
Potential Therapeutic Strategies in the Treatment of Metabolic-Associated Fatty Liver Disease


Abstract
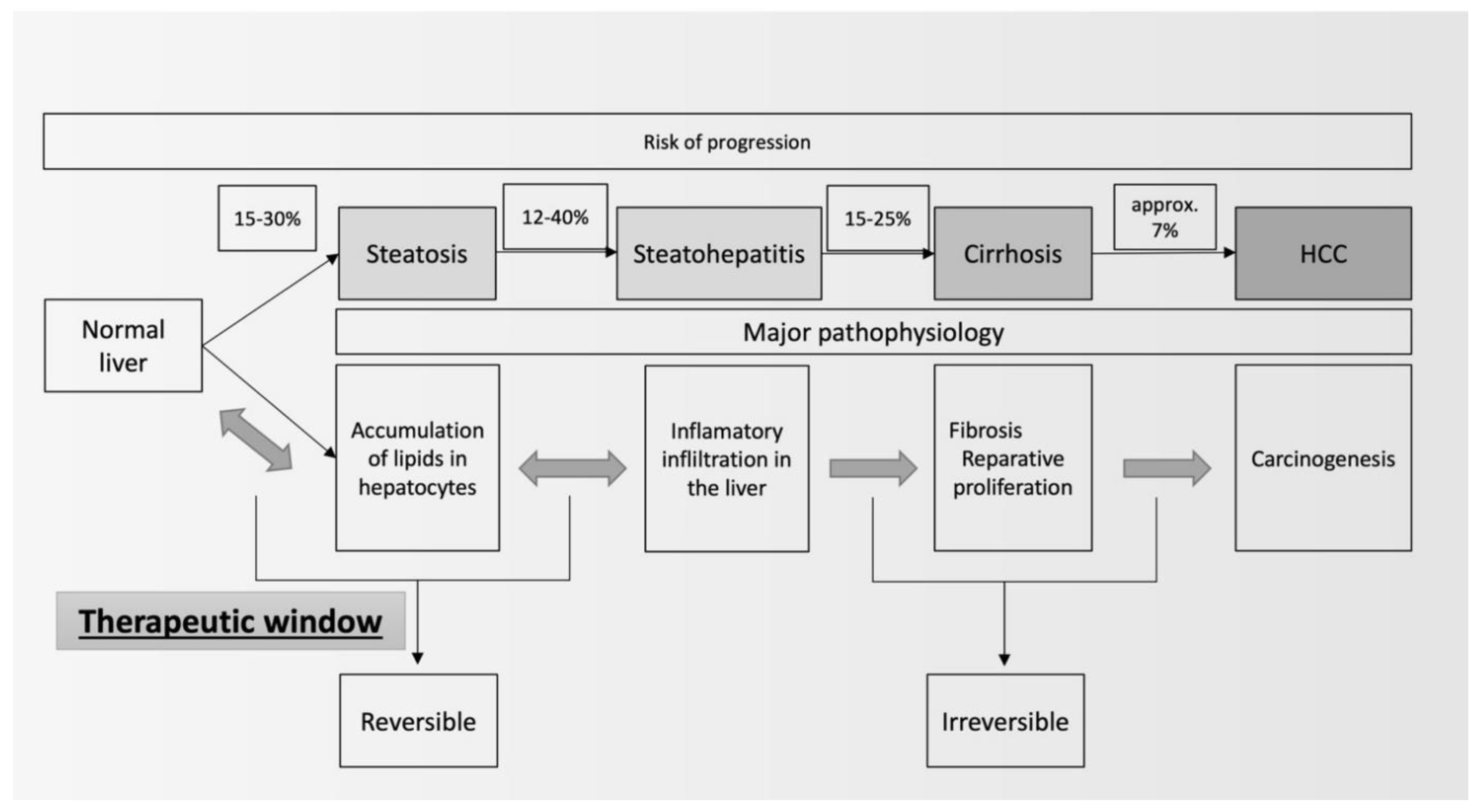
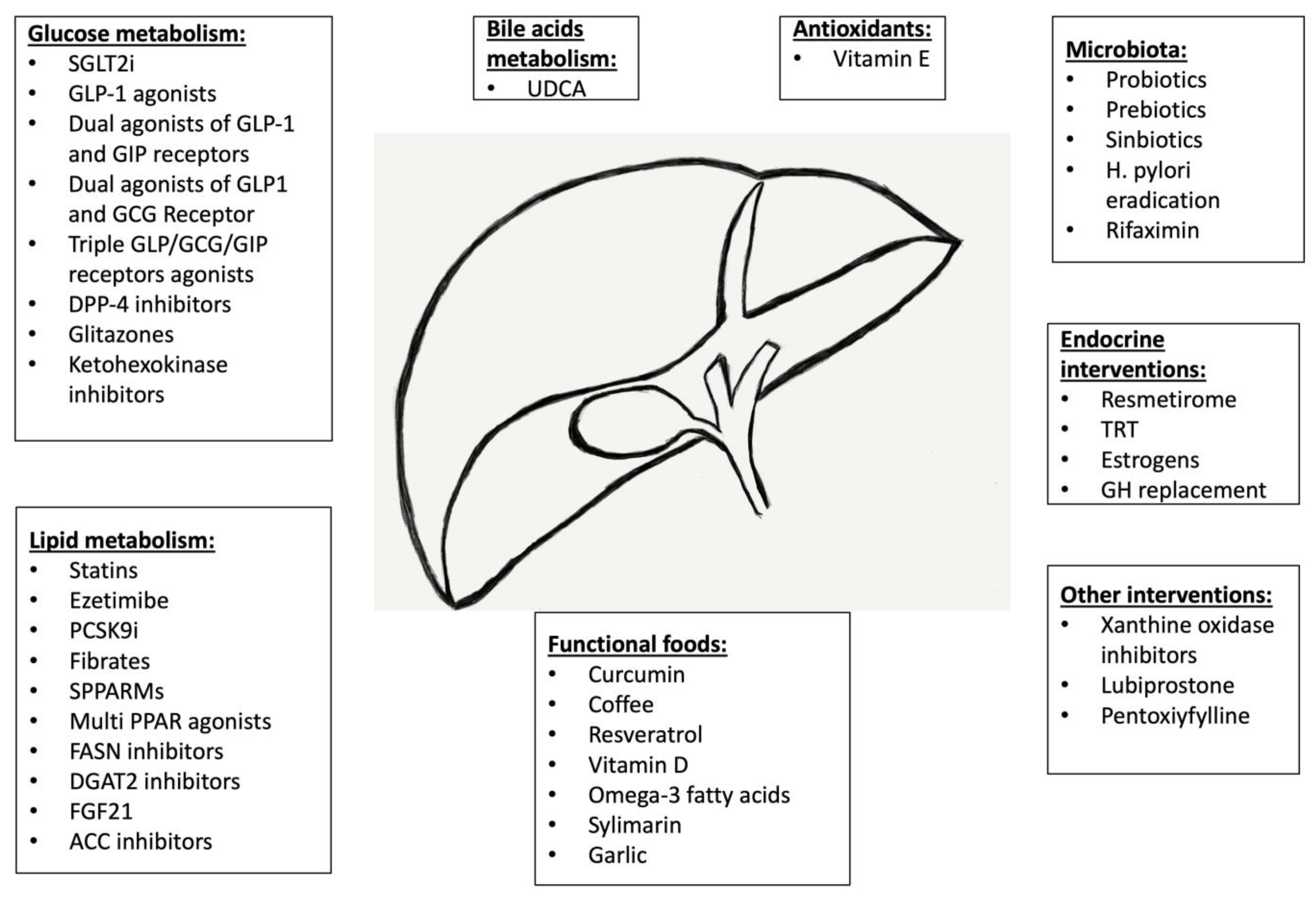
:1. Introduction
2. Therapeutic Lifestyle Changes
3. Drugs Affecting Carbohydrate Metabolism
3.1. Sodium/Glucose Cotransporter-2 Inhibitors
3.2. Agonists of Glucagon-like Peptide-1 Receptors
3.3. Dual Agonists of Incretin Receptors (Glucagon-like Peptide-1 and Glucose-Dependent Insulinotropic Polypeptide)
3.4. Dual Agonists of Incretin Receptors (Glucagon-like Peptide-1 and Glucagon)
3.5. Triple Incretin Receptor Agonists
3.6. Dipeptidyl Peptidase-4 Inhibitors
3.7. Glitazones
3.8. Ketohexokinase Inhibitors
3.9. Metformin
4. Drugs Affecting Lipid Metabolism
4.1. Core Cholesterol-Lowering Therapy (Statins or/and Ezetimibe)
4.2. PCSK9 Inhibitors
4.3. Peroxisome Proliferator-Activated Receptors Alpha Agonists
4.4. Selective Peroxisome Proliferator-Activated Receptor Modulators
4.5. Multiple Peroxisome Proliferator-Activated Receptor Agonists
4.6. Acetyl-CoA Carboxylase Inhibitors
4.7. Fatty-acid Synthase Inhibitors
4.8. Diacylglycerol Acyltransferase Inhibitors
4.9. Fibroblast Growth Factor 21
5. The Role of Ursodeoxycholic Acid in Metabolic-Associated Fatty Liver Disease
6. The Role of the Microbiota in the Pathogenesis and Management of Metabolic-Associated Fatty Liver Disease
6.1. The Role of Helicobacter pylori in the Pathogenesis and Management of Metabolic-Associated Fatty Liver Disease
6.2. Modification of Microbiota
7. Antioxidants
Vitamin E (Alpha-Tocopherol)
8. Interactions between the Endocrine System and NAFLD
8.1. Thyroid Hormones
8.2. Testosterone
8.3. Estradiol
8.4. Growth Hormone
9. Other Therapies
9.1. Xanthine Oxidase Inhibitors
9.2. Lubiprostone
9.3. Pentoxifylline
9.4. Other Drugs
10. Functional Foods
10.1. Curcumin
10.2. Coffee
10.3. Resveratrol
10.4. Vitamin D
10.5. Omega-3 Fatty Acids
10.6. Silymarin
10.7. Garlic
11. Future Perspectives
- farnesoid X receptor agonists—obeticholic acid and tropifexor;
- a lipogenesis inhibitor—aramchol;
- a galectin 3 inhibitor—belapectin;
- an A3 adenosine receptor agonist—namodenoson;
- a fatty acid—icosabutate;
- a cyclophilin inhibitor—rencofilstat;
- a modified bile acid—non-ursodeoxycholic.
12. Summary
- Physical activity and modification of the diet are of the utmost importance;
- The strengthening of weight loss with pharmacotherapy (preferably with GLP-1 analogs) is advisable;
- The introduction of functional foods might improve MAFLD;
- The consideration of the use of pro/prebiotics—modification of microbiota (screening for H. pylori);
- The exclusion of hypothyroidism, hypogonadism, and GH deficiency;
- In patients with DMT2, a preference toward novel antidiabetic drugs, i.e., SGLT-2i and incretin-based therapies;
- In patients with lipid disorders, the use of lipid-lowering drugs should be encouraged, while the risk of liver damage seems not to be greater than that in patients without liver steatosis, and the potential beneficial effects on liver functions seem to be concurrent with cardiovascular benefits.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| AACE | American Association of Clinical Endocrinology |
| AASLD | American Association for the Study of Liver Diseases |
| ACC | Acetyl-CoA Carboxylase |
| ALEH | Latin American Association for the Study of the Liver |
| ALP | Alkaline Phosphate |
| ALT | Alanine Aminotransferase |
| AMPK | Adenosine 5’-Monophosphate |
| (AMP) | Activated Protein Kinase |
| AST | Aspartate Aminotransferase |
| BLBLIs | β-Lactam/β-Lactamase Inhibitor Combinations |
| BMI | Body-Mass Index |
| CAP | Controlled Attenuation Parameter |
| CK-18 | Cytokeratin-18 |
| CKD | Chronic Kidney Disease |
| CRF | Cardiorespiratory Fitness |
| CT | Computed Tomography |
| DGATs | Diacylglycerol Acyltransferases |
| DMT2 | Type 2 Diabetes Mellitus |
| DPP4i | Dipeptidyl Peptidase-4 inhibitor |
| EASD | European Association for the Study of Diabetes |
| EASL | European Association for the Study of the Liver |
| EASO | European Association for the Study of Obesity |
| FASN | Fatty-Acid Synthase |
| FGF-21 | Fibroblast Growth Factor 21 |
| FIB-4 | Fibrosis-4 Index |
| FLI | Fatty Liver Index |
| FNI | Fibrotic Nonalcoholic steatohepatitis Index |
| FXR | Farnesoid X Receptor |
| GCG | Glucagon |
| GCGR | Glucagon Receptor |
| GGT | Gamma-Glutamyl Transferase |
| GH | Growth Hormone |
| GIP | Glucose-Dependent Insulinotropic Peptide |
| GLP-1 | Glucagon-like Peptide-1 |
| GLP-1RA | GLP-1 Receptor Agonists |
| HCC | Hepatocellular Carcinoma |
| HDL | High-Density Lipoprotein |
| HF | Heart Failure |
| HIS | Intrahepatic Steatosis |
| HOMA-IR | Homeostasis Model Assessment of Insulin Resistance |
| IGF-1 | Insulin-like Growth Factor-1 |
| IHL | Intrahepatic Lipid |
| IL | Interleukin |
| KHKis | Ketohexokinase inhibitors |
| LAI | Liver Attenuation Index |
| LFC | Liver Fat Content |
| LFTs | Liver Function Tests |
| LPS | Lipopolysaccharides |
| LSM | Liver Stiffness Measurement |
| MAFLD | Metabolic-Associated Fatty Liver Disease |
| MASH | Metabolic Dysfunction-Associated Steatohepatitis |
| MASLD | Metabolic Dysfunction-Associated Steatotic Liver Disease |
| Met-ALD | Metabolic Alcohol-Related Liver Disease |
| MRI | Magnetic Resonance Imaging |
| MRI-PDFF | MRI-Proton Density Fat Fraction |
| mTOR | mammalian Target of Rapamycin |
| NAFIC score | NASH, Ferritin, Insulin, and type IV Collagen 7S score |
| NAFLD | Nonalcoholic Fatty Liver Disease |
| NAS | NAFLD Activity Score |
| NASH | Nonalcoholic Steatohepatitis |
| NFS | NAFLD Fibrosis Score |
| PCSK9i | inhibitor of Proprotein Convertase Subtilisin/Kexin 9 |
| PI13-AKT | Phosphatidylinositol 3 Kinase-protein Kinase B |
| PPAR 9 (α) alpha | Peroxisome Proliferator-Activated Receptors alpha |
| PPARγ | Peroxisome Proliferator-Activated Receptors gamma |
| Pro-C3 | N-terminal type III collagen propeptide |
| PUFA | Polyunsaturated Fatty Acid |
| RCT | Randomized Controlled Trial |
| SGLT-2 | Sodium-Glucose Cotransporter-2 |
| SGLT-2is | Sodium-Glucose Cotransporter-2 inhibitors |
| SHBG | Sex-Hormone Binding Protein |
| SLD | Steatotic Liver Disease |
| SPPARM | Selective Peroxisome Proliferator-Activated Receptor Modulators |
| SUCRA | Surface Under the Cumulative Ranking Curve |
| SWV | Shear-Wave Velocity |
| TG | Triglyceride |
| TGF | Transforming Growth Factor |
| TLC | Therapeutic Lifestyle Change |
| TNF-alfa (α) | Tumor Necrosing Factor alpha |
| TRb | Thyroid Receptor beta |
| UDCA | Ursodeoxycholic Acid |
List of Clinical Trials
| CANVAS Study | Canagliflozin Cardiovascular Assessment Study |
| CREDENCE Study | Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation |
| DAPA-CKD Study | Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease Study |
| DAPA-HF Study | Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure Study |
| E-LIFT Study | EndoBarrier(R) in Diabetes Trial |
| EMPEROR-Preserved Study | EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure with Preserved Ejection Fraction |
| EMPEROR-Reduced Study | EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure with Reduced Ejection Fraction |
| ENLIVEN Study | Study Evaluating the Safety, Efficacy and Tolerability of BIO89-100 in Subject with Biopsy-confirmed Nonalcoholic Steatohepatitis (NASH) |
| ESSENTIAL Study | Efficacy and Safety of Sparsentan in Patients with IgA Nephropathy |
| FALCON program | Two phase 2b randomized, double-blind, placebo-controlled studies to assess the efficacy and safety of pegbelfermin in the treatment of patients with nonalcoholic steatohepatitis and bridging fibrosis or compensated cirrhosis |
| FASCINATE–1 Study | TVB-2640 (FASN inhibitor) for the Treatment of Nonalcoholic Steatohepatitis |
| GRAECE Study | Greek Atorvastatin and Coronary-heart-disease Evaluation Study |
| LEAN Study | The Liraglutide Efficacy and Action in NASH |
| LUBIPRONE Study | Efficacy, safety, and tolerability of lubiprostone for the treatment of nonalcoholic fatty liver disease in adult patients with constipation: The LUBIPRONE, double-blind, randomized, placebo-controlled study design |
| MIRNA Study | Metabolic Interventions to Resolve NASH with fibrosis |
| MOMENTUM Obesity Trials | Multi-center, Randomized, Double-blind, Placebo-controlled, Parallel-group Studies Evaluating the Safety and Efficacy of Investigational Agents in Obese or Overweight Adult Participants |
| PIVENS Trial | Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis |
| SURPASS-3 MRI Study | Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomized, open-label, parallel-group, phase 3 SURPASS-3 trial |
| SURPASS-3 Trial | Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomized, open-label, parallel-group, phase 3 trial |
| SYNERGY-NAS Trial | A Study of Tirzepatide (LY3298176) in Participants with Nonalcoholic Steatohepatitis (NASH) |
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 2023, 2023, 101133. [Google Scholar] [CrossRef]
- Lieverse, R.J.; Jansen, J.B.M.J.; Masclee, A.A.M.; Lamers, C.B.H.W. Gastrointestinal Disturbances with Obesity. Scand. J. Gastroenterol. 1993, 28, 53–58. [Google Scholar] [CrossRef]
- Grgurevic, I.; Podrug, K.; Mikolasevic, I.; Kukla, M.; Madir, A.; Tsochatzis, E.A. Natural History of Nonalcoholic Fatty Liver Disease: Implications for Clinical Practice and an Individualized Approach. Can. J. Gastroenterol. Hepatol. 2020, 2020, 9181368. [Google Scholar] [CrossRef] [PubMed]
- Basha, A.; May, S.C.; Anderson, R.M.; Samala, N.; Mirmira, R.G. Non-Alcoholic Fatty Liver Disease: Translating Disease Mechanisms into Therapeutics Using Animal Models. Int. J. Mol. Sci. 2023, 24, 9996. [Google Scholar] [CrossRef]
- Fernández, T.; Viñuela, M.; Vidal, C.; Barrera, F. Lifestyle changes in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0263931. [Google Scholar] [CrossRef]
- Kim, H.; Lee, D.S.; An, T.H.; Park, H.-J.; Kim, W.K.; Bae, K.-H.; Oh, K.-J. Metabolic Spectrum of Liver Failure in Type 2 Diabetes and Obesity: From NAFLD to NASH to HCC. Int. J. Mol. Sci. 2021, 22, 4495. [Google Scholar] [CrossRef]
- Basu, R.; Noureddin, M.; Clark, J.M. Nonalcoholic Fatty Liver Disease: Review of Management for Primary Care Providers. Mayo Clin. Proc. 2022, 97, 1700–1716. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Mátis, D.; Hegyi, P.; Teutsch, B.; Tornai, T.; Erőss, B.; Pár, G.; Váncsa, S. Improved body composition decreases the fat content in non-alcoholic fatty liver disease, a meta-analysis and systematic review of longitudinal studies. Front. Med. 2023, 10, 1114836. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef]
- Barrón-Cabrera, E.; Soria-Rodríguez, R.; Amador-Lara, F.; Martínez-López, E. Physical Activity Protocols in Non-Alcoholic Fatty Liver Disease Management: A Systematic Review of Randomized Clinical Trials and Animal Models. Healthcare 2023, 11, 1992. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-T.; Zheng, J.; Peng, H.-W.; Cai, X.-L.; Pan, X.-T.; Li, H.-Q.; Hong, Q.-Z.; Peng, X.-E. Physical activity intervention for non-diabetic patients with non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. BMC Gastroenterol. 2020, 20, 66. [Google Scholar] [CrossRef]
- Xiong, Y.; Peng, Q.; Cao, C.; Xu, Z.; Zhang, B. Effect of Different Exercise Methods on Non-Alcoholic Fatty Liver Disease: A Meta-Analysis and Meta-Regression. Int. J. Env. Res. Public. Health 2021, 18, 3242. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Barazzoni, R.; Busetto, L.; Campmans-Kuijpers, M.; Cardinale, V.; Chermesh, I.; Eshraghian, A.; Kani, H.T.; Khannoussi, W.; Lacaze, L.; et al. European guideline on obesity care in patients with gastrointestinal and liver diseases—Joint ESPEN/UEG guideline. Clin. Nutr. 2022, 41, 2364–2405. [Google Scholar] [CrossRef]
- Gofton, C.; Upendran, Y.; Zheng, M.-H.; George, J. MAFLD: How is it different from NAFLD? Clin. Mol. Hepatol. 2023, 29, S17–S31. [Google Scholar] [CrossRef] [PubMed]
- Hazlehurst, J.M.; Tomlinson, J.W. Mechanisms in endocrinology: Non-alcoholic fatty liver disease in common endocrine disorders. Eur. J. Endocrinol. 2013, 169, R27–R37. [Google Scholar] [CrossRef]
- Ranjbar, G.; Mikhailidis, D.P.; Sahebkar, A. Effects of newer antidiabetic drugs on nonalcoholic fatty liver and steatohepatitis: Think out of the box! Metabolism 2019, 101, 154001. [Google Scholar] [CrossRef]
- Rieg, T.; Vallon, V. Development of SGLT1 and SGLT2 inhibitors. Diabetologia 2018, 61, 2079–2086. [Google Scholar] [CrossRef]
- Jasleen, B.; Vishal, G.K.; Sameera, M.; Fahad, M.; Brendan, O.; Deion, S.; Pemminati, S. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors: Benefits Versus Risk. Cureus 2023, 15, 1–11. [Google Scholar] [CrossRef]
- Van Der Aart-van Der Beek, A.B.; De Boer, R.A.; Heerspink, H.J.L. Kidney and heart failure outcomes associated with SGLT2 inhibitor use. Nat. Rev. Nephrol. 2022, 18, 294–306. [Google Scholar] [CrossRef]
- Nasiri-Ansari, N.; Nikolopoulou, C.; Papoutsi, K.; Kyrou, I.; Mantzoros, C.S.; Kyriakopoulos, G.; Chatzigeorgiou, A.; Kalotychou, V.; Randeva, M.S.; Chatha, K.; et al. Empagliflozin Attenuates Non-Alcoholic Fatty Liver Disease (NAFLD) in High Fat Diet Fed ApoE(-/-) Mice by Activating Autophagy and Reducing ER Stress and Apoptosis. Int. J. Mol. Sci. 2021, 22, 818. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, H.H.; Alzaim, I.; El-Mallah, A.; Aly, R.G.; El-Yazbi, A.F.; Wahid, A. Metformin, pioglitazone, dapagliflozin and their combinations ameliorate manifestations associated with NAFLD in rats via anti-inflammatory, anti-fibrotic, anti-oxidant and anti-apoptotic mechanisms. Life Sci. 2022, 308, 120956. [Google Scholar] [CrossRef]
- Sun, L.; Deng, C.; Gu, Y.; He, Y.; Yang, L.; Shi, J. Effects of dapagliflozin in patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis of randomized controlled trials. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101876. [Google Scholar] [CrossRef] [PubMed]
- Bellanti, F.; Buglio, A.L.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Aich, P.; Singh, S.P.; Serviddio, G.; Vendemiale, G. Impact of sodium glucose cotransporter-2 inhibitors on liver steatosis/fibrosis/inflammation and redox balance in non-alcoholic fatty liver disease. WJG 2022, 28, 3243–3257. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.; Zhang, H.; Wang, X. Efficacy and Safety of Empagliflozin on Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2022, 13, 836455. [Google Scholar] [CrossRef]
- Gu, Y.; Sun, L.; Zhang, W.; Kong, T.; Zhou, R.; He, Y.; Deng, C.; Yang, L.; Kong, J.; Chen, Y.; et al. Comparative efficacy of 5 sodium-glucose cotransporter protein-2 (SGLT-2) inhibitor and 4 glucagon-like peptide-1 (GLP-1) receptor agonist drugs in non-alcoholic fatty liver disease: A GRADE-assessed systematic review and network meta-analysis of randomized controlled trials. Front. Pharmacol. 2023, 14, 1102792. [Google Scholar] [CrossRef] [PubMed]
- Phrueksotsai, S.; Pinyopornpanish, K.; Euathrongchit, J.; Leerapun, A.; Phrommintikul, A.; Buranapin, S.; Chattipakorn, N.; Thongsawat, S. The effects of dapagliflozin on hepatic and visceral fat in type 2 diabetes patients with non-alcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2021, 36, 2952–2959. [Google Scholar] [CrossRef] [PubMed]
- Borisov, A.N.; Kutz, A.; Christ, E.R.; Heim, M.H.; Ebrahimi, F. Canagliflozin and Metabolic Associated Fatty Liver Disease in Patients with Diabetes Mellitus: New Insights From CANVAS. J. Clin. Endocrinol. Metab. 2023, dgad249, online ahead of print. [Google Scholar] [CrossRef]
- Arai, T.; Atsukawa, M.; Tsubota, A.; Mikami, S.; Haruki, U.; Yoshikata, K.; Ono, H.; Kawano, T.; Yoshida, Y.; Tanabe, T.; et al. Antifibrotic effect and long-term outcome of SGLT2 inhibitors in patients with NAFLD complicated by diabetes mellitus. Hepatol. Commun. 2022, 6, 3073–3082. [Google Scholar] [CrossRef]
- Buldak, L.; Machnik, G.; Skudrzyk, E.; Boldys, A.; Maliglowka, M.; Kosowski, M.; Basiak, M.; Buldak, R.J.; Okopien, B. Exenatide prevents statin-related LDL receptor increase and improves insulin secretion in pancreatic beta cells (1.1E7) in a protein kinase A-dependent manner. J. Appl. Biomed. 2022, 20, 130–140. [Google Scholar] [CrossRef]
- Bułdak, Ł.; Skudrzyk, E.; Machnik, G.; Bołdys, A.; Bułdak, R.J.; Okopień, B. Exenatide improves antioxidant capacity and reduces the expression of LDL receptors and PCSK9 in human insulin-secreting 1.1E7 cell line subjected to hyperglycemia and oxidative stress. Postępy Hig. I Med. Doświadczalnej 2022, 76, 16–23. [Google Scholar] [CrossRef]
- Bułdak, Ł.; Machnik, G.; Skudrzyk, E.; Bołdys, A.; Okopień, B. The impact of exenatide (a GLP-1 agonist) on markers of inflammation and oxidative stress in normal human astrocytes subjected to various glycemic conditions. Exp. Ther. Med. 2019, 17, 2861–2869. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; Abouda, G.; Aldersley, M.A.; et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): A multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef]
- Study of Semaglutide for Non-Alcoholic Fatty Liver Disease (NAFLD), a Metabolic Syndrome With Insulin Resistance, Increased Hepatic Lipids, and Increased Cardiovascular Disease Risk (The SLIM LIVER Study). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04216589 (accessed on 10 August 2023).
- Non-Alcoholic Fatty Liver Disease, the HEpatic Response to Oral Glucose, and the Effect of Semaglutide (NAFLD HEROES). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT03884075 (accessed on 10 August 2023).
- Semaglutide in Nonalcoholic Fatty Liver Disease. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05813249 (accessed on 10 August 2023).
- A Multiple Dose Study of LY3502970 in Healthy Overweight and Obese Participants. Available online: https://ichgcp.net/clinical-trials-registry/NCT05841238 (accessed on 11 August 2023).
- A Study of LY3502970 in Participants With Obesity or Overweight With Weight-related Comorbidities. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05051579 (accessed on 11 August 2023).
- Pratt, E.; Ma, X.; Liu, R.; Robins, D.; Coskun, T.; Sloop, K.W.; Haupt, A.; Benson, C. Orforglipron (LY3502970), a novel, oral non-peptide glucagon-like peptide-1 receptor agonist: A Phase 1b, multicentre, blinded, placebo-controlled, randomized, multiple-ascending-dose study in people with type 2 diabetes. Diabetes Obes. Metab. 2023, 25, 2642–2649. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K.; Isaacs, S.; Barb, D.; Basu, R.; Caprio, S.; Garvey, W.T.; Kashyap, S.; Mechanick, J.I.; Mouzaki, M.; Nadolsky, K.; et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings. Endocr. Pract. 2022, 28, 528–562. [Google Scholar] [CrossRef]
- El, K.; Douros, J.D.; Willard, F.S.; Novikoff, A.; Sargsyan, A.; Perez-Tilve, D.; Wainscott, D.B.; Yang, B.; Chen, A.; Wothe, D.; et al. The incretin co-agonist tirzepatide requires GIPR for hormone secretion from human islets. Nat. Metab. 2023, 5, 945–954. [Google Scholar] [CrossRef]
- Thomas, M.K.; Nikooienejad, A.; Bray, R.; Cui, X.; Wilson, J.; Duffin, K.; Milicevic, Z.; Haupt, A.; Robins, D.A. Dual GIP and GLP-1 Receptor Agonist Tirzepatide Improves Beta-cell Function and Insulin Sensitivity in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2021, 106, 388–396. [Google Scholar] [CrossRef]
- A Study of Tirzepatide (LY3298176) in Participants With Nonalcoholic Steatohepatitis (NASH) (SYNERGY-NASH). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04166773 (accessed on 11 August 2023).
- Hartman, M.L.; Sanyal, A.J.; Loomba, R.; Wilson, J.M.; Nikooienejad, A.; Bray, R.; Karanikas, C.A.; Duffin, K.L.; Robins, D.A.; Haupt, A. Effects of Novel Dual GIP and GLP-1 Receptor Agonist Tirzepatide on Biomarkers of Nonalcoholic Steatohepatitis in Patients With Type 2 Diabetes. Diabetes Care 2020, 43, 1352–1355. [Google Scholar] [CrossRef]
- Gastaldelli, A.; Cusi, K.; Fernández Landó, L.; Bray, R.; Brouwers, B.; Rodríguez, Á. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): A substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes Endocrinol. 2022, 10, 393–406. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Lawitz, E.; Shankar, R.R.; Chaudhri, E.; Liu, J.; Lam, R.L.H.; Kaufman, K.D.; Engel, S.S.; Bruzone, S.O.; Coronel, M.J.; et al. A phase IIa active-comparator-controlled study to evaluate the efficacy and safety of efinopegdutide in patients with non-alcoholic fatty liver disease. J. Hepatol. 2023, 79, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Nahra, R.; Wang, T.; Gadde, K.M.; Oscarsson, J.; Stumvoll, M.; Jermutus, L.; Hirshberg, B.; Ambery, P. Effects of Cotadutide on Metabolic and Hepatic Parameters in Adults With Overweight or Obesity and Type 2 Diabetes: A 54-Week Randomized Phase 2b Study. Diabetes Care 2021, 44, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- A Study to Evaluate the Safety and Efficacy of Cotadutide Given by Subcutaneous Injection in Adult Participants with Non-cirrhotic Non-alcoholic Steatohepatitis With Fibrosis. (PROXYMO-ADV). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05364931 (accessed on 12 August 2023).
- Harrison, S.A.; Loomba, R.; Dubourg, J.; Ratziu, V.; Noureddin, M. Clinical Trial Landscape in NASH. Clin. Gastroenterol. Hepatol. 2023, 21, 2001–2014. [Google Scholar] [CrossRef] [PubMed]
- ALT-801 in Diabetic and Non-Diabetic Overweight and Obese Subjects with Non-alcoholic Fatty Liver Disease (NAFLD). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05006885 (accessed on 12 August 2023).
- Extension of ALT-801 in Diabetic and Non-Diabetic Overweight and Obese Subjects with (NAFLD). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05292911 (accessed on 12 August 2023).
- Prikhodko, V.A.; Bezborodkina, N.N.; Okovityi, S.V. Pharmacotherapy for Non-Alcoholic Fatty Liver Disease: Emerging Targets and Drug Candidates. Biomedicines 2022, 10, 274. [Google Scholar] [CrossRef] [PubMed]
- HM14320. Available online: https://adisinsight.springer.com/drugs/800053783 (accessed on 12 August 2023).
- A Study to Test Safety and Efficacy of BI456906 in Adults with Non-alcoholic Steatohepatitis (NASH) and Fibrosis (F1-F3). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04771273 (accessed on 12 August 2023).
- A Study to Evaluate the Efficacy and Safety of PF-06882961 in Adults with Obesity. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04707313 (accessed on 12 August 2023).
- Study to Evaluate Efficacy, Safety and Tolerability of HM15211 in Subjects. Available online: https://clinicaltrials.gov/study/NCT04505436 (accessed on 12 August 2023).
- A Study of Multiple Doses of HM15211 in Obese Subjects with NAFLD. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT03744182 (accessed on 12 August 2023).
- A Study of LY3437943 in Participants Who Have Obesity or Are Overweight. Available online: https://clinicaltrials.gov/study/NCT04881760 (accessed on 12 August 2023).
- Jastreboff, A.M.; Kaplan, L.M.; Frías, J.P.; Wu, Q.; Du, Y.; Gurbuz, S.; Coskun, T.; Haupt, A.; Milicevic, Z.; Hartman, M.L. Triple–Hormone-Receptor Agonist Retatrutide for Obesity—A Phase 2 Trial. N. Engl. J. Med. 2023, 389, 514–526. [Google Scholar] [CrossRef]
- Kongmalai, T.; Srinonprasert, V.; Anothaisintawee, T.; Kongmalai, P.; McKay, G.; Attia, J.; Thakkinstian, A. New anti-diabetic agents for the treatment of non-alcoholic fatty liver disease: A systematic review and network meta-analysis of randomized controlled trials. Front. Endocrinol. 2023, 14, 1182037. [Google Scholar] [CrossRef]
- Valenzuela-Vallejo, L.; Guatibonza-García, V.; Mantzoros, C.S. Recent guidelines for Non-Alcoholic Fatty Liver disease (NAFLD)/ Fatty Liver Disease (FLD): Are they already outdated and in need of supplementation? Metabolism 2022, 136, 155248. [Google Scholar] [CrossRef]
- Dos Santos, L.R.; Duarte, M.L.; Peccin, M.S.; Gagliardi, A.R.D.T.; Melnik, T. Dipeptidyl Peptidase IV Inhibitors for Nonalcoholic Fatty Liver Disease—Systematic Review and Metanalysis. CDR 2021, 17, e101120187811. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Ghosh, J.; Mustafa, G.; Kamal, M.; Ahmad, N. Effect of sitagliptin on hepatic histological activity and fibrosis of nonalcoholic steatohepatitis patients: A 1-year randomized control trial. HMER 2018, 10, 23–31. [Google Scholar] [CrossRef]
- Aktaş, A.; Ozan, Z. The Efficacy and safety of vildagliptin treatment for nonalcoholic fatty liver disease in type 2 diabetes mellitus. Cumhur. Med. J. 2020, 42, 491–499. [Google Scholar] [CrossRef]
- Jin, D.; Cui, Z.; Jin, S.; Zhou, T.; Guo, B.; Gao, P.; Li, G. Comparison of efficacy of anti-diabetics on non-diabetic NAFLD: A network meta-analysis. Front. Pharmacol. 2023, 13, 1096064. [Google Scholar] [CrossRef]
- Hattori, S.; Nomoto, K.; Suzuki, T.; Hayashi, S. Beneficial effect of omarigliptin on diabetic patients with non-alcoholic fatty liver disease/non-alcoholic steatohepatitis. Diabetol. Metab. Syndr. 2021, 13, 28. [Google Scholar] [CrossRef]
- Gupta, V.K. 1029-P: Teneligliptin Significantly Reduces Liver Fat Content (LFC) and Delays Progression of NASH in Type 2 Diabetes Mellitus Patients. Diabetes 2019, 68 (Suppl. S1), 1029-P. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, X.; Zhang, L.; Zheng, D. Effect of Saxagliptin, a Dipeptidyl Peptidase 4 Inhibitor, on Non-Alcoholic Fatty Liver Disease. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 3507–3518. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-J.; Zhang, P.; Fan, B.; Guo, X.-L.; Zheng, Z.-S. The efficacy of saxagliptin in T2DM patients with non-alcoholic fatty liver disease: Preliminary data. Rev. Assoc. Med. Bras. 2019, 65, 33–37. [Google Scholar] [CrossRef]
- Mashitani, T.; Noguchi, R.; Okura, Y.; Namisaki, T.; Mitoro, A.; Ishii, H.; Nakatani, T.; Kikuchi, E.; Moriyasu, H.; Matsumoto, M.; et al. Efficacy of alogliptin in preventing non-alcoholic fatty liver disease progression in patients with type 2 diabetes. Biomed. Rep. 2016, 4, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef] [PubMed]
- Aithal, G.P.; Thomas, J.A.; Kaye, P.V.; Lawson, A.; Ryder, S.D.; Spendlove, I.; Austin, A.S.; Freeman, J.G.; Morgan, L.; Webber, J. Randomized, Placebo-Controlled Trial of Pioglitazone in Nondiabetic Subjects with Nonalcoholic Steatohepatitis. Gastroenterology 2008, 135, 1176–1184. [Google Scholar] [CrossRef]
- Belfort, R.; Harrison, S.A.; Brown, K.; Darland, C.; Finch, J.; Hardies, J.; Balas, B.; Gastaldelli, A.; Tio, F.; Pulcini, J.; et al. A Placebo-Controlled Trial of Pioglitazone in Subjects with Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2006, 355, 2297–2307. [Google Scholar] [CrossRef]
- Cusi, K.; Orsak, B.; Bril, F.; Lomonaco, R.; Hecht, J.; Ortiz-Lopez, C.; Tio, F.; Hardies, J.; Darland, C.; Musi, N.; et al. Long-Term Pioglitazone Treatment for Patients With Nonalcoholic Steatohepatitis and Prediabetes or Type 2 Diabetes Mellitus: A Randomized Trial. Ann. Intern. Med. 2016, 165, 305. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; Biernacki, D.M.; Kalavalapalli, S.; Lomonaco, R.; Subbarayan, S.K.; Lai, J.; Tio, F.; Suman, A.; Orsak, B.K.; Hecht, J.; et al. Role of Vitamin E for Nonalcoholic Steatohepatitis in Patients With Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2019, 42, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.; Russo, M.; Vitale, M.; Carli, F.; Vetrani, C.; Masulli, M.; Riccardi, G.; Vaccaro, O.; Gastaldelli, A.; Rivellese, A.A.; et al. Pioglitazone even at low dosage improves NAFLD in type 2 diabetes: Clinical and pathophysiological insights from a subgroup of the TOSCA.IT randomised trial. Diabetes Res. Clin. Pract. 2021, 178, 108984. [Google Scholar] [CrossRef] [PubMed]
- Ndakotsu, A.; Vivekanandan, G. The Role of Thiazolidinediones in the Amelioration of Nonalcoholic Fatty Liver Disease: A Systematic Review. Cureus 2022, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- A 24 Week, Multicenter, Prospective, Open-labeled, Single-arm, Exploratory Phase 4 Clinical Trial to Evaluate the Safety and Efficacy of Lobeglitazone in Decreasing Intrahepatic Fat Contents in Type 2 Diabetes with NAFLD. Available online: https://classic.clinicaltrials.gov/ct2/show/results/NCT02285205?view=results (accessed on 30 August 2023).
- Lee, Y.; Kim, J.H.; Kim, S.R.; Jin, H.Y.; Rhee, E.-J.; Cho, Y.M.; Lee, B.-W. Lobeglitazone, a Novel Thiazolidinedione, Improves Non-Alcoholic Fatty Liver Disease in Type 2 Diabetes: Its Efficacy and Predictive Factors Related to Responsiveness. J. Korean Med. Sci. 2017, 32, 60. [Google Scholar] [CrossRef]
- Kazierad, D.J.; Chidsey, K.; Somayaji, V.R.; Bergman, A.J.; Birnbaum, M.J.; Calle, R.A. Inhibition of ketohexokinase in adults with NAFLD reduces liver fat and inflammatory markers: A randomized phase 2 trial. Med 2021, 2, 800–813.e3. [Google Scholar] [CrossRef]
- Saxena, A.R.; Lyle, S.; Khavandi, K.; Qiu, R.; Whitlock, M.; Esler, W.P.; Kim, A.M. A phase 2a, randomized, double-blind, placebo-controlled, three-arm, parallel-group study to assess the efficacy, safety, tolerability and pharmacodynamics of PF-06835919 in patients with non-alcoholic fatty liver disease and type 2 diabetes. Diabetes Obes. Metab. 2023, 25, 992–1001. [Google Scholar] [CrossRef] [PubMed]
- Ketohexokinase Inhibition in NAFLD (KHKi). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05463575 (accessed on 13 August 2023).
- Pinyopornpanish, K.; Leerapun, A.; Pinyopornpanish, K.; Chattipakorn, N. Effects of Metformin on Hepatic Steatosis in Adults with Nonalcoholic Fatty Liver Disease and Diabetes: Insights from the Cellular to Patient Levels. Gut Liver 2021, 15, 827–840. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, L.; Wang, B.; Wang, J.; Chen, D. Metformin in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Biomed. Rep. 2013, 1, 57–64. [Google Scholar] [CrossRef]
- Musso, G.; Cassader, M.; Rosina, F.; Gambino, R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of randomised trials. Diabetologia 2012, 55, 885–904. [Google Scholar] [CrossRef]
- Loomba, R.; Lutchman, G.; Kleiner, D.E.; Ricks, M.; Feld, J.J.; Borg, B.B.; Modi, A.; Nagabhyru, P.; Sumner, A.E.; Liang, T.J.; et al. Clinical trial: Pilot study of metformin for the treatment of non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2009, 29, 172–182. [Google Scholar] [CrossRef]
- Bugianesi, E.; Gentilcore, E.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; David, E.; Rizzetto, M.; Marchesini, G. A Randomized Controlled Trial of Metformin versus Vitamin E or Prescriptive Diet in Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2005, 100, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N. The Role of Cholesterol in the Pathogenesis of NASH. Trends Endocrinol. Metab. 2016, 27, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Bułdak, Ł. The treatment of heterozygous familial hypercholesterolemia—A local perspective. Endokrynol. Pol. 2021, 72, 189–190. [Google Scholar] [CrossRef] [PubMed]
- Okopień, B.; Bułdak, Ł.; Bołdys, A. Current and future trends in the lipid lowering therapy. Pharmacol. Rep. 2016, 68, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Boutari, C.; Pappas, P.D.; Anastasilakis, D.; Mantzoros, C.S. Statins’ efficacy in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Clin. Nutr. 2022, 41, 2195–2206. [Google Scholar] [CrossRef]
- Ahsan, F.; Oliveri, F.; Goud, H.K.; Mehkari, Z.; Mohammed, L.; Javed, M.; Althwanay, A.; Rutkofsky, I.H. Pleiotropic Effects of Statins in the Light of Non-Alcoholic Fatty Liver Disease and Non-Alcoholic Steatohepatitis. Cureus 2020, 12, 1–12. [Google Scholar] [CrossRef]
- Athyros, V.G.; Mikhailidis, D.P.; Didangelos, T.P.; Giouleme, O.I.; Liberopoulos, E.N.; Karagiannis, A.; Kakafika, A.I.; Tziomalos, K.; Burroughs, A.K.; Elisaf, M.S. Effect of multifactorial treatment on non-alcoholic fatty liver disease in metabolic syndrome: A randomised study. Curr. Med. Res. Opin. 2006, 22, 873–883. [Google Scholar] [CrossRef]
- Athyros, V.G.; Tziomalos, K.; Gossios, T.D.; Griva, T.; Anagnostis, P.; Kargiotis, K.; Pagourelias, E.D.; Theocharidou, E.; Karagiannis, A.; Mikhailidis, D.P. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: A post-hoc analysis. Lancet 2010, 376, 1916–1922. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Rhee, H.; Kim, Y.; Lee, M.; Lee, B.-W.; Kang, E.S.; Cha, B.-S.; Choi, J.-Y.; Lee, Y. Ezetimibe combination therapy with statin for non-alcoholic fatty liver disease: An open-label randomized controlled trial (ESSENTIAL study). BMC Med. 2022, 20, 93. [Google Scholar] [CrossRef]
- Lee, W.M.; Bae, J.H.; Chang, Y.; Lee, S.H.; Moon, J.E.; Jeong, S.W.; Jang, J.Y.; Kim, S.G.; Kim, H.S.; Yoo, J.-J.; et al. Effect of Nutrition Education in NAFLD Patients Undergoing Simultaneous Hyperlipidemia Pharmacotherapy: A Randomized Controlled Trial. Nutrients 2021, 13, 4453. [Google Scholar] [CrossRef]
- Lee, H.Y.; Jun, D.W.; Kim, H.J.; Oh, H.; Saeed, W.K.; Ahn, H.; Cheung, R.C.; Nguyen, M.H. Ezetimibe decreased nonalcoholic fatty liver disease activity score but not hepatic steatosis. Korean J. Intern. Med. 2019, 34, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Pani, A.; Di Rocco, A.; Menichelli, D.; Gazzaniga, G.; Farcomeni, A.; D’Erasmo, L.; Angelico, F.; Del Ben, M.; Baratta, F. Statin liver safety in non-alcoholic fatty liver disease: A systematic review and metanalysis. Brit J. Clin. Pharma 2022, 88, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Fu, S.; Liu, D.; Wang, Y.; Tan, Y. Statin can reduce the risk of hepatocellular carcinoma among patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2023, 35, 353–358. [Google Scholar] [CrossRef]
- Wargny, M.; Ducluzeau, P.-H.; Petit, J.-M.; Le May, C.; Smati, S.; Arnaud, L.; Pichelin, M.; Bouillet, B.; Lannes, A.; Blanchet, O.; et al. Circulating PCSK9 levels are not associated with the severity of hepatic steatosis and NASH in a high-risk population. Atherosclerosis 2018, 278, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, M.; Vokaer, B.; Seidah, N.G. A case of hypocholesterolemia and steatosis in a carrier of a PCSK9 loss-of-function mutation and polymorphisms predisposing to nonalcoholic fatty liver disease. J. Clin. Lipidol. 2017, 11, 1101–1105. [Google Scholar] [CrossRef]
- Emma, M.R.; Giannitrapani, L.; Cabibi, D.; Porcasi, R.; Pantuso, G.; Augello, G.; Giglio, R.V.; Re, N.L.; Capitano, A.R.; Montalto, G.; et al. Hepatic and circulating levels of PCSK9 in morbidly obese patients: Relation with severity of liver steatosis. Biochim. Et. Biophys. Acta (BBA) Mol. Cell Biol. Lipids 2020, 1865, 158792. [Google Scholar] [CrossRef] [PubMed]
- Grimaudo, S.; Bartesaghi, S.; Rametta, R.; Marra, F.; Margherita Mancina, R.; Pihlajamäki, J.; Kakol-Palm, D.; Andréasson, A.; Dongiovanni, P.; Ludovica Fracanzani, A.; et al. PCSK9 rs11591147 R46L loss-of-function variant protects against liver damage in individuals with NAFLD. Liver Int. 2021, 41, 321–332. [Google Scholar] [CrossRef]
- Scicali, R.; Di Pino, A.; Urbano, F.; Ferrara, V.; Marchisello, S.; Di Mauro, S.; Scamporrino, A.; Filippello, A.; Rabuazzo, A.M.; Purrello, F.; et al. Analysis of steatosis biomarkers and inflammatory profile after adding on PCSK9 inhibitor treatment in familial hypercholesterolemia subjects with nonalcoholic fatty liver disease: A single lipid center real-world experience. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 869–879. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, M.; Walmann, T.; Nutalapati, V.; Gibson, C.; Zafar, Y. Effects of proprotein convertase subtilisin/kexin type-9 inhibitors on fatty liver. World J. Hepatol. 2020, 12, 1258–1266. [Google Scholar] [CrossRef]
- El-Haggar, S.M.; Mostafa, T.M. Comparative clinical study between the effect of fenofibrate alone and its combination with pentoxifylline on biochemical parameters and liver stiffness in patients with non-alcoholic fatty liver disease. Hepatol. Int. 2015, 9, 471–479. [Google Scholar] [CrossRef]
- Yaghoubi, M.; Jafari, S.; Sajedi, B.; Gohari, S.; Akbarieh, S.; Heydari, A.H.; Jameshoorani, M. Comparison of fenofibrate and pioglitazone effects on patients with nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1385–1388. [Google Scholar] [CrossRef]
- Oscarsson, J.; Önnerhag, K.; Risérus, U.; Sundén, M.; Johansson, L.; Jansson, P.-A.; Moris, L.; Nilsson, P.M.; Eriksson, J.W.; Lind, L. Effects of free omega-3 carboxylic acids and fenofibrate on liver fat content in patients with hypertriglyceridemia and non-alcoholic fatty liver disease: A double-blind, randomized, placebo-controlled study. J. Clin. Lipidol. 2018, 12, 1390–1403. [Google Scholar] [CrossRef]
- Lawitz, E.J.; Bhandari, B.R.; Ruane, P.J.; Kohli, A.; Harting, E.; Ding, D.; Chuang, J.-C.; Huss, R.S.; Chung, C.; Myers, R.P.; et al. Fenofibrate Mitigates Hypertriglyceridemia in Nonalcoholic Steatohepatitis Patients Treated With Cilofexor/Firsocostat. Clin. Gastroenterol. Hepatol. 2023, 21, 143–152. [Google Scholar] [CrossRef]
- Araki, E.; Yamashita, S.; Arai, H.; Yokote, K.; Satoh, J.; Inoguchi, T.; Nakamura, J.; Maegawa, H.; Yoshioka, N.; Tanizawa, Y.; et al. Effects of Pemafibrate, a Novel Selective PPARα Modulator, on Lipid and Glucose Metabolism in Patients With Type 2 Diabetes and Hypertriglyceridemia: A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Trial. Diabetes Care 2018, 41, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, S.; Sugihara, T.; Hoshino, Y.; Matsuki, Y.; Nagahara, T.; Okano, J.; Kitao, S.; Fujioka, Y.; Yamamoto, K.; Isomoto, H. Pemafibrate Dramatically Ameliorated the Values of Liver Function Tests and Fibrosis Marker in Patients with Non-Alcoholic Fatty Liver Disease. Yonago Acta Med. 2020, 63, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Seko, Y.; Yamaguchi, K.; Umemura, A.; Yano, K.; Takahashi, A.; Okishio, S.; Kataoka, S.; Okuda, K.; Moriguchi, M.; Okanoue, T.; et al. Effect of pemafibrate on fatty acid levels and liver enzymes in non-alcoholic fatty liver disease patients with dyslipidemia: A single-arm, pilot study. Hepatol. Res. 2020, 50, 1328–1336. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, S.; Tahara, T.; Lefor, A.K.; Ogura, M. Pemafibrate decreases markers of hepatic inflammation in patients with non-alcoholic fatty liver disease. Clin. Exp. Hepatol. 2020, 6, 270–274. [Google Scholar] [CrossRef]
- Hatanaka, T.; Kakizaki, S.; Saito, N.; Nakano, Y.; Nakano, S.; Hazama, Y.; Yoshida, S.; Hachisu, Y.; Tanaka, Y.; Kashiwabara, K.; et al. Impact of Pemafibrate in Patients with Hypertriglyceridemia and Metabolic Dysfunction-associated Fatty Liver Disease Pathologically Diagnosed with Non-alcoholic Steatohepatitis: A Retrospective, Single-arm Study. Intern. Med. 2021, 60, 2167–2174. [Google Scholar] [CrossRef]
- Shinozaki, S.; Tahara, T.; Kawarai Lefor, A.; Ogura, M. Pemafibrate improves hepatic inflammation, function and fibrosis in patients with non-alcoholicfatty liver disease: A one-year observational study. Clin. Exp. Hepatol. 2021, 7, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, A.; Eguchi, Y.; Yoneda, M.; Imajo, K.; Tamaki, N.; Suganami, H.; Nojima, T.; Tanigawa, R.; Iizuka, M.; Iida, Y.; et al. Randomised clinical trial: Pemafibrate, a novel selective peroxisome proliferator-activated receptor α modulator (SPPARMα), versus placebo in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2021, 54, 1263–1277. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, T.; Kosone, T.; Saito, N.; Takakusagi, S.; Tojima, H.; Naganuma, A.; Takagi, H.; Uraoka, T.; Kakizaki, S. Effect of 48-week pemafibrate on non-alcoholic fatty liver disease with hypertriglyceridemia, as evaluated by the FibroScan- aspartate aminotransferase score. JGH Open 2021, 5, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Morishita, A.; Oura, K.; Takuma, K.; Nakahara, M.; Tadokoro, T.; Fujita, K.; Tani, J.; Shi, T.; Himoto, T.; Tatsuta, M.; et al. Pemafibrate improves liver dysfunction and non-invasive surrogates for liver fibrosis in patients with non-alcoholic fatty liver disease with hypertriglyceridemia: A multicenter study. Hepatol. Int. 2023, 17, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, R.; Iwasa, M.; Eguchi, A.; Tamai, Y.; Shigefuku, R.; Fujiwara, N.; Tanaka, H.; Kobayashi, Y.; Ikoma, J.; Kaito, M.; et al. Effect of pemafibrate on liver enzymes and shear wave velocity in non-alcoholic fatty liver disease patients. Front. Med. 2023, 10, 1073025. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, S.; Tahara, T.; Miura, K.; Kawarai Lefor, A.; Yamamoto, H. Pemafibrate therapy for non-alcoholic fatty liver disease is more effective in lean patients than obese patients. Clin. Exp. Hepatol. 2022, 8, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Roy, S. Clinical Case Series of Decrease in Shear Wave Elastography Values in Ten Diabetic Dyslipidemia Patients Having NAFLD with Saroglitazar 4 mg: An Indian Experience. Case Rep. Med. 2020, 2020, 4287075. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A. An Observational Study of Reduction in Glycemic Parameters and Liver Stiffness by Saroglitazar 4 mg in Patients With Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease. Cureus 2020, 12, 1–7. [Google Scholar] [CrossRef]
- Goyal, O.; Nohria, S.; Goyal, P.; Kaur, J.; Sharma, S.; Sood, A.; Chhina, R.S. Saroglitazar in patients with non-alcoholic fatty liver disease and diabetic dyslipidemia: A prospective, observational, real world study. Sci. Rep. 2020, 10, 21117. [Google Scholar] [CrossRef] [PubMed]
- Rajesh, N.A.; Drishya, L.; Ambati, M.M.R.; Narayanan, A.L.; Alex, M.; Kumar, K.K.; Abraham, J.J.; Vijayakumar, T.M. Safety and Efficacy of Saroglitazar in Nonalcoholic Fatty Liver Patients With Diabetic Dyslipidemia—A Prospective, Interventional, Pilot Study. J. Clin. Exp. Hepatol. 2022, 12, 61–67. [Google Scholar] [CrossRef]
- Padole, P.; Arora, A.; Sharma, P.; Chand, P.; Verma, N.; Kumar, A. Saroglitazar for Nonalcoholic Fatty Liver Disease: A Single Centre Experience in 91 Patients. J. Clin. Exp. Hepatol. 2022, 12, 435–439. [Google Scholar] [CrossRef]
- Siddiqui, M.S.; Parmar, D.; Sheikh, F.; Sarin, S.K.; Cisneros, L.; Gawrieh, S.; Momin, T.; Duseja, A.; Sanyal, A.J. Saroglitazar, a Dual PPAR α/γ Agonist, Improves Atherogenic Dyslipidemia in Patients With Non-Cirrhotic Nonalcoholic Fatty Liver Disease: A Pooled Analysis. Clin. Gastroenterol. Hepatol. 2023, 21, 2597–2605. [Google Scholar] [CrossRef]
- Malik, A.; Nadeem, M.; Malik, M.I. Efficacy of elafibranor in patients with liver abnormalities especially non-alcoholic steatohepatitis: A systematic review and meta-analysis. Clin. J. Gastroenterol. 2021, 14, 1579–1586. [Google Scholar] [CrossRef]
- Kotsiliti, E. Lanifibranor and NASH resolution. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 832. [Google Scholar] [CrossRef] [PubMed]
- Fabbrini, E.; Sullivan, S.; Klein, S. Obesity and nonalcoholic fatty liver disease: Biochemical, metabolic, and clinical implications. Hepatology 2010, 51, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.E.; Ramos-Roman, M.A.; Browning, J.D.; Parks, E.J. Increased de novo lipogenesis is a distinct characteristic of individuals with nonalcoholic fatty liver disease. Gastroenterology 2014, 146, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-W.; Addy, C.; Kusunoki, J.; Anderson, N.N.; Deja, S.; Fu, X.; Burgess, S.C.; Li, C.; Ruddy, M.; Chakravarthy, M.; et al. Acetyl CoA Carboxylase Inhibition Reduces Hepatic Steatosis but Elevates Plasma Triglycerides in Mice and Humans: A Bedside to Bench Investigation. Cell Metab. 2017, 26, 394–406.e6. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Kayali, Z.; Noureddin, M.; Ruane, P.; Lawitz, E.J.; Bennett, M.; Wang, L.; Harting, E.; Tarrant, J.M.; McColgan, B.J.; et al. GS-0976 Reduces Hepatic Steatosis and Fibrosis Markers in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2018, 155, 1463–1473.e6. [Google Scholar] [CrossRef]
- Metabolic Interventions to Resolve Non-Alcoholic Steatohepatitis (NASH) with Fibrosis (MIRNA). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04321031 (accessed on 28 September 2023).
- O’Farrell, M.; Duke, G.; Crowley, R.; Buckley, D.; Martins, E.B.; Bhattacharya, D.; Friedman, S.L.; Kemble, G. FASN inhibition targets multiple drivers of NASH by reducing steatosis, inflammation and fibrosis in preclinical models. Sci. Rep. 2022, 12, 15661. [Google Scholar] [CrossRef]
- Syed-Abdul, M.M.; Parks, E.J.; Gaballah, A.H.; Bingham, K.; Hammoud, G.M.; Kemble, G.; Buckley, D.; McCulloch, W.; Manrique-Acevedo, C. Fatty Acid Synthase Inhibitor TVB-2640 Reduces Hepatic de Novo Lipogenesis in Males With Metabolic Abnormalities. Hepatology 2020, 72, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Mohseni, R.; Lucas, K.J.; Gutierrez, J.A.; Perry, R.G.; Trotter, J.F.; Rahimi, R.S.; Harrison, S.A.; Ajmera, V.; Wayne, J.D.; et al. TVB-2640 (FASN Inhibitor) for the Treatment of Nonalcoholic Steatohepatitis: FASCINATE-1, a Randomized, Placebo-Controlled Phase 2a Trial. Gastroenterology 2021, 161, 1475–1486. [Google Scholar] [CrossRef]
- Study of TVB-2640 in Subjects with Nonalcoholic Steatohepatitis (NASH). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04906421 (accessed on 24 September 2023).
- Calle, R.A.; Amin, N.B.; Carvajal-Gonzalez, S.; Ross, T.T.; Bergman, A.; Aggarwal, S.; Crowley, C.; Rinaldi, A.; Mancuso, J.; Aggarwal, N.; et al. ACC inhibitor alone or co-administered with a DGAT2 inhibitor in patients with non-alcoholic fatty liver disease: Two parallel, placebo-controlled, randomized phase 2a trials. Nat. Med. 2021, 27, 1836–1848. [Google Scholar] [CrossRef]
- Amin, N.B.; Darekar, A.; Anstee, Q.M.; Wong, V.W.-S.; Tacke, F.; Vourvahis, M.; Lee, D.S.; Charlton, M.; Alkhouri, N.; Nakajima, A.; et al. Efficacy and safety of an orally administered DGAT2 inhibitor alone or coadministered with a liver-targeted ACC inhibitor in adults with non-alcoholic steatohepatitis (NASH): Rationale and design of the phase II, dose-ranging, dose-finding, randomised, placebo-controlled MIRNA (Metabolic Interventions to Resolve NASH with fibrosis) study. BMJ Open 2022, 12, e056159. [Google Scholar] [CrossRef] [PubMed]
- A Study to Assess the Safety, Efficacy, and Pharmacokinetics of Multiple Doses of ION224. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04932512 (accessed on 24 September 2023).
- Woo, Y.C.; Xu, A.; Wang, Y.; Lam, K.S.L. Fibroblast growth factor 21 as an emerging metabolic regulator: Clinical perspectives. Clin. Endocrinol. 2013, 78, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Lawitz, E.J.; Frias, J.P.; Ortiz-Lasanta, G.; Johansson, L.; Franey, B.B.; Morrow, L.; Rosenstock, M.; Hartsfield, C.L.; Chen, C.-Y.; et al. Safety, pharmacokinetics, and pharmacodynamics of pegozafermin in patients with non-alcoholic steatohepatitis: A randomised, double-blind, placebo-controlled, phase 1b/2a multiple-ascending-dose study. Lancet Gastroenterol. Hepatol. 2023, 8, 120–132. [Google Scholar] [CrossRef]
- Loomba, R.; Sanyal, A.J.; Kowdley, K.V.; Bhatt, D.L.; Alkhouri, N.; Frias, J.P.; Bedossa, P.; Harrison, S.A.; Lazas, D.; Barish, R.; et al. Randomized, Controlled Trial of the FGF21 Analogue Pegozafermin in NASH. N. Engl. J. Med. 2023, 389, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- To Evaluate the Efficacy and Safety of Pegozafermin in Subjects with Severe Hypertriglyceridemia (ENTRUST). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05852431 (accessed on 24 September 2023).
- Puengel, T.; Tacke, F. Efruxifermin, an investigational treatment for fibrotic or cirrhotic nonalcoholic steatohepatitis (NASH). Expert. Opin. Investig. Drugs 2023, 32, 451–461. [Google Scholar] [CrossRef]
- Bristol Myers Becomes Latest Victim of Unforgiving NASH as Midstage Asset Shelved. Available online: https://www.fiercebiotech.com/biotech/bristol-myers-becomes-latest-victim-unforgiving-nash-as-mid-stage-asset-shelved (accessed on 24 September 2023).
- Zhang, W.; Tang, Y.; Huang, J.; Hu, H. Efficacy of ursodeoxycholic acid in nonalcoholic fatty liver disease: An updated meta-analysis of randomized controlled trials. Asia Pac. J. Clin. Nutr. 2020, 29, 696–705. [Google Scholar] [CrossRef]
- Lin, X.; Mai, M.; He, T.; Huang, H.; Zhang, P.; Xia, E.; Guo, H. Efficiency of ursodeoxycholic acid for the treatment of nonalcoholic steatohepatitis: A systematic review and meta-analysis. Expert. Rev. Gastroenterol. Hepatol. 2022, 16, 537–545. [Google Scholar] [CrossRef]
- Ferro, D.; Baratta, F.; Pastori, D.; Cocomello, N.; Colantoni, A.; Angelico, F.; Del Ben, M. New Insights into the Pathogenesis of Non-Alcoholic Fatty Liver Disease: Gut-Derived Lipopolysaccharides and Oxidative Stress. Nutrients 2020, 12, 2762. [Google Scholar] [CrossRef]
- An, L.; Wirth, U.; Koch, D.; Schirren, M.; Drefs, M.; Koliogiannis, D.; Nieß, H.; Andrassy, J.; Guba, M.; Bazhin, A.V.; et al. The Role of Gut-Derived Lipopolysaccharides and the Intestinal Barrier in Fatty Liver Diseases. J. Gastrointest. Surg. 2022, 26, 671–683. [Google Scholar] [CrossRef]
- Carpi, R.Z.; Barbalho, S.M.; Sloan, K.P.; Laurindo, L.F.; Gonzaga, H.F.; Grippa, P.C.; Zutin, T.L.M.; Girio, R.J.S.; Repetti, C.S.F.; Detregiachi, C.R.P.; et al. The Effects of Probiotics, Prebiotics and Synbiotics in Non-Alcoholic Fat Liver Disease (NAFLD) and Non-Alcoholic Steatohepatitis (NASH): A Systematic Review. Int. J. Mol. Sci. 2022, 23, 8805. [Google Scholar] [CrossRef]
- Sharpton, S.R.; Maraj, B.; Harding-Theobald, E.; Vittinghoff, E.; Terrault, N.A. Gut microbiome-targeted therapies in nonalcoholic fatty liver disease: A systematic review, meta-analysis, and meta-regression. Am. J. Clin. Nutr. 2019, 110, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Davani-Davari, D.; Negahdaripour, M.; Karimzadeh, I.; Seifan, M.; Mohkam, M.; Masoumi, S.J.; Berenjian, A.; Ghasemi, Y. Prebiotics: Definition, Types, Sources, Mechanisms, and Clinical Applications. Foods 2019, 8, 92. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, X.; Zhang, L.; Zheng, K.; Xiong, J.; Li, J.; Cong, C.; Gong, Z.; Mao, J. Effect of Probiotics Therapy on Nonalcoholic Fatty Liver Disease. Comput. Math. Methods Med. 2022, 2022, 7888076. [Google Scholar] [CrossRef] [PubMed]
- Mavilia-Scranton, M.G.; Wu, G.Y.; Dharan, M. Impact of Helicobacter pylori Infection on the Pathogenesis and Management of Nonalcoholic Fatty Liver Disease. J. Clin. Transl. Hepatol. 2023, 11, 670. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Ma, S.; Dong, L.; Mendez-Sanchez, N.; Li, H.; Qi, X. Relationship of Helicobacter pylori Infection with Nonalcoholic Fatty Liver Disease: A Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2023, 2023, 5521239. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Camargo, M.C.; El-Omar, E.; Liou, J.-M.; Peek, R.; Schulz, C.; Smith, S.I.; Suerbaum, S. Helicobacter pylori infection. Nat. Rev. Dis. Primers 2023, 9, 19. [Google Scholar] [CrossRef]
- Aydemir, S.; Bayraktaroglu, T.; Sert, M.; Sokmen, C.; Atmaca, H.; Mungan, G.; Gun, B.D.; Borazan, A.; Ustundag, Y. The Effect of Helicobacter pylori on Insulin Resistance. Dig. Dis. Sci. 2005, 50, 2090–2093. [Google Scholar] [CrossRef]
- Chen, L.-W.; Chien, C.-Y.; Yang, K.-J.; Kuo, S.-F.; Chen, C.-H.; Chien, R.-N. Helicobacter pylori Infection Increases Insulin Resistance and Metabolic Syndrome in Residents Younger than 50 Years Old: A Community-Based Study. PLoS ONE 2015, 10, e0128671. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, C.; Wang, X.; Zhang, F.; Zhang, Z.; Ma, P.; Feng, S. Helicobacter pylori infection may increase the severity of nonalcoholic fatty liver disease via promoting liver function damage, glycometabolism, lipid metabolism, inflammatory reaction and metabolic syndrome. Eur. J. Gastroenterol. Hepatol. 2020, 32, 857–866. [Google Scholar] [CrossRef]
- Azami, M.; Baradaran, H.R.; Dehghanbanadaki, H.; Kohnepoushi, P.; Saed, L.; Moradkhani, A.; Moradpour, F.; Moradi, Y. Association of Helicobacter pylori infection with the risk of metabolic syndrome and insulin resistance: An updated systematic review and meta-analysis. Diabetol. Metab. Syndr. 2021, 13, 145. [Google Scholar] [CrossRef]
- Tsuji, A.; Yoshikawa, S.; Ikeda, Y.; Taniguchi, K.; Sawamura, H.; Morikawa, S.; Nakashima, M.; Asai, T.; Matsuda, S. Tactics with Prebiotics for the Treatment of Metabolic Dysfunction-Associated Fatty Liver Disease via the Improvement of Mitophagy. Int. J. Mol. Sci. 2023, 24, 5465. [Google Scholar] [CrossRef] [PubMed]
- Arellano-García, L.; Portillo, M.P.; Martínez, J.A.; Milton-Laskibar, I. Usefulness of Probiotics in the Management of NAFLD: Evidence and Involved Mechanisms of Action from Preclinical and Human Models. Int. J. Mol. Sci. 2022, 23, 3167. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Sun, D.; Wang, Y.; Du, Q.; Zhang, Y.; Han, R.; Teng, M.; Zhang, T.; Shi, L.; Zheng, G.; et al. Evaluation of the current guidelines for antibacterial therapy strategies in patients with cirrhosis or liver failure. BMC Infect. Dis. 2022, 22, 23. [Google Scholar] [CrossRef]
- Gangarapu, V.; Ince, A.T.; Baysal, B.; Kayar, Y.; Kılıç, U.; Gök, Ö.; Uysal, Ö.; Şenturk, H. Efficacy of rifaximin on circulating endotoxins and cytokines in patients with nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2015, 27, 840–845. [Google Scholar] [CrossRef]
- Abdel-Razik, A.; Mousa, N.; Shabana, W.; Refaey, M.; Elzehery, R.; Elhelaly, R.; Zalata, K.; Abdelsalam, M.; Eldeeb, A.A.; Awad, M.; et al. Rifaximin in nonalcoholic fatty liver disease: Hit multiple targets with a single shot. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1237–1246. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Zocco, M.A.; D’Aversa, F.; Pompili, M.; Gasbarrini, A. Eubiotic properties of rifaximin: Disruption of the traditional concepts in gut microbiota modulation. World J. Gastroenterol. 2017, 23, 4491–4499. [Google Scholar] [CrossRef]
- Chen, H.-T.; Huang, H.-L.; Li, Y.-Q.; Xu, H.-M.; Zhou, Y.-J. Therapeutic advances in non-alcoholic fatty liver disease: A microbiota-centered view. World J. Gastroenterol. 2020, 26, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Podszun, M.C.; Alawad, A.S.; Lingala, S.; Morris, N.; Huang, W.-C.A.; Yang, S.; Schoenfeld, M.; Rolt, A.; Ouwerkerk, R.; Valdez, K.; et al. Vitamin E treatment in NAFLD patients demonstrates that oxidative stress drives steatosis through upregulation of de-novo lipogenesis. Redox Biol. 2020, 37, 101710. [Google Scholar] [CrossRef]
- Podszun, M.C.; Frank, J. Impact of vitamin E on redox biomarkers in non-alcoholic fatty liver disease. Redox Biol. 2021, 42, 101937. [Google Scholar] [CrossRef]
- Luo, Q.; Wei, R.; Cai, Y.; Zhao, Q.; Liu, Y.; Liu, W.J. Efficacy of Off-Label Therapy for Non-alcoholic Fatty Liver Disease in Improving Non-invasive and Invasive Biomarkers: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Front Med. 2022, 9, 793203. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Sohn, J.H. Pharmacological advances in the treatment of nonalcoholic fatty liver diseases: Focused on global results of randomized controlled trials. Clin. Mol. Hepatol. 2023, 29, S268–S275. [Google Scholar] [CrossRef]
- Lahmi, A.; Oryan, S.; Eidi, A.; Rohani, A.H. Comparative effects of thymol and vitamin E on nonalcoholic fatty liver disease in male Wistar rats. Braz. J. Biol. 2023, 84, e268781. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Li, T.; Liu, J.; Wang, Y.; Wang, C.; Ju, S.; Zhou, C.; Chen, Y.; Yao, W.; Xiong, B. Aerobic exercise and vitamin E improve high-fat diet-induced NAFLD in rats by regulating the AMPK pathway and oxidative stress. Eur. J. Nutr. 2023, 62, 2621–2632. [Google Scholar] [CrossRef]
- Vadarlis, A.; Antza, C.; Bakaloudi, D.R.; Doundoulakis, I.; Kalopitas, G.; Samara, M.; Dardavessis, T.; Maris, T.; Chourdakis, M. Systematic review with meta-analysis: The effect of vitamin E supplementation in adult patients with non-alcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2021, 36, 311–319. [Google Scholar] [CrossRef]
- Abdel-Maboud, M.; Menshawy, A.; Menshawy, E.; Emara, A.; Alshandidy, M.; Eid, M. The efficacy of vitamin E in reducing non-alcoholic fatty liver disease: A systematic review, meta-analysis, and meta-regression. Ther. Adv. Gastroenterol. 2020, 13, 175628482097491. [Google Scholar] [CrossRef] [PubMed]
- Bułdak, Ł.; Marek, B.; Kajdaniuk, D.; Urbanek, A.; Janyga, S.; Bołdys, A.; Basiak, M.; Maligłówka, M.; Okopień, B. Endocrine diseases as causes of secondary hyperlipidemia. Endokrynol. Pol. 2019, 70, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Tanase, D.M.; Gosav, E.M.; Neculae, E.; Costea, C.F.; Ciocoiu, M.; Hurjui, L.L.; Tarniceriu, C.C.; Floria, M. Hypothyroidism-Induced Nonalcoholic Fatty Liver Disease (HIN): Mechanisms and Emerging Therapeutic Options. Int. J. Mol. Sci. 2020, 21, 5927. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Bashir, M.R.; Guy, C.D.; Zhou, R.; Moylan, C.A.; Frias, J.P.; Alkhouri, N.; Bansal, M.B.; Baum, S.; Neuschwander-Tetri, B.A.; et al. Resmetirom (MGL-3196) for the treatment of non-alcoholic steatohepatitis: A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2019, 394, 2012–2024. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Bashir, M.; Moussa, S.E.; McCarty, K.; Frias, J.P.; Taub, R.; Alkhouri, N. Effects of Resmetirom on Noninvasive Endpoints in a 36-Week Phase 2 Active Treatment Extension Study in Patients With NASH. Hepatol. Commun. 2021, 5, 573–588. [Google Scholar] [CrossRef] [PubMed]
- A Phase 3 Study to Evaluate Safety and Biomarkers of Resmetirom (MGL-3196) in Patients with Non-alcoholic Fatty Liver Disease (NAFLD), MAESTRO-NAFLD-Open-Label-Extension (MAESTRO-NAFLD-OLE). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04951219 (accessed on 5 May 2023).
- Polyzos, S.A.; Mousiolis, A.; Mintziori, G.; Goulis, D.G. Nonalcoholic fatty liver disease in males with low testosterone concentrations. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1571–1577. [Google Scholar] [CrossRef] [PubMed]
- Yassin, A.A.; Alwani, M.; Talib, R.; Almehmadi, Y.; Nettleship, J.E.; Alrumaihi, K.; Albaba, B.; Kelly, D.M.; Saad, F. Long-term testosterone therapy improves liver parameters and steatosis in hypogonadal men: A prospective controlled registry study. Aging Male 2020, 23, 1553–1563. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.; Jothimani, D.; Harika, K.; Hakeem, A.R.; Sachan, D.; Vij, M.; Rela, M. Versatility of Anabolic Androgenic Steroid-Induced Hepatotoxicity. J. Clin. Exp. Hepatol. 2022, 12, 216–221. [Google Scholar] [CrossRef]
- Palmisano, B.T.; Zhu, L.; Stafford, J.M. Role of Estrogens in the Regulation of Liver Lipid Metabolism. Adv. Exp. Med. Biol. 2017, 1043, 227–256. [Google Scholar] [CrossRef]
- Gutierrez-Grobe, Y.; Ponciano-Rodríguez, G.; Ramos, M.H.; Uribe, M.; Méndez-Sánchez, N. Prevalence of non alcoholic fatty liver disease in premenopausal, posmenopausal and polycystic ovary syndrome women. The role of estrogens. Ann. Hepatol. 2010, 9, 402–409. [Google Scholar] [PubMed]
- Cao, W.; Xu, Y.; Shen, Y.; Wang, Y.; Ma, X.; Bao, Y. Associations between sex hormones and metabolic-associated fatty liver disease in a middle-aged and elderly community. Endocr. J. 2022, 69, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Lambrinoudaki, I.; Goulis, D.G. Menopausal hormone therapy in women with dyslipidemia and nonalcoholic fatty liver disease. Hormones 2022, 21, 375–381. [Google Scholar] [CrossRef] [PubMed]
- DiStefano, J.K. NAFLD and NASH in Postmenopausal Women: Implications for Diagnosis and Treatment. Endocrinology 2020, 161, bqaa134. [Google Scholar] [CrossRef] [PubMed]
- Florio, A.A.; Graubard, B.I.; Yang, B.; Thistle, J.E.; Bradley, M.C.; McGlynn, K.A.; Petrick, J.L. Oophorectomy and risk of non-alcoholic fatty liver disease and primary liver cancer in the Clinical Practice Research Datalink. Eur. J. Epidemiol. 2019, 34, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Oxley, M.; Francis, H.; Sato, K. Growth Hormone Signaling in Liver Diseases: Therapeutic Potentials and Controversies. Semin. Liver Dis. 2023, 43, 024–030. [Google Scholar] [CrossRef]
- Hwang, Y.; Lee, H.W.; Ahn, S.H.; Lee, E.J.; Ku, C.R.; Kim, S.U. Positive association between nonalcoholic fatty liver disease and growth hormone deficiency in patients with nonfunctioning pituitary adenoma. Front. Endocrinol. 2023, 13, 1057769. [Google Scholar] [CrossRef]
- Dichtel, L.E.; Corey, K.E.; Haines, M.S.; Chicote, M.L.; Kimball, A.; Colling, C.; Simon, T.G.; Long, M.T.; Husseini, J.; Bredella, M.A.; et al. The GH/IGF-1 Axis Is Associated with Intrahepatic Lipid Content and Hepatocellular Damage in Overweight/Obesity. J. Clin. Endocrinol. Metab. 2022, 107, e3624–e3632. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.S.; Weiss, J.J.; Fourman, L.T.; Buckless, C.; Branch, K.L.; Lee, H.; Torriani, M.; Misra, M.; Stanley, T.L. Effect of recombinant human growth hormone on liver fat content in young adults with nonalcoholic fatty liver disease. Clin. Endocrinol. 2021, 94, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Que, S.; Zhou, L.; Zheng, S. Dose-response Relationship of Serum Uric Acid with Metabolic Syndrome and Non-alcoholic Fatty Liver Disease Incidence: A Meta-analysis of Prospective Studies. Sci. Rep. 2015, 5, 14325. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, T.; Nagata, N.; Shimakami, T.; Shirakura, T.; Matsui, C.; Ni, Y.; Zhuge, F.; Xu, L.; Chen, G.; Nagashimada, M.; et al. Xanthine oxidase inhibition attenuates insulin resistance and diet-induced steatohepatitis in mice. Sci. Rep. 2020, 10, 815. [Google Scholar] [CrossRef]
- Kakimoto, M.; Fujii, M.; Sato, I.; Honma, K.; Nakayama, H.; Kirihara, S.; Fukuoka, T.; Ran, S.; Hirohata, S.; Kitamori, K.; et al. Antioxidant action of xanthine oxidase inhibitor febuxostat protects the liver and blood vasculature in SHRSP5/Dmcr rats. J. Appl. Biomed. 2023, 21, 80–90. [Google Scholar] [CrossRef]
- NCT05474560. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05474560 (accessed on 9 June 2023).
- Kessoku, T.; Kobayashi, T.; Tanaka, K.; Yamamoto, A.; Takahashi, K.; Iwaki, M.; Ozaki, A.; Kasai, Y.; Nogami, A.; Honda, Y.; et al. The Role of Leaky Gut in Nonalcoholic Fatty Liver Disease: A Novel Therapeutic Target. Int. J. Mol. Sci. 2021, 22, 8161. [Google Scholar] [CrossRef]
- Wilson, N.; Schey, R. Lubiprostone in constipation: Clinical evidence and place in therapy. Ther. Adv. Chronic Dis. 2015, 6, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-Y.; Lee, S.-J.; Randolph, G.; Han, Y.-H. Lubiprostone significantly represses fatty liver diseases via induction of mucin and HDL release in mice. Life Sci. 2022, 311, 121176. [Google Scholar] [CrossRef]
- Kessoku, T.; Imajo, K.; Kobayashi, T.; Ozaki, A.; Iwaki, M.; Honda, Y.; Kato, T.; Ogawa, Y.; Tomeno, W.; Kato, S.; et al. Lubiprostone in patients with non-alcoholic fatty liver disease: A randomised, double-blind, placebo-controlled, phase 2a trial. Lancet Gastroenterol. Hepatol. 2020, 5, 996–1007. [Google Scholar] [CrossRef]
- NCT05768334. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05768334 (accessed on 30 May 2023).
- El-Deen, R.M.; Heeba, G.H.; Abdel-latif, R.G.; Khalifa, M.M.A. Comparative effectiveness of phosphodiesterase 3, 4, and 5 inhibitors in amelioration of high-fat diet-induced nonalcoholic fatty liver in rats. Fundam. Clin. Pharmacol. 2020, 34, 353–364. [Google Scholar] [CrossRef]
- Vachliotis, I.D.; Polyzos, S.A. The Role of Tumor Necrosis Factor-Alpha in the Pathogenesis and Treatment of Nonalcoholic Fatty Liver Disease. Curr. Obes. Rep. 2023, 12, 191–206. [Google Scholar] [CrossRef]
- Du, J. Effects of pentoxifylline on nonalcoholic fatty liver disease: A meta-analysis. World J. Gastroenterol. 2014, 20, 569. [Google Scholar] [CrossRef] [PubMed]
- Ipsen, D.H.; Skat-Rørdam, J.; Svenningsen, M.; Andersen, M.; Latta, M.; Buelund, L.E.; Lintrup, K.; Skaarup, R.; Lykkesfeldt, J.; Tveden-Nyborg, P. The effect of acetylsalicylic acid and pentoxifylline in guinea pigs with non-alcoholic steatohepatitis. Basic. Clin. Pharmacol. Toxicol. 2021, 128, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Mahjoubin-Tehran, M.; De Vincentis, A.; Mikhailidis, D.P.; Atkin, S.L.; Mantzoros, C.S.; Jamialahmadi, T.; Sahebkar, A. Non-alcoholic fatty liver disease and steatohepatitis: State of the art on effective therapeutics based on the gold standard method for diagnosis. Mol. Metab. 2021, 50, 101049. [Google Scholar] [CrossRef]
- Malladi, N.; Alam, M.J.; Maulik, S.K.; Banerjee, S.K. The role of platelets in non-alcoholic fatty liver disease: From pathophysiology to therapeutics. Prostaglandins Other Lipid Mediat. 2023, 169, 106766. [Google Scholar] [CrossRef]
- Meng, C.; Song, Z.; Zhang, L.; Geng, Y.; Sun, J.; Miao, G.; Liu, P. Effects of losartan in patients with NAFLD: A meta-analysis of randomized controlled trial. Open Life Sci. 2023, 18, 20220583. [Google Scholar] [CrossRef] [PubMed]
- Surma, S.; Sahebkar, A.; Urbański, J.; Penson, P.E.; Banach, M. Curcumin—The Nutraceutical With Pleiotropic Effects? Which Cardiometabolic Subjects Might Benefit the Most? Front. Nutr. 2022, 9, 865497. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Colletti, A.; Bajraktari, G.; Descamps, O.; Djuric, D.M.; Ezhov, M.; Fras, Z.; Katsiki, N.; Langlois, M.; Latkovskis, G.; et al. Lipid lowering nutraceuticals in clinical practice: Position paper from an International Lipid Expert Panel. Arch. Med. Sci. 2017, 13, 965–1005. [Google Scholar] [CrossRef] [PubMed]
- Banach, M.; Burchardt, P.; Chlebus, K.; Dobrowolski, P.; Dudek, D.; Dyrbuś, K.; Gąsior, M.; Jankowski, P.; Jóźwiak, J.; Kłosiewicz-Latoszek, L.; et al. PoLA/CFPiP/PCS/PSLD/PSD/PSH guidelines on diagnosis and therapy of lipid disorders in Poland 2021. Arch. Med. Sci. 2021, 17, 1447–1547. [Google Scholar] [CrossRef]
- Ruscica, M.; Penson, P.E.; Ferri, N.; Sirtori, C.R.; Pirro, M.; Mancini, G.B.J.; Sattar, N.; Toth, P.P.; Sahebkar, A.; Lavie, C.J.; et al. Impact of nutraceuticals on markers of systemic inflammation: Potential relevance to cardiovascular diseases— A position paper from the International Lipid Expert Panel (ILEP). Prog. Cardiovasc. Dis. 2021, 67, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Ashtary-Larky, D.; Rezaei Kelishadi, M.; Bagheri, R.; Moosavian, S.P.; Wong, A.; Davoodi, S.H.; Khalili, P.; Dutheil, F.; Suzuki, K.; Asbaghi, O. The Effects of Nano-Curcumin Supplementation on Risk Factors for Cardiovascular Disease: A GRADE-Assessed Systematic Review and Meta-Analysis of Clinical Trials. Antioxid 2021, 10, 1015. [Google Scholar] [CrossRef]
- Ngu, M.H.; Norhayati, M.N.; Rosnani, Z.; Zulkifli, M.M. Curcumin as adjuvant treatment in patients with non-alcoholic fatty liver (NAFLD) disease: A systematic review and meta-analysis. Complement. Ther. Med. 2022, 68, 102843. [Google Scholar] [CrossRef] [PubMed]
- Lukkunaprasit, T.; Tansawet, A.; Boonmanunt, S.; Sobhonslidsuk, A.; McKay, G.J.; Attia, J.; Thakkinstian, A. An updated meta-analysis of effects of curcumin on metabolic dysfunction-associated fatty liver disease based on available evidence from Iran and Thailand. Sci. Rep. 2023, 13, 5824. [Google Scholar] [CrossRef]
- Surma, S.; Kokot, F. Influence of chronic coffee consumption on the risk of kidney and other organ diseases. Review of the literature and clinical studies. Ren. Dis. Transplant. Forum 2022, 15, 1–18. [Google Scholar] [CrossRef]
- Surma, S.; Sahebkar, A.; Banach, M. Coffee or tea: Anti-inflammatory properties in the context of atherosclerotic cardiovascular disease prevention. Pharmacol. Res. 2023, 187, 106596. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Bhupathiraju, S.N.; Chen, M.; van Dam, R.M.; Hu, F.B. Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: A systematic review and a dose-response meta-analysis. Diabetes Care 2014, 37, 569–586. [Google Scholar] [CrossRef]
- Surma, S.; Oparil, S. Coffee and Arterial Hypertension. Curr. Hypertens. Rep. 2021, 23, 38. [Google Scholar] [CrossRef]
- Surma, S.; Banach, M. Coffee and caffeine consumption and overall mortality. Pleasure with restrictions-where do we really stand in 2022? Nutrition 2022, 102, 111747. [Google Scholar] [CrossRef] [PubMed]
- Sewter, R.; Heaney, S.; Patterson, A. Coffee Consumption and the Progression of NAFLD: A Systematic Review. Nutrients 2021, 13, 2381. [Google Scholar] [CrossRef]
- Hayat, U.; Siddiqui, A.A.; Okut, H.; Afroz, S.; Tasleem, S.; Haris, A. The effect of coffee consumption on the non-alcoholic fatty liver disease and liver fibrosis: A meta-analysis of 11 epidemiological studies. Ann. Hepatol. 2021, 20, 100254. [Google Scholar] [CrossRef] [PubMed]
- Kositamongkol, C.; Kanchanasurakit, S.; Auttamalang, C.; Inchai, N.; Kabkaew, T.; Kitpark, S.; Chaiyakunapruk, N.; Duangjai, A.; Saokaew, S.; Phisalprapa, P. Coffee Consumption and Non-alcoholic Fatty Liver Disease: An Umbrella Review and a Systematic Review and Meta-analysis. Front. Pharmacol. 2021, 12, 786596. [Google Scholar] [CrossRef]
- Kennedy, O.J.; Roderick, P.; Buchanan, R.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Systematic review with meta-analysis: Coffee consumption and the risk of cirrhosis. Aliment. Pharmacol. Ther. 2016, 43, 562–574. [Google Scholar] [CrossRef] [PubMed]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Mishra, A.P.; Nigam, M.; Sener, B.; Kilic, M.; Sharifi-Rad, M.; Fokou, P.V.T.; Martins, N.; Sharifi-Rad, J. Resveratrol: A Double-Edged Sword in Health Benefits. Biomedicines 2018, 6, 91. [Google Scholar] [CrossRef]
- Zhang, C.; Yuan, W.; Fang, J.; Wang, W.; He, P.; Lei, J.; Wang, C. Efficacy of Resveratrol Supplementation against Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Placebo-Controlled Clinical Trials. PLoS ONE 2016, 11, e0161792. [Google Scholar] [CrossRef]
- Jakubczyk, K.; Skonieczna-Żydecka, K.; Kałduńska, J.; Stachowska, E.; Gutowska, I.; Janda, K. Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease-A Meta-Analysis. Nutrients 2020, 12, 2435. [Google Scholar] [CrossRef] [PubMed]
- Adamczak, M.; Surma, S.; Więcek, A. Vitamin D and Arterial Hypertension: Facts and Myths. Curr. Hypertens. Rep. 2020, 22, 57. [Google Scholar] [CrossRef] [PubMed]
- De la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef]
- Eliades, M.; Spyrou, E.; Agrawal, N.; Lazo, M.; Brancati, F.L.; Potter, J.J.; Koteish, A.A.; Clark, J.M.; Guallar, E.; Hernaez, R. Meta-analysis: Vitamin D and non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2013, 38, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Sindhughosa, D.A.; Wibawa, I.D.N.; Mariadi, I.K.; Somayana, G. Additional treatment of vitamin D for improvement of insulin resistance in non-alcoholic fatty liver disease patients: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 7716. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, S.; Tabrizi, R.; Nowrouzi-Sohrabi, P.; Jalali, M.; Shabani-Borujeni, M.; Modaresi, S.; Gholamalizadeh, M.; Doaei, S. The Effects of Vitamin D Supplementation on Anthropometric and Biochemical Indices in Patients with Non-alcoholic Fatty Liver Disease: A Systematic Review and Meta-analysis. Front. Pharmacol. 2021, 12, 732496. [Google Scholar] [CrossRef]
- Rizzo, M.; Colletti, A.; Penson, P.E.; Katsiki, N.; Mikhailidis, D.P.; Toth, P.P.; Gouni-Berthold, I.; Mancini, J.; Marais, D.; Moriarty, P.; et al. Nutraceutical approaches to non-alcoholic fatty liver disease (NAFLD): A position paper from the International Lipid Expert Panel (ILEP). Pharmacol. Res. 2023, 189, 106679. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.-H.; Guan, B.-J.; Gao, H.-Y.; Peng, X.-E. Omega-3 polyunsaturated fatty acid supplementation and non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Medicine 2018, 97, e12271. [Google Scholar] [CrossRef]
- Moore, E.; Patanwala, I.; Jafari, A.; Davies, I.G.; Kirwan, R.P.; Newson, L.; Mazidi, M.; Lane, K.E. A systematic review and meta-analysis of randomized controlled trials to evaluate plant-based omega-3 polyunsaturated fatty acids in nonalcoholic fatty liver disease patient biomarkers and parameters. Nutr. Rev. 2023, nuad054, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Federico, A.; Dallio, M.; Loguercio, C. Silymarin/Silybin and Chronic Liver Disease: A Marriage of Many Years. Molecules 2017, 22, 191. [Google Scholar] [CrossRef]
- Kalopitas, G.; Antza, C.; Doundoulakis, I.; Siargkas, A.; Kouroumalis, E.; Germanidis, G.; Samara, M.; Chourdakis, M. Impact of Silymarin in individuals with nonalcoholic fatty liver disease: A systematic review and meta-analysis. Nutrition 2021, 83, 111092. [Google Scholar] [CrossRef] [PubMed]
- Surma, S.; Romańczyk, M.; Czerniuk, M.R.; Filipiak, K.J. Garlic for arterial hypertension and hypercholesterolaemia. Review of literature studies and clinical studies. Folia Cardiol. 2021, 16, 296–302. [Google Scholar] [CrossRef]
- Yu, L.; Zhao, R.; Wang, C.; Zhang, C.; Chu, C.; Zhao, J.; Zhang, H.; Zhai, Q.; Chen, W.; Zhang, H.; et al. Effects of garlic supplementation on non-alcoholic fatty liver disease: A systematic review and meta-analysis of randomized controlled trials. J. Funct. Foods 2022, 99, 105294. [Google Scholar] [CrossRef]
- Rastkar, M.; Nikniaz, L.; Abbasalizad Farhangi, M.; Nikniaz, Z. Systematic review and meta-analysis of the effect of garlic in patients with non-alcoholic fatty liver disease. Indian J. Gastroenterol. 2022, 41, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Wiering, L.; Tacke, F. Treating inflammation to combat non-alcoholic fatty liver disease. J. Endocrinol. 2023, 256, e220194. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| (A) | ||||||
| Class | Level | Daily Doses | Expected Effects on LDL-C | Effects on other CV Risk Biomarkers | Direct Vascular Effects | |
| IIa | B | 1–3 g | −5% | ↓ TG, Lp(a), glucose, HbA1c, HOMA index, hs-CRP, TNF-α, and IL-6; ↑ adiponectin and HDL-C | ↑ FMD; ↓ PWV | |
| (B) | ||||||
| Name | Recommended Dosage | Expected Effects on LDL-C | Class of Recommendation | Level of Recommendation | ||
| Curcumin | 0.5–3 g | from –5% to –10% | IIa | A | ||
| (C) | ||||||
| Nutraceuticals | Class | Level | Impact on Markers of Inflammation | |||
| Curcumin | IIa | B | A significant decrement in serum concentrations of TNF-α (−4.69 pg/mL), IL-6, TGF-β, and MCP-1 | |||
| Metabolic Parameter | WMD | 95% CI | Comments |
|---|---|---|---|
| TG (mg/dL) | −24.87 −27.23 | from −37.34 to −12.40; p < 0.001 from −43.11 to −11.35; p = 0.001 | Baseline TG ≥ 150 mg/dL Obese (>30 Kg/m2) |
| TC (mg/dL) | −10.90 | from −16.40 to −5.39; p < 0.001 | Baseline TC ≥ 200 mg/dL and obese (>30 Kg/m2) |
| LDL-C (mg/dL) | −13.70 | from −19.26 to −8.13; p < 0.001 | Baseline LDL-C ≥ 100 mg/dL and obese (>30 Kg/m2) |
| HDL-C (mg/dL) | 5.77 | from 2.90 to 8.64; p < 0.001 | Overall effect |
| FBG (md/dL) | −18.14 | from −29.31 to −6.97; p = 0.001 | Overall effect |
| Fasting Insulin | −1.21 | from −1.43 to −1.00; p < 0.001 | Overall effect |
| HOMA-IR | −0.28 | from −0.33 to −0.23; p < 0.001 | Overall effect |
| SBP (mmHg) | −7.09 | from −12.98 to −1.20; p < 0.001 | Overall effect |
| CRP (mg/L) | −1.29 | from −2.15 to −0.44; p = 0.003 | Overall effect |
| IL-6 (pg/mL) | −2.78 | from −3.76 to −1.79; p < 0.001 | Overall effect |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bołdys, A.; Bułdak, Ł.; Maligłówka, M.; Surma, S.; Okopień, B. Potential Therapeutic Strategies in the Treatment of Metabolic-Associated Fatty Liver Disease. Medicina 2023, 59, 1789. https://doi.org/10.3390/medicina59101789
Bołdys A, Bułdak Ł, Maligłówka M, Surma S, Okopień B. Potential Therapeutic Strategies in the Treatment of Metabolic-Associated Fatty Liver Disease. Medicina. 2023; 59(10):1789. https://doi.org/10.3390/medicina59101789
Chicago/Turabian StyleBołdys, Aleksandra, Łukasz Bułdak, Mateusz Maligłówka, Stanisław Surma, and Bogusław Okopień. 2023. "Potential Therapeutic Strategies in the Treatment of Metabolic-Associated Fatty Liver Disease" Medicina 59, no. 10: 1789. https://doi.org/10.3390/medicina59101789
APA StyleBołdys, A., Bułdak, Ł., Maligłówka, M., Surma, S., & Okopień, B. (2023). Potential Therapeutic Strategies in the Treatment of Metabolic-Associated Fatty Liver Disease. Medicina, 59(10), 1789. https://doi.org/10.3390/medicina59101789