figure 1, Figure 2 and Figure 3 belonging to appropriate patients. | |||
| Laboratory Findings | Patient No 1 | Patient No 2 | Patient No 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| vvECMO Day 1 | Decannulation Day | 48h after Decannulation | vvECMO Day 1 | Decannulation Day | 48h after Decannulation | vvECMO Day 1 | Decannulation Day | 48h after Decannulation | |
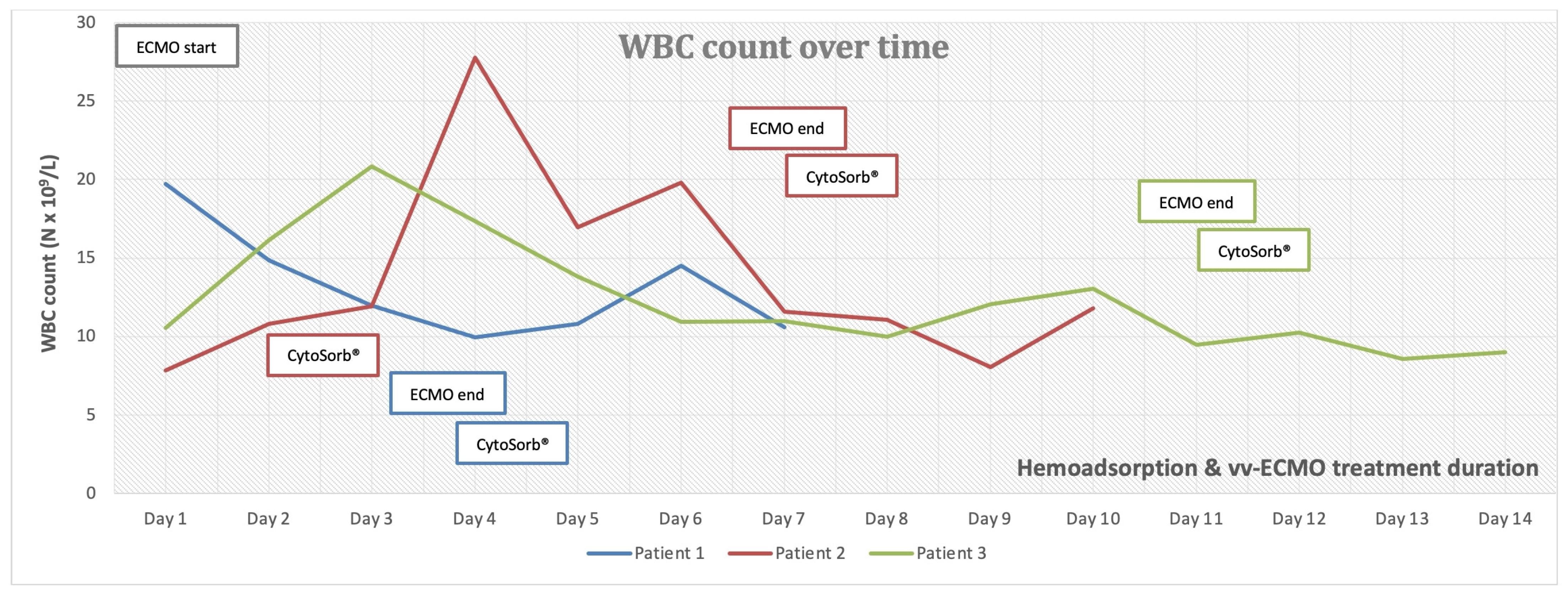
| Leucocytes (N × 109/L) | 19.7 | 13.6 | 10.5 | 2.7 | 3.2 | 3.9 | 10.5 | 9.5 | 8.6 |
| Platelets (N × 109/L) | 202.0 | 196.0 | 169.0 | 30.0 | 94.0 | 104.0 | 283.0 | 95.0 | 108.0 |
| Creatinine (µmol/L) | 52.0 | 47.0 | 45.0 | 506.0 | 131.0 | 211.0 | 81.0 | 117.0 | 72.0 |
| AST (U/L) | 151.0 | 122.0 | 133.0 | 112.0 | 33.0 | 69.0 | 95.0 | 180.0 | 108.0 |
| ALT (U/L) | 288.0 | 269.0 | 286.0 | 59.0 | 81.0 | 211.0 | 286.0 | 211.0 | 86.0 |
| Bilirubin total (µmol/L) | 44.8 | 33.6 | 50.0 | 72.0 | 31.0 | 28.7 | 12.3 | 34.6 | 31.5 |
| Bilirubin direct (µmol/L) | 24.7 | 22.7 | 31.9 | 53.4 | 14.3 | 20.1 | 8.6 | 24.8 | 21.5 |
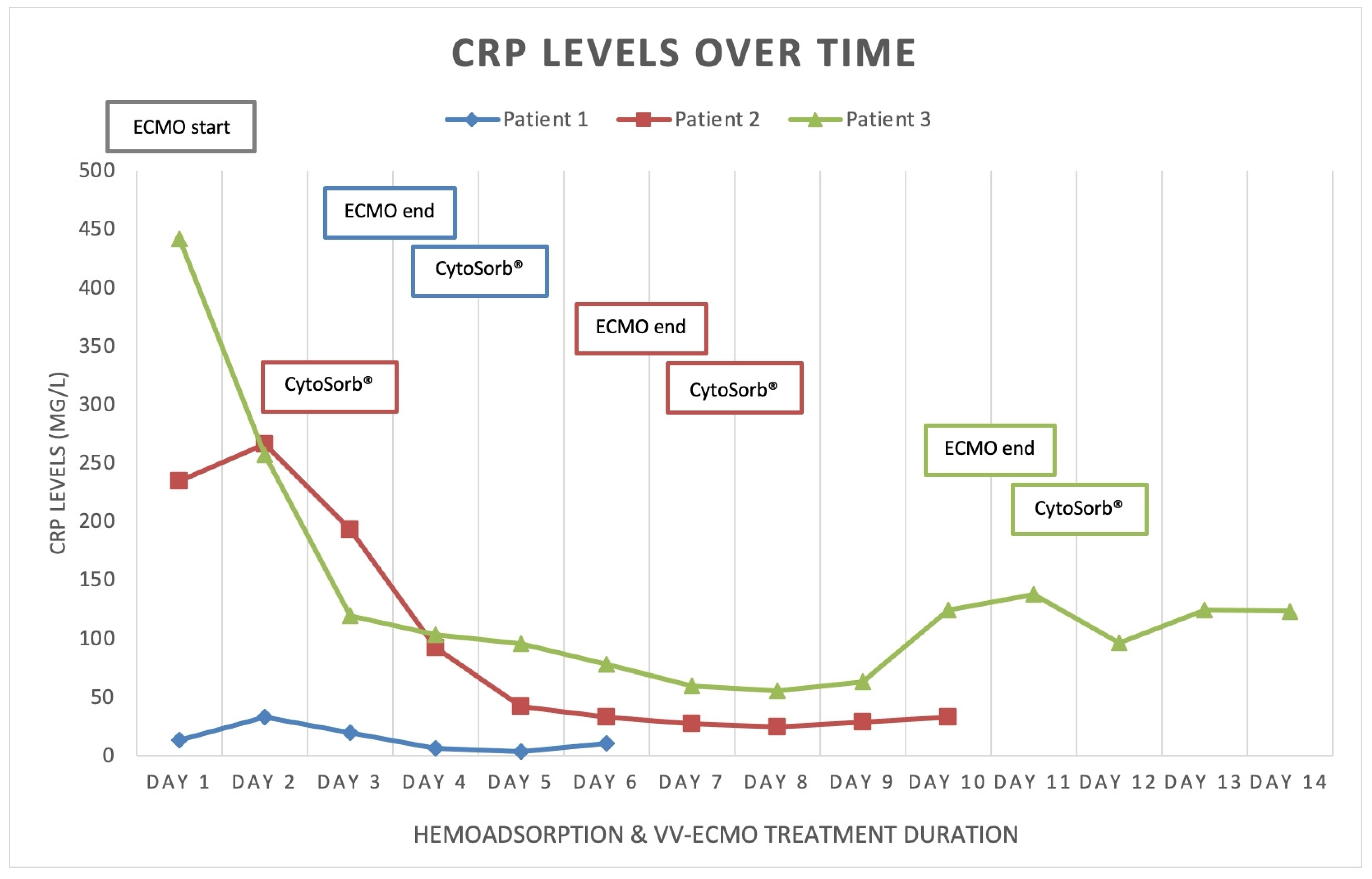
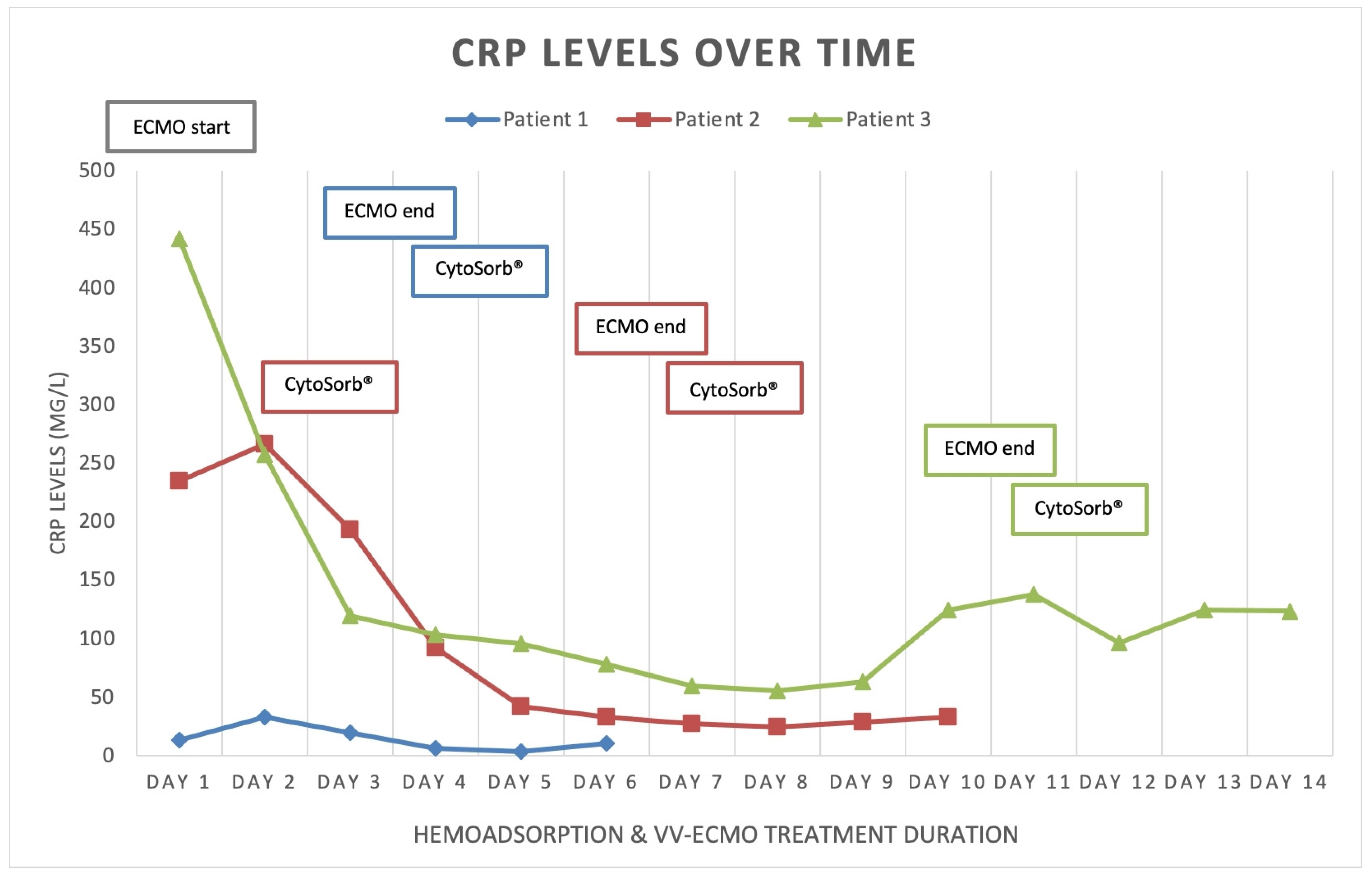
| CRP (mg/L) | 13.1 | 3.7 | 10.8 | 234.8 | 24.9 | 32.9 | 442 | 137.7 | 124.1 |
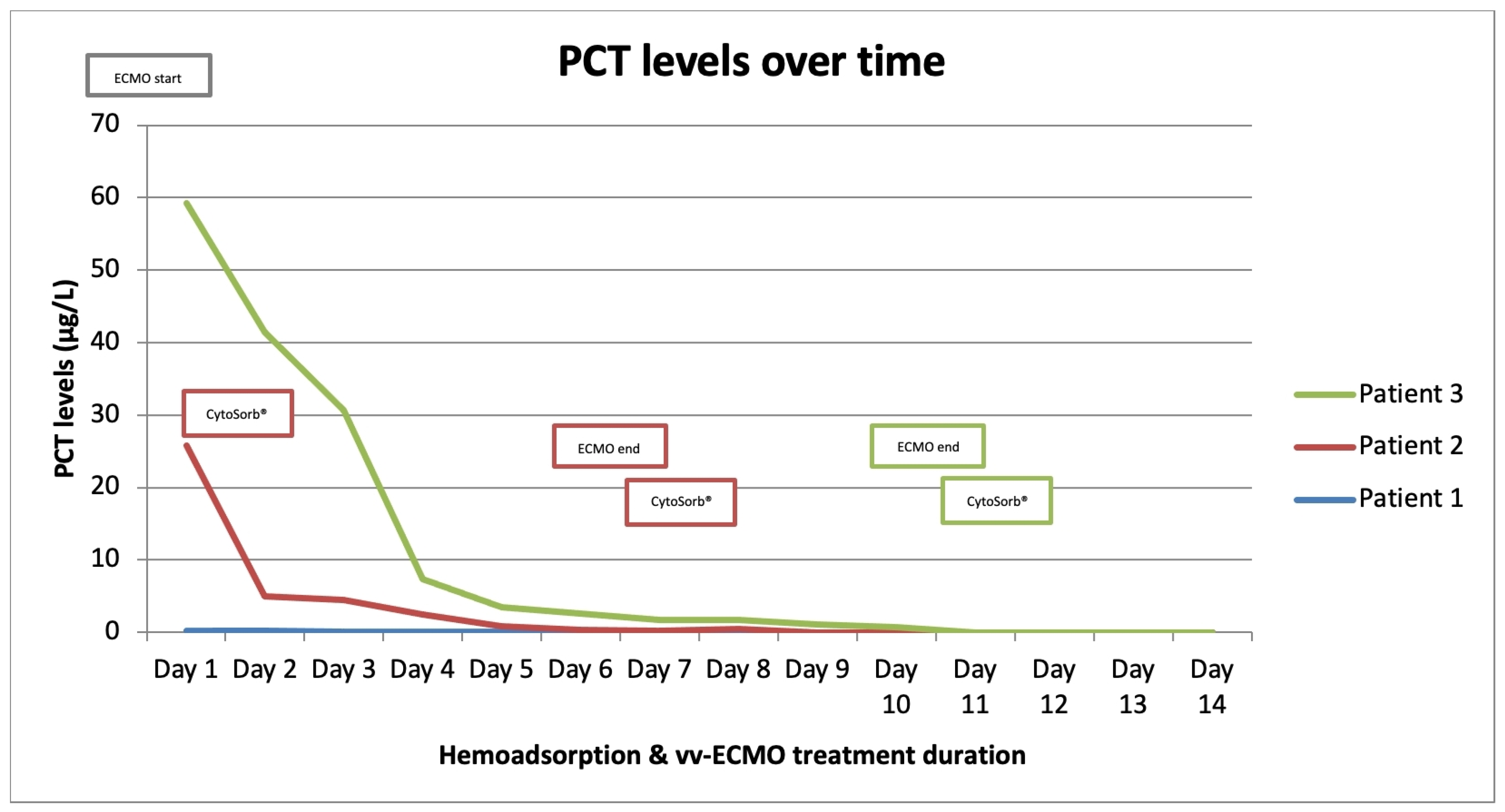
| Procalcitonin (µg/L) | 0.2 | 0.07 | 0.06 | 25.6 | 0.3 | 0.2 | 27.5 | 1.3 | 0.7 |
| Lactate (mmol/L) | 1.3 | 0.8 | 1.0 | 1.4 | 1.6 | 1.2 | 4.2 | 1.8 | 0.8 |
| Temperature (°C) | 37.1 | 36.3 | 36.6 | 36.6 | 36.5 | 36.8 | 36.5 | 36.7 | 36.7 |
| Different colors in columns correspond to colors of graphs and other elements in Figure 1, Figure 2 and Figure 3 belonging to appropriate patients. | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovacevic, P.; Dragic, S.; Jandric, M.; Momcicevic, D.; Topolovac, S.; Malesevic, V.; Kovacevic, T.; Matejic-Spasic, M.; Knezevic, T.; Zlojutro, B. Post VV-ECMO Weaning Hyperinflammation—Can Prophylactic Hemoadsorption Treatment Prevent Complications? Medicina 2023, 59, 1818. https://doi.org/10.3390/medicina59101818
Kovacevic P, Dragic S, Jandric M, Momcicevic D, Topolovac S, Malesevic V, Kovacevic T, Matejic-Spasic M, Knezevic T, Zlojutro B. Post VV-ECMO Weaning Hyperinflammation—Can Prophylactic Hemoadsorption Treatment Prevent Complications? Medicina. 2023; 59(10):1818. https://doi.org/10.3390/medicina59101818
Chicago/Turabian StyleKovacevic, Pedja, Sasa Dragic, Milka Jandric, Danica Momcicevic, Sandra Topolovac, Vedrana Malesevic, Tijana Kovacevic, Marijana Matejic-Spasic, Tanja Knezevic, and Biljana Zlojutro. 2023. "Post VV-ECMO Weaning Hyperinflammation—Can Prophylactic Hemoadsorption Treatment Prevent Complications?" Medicina 59, no. 10: 1818. https://doi.org/10.3390/medicina59101818
APA StyleKovacevic, P., Dragic, S., Jandric, M., Momcicevic, D., Topolovac, S., Malesevic, V., Kovacevic, T., Matejic-Spasic, M., Knezevic, T., & Zlojutro, B. (2023). Post VV-ECMO Weaning Hyperinflammation—Can Prophylactic Hemoadsorption Treatment Prevent Complications? Medicina, 59(10), 1818. https://doi.org/10.3390/medicina59101818