
Metabolomic Phenotype of Hepatic Steatosis and Fibrosis in Mexican Children Living with Obesity

 , , , , , , ,
, , , , , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Measurements
2.2.1. Anthropometry
2.2.2. Biochemical Evaluation
2.2.3. Evaluation of Liver Steatosis and Fibrosis
2.2.4. Targeted Metabolomic Determinations
2.3. Statistical Analysis
3. Results
3.1. Metabolic Phenotypes According to the Progression of MASLD
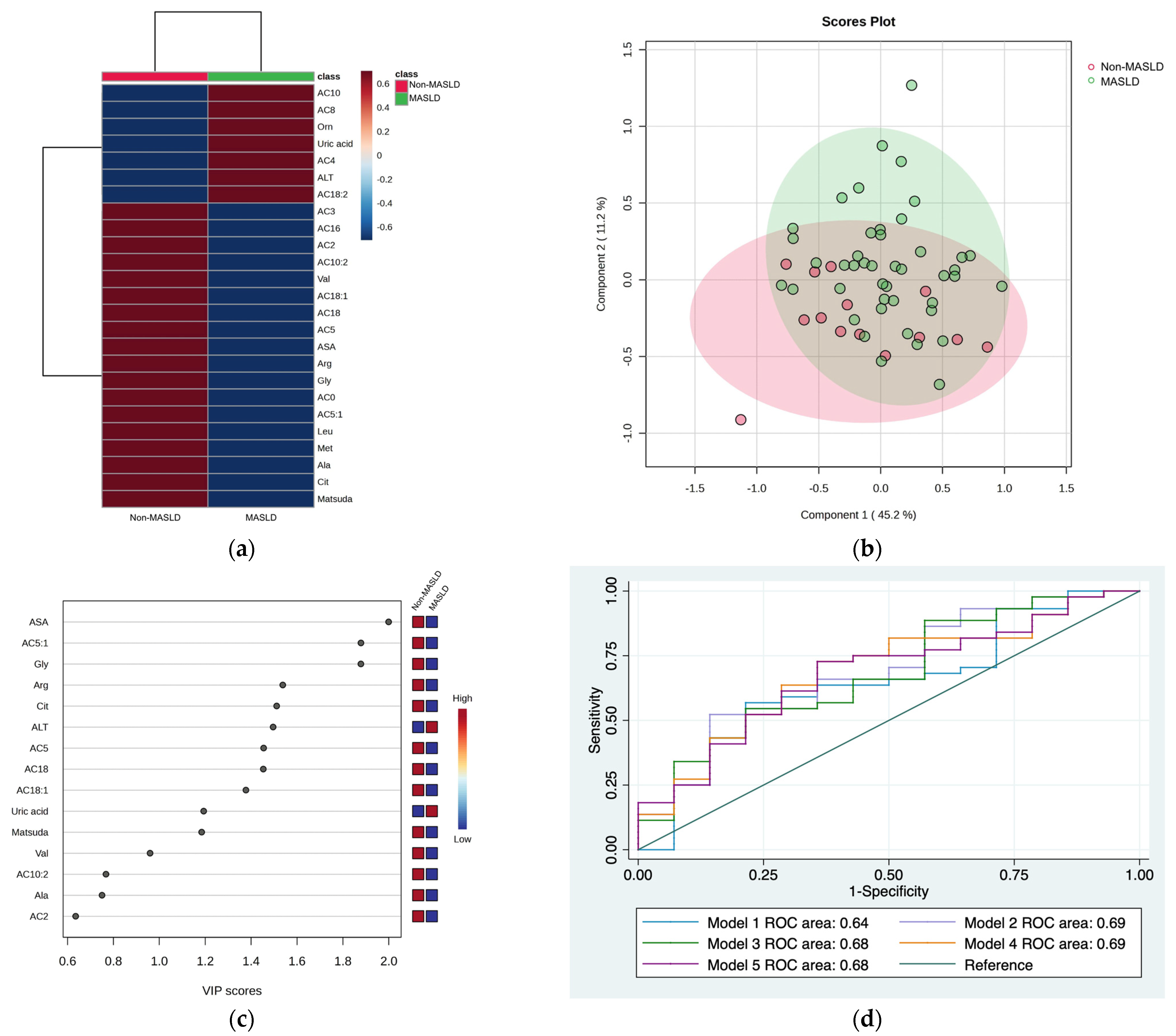
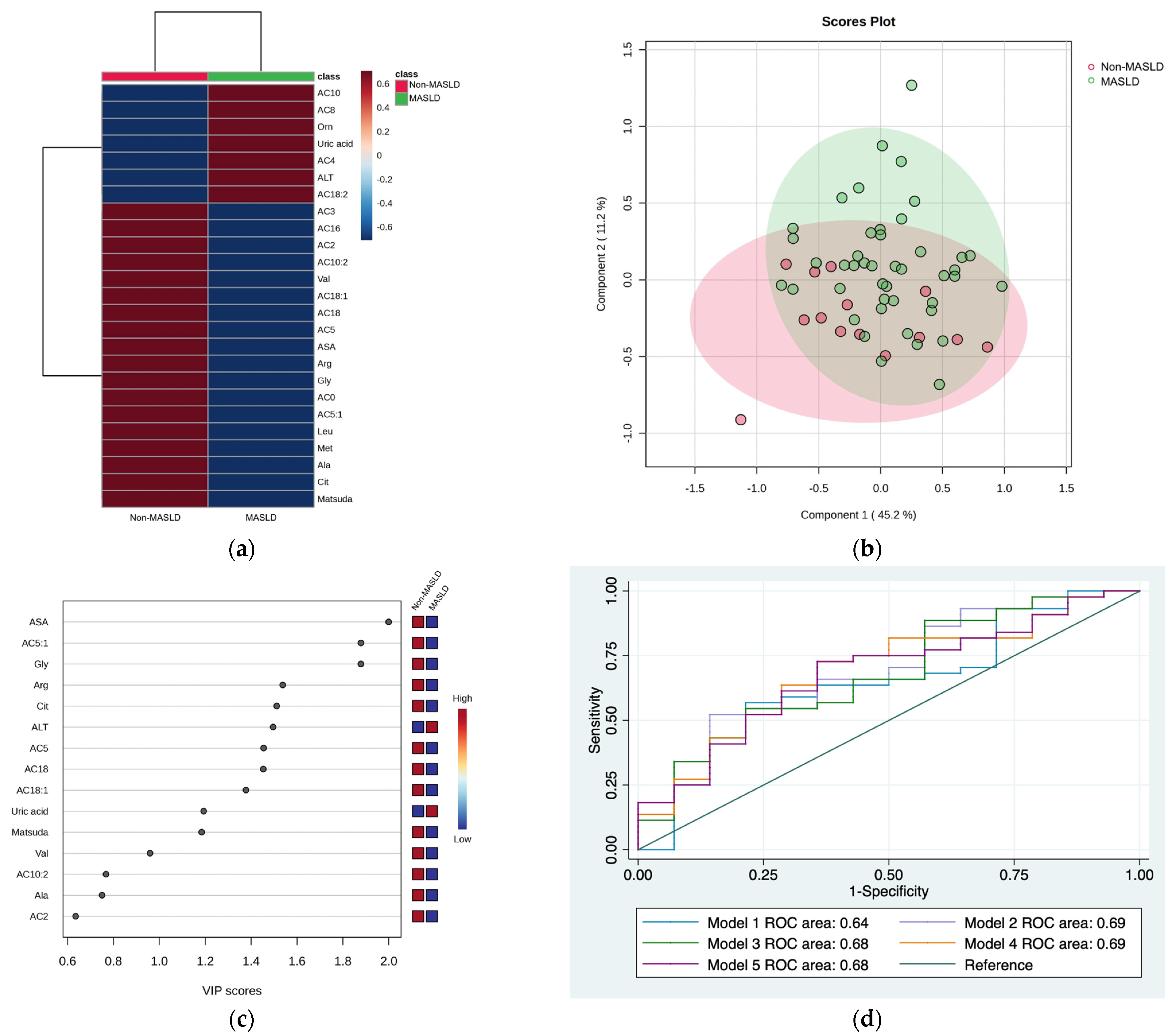
3.1.1. Non-MASLD and MASLD
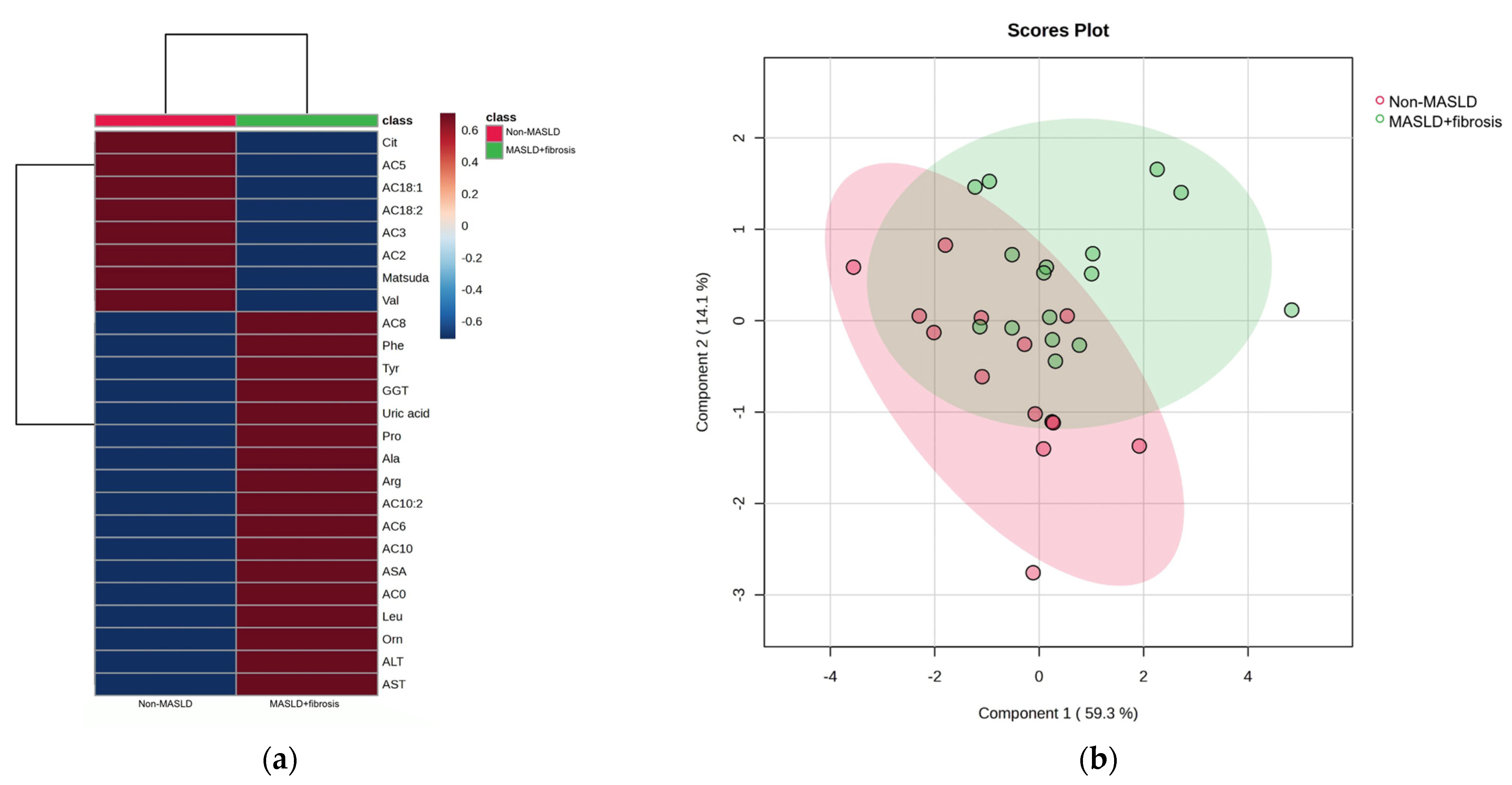
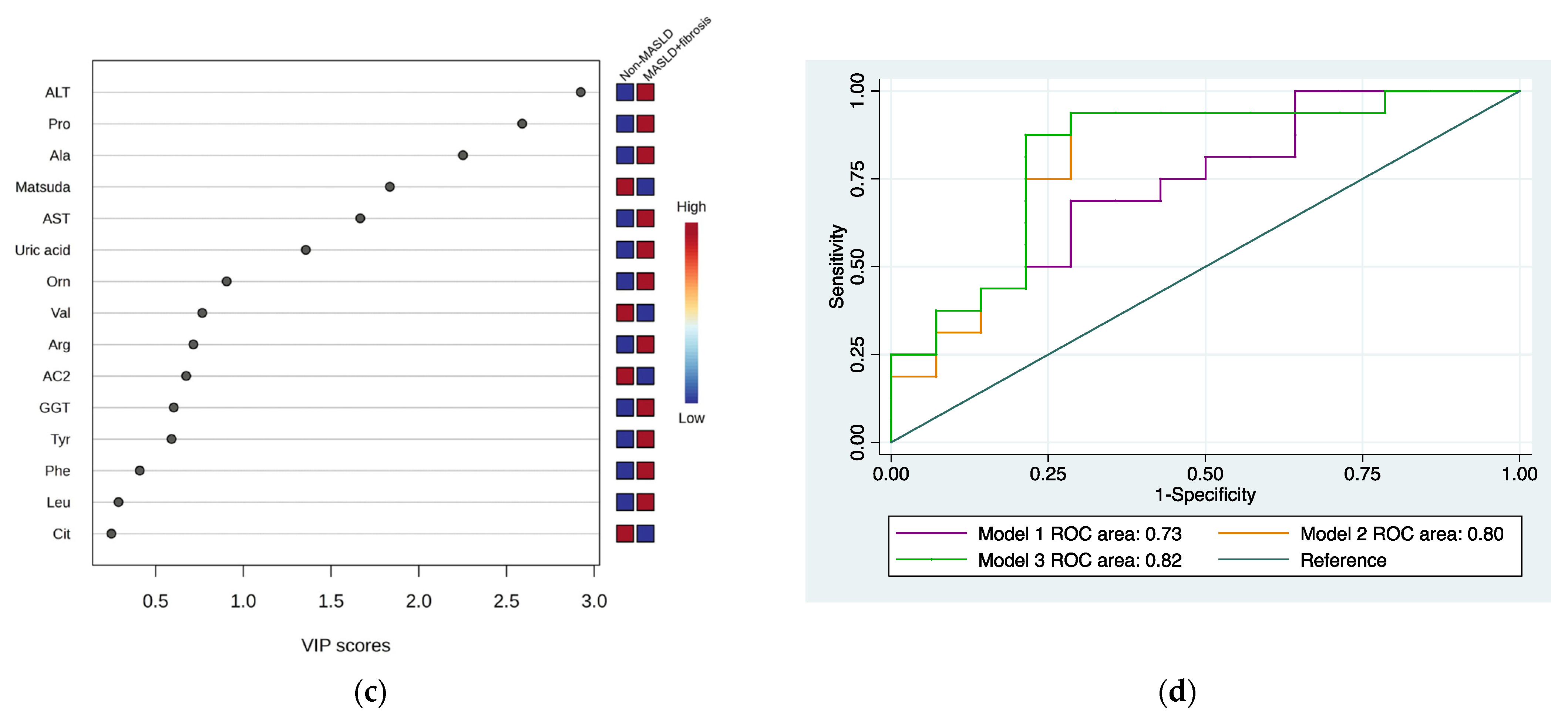
3.1.2. Non-MASLD and MASLD + Fibrosis
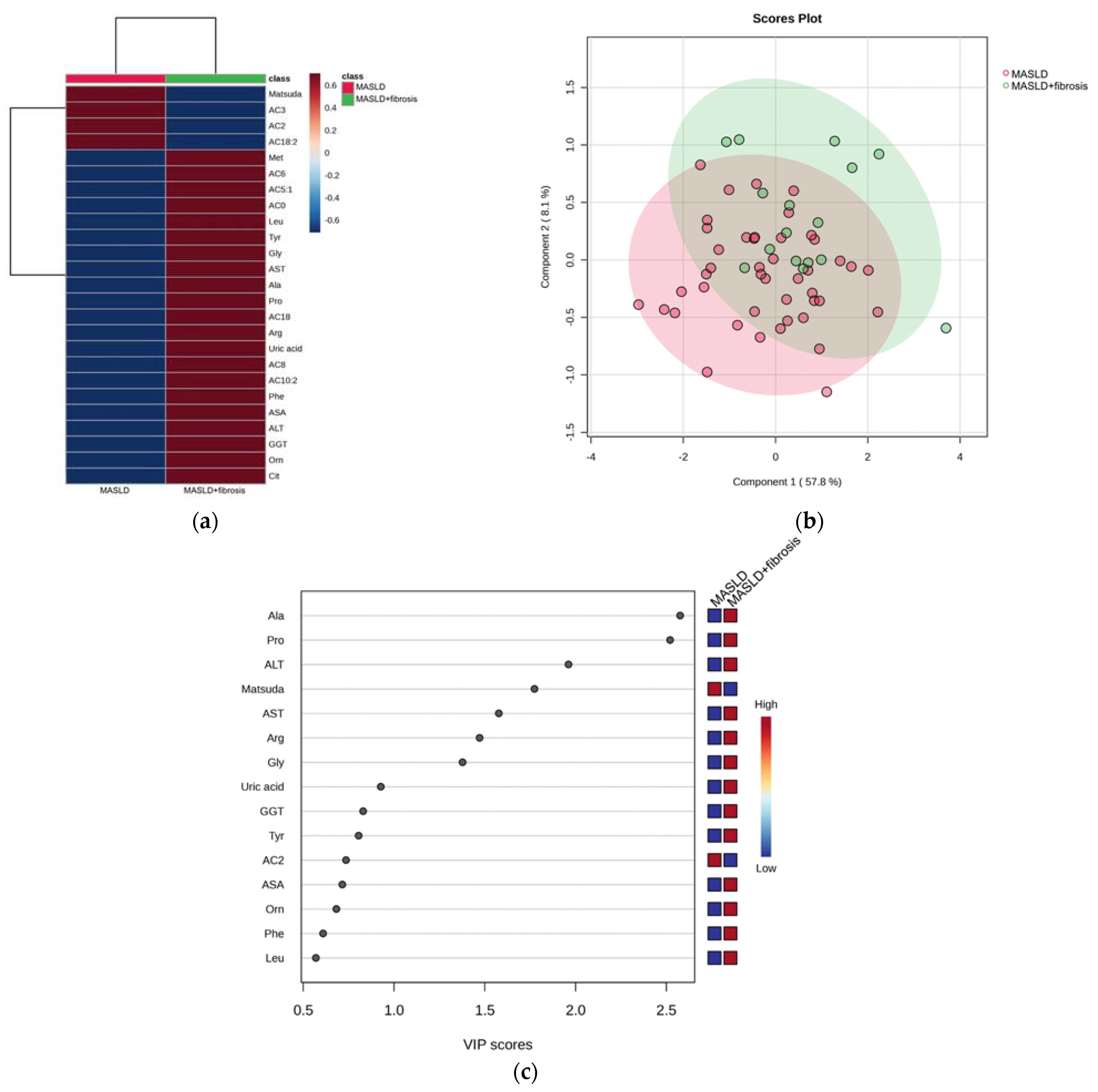
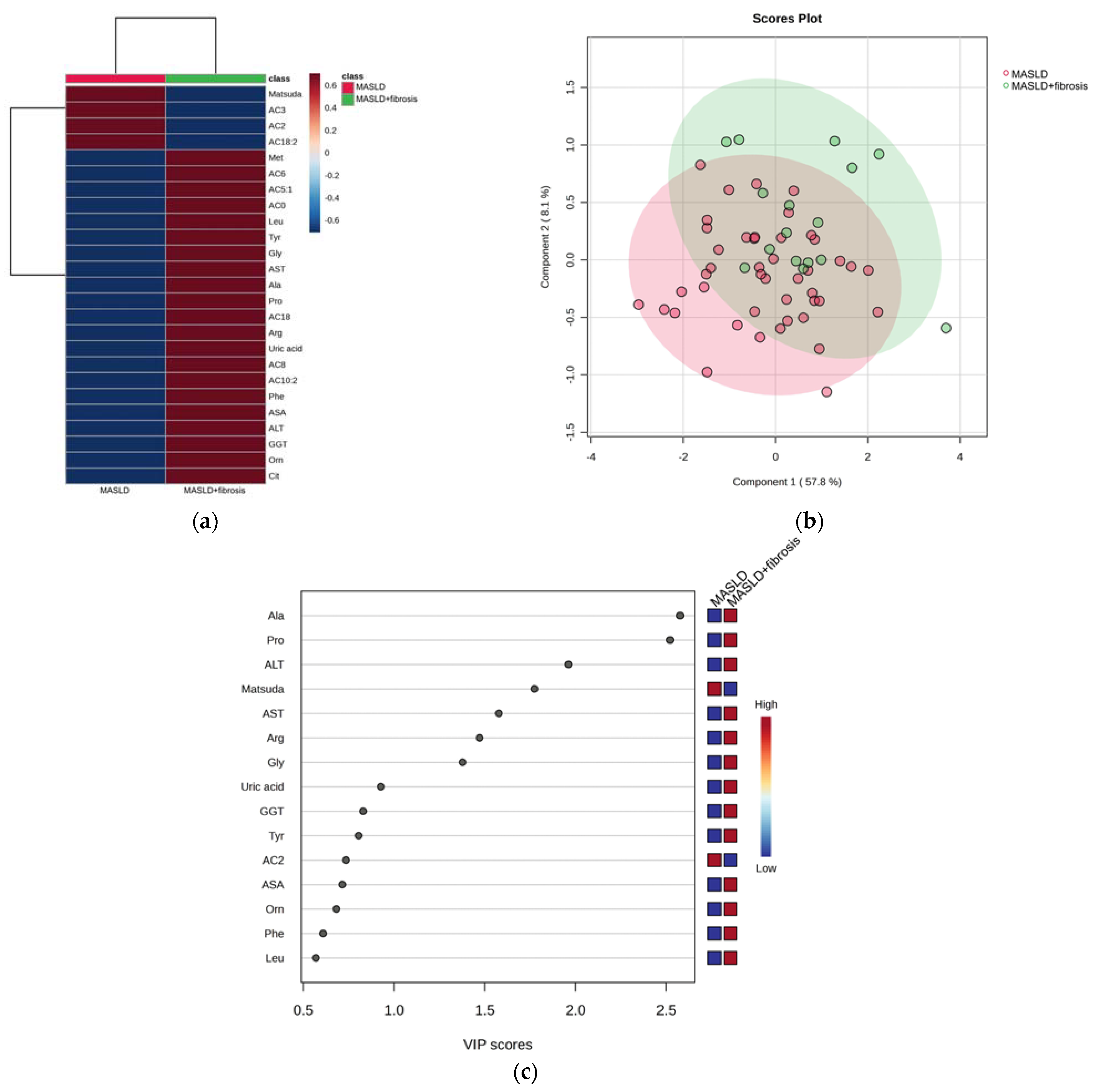
3.1.3. MASLD and MASLD + Fibrosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multi-Society Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. Hepatology 2023. [Google Scholar] [CrossRef]
- Anderson, E.L.; Howe, L.D.; Jones, H.E.; Higgins, J.P.T.; Lawlor, D.A.; Fraser, A. The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0140908. [Google Scholar] [CrossRef]
- Nobili, V.; Alisi, A.; Valenti, L.; Miele, L.; Feldstein, A.E.; Alkhouri, N. NAFLD in Children: New Genes, New Diagnostic Modalities and New Drugs. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 517–530. [Google Scholar] [CrossRef] [PubMed]
- Berentzen, T.L.; Gamborg, M.; Holst, C.; Sørensen, T.I.A.; Baker, J.L. Body Mass Index in Childhood and Adult Risk of Primary Liver Cancer. J. Hepatol. 2014, 60, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, J.B.; Newton, K.P.; Awai, H.I.; Choi, L.J.; Garcia, M.A.; Ellis, L.L.; Vanderwall, K.; Fontanesi, J. Paediatric Gastroenterology Evaluation of Overweight and Obese Children Referred from Primary Care for Suspected Non-Alcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2013, 38, 1267–1277. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, A.E.; Charatcharoenwitthaya, P.; Treeprasertsuk, S.; Benson, J.T.; Enders, F.B.; Angulo, P. The Natural History of Non-Alcoholic Fatty Liver Disease in Children: A Follow-up Study for up to 20 Years. Gut 2009, 58, 1538–1544. [Google Scholar] [CrossRef]
- Angulo, P. Long-Term Mortality in Nonalcoholic Fatty Liver Disease: Is Liver Histology of Any Prognostic Significance? Hepatology 2010, 51, 373–375. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD Fibrosis Score: A Noninvasive System That Identifies Liver Fibrosis in Patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Mandelia, C.; Collyer, E.; Mansoor, S.; Lopez, R.; Lappe, S.; Nobili, V.; Alkhouri, N. Plasma Cytokeratin-18 Level As a Novel Biomarker for Liver Fibrosis in Children With Nonalcoholic Fatty Liver Disease. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 181–187. [Google Scholar] [CrossRef]
- Jackson, J.A.; Konomi, J.V.; Mendoza, M.V.; Krasinskas, A.; Jin, R.; Caltharp, S.; Mouzaki, M.; Vos, M.B. Performance of Fibrosis Prediction Scores in Paediatric Non-Alcoholic Fatty Liver Disease. J. Paediatr. Child Health 2018, 54, 172–176. [Google Scholar] [CrossRef]
- Mansoor, S.; Yerian, L.; Kohli, R.; Xanthakos, S.; Angulo, P.; Ling, S.; Lopez, R.; Christine, C.-K.; Feldstein, A.E.; Alkhouri, N. The Evaluation of Hepatic Fibrosis Scores in Children with Nonalcoholic Fatty Liver Disease. Dig. Dis. Sci. 2015, 60, 1440–1447. [Google Scholar] [CrossRef] [PubMed]
- Shannon, A.; Alkhouri, N.; Carter-Kent, C.; Monti, L.; Devito, R.; Lopez, R.; Feldstein, A.E.; Nobili, V. Ultrasonographic Quantitative Estimation of Hepatic Steatosis in Children With NAFLD. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Runge, J.H.; van Giessen, J.; Draijer, L.G.; Deurloo, E.E.; Smets, A.M.J.B.; Benninga, M.A.; Koot, B.G.P.; Stoker, J. Accuracy of Controlled Attenuation Parameter Compared with Ultrasound for Detecting Hepatic Steatosis in Children with Severe Obesity. Eur. Radiol. 2021, 31, 1588–1596. [Google Scholar] [CrossRef]
- Middleton, M.S.; Van Natta, M.L.; Heba, E.R.; Alazraki, A.; Trout, A.T.; Masand, P.; Brunt, E.M.; Kleiner, D.E.; Doo, E.; Tonascia, J.; et al. Diagnostic Accuracy of Magnetic Resonance Imaging Hepatic Proton Density Fat Fraction in Pediatric Nonalcoholic Fatty Liver Disease. Hepatology 2018, 67, 858–872. [Google Scholar] [CrossRef] [PubMed]
- Draijer, L.G.; van Oosterhout, J.P.M.; Vali, Y.; Zwetsloot, S.; van der Lee, J.H.; van Etten-Jamaludin, F.S.; Chegary, M.; Benninga, M.A.; Koot, B.G.P. Diagnostic Accuracy of Fibrosis Tests in Children with Non-Alcoholic Fatty Liver Disease: A Systematic Review. Liver Int. Off. J. Int. Assoc. Study Liver 2021, 41, 2087–2100. [Google Scholar] [CrossRef] [PubMed]
- de Lédinghen, V.; Le Bail, B.; Rebouissoux, L.; Fournier, C.; Foucher, J.; Miette, V.; Castéra, L.; Sandrin, L.; Merrouche, W.; Lavrand, F.; et al. Liver Stiffness Measurement in Children Using FibroScan: Feasibility Study and Comparison with Fibrotest, Aspartate Transaminase to Platelets Ratio Index, and Liver Biopsy. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 443–450. [Google Scholar] [CrossRef]
- Kordy, K.; Li, F.; Lee, D.J.; Kinchen, J.M.; Jew, M.H.; La Rocque, M.E.; Zabih, S.; Saavedra, M.; Woodward, C.; Cunningham, N.J.; et al. Metabolomic Predictors of Non-Alcoholic Steatohepatitis and Advanced Fibrosis in Children. Front. Microbiol. 2021, 12, 713234. [Google Scholar] [CrossRef]
- Goffredo, M.; Santoro, N.; Tricò, D.; Giannini, C.; D’Adamo, E.; Zhao, H.; Peng, G.; Yu, X.; Lam, T.T.; Pierpont, B.; et al. A Branched-Chain Amino Acid-Related Metabolic Signature Characterizes Obese Adolescents with Non-Alcoholic Fatty Liver Disease. Nutrients 2017, 9, 642. [Google Scholar] [CrossRef]
- Lischka, J.; Schanzer, A.; Hojreh, A.; Ba Ssalamah, A.; Item, C.B.; de Gier, C.; Walleczek, N.; Metz, T.F.; Jakober, I.; Greber-Platzer, S.; et al. A Branched-chain Amino Acid-based Metabolic Score Can Predict Liver Fat in Children and Adolescents with Severe Obesity. Pediatr. Obes. 2021, 16, e12739. [Google Scholar] [CrossRef]
- Jin, R.; Banton, S.; Tran, V.T.; Konomi, J.V.; Li, S.; Jones, D.P.; Vos, M.B. Amino Acid Metabolism Is Altered in Adolescents with NAFLD—An Untargeted, High Resolution Metabolomics Study. J. Pediatr. 2016, 172, 14–19.e5. [Google Scholar] [CrossRef]
- Caballero, B.; Vorkoper, S.; Anand, N.; Rivera, J.A. Preventing Childhood Obesity in Latin America: An Agenda for Regional Research and Strategic Partnerships. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18 (Suppl. S2), 3–6. [Google Scholar] [CrossRef]
- Gulati, A.K.; Kaplan, D.W.; Daniels, S.R. Clinical Tracking of Severely Obese Children: A New Growth Chart. Pediatrics 2012, 130, 1136–1140. [Google Scholar] [CrossRef] [PubMed]
- Marshall, W.A.; Tanner, J.M. Variations in the Pattern of Pubertal Changes in Boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; DeFronzo, R. Insulin Sensitivity Indices Obtained from Comparison with the Euglycemic Insulin Clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and β-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Desai, N.K.; Harney, S.; Raza, R.; Al-Ibraheemi, A. Comparison of Controlled Attenuation Parameter and Liver Biopsy to Assess Hepatic Steatosis in Pediatric Patients. J. Pediatr. 2016, 173, 160–164. [Google Scholar] [CrossRef]
- Nobili, V.; Vizzutti, F.; Arena, U.; Abraldes, J.G.; Marra, F.; Pietrobattista, A.; Fruhwirth, R.; Marcellini, M.; Pinzani, M. Accuracy and Reproducibility of Transient Elastography for the Diagnosis of Fibrosis in Pediatric Nonalcoholic Steatohepatitis. Hepatology 2008, 48, 442–448. [Google Scholar] [CrossRef]
- Hadizadeh, F.; Faghihimani, E.; Adibi, P. Nonalcoholic Fatty Liver Disease: Diagnostic Biomarkers. World J. Gastrointest. Pathophysiol. 2017, 8, 11–26. [Google Scholar] [CrossRef]
- Ma, Q.; Liao, X.; Shao, C.; Lin, Y.; Wu, T.; Sun, Y.; Feng, S.-T.; Ye, J.; Zhong, B. Normalization of γ-Glutamyl Transferase Levels Is Associated with Better Metabolic Control in Individuals with Nonalcoholic Fatty Liver Disease. BMC Gastroenterol. 2021, 21, 215. [Google Scholar] [CrossRef]
- Vos, M.B.; Abrams, S.H.; Barlow, S.E.; Caprio, S.; Daniels, S.R.; Kohli, R.; Mouzaki, M.; Sathya, P.; Schwimmer, J.B.; Sundaram, S.S.; et al. NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 319–334. [Google Scholar] [CrossRef]
- Fracanzani, A.L.; Valenti, L.; Bugianesi, E.; Andreoletti, M.; Colli, A.; Vanni, E.; Bertelli, C.; Fatta, E.; Bignamini, D.; Marchesini, G.; et al. Risk of Severe Liver Disease in Nonalcoholic Fatty Liver Disease with Normal Aminotransferase Levels: A Role for Insulin Resistance and Diabetes. Hepatology 2008, 48, 792–798. [Google Scholar] [CrossRef]
- Morris, S.M. Arginine Metabolism Revisited. J. Nutr. 2016, 146, 2579S–2586S. [Google Scholar] [CrossRef] [PubMed]
- Scheja, L.; Kluwe, J. Arginine and NASH—Do Macrophages Deliver the First Hit? J. Hepatol. 2015, 62, 260–261. [Google Scholar] [CrossRef] [PubMed]
- Forzano, I.; Avvisato, R.; Varzideh, F.; Jankauskas, S.S.; Cioppa, A.; Mone, P.; Salemme, L.; Kansakar, U.; Tesorio, T.; Trimarco, V.; et al. L-Arginine in Diabetes: Clinical and Preclinical Evidence. Cardiovasc. Diabetol. 2023, 22, 89. [Google Scholar] [CrossRef]
- Scapaticci, S.; D’Adamo, E.; Mohn, A.; Chiarelli, F.; Giannini, C. Non-Alcoholic Fatty Liver Disease in Obese Youth With Insulin Resistance and Type 2 Diabetes. Front. Endocrinol. 2021, 12, 639548. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.; Bassot, A.; Bulteau, A.-L.; Pirola, L.; Morio, B. Glycine Metabolism and Its Alterations in Obesity and Metabolic Diseases. Nutrients 2019, 11, 1356. [Google Scholar] [CrossRef]
- Gaggini, M.; Carli, F.; Rosso, C.; Buzzigoli, E.; Marietti, M.; Della Latta, V.; Ciociaro, D.; Abate, M.L.; Gambino, R.; Cassader, M.; et al. Altered Amino Acid Concentrations in NAFLD: Impact of Obesity and Insulin Resistance. Hepatology 2018, 67, 145–158. [Google Scholar] [CrossRef]
- Butte, N.F.; Liu, Y.; Zakeri, I.F.; Mohney, R.P.; Mehta, N.; Voruganti, V.S.; Göring, H.; Cole, S.A.; Comuzzie, A.G. Global Metabolomic Profiling Targeting Childhood Obesity in the Hispanic Population. Am. J. Clin. Nutr. 2015, 102, 256–267. [Google Scholar] [CrossRef]
- Chae, W.; Lee, K.J.; Huh, K.Y.; Moon, J.S.; Ko, J.S.; Cho, J.-Y. Association of Metabolic Signatures with Nonalcoholic Fatty Liver Disease in Pediatric Population. Metabolites 2022, 12, 881. [Google Scholar] [CrossRef]
- Violante, S.; IJlst, L.; Ruiter, J.; Koster, J.; van Lenthe, H.; Duran, M.; de Almeida, I.T.; Wanders, R.J.A.; Houten, S.M.; Ventura, F.V. Substrate Specificity of Human Carnitine Acetyltransferase: Implications for Fatty Acid and Branched-Chain Amino Acid Metabolism. Biochim. Biophys. Acta BBA-Mol. Basis Dis. 2013, 1832, 773–779. [Google Scholar] [CrossRef]
- Danese, C.; Cirene, M.; Colotto, M.; Aratari, A.; Amato, S.; Di Bona, S.; Curione, M. Cardiac Involvement in Inflammatory Bowel Disease: Role of Acylcarnitine Esters. Clin. Ter. 2011, 162, e105–e109. [Google Scholar]
- Yu, Z.-R.; Ning, Y.; Yu, H.; Tang, N.-J. A HPLC-Q-TOF-MS-Based Urinary Metabolomic Approach to Identification of Potential Biomarkers of Metabolic Syndrome. J. Huazhong Univ. Sci. Technol. Med. Sci. Huazhong Keji Daxue Xuebao Yixue Yingdewen Ban 2014, 34, 276–283. [Google Scholar] [CrossRef]
- Vettore, L.A.; Westbrook, R.L.; Tennant, D.A. Proline Metabolism and Redox; Maintaining a Balance in Health and Disease. Amino Acids 2021, 53, 1779–1788. [Google Scholar] [CrossRef]
- Wu, G.; Bazer, F.W.; Burghardt, R.C.; Johnson, G.A.; Kim, S.W.; Knabe, D.A.; Li, P.; Li, X.; McKnight, J.R.; Satterfield, M.C.; et al. Proline and Hydroxyproline Metabolism: Implications for Animal and Human Nutrition. Amino Acids 2011, 40, 1053–1063. [Google Scholar] [CrossRef]
- Bataller, R.; Brenner, D.A. Liver Fibrosis. J. Clin. Investig. 2005, 115, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Heyens, L.J.M.; Busschots, D.; Koek, G.H.; Robaeys, G.; Francque, S. Liver Fibrosis in Non-Alcoholic Fatty Liver Disease: From Liver Biopsy to Non-Invasive Biomarkers in Diagnosis and Treatment. Front. Med. 2021, 8, 615978. [Google Scholar] [CrossRef] [PubMed]
- Gabr, S.A.; Alghadir, A.H.; Sherif, Y.E.; Ghfar, A.A. Hydroxyproline as a Biomarker in Liver Disease. In Biomarkers in Liver Disease; Patel, V.B., Preedy, V.R., Eds.; Biomarkers in Disease: Methods, Discoveries and Applications; Springer: Dordrecht, The Netherlands, 2017; pp. 471–491. ISBN 978-94-007-7675-3. [Google Scholar]
- Romero-Ibarguengoitia, M.E.; Vadillo-Ortega, F.; Caballero, A.E.; Ibarra-González, I.; Herrera-Rosas, A.; Serratos-Canales, M.F.; León-Hernández, M.; González-Chávez, A.; Mummidi, S.; Duggirala, R.; et al. Family History and Obesity in Youth, Their Effect on Acylcarnitine/Aminoacids Metabolomics and Non-Alcoholic Fatty Liver Disease (NAFLD). Structural Equation Modeling Approach. PLoS ONE 2018, 13, e0193138. [Google Scholar] [CrossRef]
- Lavine, J.E.; Schwimmer, J.B.; Van Natta, M.L.; Molleston, J.P.; Murray, K.F.; Rosenthal, P.; Abrams, S.H.; Scheimann, A.O.; Sanyal, A.J.; Chalasani, N.; et al. Effect of Vitamin E or Metformin for Treatment of Nonalcoholic Fatty Liver Disease in Children and Adolescents: The TONIC Randomized Controlled Trial. JAMA 2011, 305, 1659–1668. [Google Scholar] [CrossRef]
- Chaidez, A.; Pan, Z.; Sundaram, S.S.; Boster, J.; Lovell, M.; Sokol, R.J.; Mack, C.L. The Discriminatory Ability of FibroScan Liver Stiffness Measurement, Controlled Attenuation Parameter, and FibroScan-Aspartate Aminotransferase to Predict Severity of Liver Disease in Children. Hepatol. Commun. 2022, 6, 3015–3023. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Non-MASLD n = 14 Mean (SD) | MASLD n = 44 Mean (SD) | MASLD + Fibrosis n = 16 Mean (SD) | p-Value |
|---|---|---|---|---|
| Age (years) | 10.46 ± 1.39 | 11.31 ± 2.39 | 11.69 ± 2.24 | 0.32 |
| Duration of obesity (years) | 4.73 ± 4.28 | 5.57 ± 4.12 | 4.15 ± 2.60 | 0.49 |
| Weight (kg) | 51.80 ± 10.42 | 61.58 ± 14.08 | 62.54 ± 13.22 | 0.053 |
| Height (cm) | 142.69 ± 7.54 | 148.55 ± 10.43 | 150.11 ± 11.55 | 0.12 |
| BMI z-Score | 1.88 ± 0.17 | 2.05 ± 0.29 | 2.07 ± 0.41 | 0.17 |
| Waist circumference (cm) | 80.63 ± 9.37 a | 87.48 ± 8.26 b | 88.85 ± 8.59 b | 0.023 |
| Lean body mass (kg) | 36.16 ± 4.78 | 41.17 ± 7.39 | 41.71 ± 8.43 | 0.72 |
| Body Fat Mass (kg) | 15.03 ± 6.27 | 19.82 ± 7.29 | 20.45 ± 5.54 | 0.061 |
| Systolic BP (mmHg) | 103.54 ± 9.30 | 105.56 ± 9.78 | 108.30 ± 14.32 | 0.49 |
| Diastolic BP (mmHg) | 66.67 ± 8.36 | 69.40 ± 7.21 | 69.25 ± 11.25 | 0.60 |
| Glucose (mg/dL) | 89.30 ± 5.43 | 89.44 ± 8.55 | 94.00 ± 6.07 | 0.17 |
| Uric acid (mg/dL) | 5.03 ± 1.21 | 5.58 ± 0.96 | 5.92 ± 0.98 | 0.36 |
| Total cholesterol (mg/dL) | 158.61 ± 28.32 | 158.82 ± 24.86 | 158.87 ± 26.16 | 0.46 |
| Triglycerides (mg/dL) | 141.07 ± 61.20 | 168.68 ± 86.37 | 149.68 ± 108.30 | 0.72 |
| HDL-Chol (mg/dL) | 39.07 ± 3.88 | 38.88 ± 8.42 | 37.75 ± 7.10 | 0.38 |
| LDL-Chol (mg/dL) | 102.30 ± 22.98 | 100.95 ± 17.89 | 105.75 ± 22.43 | 0.28 |
| ALT IU/L | 18.38 ± 4.94 a | 29.02 ± 19.02 b | 36.81 ± 25.57 b | 0.014 |
| AST IU/L | 23.84 ± 3.78 | 26.88 ± 8.73 | 31.00 ± 13.11 | 0.22 |
| GGT IU/L | 16.15 ± 5.36 | 19.28 ± 8.67 | 20.06 ± 9.69 | 0.69 |
| Insulin IU/L | 16.53 ± 11.11 | 18.34 ± 9.6 | 21.46 ± 8.23 | 0.29 |
| HOMA-IR | 3.63 ± 2.49 | 4.20 ± 2.27 | 5.00 ± 1.99 | 0.23 |
| Matsuda-ISI | 3.48 ± 2.53 | 3.23 ± 2.22 | 2.07 ± 1.07 | 0.051 |
| CAP dB/m | 176.60 ± 45.03 a | 279.69 ± 37.90 b | 287.06 ± 56.17 b | <0.001 |
| kPa | 3.97 ± 0.59 a | 3.91 ± 0.72 a | 6.25 ± 1.80 b | <0.001 |
| Glycine | 100.81 ± 22.85 | 100.39 ± 16.90 | 103.83 ± 16.90 | 0.31 |
| Arginine | 29.23 ± 4.85 | 29.01 ± 4.00 | 31.89 ± 6.59 | 0.10 |
| Citrulline | 9.23 ± 1.72 | 9.39 ± 1.46 | 9.41 ± 2.29 | 0.45 |
| Proline | 63.12 ± 8.69 a | 67.56 ± 16.18 a | 81.29 ± 21.18 b | 0.005 |
| Alanine | 115.77 ± 23.38 a | 119.43 ± 18.86 a | 137.54 ± 20.19 b | 0.014 |
| ASA | 1.75 ± 0.14 | 1.73 ± 0.20 | 1.81 ± 0.22 | 0.39 |
| Tiglylcarnitine (C5:1) | 0.03385 ± 0.004 | 0.03333 ± 0.0054 | 0.03375 ± 0.005 | 0.28 |
| Pubertal Tanner stage | n (%) | n (%) | n (%) | p-value |
| Prepubertal | 8 (57.1) | 17 (38.6) | 4 (25.0) | 0.526 |
| Early puberty | 3 (21.4) | 15 (34.1) | 6 (37.5) | |
| Advanced puberty | 3 (21.4) | 12 (27.3) | 6 (37.5) |
| Model Tested | ROC Area |
|---|---|
| MASLD phenotype | |
| Model 1: ASA + AC5:1 + glycine + arginine + citrulline | 0.64 |
| Model 2: Model 1 + ALT | 0.68 |
| Model 3: AC5:1 + glycine + arginine + citrulline + ALT | 0.68 |
| Model 4: AC5:1 + glycine + arginine + ALT | 0.69 |
| Model 5: glycine + arginine + ALT | 0.69 |
| MASLD + fibrosis phenotype | |
| Model 1: ALT + proline + alanine | 0.73 |
| Model 2: ALT + proline + alanine + Matsuda Index | 0.80 |
| Model 3: ALT + proline + alanine + Matsuda Index + AST | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garibay-Nieto, N.; Pedraza-Escudero, K.; Omaña-Guzmán, I.; Garcés-Hernández, M.J.; Villanueva-Ortega, E.; Flores-Torres, M.; Pérez-Hernández, J.L.; León-Hernández, M.; Laresgoiti-Servitje, E.; Palacios-González, B.; et al. Metabolomic Phenotype of Hepatic Steatosis and Fibrosis in Mexican Children Living with Obesity. Medicina 2023, 59, 1785. https://doi.org/10.3390/medicina59101785
Garibay-Nieto N, Pedraza-Escudero K, Omaña-Guzmán I, Garcés-Hernández MJ, Villanueva-Ortega E, Flores-Torres M, Pérez-Hernández JL, León-Hernández M, Laresgoiti-Servitje E, Palacios-González B, et al. Metabolomic Phenotype of Hepatic Steatosis and Fibrosis in Mexican Children Living with Obesity. Medicina. 2023; 59(10):1785. https://doi.org/10.3390/medicina59101785
Chicago/Turabian StyleGaribay-Nieto, Nayely, Karen Pedraza-Escudero, Isabel Omaña-Guzmán, María José Garcés-Hernández, Eréndira Villanueva-Ortega, Mariana Flores-Torres, José Luis Pérez-Hernández, Mireya León-Hernández, Estibalitz Laresgoiti-Servitje, Berenice Palacios-González, and et al. 2023. "Metabolomic Phenotype of Hepatic Steatosis and Fibrosis in Mexican Children Living with Obesity" Medicina 59, no. 10: 1785. https://doi.org/10.3390/medicina59101785
APA StyleGaribay-Nieto, N., Pedraza-Escudero, K., Omaña-Guzmán, I., Garcés-Hernández, M. J., Villanueva-Ortega, E., Flores-Torres, M., Pérez-Hernández, J. L., León-Hernández, M., Laresgoiti-Servitje, E., Palacios-González, B., López-Alvarenga, J. C., Lisker-Melman, M., & Vadillo-Ortega, F. (2023). Metabolomic Phenotype of Hepatic Steatosis and Fibrosis in Mexican Children Living with Obesity. Medicina, 59(10), 1785. https://doi.org/10.3390/medicina59101785